
Abstract
Background
A representative method for compensating for tooth loss is implant placement. Dental implants consist of a crown, an abutment, and an artificial tooth root, and are made of various materials. Proper care is essential for the long-term use of implants, and negligence in care can lead to inflammation around the implant. The most representative inflammation that occurs around implants is peri-implantitis, and various laser treatments are being studied recently to eliminate it.
Objective
In this study, the effect of implant materials on temperature rise within inflamed tissue was analyzed both theoretically and numerically in removal of peri-implantitis using photothermal therapy.
Methods
The temperature distribution in tissue for various artificial root materials, laser irradiation angles, and intensities was calculated, and degree of tissue death was determined using the Arrhenius damage integral. Furthermore, percentage of tissue death was analyzed using the Arrhenius thermal damage ratio and the normal tissue Arrhenius thermal damage ratio to identify trends in the results based on treatment conditions.
Results
Consequently, with regard to materials used for artificial tooth roots, the prevailing trend in treatment indicates that zirconia is the most effective material, followed by Ti-6Al-4V, titanium, and tantalum. The efficacy of laser irradiation increases as the angle approaches vertical.
Conclusion
The findings indicate that increasing laser power and reducing the irradiation angle are beneficial when focusing solely on inflammation.
Introduction
Tooth damage is on the rise due to lifestyle and dietary influences, leading to an increase in dental implant placement to replace damaged teeth.1,2 Proper care is necessary to maintain these implants over the long term; otherwise, inflammation can occur around the implant, potentially requiring removal. 3 A representative example of such inflammation is peri-implantitis, which, if left untreated for an extended period, can damage the surrounding tissues.4,5 Therefore, proper management of the implant and rapid removal of inflammation are essential to preserve the implant and prevent damage to the surrounding tissue.6,7
There are two main methods to remove the inflammation that occurs around implants.8,9 Physical removal has the advantage of ensuring complete removal, but it can be challenging depending on the location of the inflammation. 10 Chemical removal has the benefit of causing less physical damage and no bleeding, but it may have potential side effects. 11 As a result, laser treatment techniques have recently gained traction in the dental field. 12 Photothermal therapy is a type of laser treatment that uses a photothermal effect to raise the temperature of the inflamed tissue, effectively killing it. 13 This treatment offers advantages such as no bleeding and rapid recovery. 14
Research on laser dental treatments is being conducted from various perspectives. Ren et al. 15 performed treatment of chronic periodontitis using low-level laser irradiation. A clinical trial was conducted on 27 adults, where repeated diode laser treatment was performed on one side of the teeth, and pseudo-laser treatment was performed on the other side. Subjective pain, periodontal status, cytokines in gingival crevicular fluid, and periodontopathic bacteria were evaluated. The results showed that the intensity of pain was lower on the laser-treated side compared to the control side, with the exception of bacterial levels, indicating a benefit of laser treatment. Sezen et al. 16 determined the clinical and biochemical efficacy of treatment with various lasers in combination with non-surgical periodontal treatment (NSPT) in patients with periodontitis. Plaque index, gingival index, probing depth, clinical attachment level, bleeding on probing, gingival crevicular fluid (GCF) volume and IL-1β and MMP-8 levels in GCF were measured. The treatment results confirmed a statistically significant clinical improvement with laser treatment, and that Er,Cr:YSGG laser treatment performed in conjunction with NSPT reduced clinical inflammation.
Laser treatment studies in dentistry primarily focus on analyzing treatment outcomes, and there is still a lack of research on establishing treatment conditions through theoretical analysis. The artificial tooth roots in dental implants are made from a variety of materials. 17 However, research analyzing treatment outcomes for artificial roots made of different materials is also insufficient. Therefore, in this study, the temperature distribution in inflamed and surrounding normal tissues was theoretically analyzed for various artificial root materials, laser irradiation angles, and power levels during photothermal treatment of peri-implantitis. By applying the Arrhenius damage integral, which identifies the degree of tissue death based on the calculated temperature distribution, the degree of death of inflamed and normal tissues was calculated. The Arrhenius thermal damage ratio proposed by Paik et al. 18 was used to quantitatively determine the percentage of tissue death.
Materials and methods
Tissue temperature analysis theory
In this study, the temperature distribution in the tissue under laser irradiation for peri-implantitis was calculated. The Pennes bioheat equation was used, as shown in Equation (1).
19
The temperature change over time is calculated by considering blood flow, metabolism, and heat transfer by the laser, where ρ, cp, T, k, qb, ωb, Tb, and qm represent density, specific heat, temperature, thermal conductivity, heat transfer term by blood flow, blood perfusion rate, blood temperature, and heat transfer term by metabolism, respectively.

In Equation (2), ql represents the heat transfer term by the laser. The reflectivity of the tissue, energy depending on the irradiated area, energy attenuation for each coordinate, laser irradiation angle, and the effect of the irradiation position are considered, where Rt, μa, θ, Pl, rl, μtot, dx, and dz represent reflectivity, absorption coefficient, laser irradiation angle, laser power, laser radius, attenuation coefficient, and differential length for x and z directions, respectively.20,21

For total reflectance Rt, it is calculated as the sum of specular R1 and diffuse R2 (Equation (3)). R1 is calculated from θ and the refractive indices of air (n1) and inflammation (n2), which are 1 and 1.373, respectively.22,23 R2 varies depending on the wavelength of the laser used; in this study, a value of 0.28 at a wavelength of 630 nm was used. 24
Inflammation elimination analysis theory
As the final objective of this study was to quantify the magnitude of peri-implantitis death, the Arrhenius damage integral was used to determine this (Eq. (4)).
25
Where Ω, A, R, and Ea represent the damage degree of inflammation, frequency factor, ideal gas constant (8.314 J/mol·K), and activation energy, respectively. If Ω is ≥ 1, it can be concluded that the tissue has died. Due to the lack of information on A and Ea for peri-implantitis, this study used the values of A = 2.84 × 1099 s-1 and Ea = 0.618 MJ/mol for normal cells. 26
Additionally, using the calculated Ω, the percentage of inflammation and surrounding normal tissue death was quantitatively confirmed. Arrhenius thermal damage ratio (ϕArrh) proposed by Paik et al.
18
was used, which is calculated as the ratio of the area with Ω ≥ 1 to the total inflammation (Equation (5)). Moreover, a variable called normal tissue Arrhenius thermal damage ratio (ϕNArrh) is presented to determine the percentage of surrounding normal tissue death. ϕNArrh can be calculated as the ratio of the area in the surrounding normal tissue with Ω ≥ 1 to the volume of the total surrounding normal tissue (Equation (6)). As different values of ϕNArrh are calculated depending on the range of surrounding normal tissue, a distance of up to 50% of the inflammation transverse length was selected as the volume of total normal tissue in this study.
27


Numerical analysis conditions
In this study, photothermal treatment for peri-implantitis was simulated using the commercial program COMSOL Multiphysics. Figure 1 shows a schematic of the implant and its surrounding tissues. A three-dimensional numerical analysis model was established, including the implants, gingival, alveolar bone, and inflammation. The upper part of the implant is set in the air zone, and the implants itself consists of a crown, abutment, and artificial tooth root. The vertical lengths of each component were set to 8.5 mm, 2 mm, and 13 mm, respectively. The inflammation was modeled as a cone shape and was assumed to be located between the right surface of the implant and the gum. The width and depth of the inflammation were set to 1.5 mm and 9 mm, respectively. The physical properties and geometry of each tissue may vary by race, gender, and for each individual. However, there are too many variables to account for all of these, making it difficult to analyze the results, so this study used geometry information from each of the previous studies.28–31 The thermal and optical properties for each component are summarized in Table 1.

Schematic of numerical analysis.
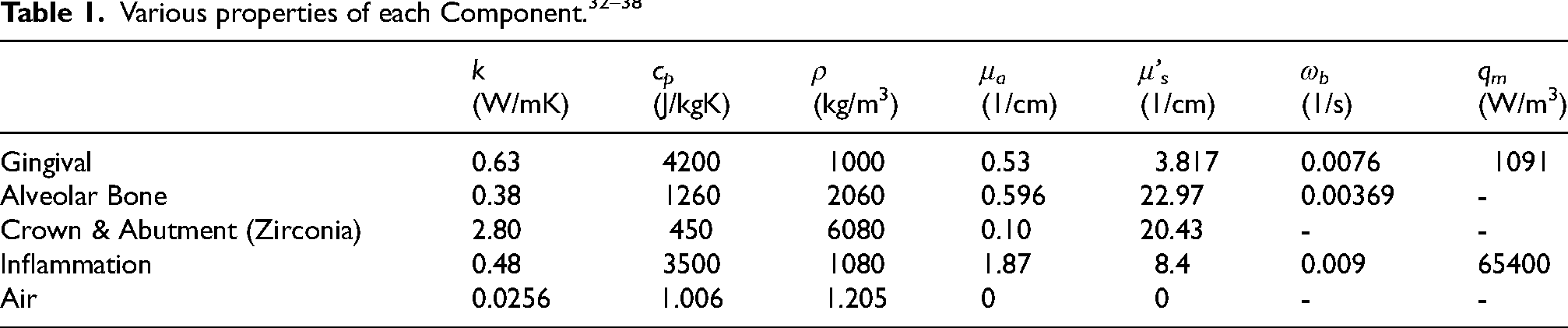
Additionally, the study varied the material of the implant's artificial tooth root to determine the treatment effects of each material. Four materials were selected for the artificial tooth roots: zirconia, Ti-6Al-4V, tantalum, and titanium. The thermal and optical properties of each material are summarized in Table 2.
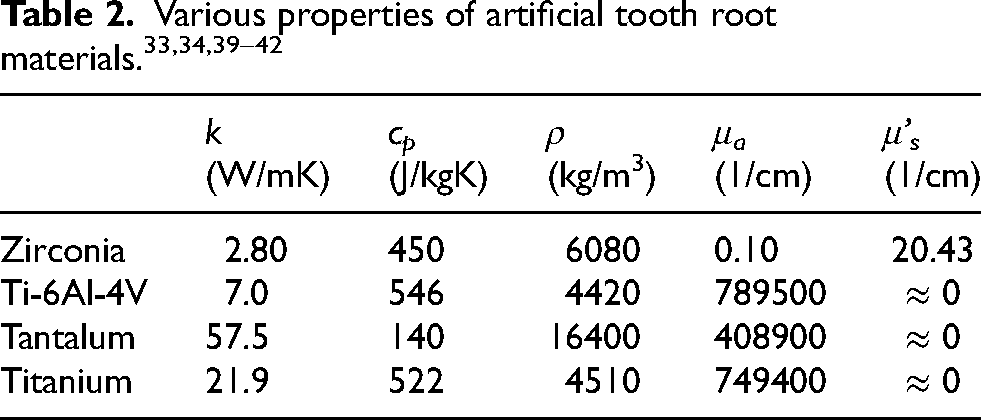
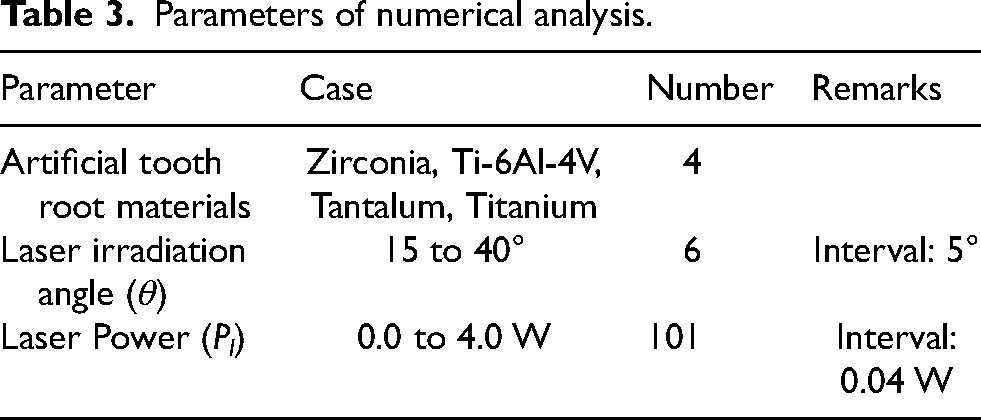
The numerical analysis was performed by varying the irradiation angle and laser power for the different artificial tooth root materials listed in Table 2. A total of 2424 numerical simulation cases were conducted, considering four types of artificial tooth roots—zirconia, Ti-6Al-4V, tantalum, and titanium—with laser irradiation angles ranging from 15° to 40°, and laser power ranging from 0 W to 4 W. A 630 nm wavelength laser was used, with a fixed laser radius of 0.2 mm and an irradiation time of 300 s. All numerical simulation conditions are summarized in Table 3.
Parameters of numerical analysis.
The verification of the numerical modeling was performed by calculating the error based on the mesh number and iteration count. The results converged with a mesh number of approximately 2.2 million or more, and the error was calculated to be less than 10−4% for iteration counts of 34 or more. This confirms the validity of the numerical modeling proposed in this study.
Results
Inflammation elimination range for various artificial tooth root materials and laser irradiation angle
The degree of inflammation death was confirmed for different artificial tooth root materials and laser irradiation angles. Figure 2 shows the temperature distribution and degree of tissue death for various artificial tooth root materials and laser irradiation angles, with the laser power fixed at 2 W. The results are presented for two cases with laser irradiation angles of 20° and 40°. The black line in the figure indicates the point where Ω equals 1. When analyzing the results, the degree of inflammation death varies for each artificial tooth root material. In addition, for large θ, the difference in the degree of eradication is clearly visible in the gingival and alveolar regions.

Temperature and Ω for various artificial tooth root materials and laser irradiation angle (Pl = 2 W, XZ plane (y = 0)).
Inflammation elimination range for various artificial tooth root materials and laser power
Figure 3 shows the temperature distribution and degree of tissue death for different artificial tooth root materials and laser power, with the irradiation angle of the laser fixed at 30°. The results are presented for two cases with laser powers of 1 W and 3 W. When analyzing the results, it appears that the variation in laser power with a fixed laser angle does not significantly affect the degree of death for different materials.
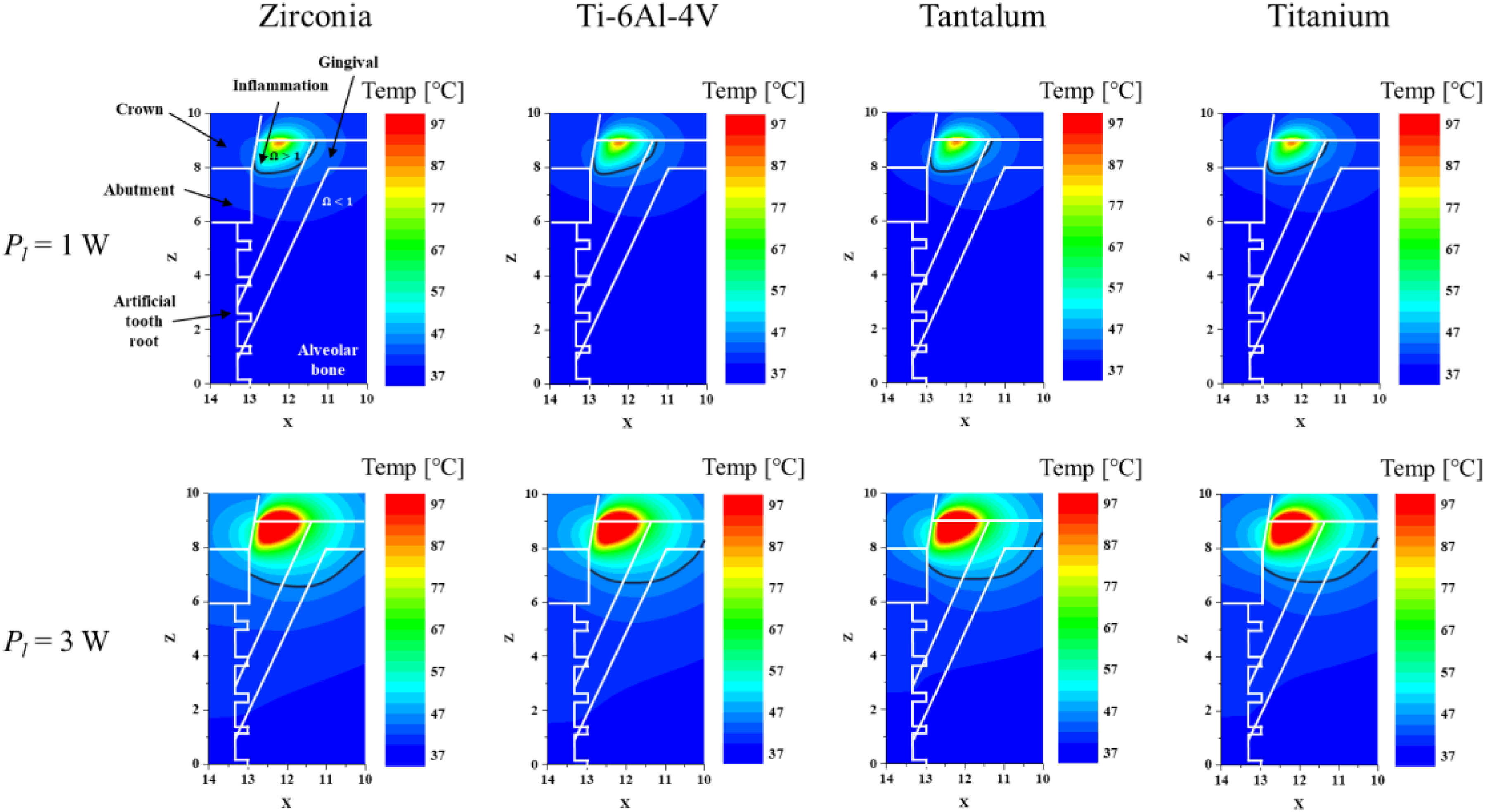
Temperature and Ω for various artificial tooth root materials and laser power (θ = 30°, XZ plane (y = 0)).
Elimination proportion for inflammation and normal tissue
Based on the calculated temperature distribution, the death rate of inflammation and surrounding normal tissue was determined and shown in Figures 4 and 5. Figure 4 shows the Arrhenius thermal damage ratio (ϕArrh), indicating the rate of inflammation death, as a function of laser irradiation angle and power for four different artificial tooth root materials. As confirmed from the temperature distribution above, the degree of inflammation death is high in the order of zirconia, Ti-6Al-4V, titanium, and tantalum. Furthermore, the results showed that the rate of death increased for all four materials as the laser irradiation angle approached vertical.
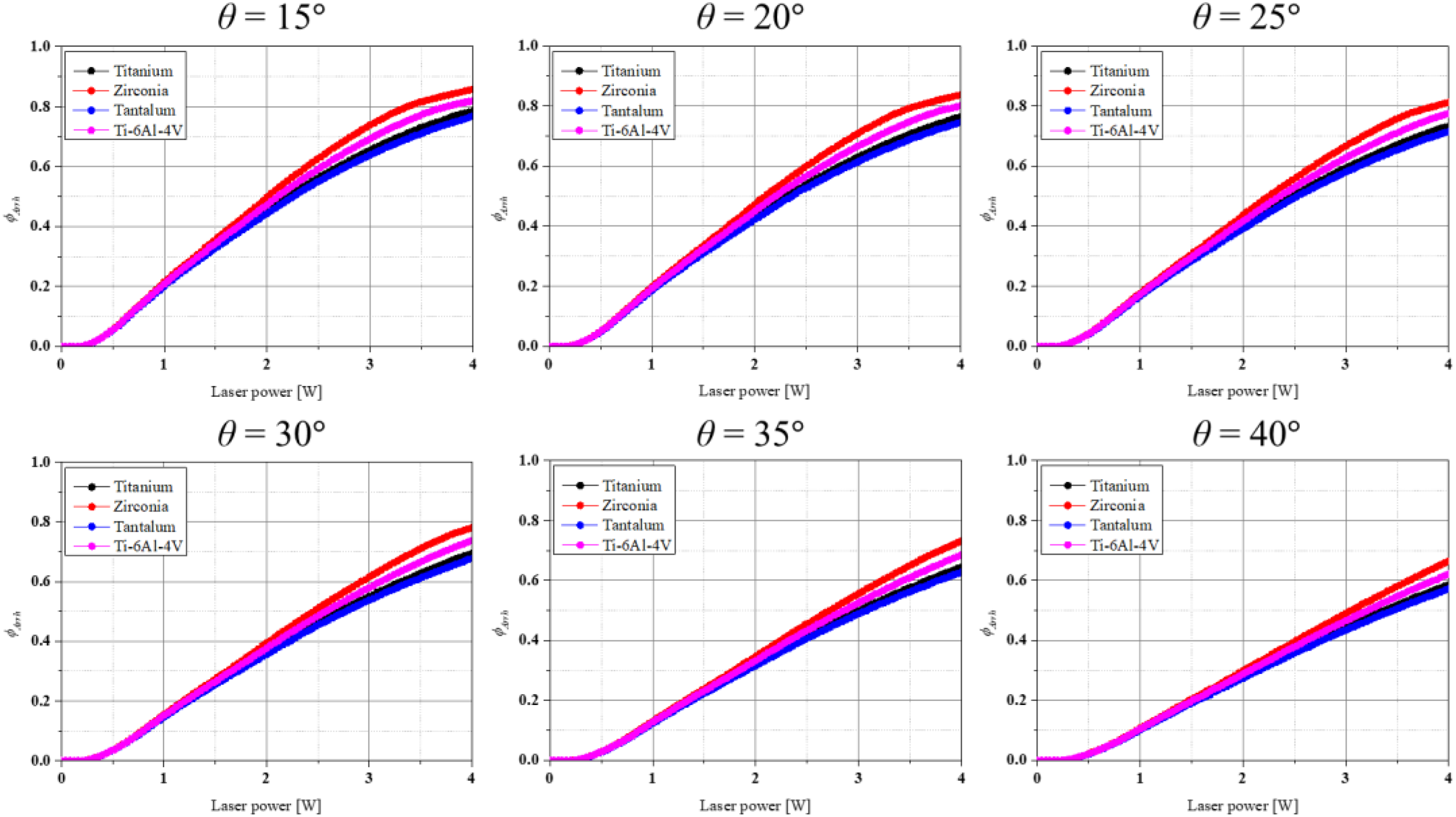
Arrhenius thermal damage ratio for various artificial tooth root materials at each irradiation angle and laser power.
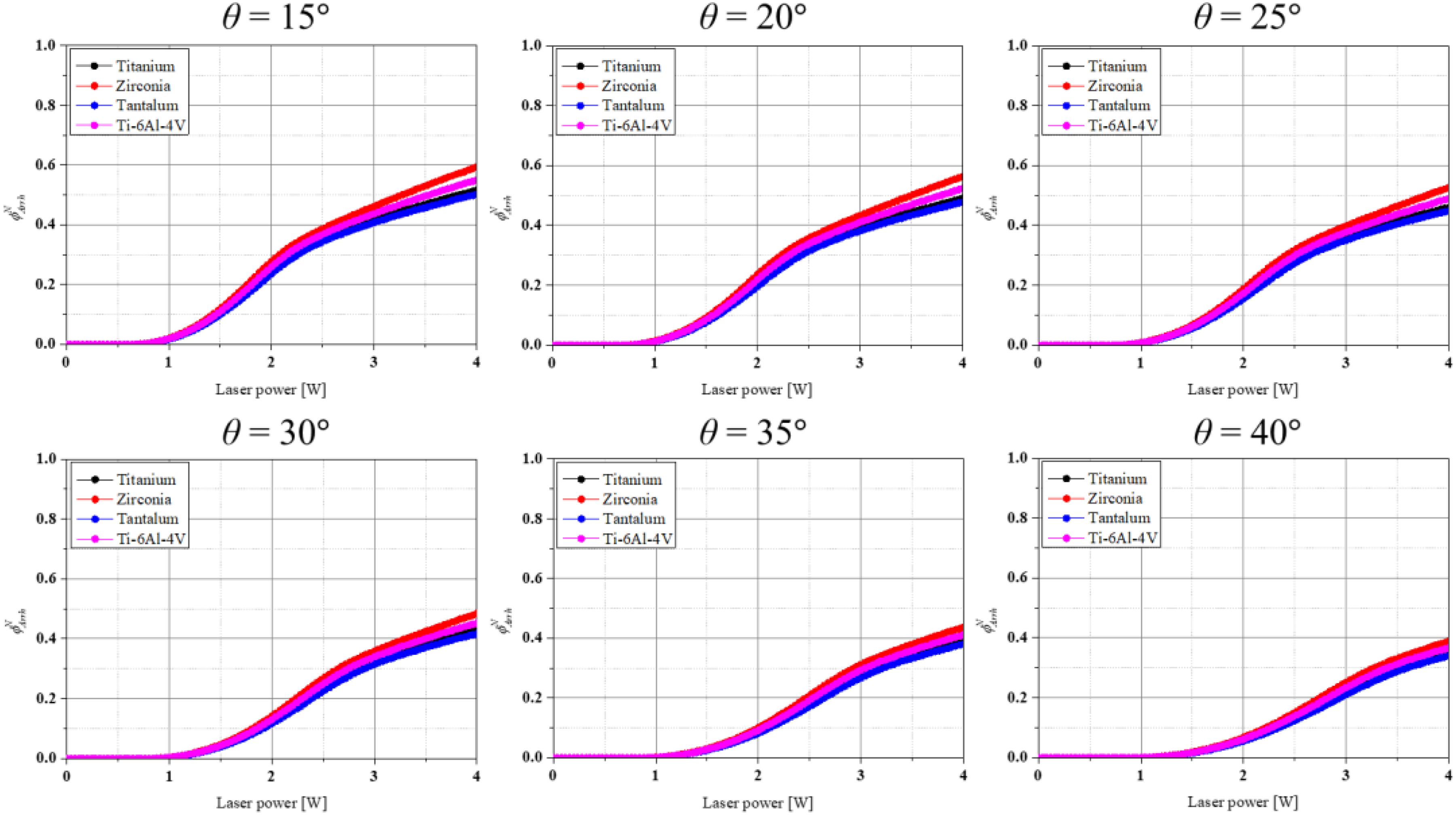
Normal tissue Arrhenius thermal damage ratio for various artificial tooth root materials at each irradiation angle and laser power.
Discussion
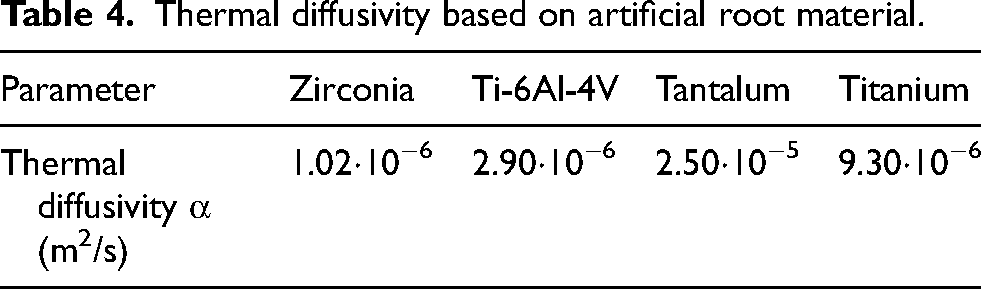
As shown in Figures 2 and 3, the degree of inflammation death varied for each artificial tooth root material, even under the same treatment conditions. The overall treatment trend indicated that the effectiveness was highest for zirconia, followed by Ti-6Al-4V, titanium, and tantalum from the perspective of artificial tooth root material. This is presumably closely related to the thermal diffusivity of each material. Thermal diffusivity is calculated as the ratio of the thermal conductivity of a medium to its heat capacity (the product of its density and specific heat) (Equation (7)), and it is a physical property that characterizes how quickly a substance responds to a change in temperature.
Table 4 shows thermal diffusivity for each artificial tooth root material. When the thermal diffusivity is high, heat transfer occurs quickly; when it is low, heat transfer occurs slowly. Calculating the thermal diffusivity for each material shows that tantalum has the highest and zirconia has the lowest thermal diffusivity. This indicates that tantalum allows the energy transferred to the artificial tooth root to dissipate relatively quickly, preventing the temperature rise in inflammation.
Thermal diffusivity based on artificial root material.
In terms of laser irradiation angle, it was found that the treatment effect improves as the irradiation angle decreases, i.e., as it becomes closer to vertical. This is because even if the same Pl is applied, the energy absorbed per unit area varies depending on θ, and the direction of energy penetration also varies. As θ increases, i.e., becomes closer to horizontal, the amount of energy absorbed by the inflammation decreases because the energy is transmitted more in the direction of the implant rather than the inflammation.
This trend is also evident in ϕArrh and ϕNArrh, which calculate the death ratio of inflammation and surrounding normal tissue, respectively (Figure 4 and 5). As mentioned earlier, the highest percentage of inflammation death was observed when zirconia was used as the artificial tooth root material, and the lowest when tantalum was used. However, the death rate of normal tissue followed the same trend. This is because inducing death in the inflammation requires a high internal temperature, which also raises the temperature of the surrounding normal tissue due to heat transfer. Therefore, conditions that maximize the inflammation death by applying high laser power will also increase the damage to the surrounding normal tissue. Thus, appropriate treatment conditions should be used to maximize inflammation death while minimizing damage to the surrounding normal tissue. From this perspective, calculating the ratio of ϕArrh to ϕNArrh suggests that it is more beneficial to increase the laser angle, i.e., to irradiate in a more horizontal direction. However, since the primary goal of the treatment is to maximize inflammation's death, it is believed that the laser angle should be vertical if the treatment is to be performed at the risk of damaging normal tissue.
Conclusions
In this study, the influence of implant material on the temperature rise within the peri-implantitis was numerically analyzed in photothermal therapy for peri-implantitis removal. The Pennes bioheat equation was used to calculate the temperature distribution in the tissue, and the results were applied to the Arrhenius damage integral to determine the degree of tissue death. Additionally, the Arrhenius thermal damage ratio and normal tissue thermal damage ratio were calculated to quantitatively determine the death rate of inflammation and surrounding normal tissue.
As a result, in terms of artificial tooth root material, the overall treatment trend showed that zirconia was the most effective material, followed by Ti-6Al-4V, titanium, and tantalum. This is presumably associated with each material's thermal diffusivity. For the laser irradiation angle, treatment effectiveness has been shown to improve as the angle gets closer to vertical. This result can be verified more quantitatively by calculating ϕArrh and ϕNArrh. The results show death degree of inflammation and surrounding normal tissue, and it is beneficial from a therapeutic point of view to increase the laser power and decrease irradiation angle unconditionally if only inflammation is considered. However, this will also cause the death of surrounding normal tissue, so it is essential to apply the appropriate laser power and irradiation angle. This can be seen from the fact that at 4 W and a laser angle of 15 degrees vertically, about 85% of the inflammation is thermally damaged, but about 60% of the surrounding normal tissue is also damaged. However, since treatment is ultimately about eliminating inflammation, clinicians should consider increasing the death rate of inflammation at the risk of damaging normal tissue.
Footnotes
Nomenclature
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (NSIT) (No. NRF-2022R1A2C2012470).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.