
Abstract
Background
Although game-based exercises for injured patients are expected to reduce post-traumatic stress disorder (PTSD) and anxiety while improving neuromuscular function and enhancing isokinetic moments, there is a lack of research. Furthermore, it is not known whether there are gender differences in these variables.
Objective
To verify the effects of the interactive line game (ILG) on psychophysical conditions in knee injury patients. This study also aimed to observe changes in these variables based on gender.
Methods
A total of 54 patients, aged between 20 and 24 years, were included. They were randomly assigned to either control group (CON, n = 28) or game exercise group (GE, n = 26), with an equal gender ratio in both groups. The ILG for the GE was performed 3 days a week for 8 weeks.
Results
After 8 weeks of ILG, neuromuscular function scores tended to decrease in both genders in the CON, whereas they showed an improvement in both genders in the GE. In contrast to the changes observed in the CON, the peak torque (PT) of GE males showed a significant increase only in the right hamstring (p < 0.001), while no significant differences were found in other variables. Meanwhile, work per repetition (WR) improved in all regions for the GE male group, whereas in the GE female group, it showed a significant increase only in the right (p < 0.01) and left (p < 0.05) hamstrings. Notably, a significant reduction in total PTSD scores was observed in both males and females in the GE. However, for anxiety scores, a significant change was only evident in males (p < 0.001), although differences between groups were observed for females (p = 0.009).
Conclusions
This study indicates that a gamified protocol designed for patients with knee injuries could promote the development of isokinetic moments through the enhancement of neuromuscular function, thereby effectively helping to alleviate PTSD and anxiety. Specifically, it showed more pronounced results in WR compared to PT, with clearer statistical outcomes in males than in females.
Introduction
In the sports arena, damage to the knee joint is a significant sports injury, accounting for approximately 25% of all injuries to the human body. 1 The causes of knee injuries include activities such as cutting, pivoting, decelerating, jumping, and landing, which are frequently employed during exercise. 2 Injuries associated with the knee joint are reported to encompass the anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, meniscal tears, and complex joint injuries. 3
According to some studies, even patients who have successfully completed rehabilitation after an injury still experience high levels of stress and anxiety related to the risk of recurrence, and they tend to avoid movements similar to those performed before the injury.4,5 Scholars refer to this condition as post-injury stress or post-traumatic stress disorder (PTSD), noting that it can manifest not only as mental symptoms like anxiety, tension, or unease but also as physical or cognitive symptoms, potentially causing significant disruption to daily life. 4 A study reported that the estimated lifetime remission rate of PTSD is 92%, but the median time to remission was 14 years. 5 A diagnosis of PTSD is given when symptoms of acute stress disorder persist for more than one month. 6
Various studies have been conducted to facilitate the return to the sports field after injuries. 7 Rehabilitation of the damaged knee joint involves a combination of conservative, proprioceptive, neuromuscular, and/or isokinetic exercises to promote recovery. 8 Physical rehabilitation exercise is recognised for its positive impact on the nervous system, including the peripheral nervous system and neuromuscular junctions. 9 It has been shown to enhance recovery from peripheral nerve injuries or degenerative changes. 10 In particular, neuromuscular function exercises that focus on factors limiting strength, speed, and power performance during rehabilitation can promote adaptation to exercise training and have a positive impact on psychological deconditioning. 11 In addition, an isokinetic dynamometer allows to assess muscular function with an accommodating resistance, at a constant angular velocity, thereby enabling maximum force or moments production throughout a prescribed range of motion. 12 However, some reports suggest that traditional forms of rehabilitation exercises are time-consuming and may lead to decreased interest or motivation, 13 highlighting the need for improving a psychological response or adaptation. 14
Software developed as part of the recent gaming industry is considered a potential tool for enhancing psychological motivation and providing more effective rehabilitation exercise therapy when utilised effectively.15,16 Game-based rehabilitation exercise involves the use of video games or game simulations to stimulate the interest of patients for psychophysical rehabilitation, potentially generating greater motivation compared to traditional rehabilitation methods. 15 The isokinetic device also tracks advancements in musculoskeletal rehabilitation, promoting psychological stability and proactive engagement. 17 The isokinetic equipment includes a game-based protocol called ‘Interactive Line,’ which requires users to maintain an ‘M'-shaped line using an upper and lower ball as time progresses. This design not only provides psychological enjoyment but also a sense of achievement based on scores. 18 Specifically, when moving up the ‘M’ shape, active concentric muscle contraction is required, while moving down involves eccentric contraction, promoting neuromuscular development. The score increases when there are fewer deviations from the line. Although there are several similar game-based exercises integrated into isokinetic equipment, their utilisation remains limited. Moreover, it is not yet known how such exercises affect neuromuscular development in patients who have experienced the injuries, as well as their psychological conditions. Therefore, this study aimed to investigate how the application of Interactive Line Game (ILG) software using an isokinetic machine affects the neuromuscular function and isokinetic moment of patients with knee joint injuries, and how these effects influence PTSD and anxiety levels. Additionally, this study sought to observe changes in these variables based on gender and to examine whether there are any gender differences.
Methods
Participants
The participants in the study were aged between 20 and 24 years, with a stature range of 155–185 cm and a weight range of 53.6–91.2 kg. The sex ratio was evenly balanced between males and females. The target population was young adults, and they were grouped through a randomized sampling method. The participants were included patients who had experienced meniscus tears, articular cartilage injuries, anterior cruciate ligament injuries, posterior cruciate ligament injuries, or patellar tendonitis and had fully recovered through non-surgical treatment. The cohort consisted solely of individuals without any bone injuries or degenerative diseases of the knee joint. Participants with musculoskeletal issues in other areas or specific medical conditions were excluded. Participants were also excluded (1) if they had lower and/or upper extremity injuries that had limited their physical activity level in the past 6-mon, (2) if they had a diagnosis interfering with a proper execution of the test, or (3) if they used medication that could influence their ability to deliver strength. The sample size was determined using the G*Power programme for a basic research design of a two-way repeated measures ANOVA. Parameters used were effect size f (V) = 0.25, α error probability = 0.05, β error probability = 0.95, number of groups = 2 (control (CON) group vs. game exercise (GE) group), and number of measurements = 2 (pre vs. post). The calculated sample size was determined to be a minimum of 54 participants. Considering an approximate dropout rate of 20% in the study, 19 63 participants were recruited. Following the research design, 30 participants were allocated to each of the two groups. Utilising a simple randomisation method based on the order of arrival (1:1), participants were assigned to two groups using a web-based randomiser. 20 Each participant selected a numbered ticket from a jar, and these numbers, ranging from 1 to 60, were inputted into the program as individual sets of 1. The program then randomly allocated participants into two distinct groups: the CON group and the GE group. Over the follow-up period, two individuals from the GE group dropped out, leading to a final analysis involving 54 individuals as shown in Figure 1. In the end, the CON group consisted of 14 males and 14 females, while the GE group included 13 males and 13 females. To prevent communication between the groups, participants were divided based on their community block. Interventions and measurements were scheduled with the CON group at 10:00 and the GE group at 14:00.
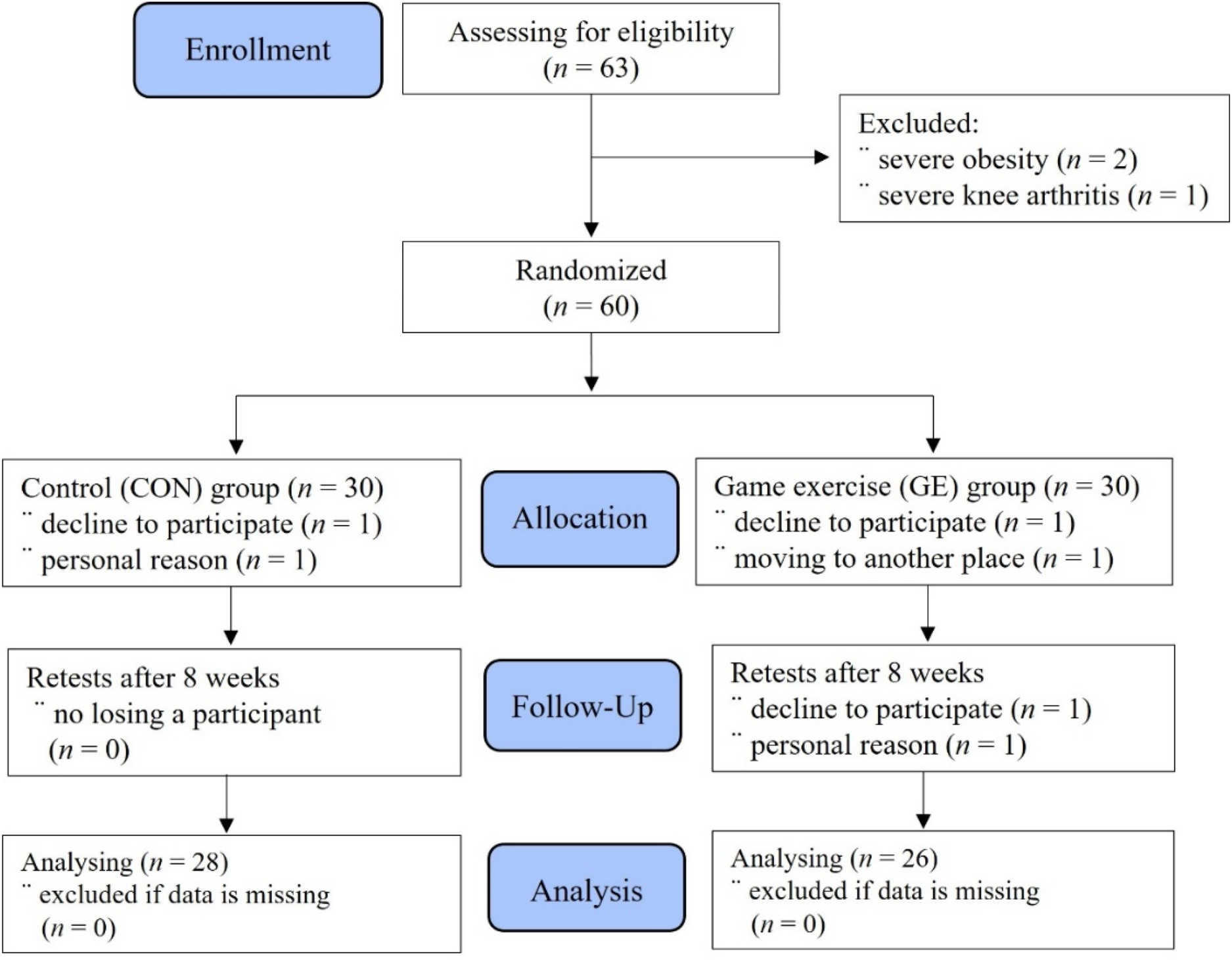
Allocation of participants (trials flow diagram using consolidated standards).
This research was a single-blind randomized controlled trial that aimed to investigate the effects of a gamified exercise on neuromuscular function including isokinetic moments, PTSD or anxiety levels in patients with knee injuries. To assess the impact of gamified exercise on psychophysiological conditions, the type of gamified exercise was standardised using an ILG within the isokinetic machine (HUMAC®/NORMTM Testing and Rehabilitation System, CSMi, Stoughton, MA, USA). The data was collected between March 13, 2024, and June 16, 2024. This study was approved by Hanseo University Institutional Review Board for Human (HS23-11-23-1). Prior to the study, all participants were informed about the experimental procedures and the purpose of the research, and informed consent was obtained from them. This research has also been registered on ClinicalTrials.gov (KCT0009153). The GE group followed the ILG three days a week (on Mondays, Wednesdays, and Fridays) for 8 weeks. While the GE group was participated in the ILG program, the CON group sat on mats and attended health education lectures on the same days.
Measurements
Body composition and controlled variables measures
Body composition was assessed using a bioelectrical impedance analysis method with an analyzer (Inbody 770, Biospace, Seoul, Korea) to obtain the participants’ physical characteristics after manually measuring their statures. The daily diet was tracked using CAN-Pro 5.0 (Korean Nutrition Society, Seoul, Korea, 2023), and physical activity levels were monitored with the International Physical Activity Questionnaire. 21 Both variables were logged daily on a computer and averaged at the end of the month. 22
Neuromuscular function and intervention program using an ILG
The program utilized in this study was the gamified Interactive Line, which follows a protocol involving isokinetic contractions (Figure 2A) as participants attempt to keep two balls aligned with a target point, as shown in Figure 2B. In the position mode, the location of the balls corresponded to the position of the limb. In the isokinetic contraction mode, the balls’ positions represented torque generation, with the X-axis displaying the percentage of maximum voluntary contraction. The green ball indicated that the participant had reached the target, while the red ball signified a failure to reach the target. The score dial represented the percentage of time the participant reached the target during both the concentric and eccentric phases of the exercise, and the time was displayed in MM: SS format. In this study, participants’ muscle contraction accuracy scores for both legs, recorded while performing the ILG, were stored on a computer each time and then averaged monthly for analysis and presentation of results.
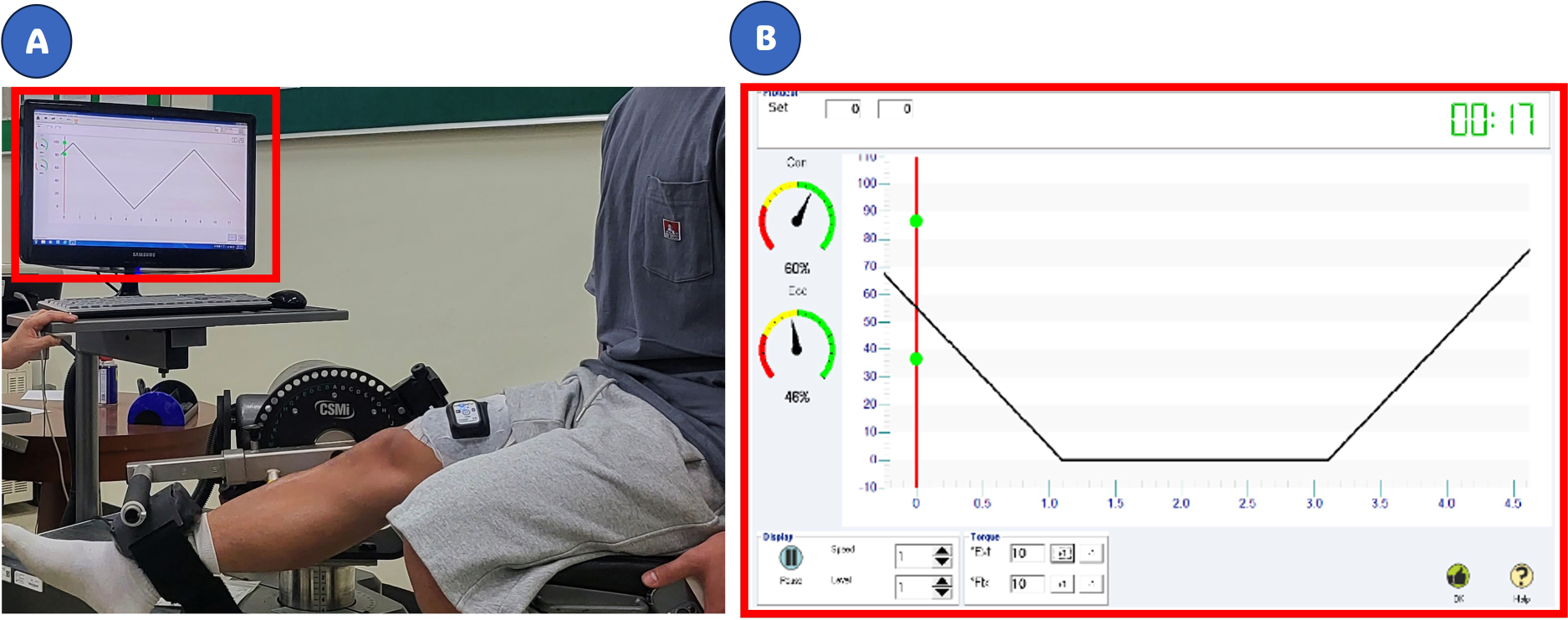
Interactive line execution actions (A) and program screens (B).
The intensity was set to 10 Nm for concentric contractions and 13 Nm for eccentric contractions, with each session lasting 30-s to 1-min as specified in the operating manual. Participants were instructed to stop the exercise if they experienced any discomfort or pain in their knee joints. Throughout the ILG, all participants received visual feedback from the system monitor, and the researcher encouraged them to keep two green balls within the line as much as possible. For the first 4 weeks, the ILG consisted of 10 sets of 30-s of exercise followed by 1-min rest. From the 5th to the 8th week, participants were advised to perform 10 sets with 1-min of exercise followed by 1-min rest.
All subjects participated in a stretching and warm-up program prior to the test. They performed at least four submaximal practice repetitions at a test speed, involving movement from full knee extension to full knee flexion. Each participant was seated in the equipment's adjustable chair, with the tested limb secured by a Velcro strap over the thigh, and the knee joint positioned at a 90° flexion. Testing was conducted while seated, with the apparatus set up uniformly across participants. The participant's leg was statically weighed to account for gravity compensation in the test data. All participants were tested at 60°/s concentrically, following recommendations by many researchers.12,23–25 Testing began on the uninvolved side to reduce anxiety, then proceeded to the involved side. All tests were overseen by a single trained researcher. The outcome measures were peak torque (PT) and work per repetition (WR). The identical test protocol was executed on two distinct occasions, at baseline and Week 8.
Post-traumatic stress measures
This study utilized the shorten version of the PTSD Checklist for DSM-5 (PCL-5) to investigate PTSD in patients with knee injuries. 26 The survey consisted of four items, and all participants completed the survey at the same time points both before and after the experiment. The 1st question asked, “Do you suddenly feel or act as if the stressful experience is happening again (as if you are actually reliving it)?” The 2nd question was, “Do you avoid external reminders of the stressful experience (such as people, places, conversations, activities, objects, or situations)?” The 3rd question asked, “Do you feel distant or disconnected from other people?” The 4th question was, “Do you exhibit irritable behaviour, angry outbursts, or act aggressively?” Each item was rated on a Likert scale, where a score of ‘0’ indicated no PTSD symptoms and a score of ‘4’ indicated severe symptoms. 25 The reliability coefficient, as measured by Cronbach's alpha, was 0.901, indicating satisfactory internal consistency.
Anxiety measures
Anxiety is a sensation characterised by fear, apprehension, and discomfort regarding the injury. In this study, an adapted version of research utilizing the visual analogue scale (VAS) was employed to assess the level of anxiety. 27 Each participant was instructed to indicate their level of self-perceived state in response to the researcher's questions. They were asked to assess their “Concerns about potential anxiety before participating in an isokinetic interactive game” using a 10-cm bipolar rating scale before and after the experiment. Participants who felt no anxiety before and after the ILG could mark “V” close to “0” on the scale, while those experiencing extreme anxiety could mark close to “10”. The reliability of the questionnaire was measured using Cronbach's α to determine internal consistency, with the anxiety scale showing a Cronbach's α coefficient of 0.870.
Statistical analysis
In this study, data was statistical analyzed with the SPSS statistical processing program (SPSS 23.0/PC, IBM, Armonk, NY, USA). In addition, GraphPad Prism (ver. 10.3, Boston, MA, USA) was employed for the creation of graphical representations. All data are presented as mean ± standard deviation (SD). The normality of demographic, anthropometric, and clinical measures was assessed using the Shapiro-Wilk test. Categorical variables, expressed as n (%), were compared using suitable statistical tests such as χ² or Fisher's exact test. Prior to the comprehensive analysis, baseline differences were evaluated by applying the Mann-Whitney U test to the pre-levels of variables. For normally distributed data, repeated measures (2 × 2) ANOVA was used for variable comparisons. In the case of non-normally distributed data, the non-parametric test was applied, with adjustments made for multiple comparisons. Detailed data analysis was conducted by calculating each period as delta (Δ)%. The effect size in this study was computed using Rhea's formula. 28 The effect sizes were categorised for untrained individuals as follows: < 0.50 (trivial), 0.5–1.25 (small), 1.25–1.9 (moderate), and 2.0 or higher (large). Statistical significance was set at p ≤ 0.05.
Results
Demographic and physical characteristics before the experiment
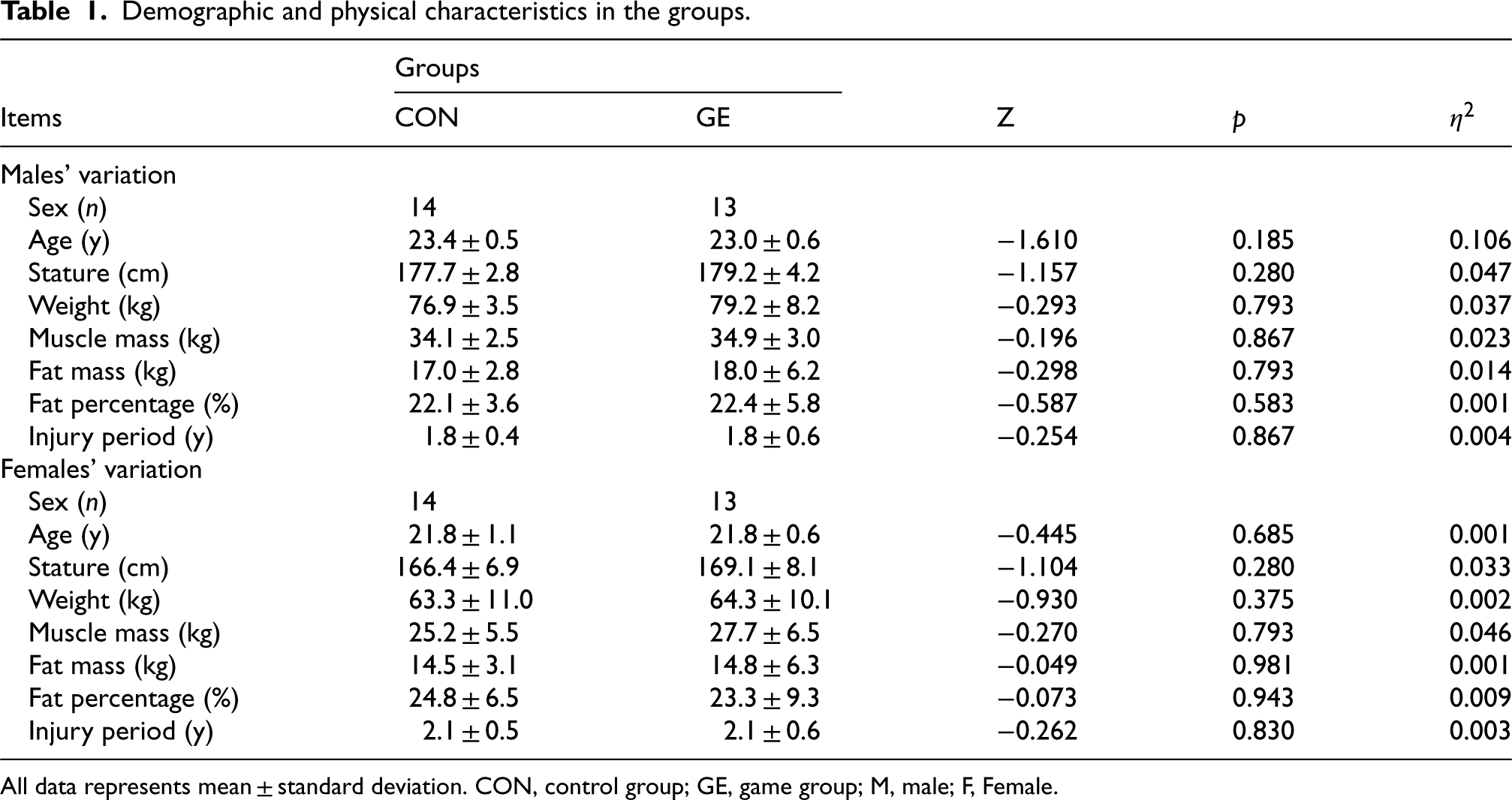
In the CON group, the ratio of females to males was evenly split at 50% each, and the GE group also had an equal distribution of females and males. As shown in Table 1, there were no significant differences between the two groups in terms of age, sex distribution, stature, or weight before the experiment. Additionally, there was no statistically significant difference in the injury duration between the CON group and the GE group. These results showed similar outcomes when comparing the variables of the CON group and the GE group separately for males and females. Meanwhile, in terms of injury history, there was a statistically significant difference between the overall male and female groups (Z = -1.971; p = 0.049). However, there was no significant difference between genders within the CON group (Z = -1.849; p = 0.164) and the GE group (Z = -0.989; p = 0.430).
Demographic and physical characteristics in the groups.
Demographic and physical characteristics in the groups.
All data represents mean ± standard deviation. CON, control group; GE, game group; M, male; F, Female.
After 4 weeks of the experiment, the calorie intake in the CON group was 2336.5 ± 222.1 kcal, and in the GE group, it was 2373.1 ± 210.4 kcal, with no significant difference (Z = -0.996, p = 0.319; η2 = 0.007). After 8 weeks, the calorie intake in the CON group was 2414.2 ± 183.9 kcal, and in the GE group, it was 2361.1 ± 202.4 kcal, again showing no significant difference (Z = -1.135; p = 0.257; η2 = 0.019). After 4 weeks of the experiment, the physical activity level in the CON group was 1545.1 ± 360.2 MET⋅min⋅week−1, and in the GE group, it was 1587.7 ± 390.1 MET⋅min⋅week−1, with no significant difference (Z = -0.348, p = 0.728; η2 = 0.003). After 8 weeks, the physical activity level in the CON group was 1516.6 ± 355.0 MET⋅min⋅week−1, and in the GE group, it was 1545.4 ± 396.7 MET⋅min⋅week−1, again showing no statistically significant difference (Z = -0.113; p = 0.910; η2 = 0.002).
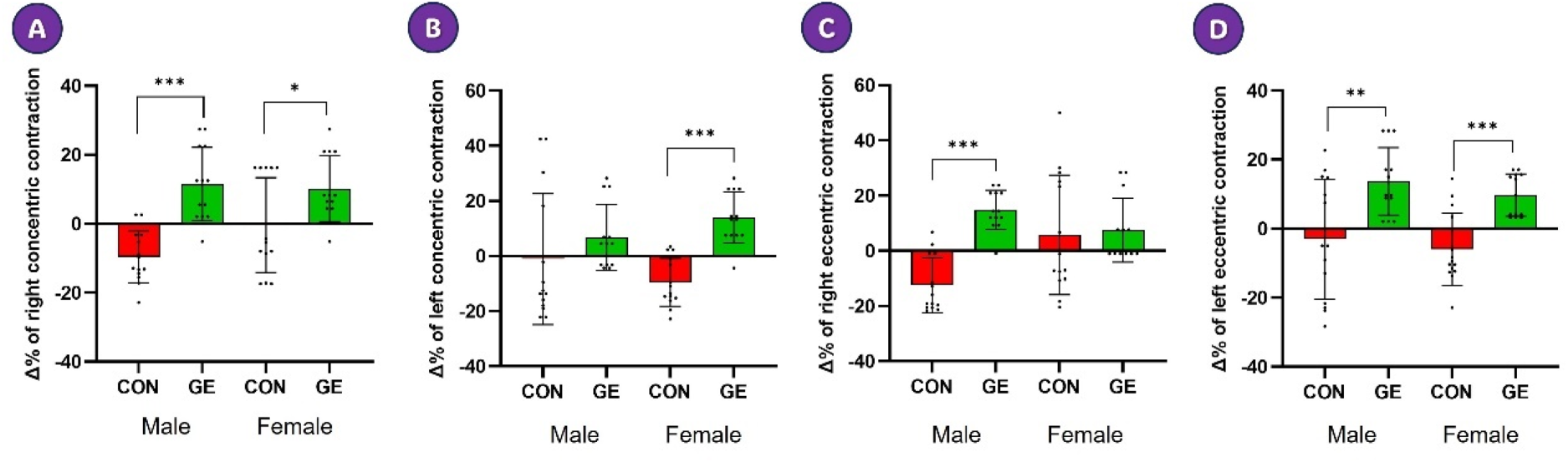
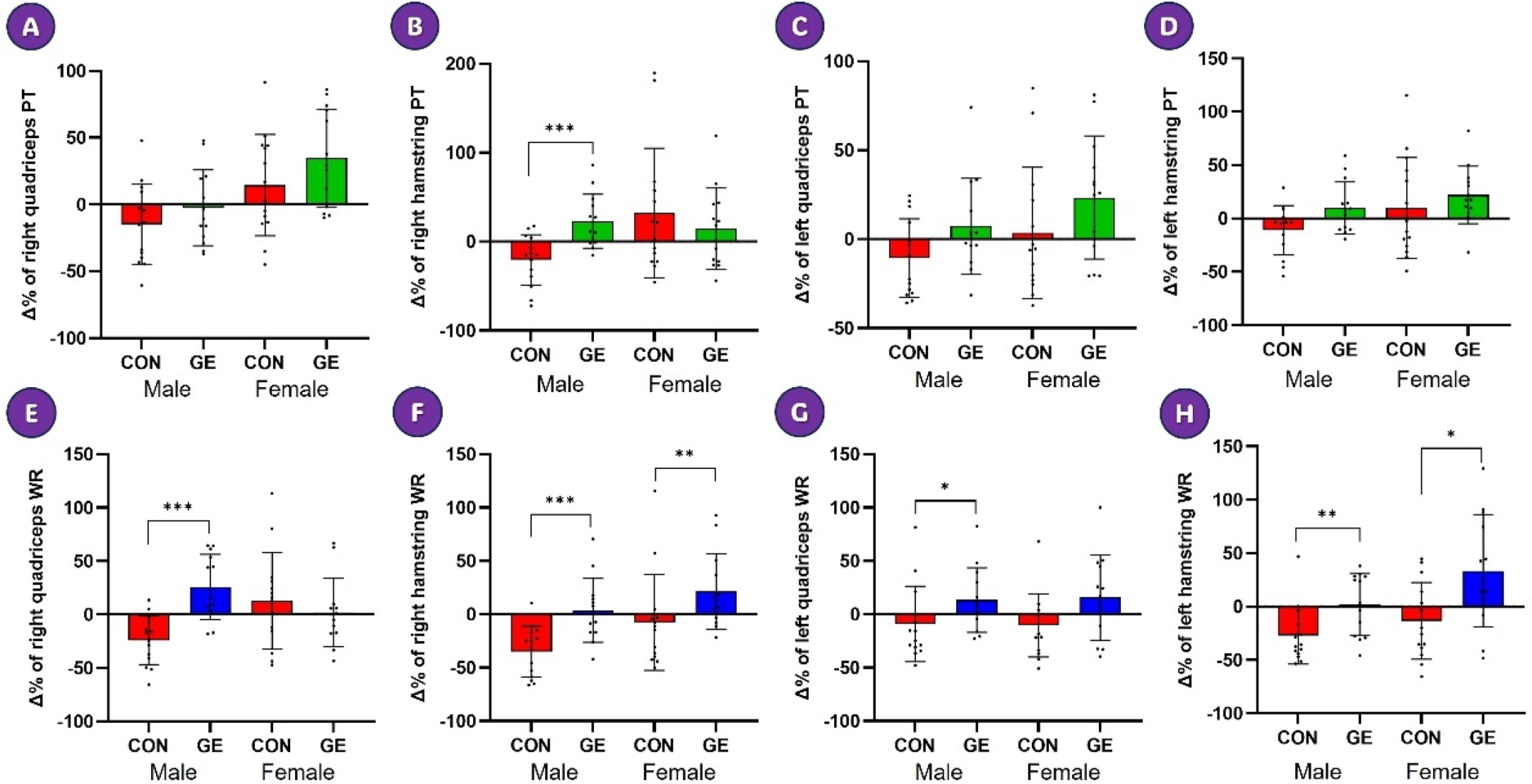
Differences in the percentage change of neuromuscular function scores. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001.
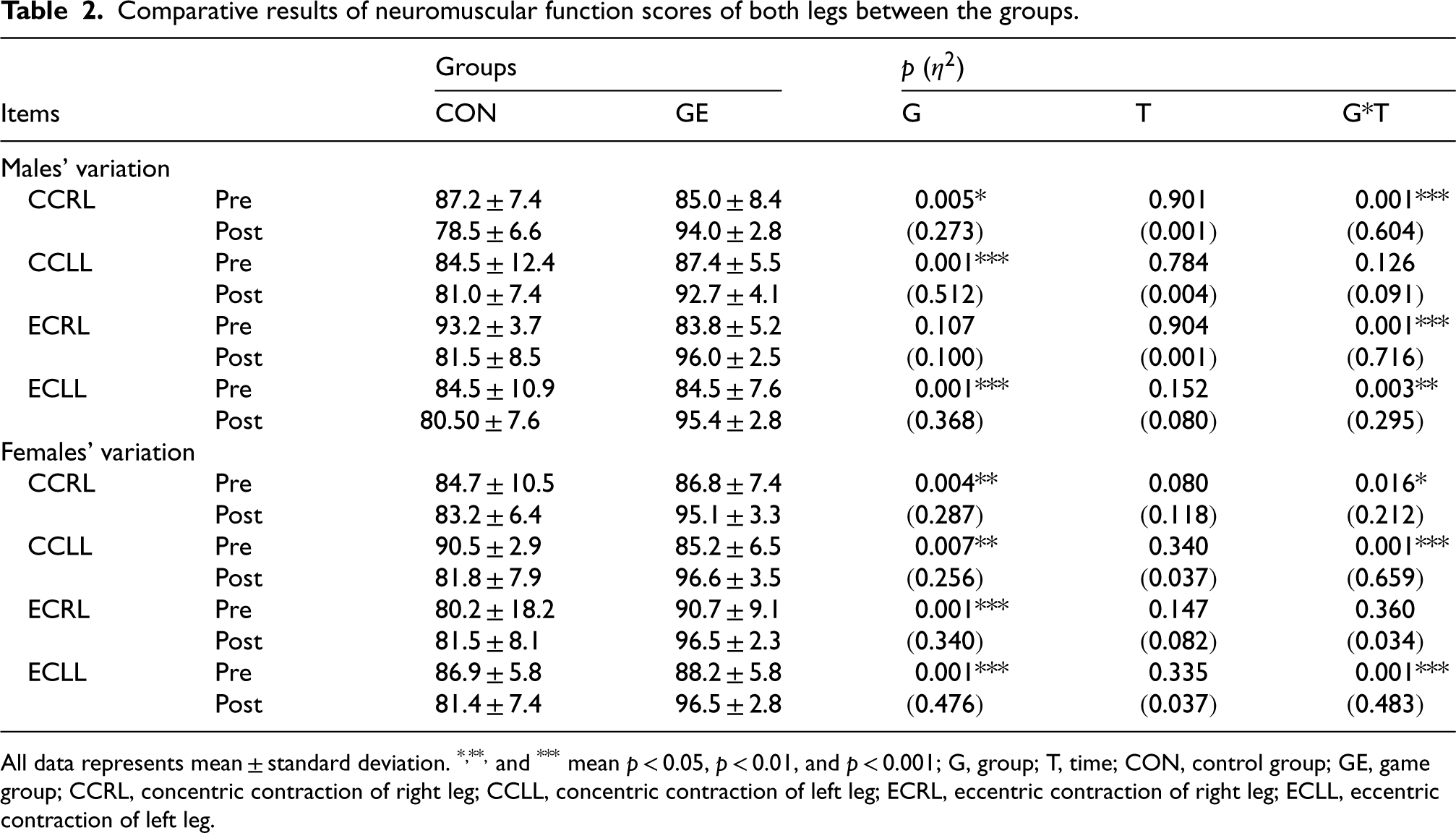
As shown in Table 2, in the male CON group, the accuracy score of right concentric contraction decreased (−9.6%), whereas the score in the male GE group increased (11.5%), showing a significant interaction effect (p < 0.001). Similarly, the score in the female CON group decreased (−0.4%), while the score in the female GE group increased (10.2%), also showing a significant interaction effect (p < 0.05). These results were similarly observed in the Δ% after the completion of the experiment (Figure 3A). In the male CON group, the accuracy score for left concentric contraction slightly declined (−1.1%), whereas it rose in the male GE group (6.7%), though without a significant interaction effect. However, in the female CON group, the score dropped (−9.5%), while it increased significantly in the female GE group (14.1%), showing a notable interaction effect. These results were also reflected in the Δ% change after the experiment (Figure 3B). In the male CON group, the accuracy score for right eccentric contraction dropped (−12.5%), whereas it rose in the male GE group (14.8%), showing a significant interaction effect. In contrast, the score in the female CON group declined (−5.8%), while it increased in the female GE group (7.5%), although this did not demonstrate a significant interaction effect. These findings were similarly reflected in the Δ% change after the experiment (Figure 3C). In the male CON group, the score for left eccentric contraction dropped (−3.0%), whereas it increased in the male GE group (13.9%), showing a significant interaction effect. Likewise, in the female CON group, the score declined (−5.9%), while it rose in the female GE group (9.6%), also demonstrating a significant interaction effect. These results were similarly observed in the Δ% change after the experiment (Figure 3D).
Comparative results of neuromuscular function scores of both legs between the groups.
Comparative results of neuromuscular function scores of both legs between the groups.
All data represents mean ± standard deviation. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001; G, group; T, time; CON, control group; GE, game group; CCRL, concentric contraction of right leg; CCLL, concentric contraction of left leg; ECRL, eccentric contraction of right leg; ECLL, eccentric contraction of left leg.
As shown in Table 3, in the male CON group, PT decreased (−14.7%), while there was no change in the male GE group. In contrast, in the female CON group, PT increased (14.4%), and it rose even further in the female GE group (34.9%), demonstrating a significant interaction effect. These results were similarly reflected in the Δ% change after the experiment (Figure 4A). In the male CON group, PT decreased (−20.7%), whereas it increased (22.7%) in the male GE group, indicating a significant interaction effect. Meanwhile, PT in the female CON and GE groups increased by 31.1% and 14.4%, respectively, showing no significant interaction effect. These findings were reflected in the Δ% change after the experiment (Figure 4B). PT decreased in the male CON group (−10.6%), while it increased in the male GE group (7.2%), indicating no significant interaction effect. In contrast, PT in the female CON group increased (3.4%) and rose even further in the female GE group (23.3%), demonstrating a significant interaction effect. These results were reflected in the Δ% change following the experiment (Figure 4C). In the male CON group, PT decreased (−11.1%), while it increased in the male GE group (9.9%), showing a significant interaction effect. Conversely, in the female CON group, PT increased (9.7%) and rose even further in the female GE group (22.1%), though without a significant interaction effect. These results were similarly reflected in the Δ% change following the experiment (Figure 4D).
Differences in the percentage change of isokinetic moments. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001.
Comparative results of isokinetic moments of both legs between the groups.
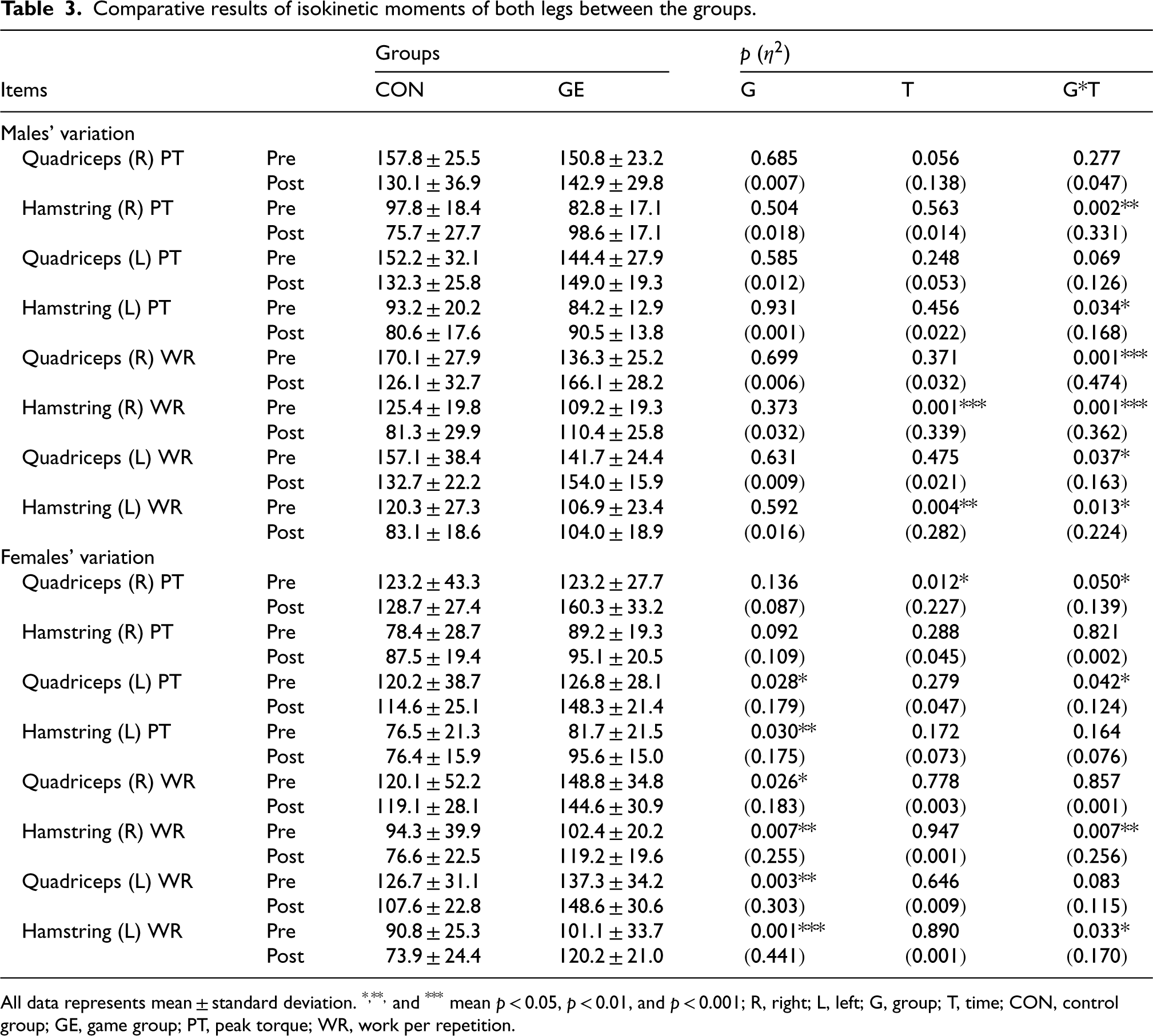
All data represents mean ± standard deviation. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001; R, right; L, left; G, group; T, time; CON, control group; GE, game group; PT, peak torque; WR, work per repetition.
As shown in Table 3, in the male CON group, WR decreased (−24.0%), whereas it increased in the male GE group (25.6%), indicating a significant interaction effect. In contrast, WR in the female CON group and GE group increased by 12.6% and 1.8%, respectively, demonstrating no significant interaction effect. These results were reflected in the Δ% change following the experiment (Figure 4E). In the male CON group, WR decreased markedly (−34.8%), whereas it increased slightly in the male GE group (3.7%), demonstrating a significant interaction effect. Similarly, in the female CON group, WR decreased (−7.7%), while it increased significantly in the female GE group (21.4%), indicating a significant interaction effect. These findings were also reflected in the Δ% change after the experiment (Figure 4F). In the male CON group, WR decreased (−9.1%), whereas it increased in the male GE group (13.2%), also indicating a significant interaction effect. In contrast, WR in the female CON group decreased by −10.2%, while it increased by 15.7% in the female GE group, though this did not demonstrate a significant interaction effect. These findings were similarly reflected in the Δ% change after the experiment (Figure 4G). In the male CON group, WR decreased considerably (−27.1%), whereas it increased slightly in the male GE group (2.0%), demonstrating a significant interaction effect. Similarly, in the female CON group, WR decreased by −13.4%, while it increased in the female GE group by 33.2%, indicating a significant interaction effect. These findings were also reflected in the Δ% change after the experiment (Figure 4H).
As shown in Table 4, in the male CON group, the PTSD1score rose by 27.4%, while it fell by −35.7% in the male GE group, indicating a significant interaction effect. In contrast, the female CON group experienced a decrease of −2.4%, while the female GE group saw a slight increase of 1.3%, though this did not demonstrate a significant interaction effect. These results were similarly reflected in the Δ% change following the experiment (Figure 5A). In the male CON group, the PTSD2 score rose by 61.9%, whereas it fell by −5.1% in the male GE group. Similarly, the female CON group experienced an increase of 14.3%, while the female GE group saw a slight decrease of −11.5%, though this did not demonstrate a significant interaction effect. These results were also reflected in the Δ% change following the experiment (Figure 5B). In the male CON group, the PTSD3 score rose by 28.5%, while it fell by −1.7% in the male GE group, also indicating a significant interaction effect. Similarly, the female CON group experienced an increase of 70.2%, while the female GE group saw a slight decrease of −11.5%, indicating a significant interaction effect. These findings were also reflected in the Δ% change following the experiment (Figure 5C). In the male CON group, the PTSD4 score rose by 53.5%, while it fell by −1.9% in the male GE group, indicating a significant interaction effect. Similarly, the female CON group experienced an increase of 82.1%, while the female GE group saw a slight decrease of −11.5%, indicating a significant interaction effect. These findings were also reflected in the Δ% change following the experiment (Figure 5D). Finally, in the male CON group, the PTSD sum score rose by 31.7%, whereas it fell by −15.7% in the male GE group, indicating a significant interaction effect. Similarly, the female CON group experienced an increase of 29.1%, while the female GE group saw a decrease of −14.8%, indicating a significant interaction effect. These findings were reflected in the Δ% change following the experiment. Meanwhile, in the male CON group, the anxiety score rose by 120.1%, while it fell by −50.0% in the male GE group, indicating a significant interaction effect. However, the female CON group experienced an increase of 35.7%, while the female GE group saw a slight decrease of −13.4%, indicating no significant interaction effect. These findings were similarly reflected in the Δ% change following the experiment (Figure 5F).
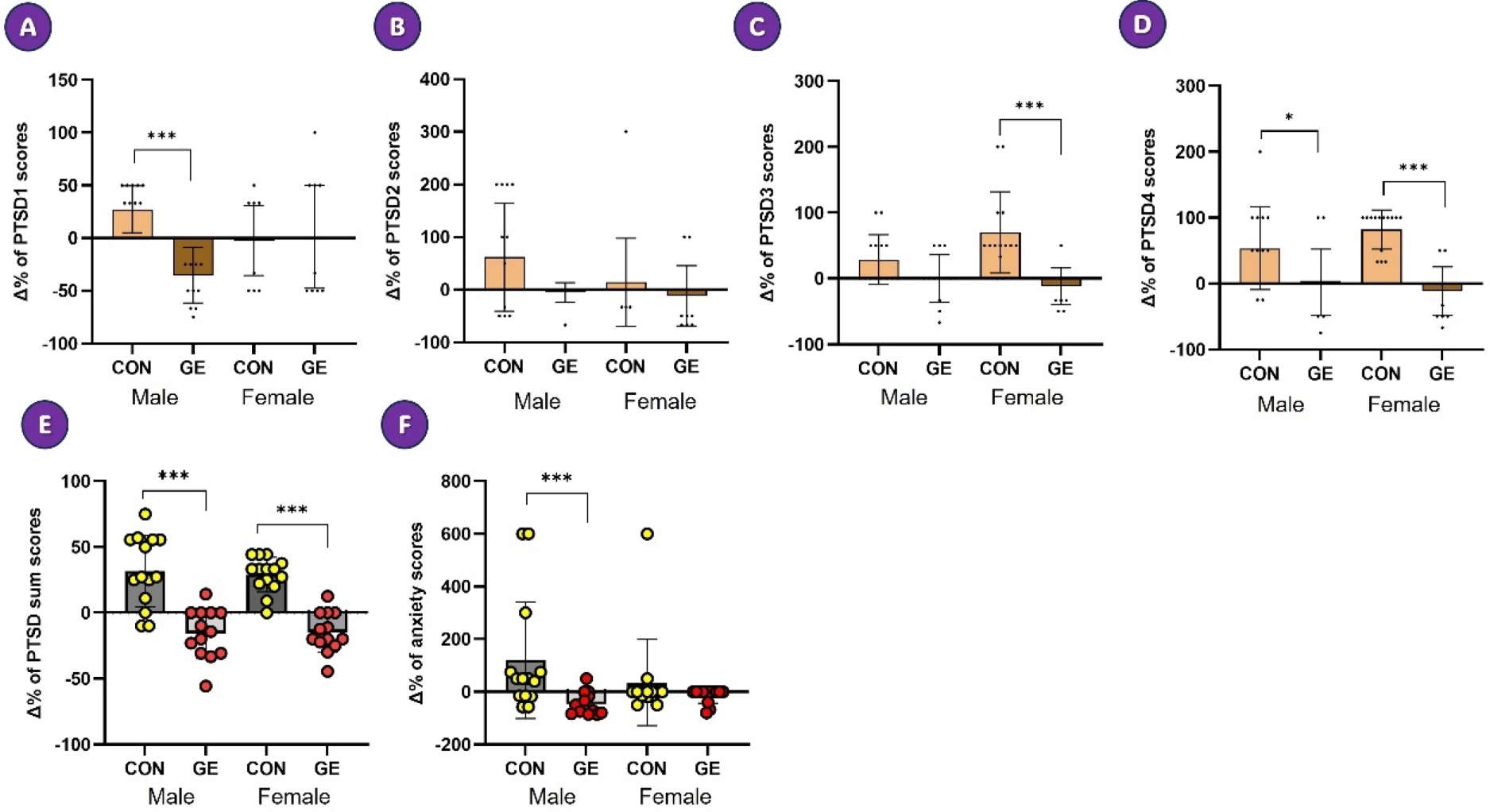
Differences in the percentage change of psychological conditioning factors. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001.
Comparative results of PTSD and anxiety levels between the groups.
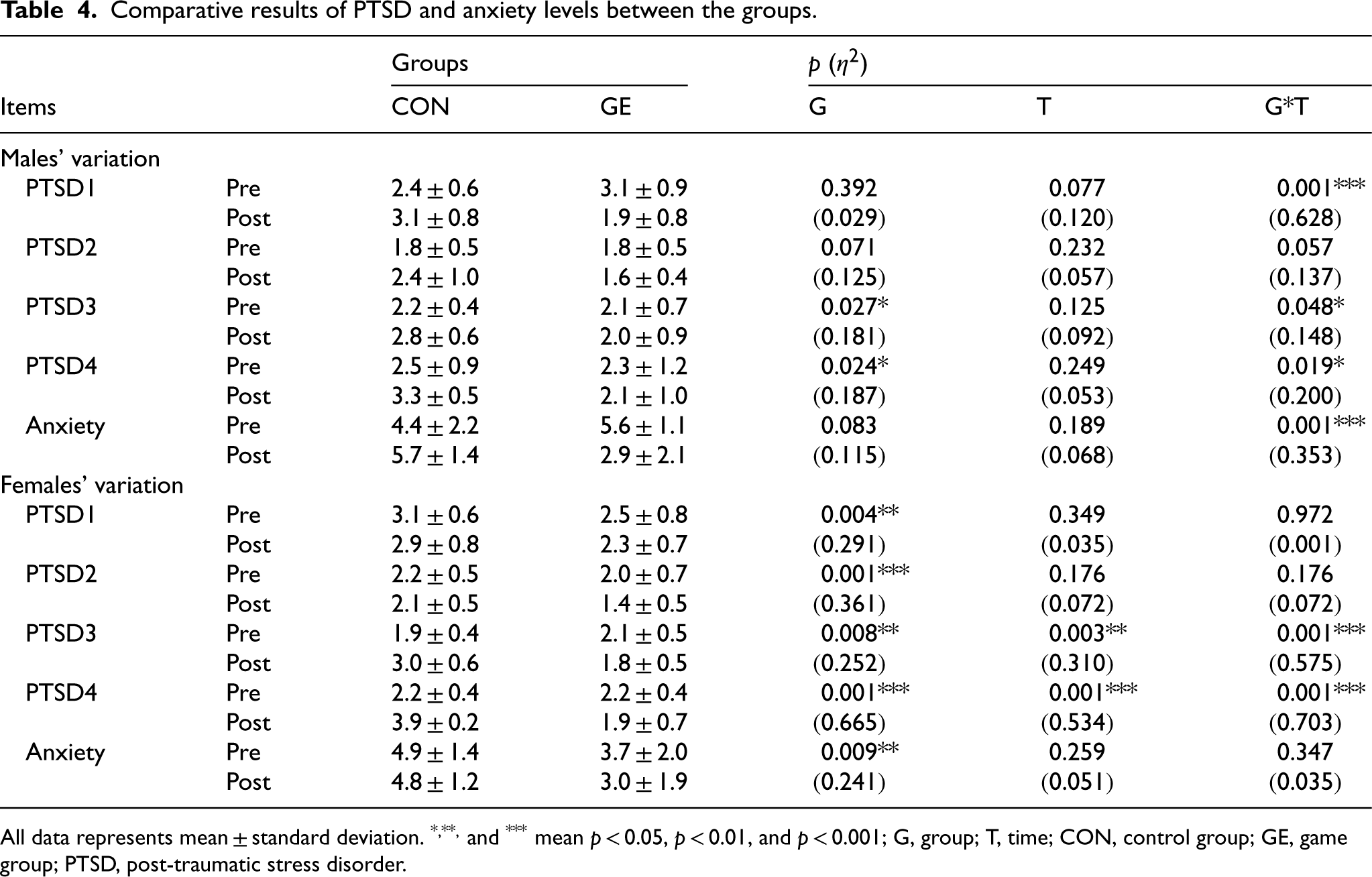
All data represents mean ± standard deviation. *, **, and *** mean p < 0.05, p < 0.01, and p < 0.001; G, group; T, time; CON, control group; GE, game group; PTSD, post-traumatic stress disorder.
The study found that after ILG exercises, which are game-based rehabilitation for patients with knee injuries, both neuromuscular function and isokinetic moments improved, alleviating of PTSD and anxiety levels. PTSD is a condition in which an individual experiences fear and ongoing distress through continuous re-experiencing of a traumatic event. After the event, individuals with PTSD expend energy trying to cope with and escape from the distress, negatively impacting their normal psychophysical functioning.4–6 In sports settings, PTSD related to knee injuries refers to the psychological and emotional distress experienced by individuals who have suffered traumatic events or injuries affecting the knee joint, leading them to avoid various activities.29,30 PTSD is often accompanied by symptoms of various physical and mental conditions, such as anxiety, sleep disorders, chronic pain, obesity, and metabolic syndrome.31–33 Especially, an anxiety can manifest in various ways and can have both immediate and long-term impacts on an individual's life.34–38
This study utilized a shortened version of the PTSD checklist to assess PTSD in knee injury patients, revealing that they exhibited mild to moderate PTSD levels, approximately 32% of the very severe symptom score (28 points) reported by Zuromski et al. 26 Meanwhile, in this study, the pre-experiment anxiety scores measured by the modified VAS were in the high 4.0 range, accounting for approximately 46% to 48% of the very severe level (10 points). It can be interpreted that the participants in this study had mild to moderate levels of PTSD and anxiety. In general, patients who have suffered knee injuries tend to experience psychological setbacks, which can lead to a decline in basic motor function and daily activities. This instinct to avoid movement can result in neurological deterioration and muscle atrophy.35,36 To the best of our knowledge, appropriate exercise rehabilitation therapy that emphasises psychologically comfortable and active elements is necessary to minimise psychological side effects resulting from such injuries. For this purpose, we initiated a study under the hypothesis that applying game-based rehabilitation tools, which are psychologically approachable, to patients with knee disorders could improve neuromuscular function as well as alleviate PTSD and anxiety.
The ILG used in this study involves positioning two green points along a specific line over time, serving as a tool to assess proprioceptive neuromuscular function and indicate whether muscle function is adequate. Prior to the experiment, participants’ knee joint function was assessed using this tool, with most scoring in the high 80 s. The PT and WR of the knee joint also showed lower results. These results suggest that the previously mentioned knee injury experiences lead to not only psychological distress but also physical decline,31,36 resulting in restricted neuromuscular activity and decreased muscular function. Meanwhile, the ILG performed in this study was applied to patients with knee joint issues and produced highly positive results both physically and psychologically. This is regarded as the neuromuscular system's ability to functionally control and drive movement through sensory feedback, reflex activities, central motor drive, muscle recruitment patterns, excitation-contraction coupling of muscles, and the proper integration, coordination, and utilization of energy.39,40
Neuromuscular weakness in the quadriceps and hamstring is commonly recognized as a major problem in cases of knee injuries, with affected individuals often showing a 20–40% reduction compared to healthy people.27,41 Conversely, if the root causes of these weaknesses are identified and addressed, 27 it could lead to neuromuscular recovery, thereby reducing the psychological setbacks. In this study, the ILG intervention used to enhance neuromuscular function resulted in increased concentric and eccentric contraction scores for both legs in the GE group after 8 weeks, whereas the scores in the CON group either decreased or showed no change. Specifically, the scores for neuromuscular function generally showed no significant differences between genders; however, the scores observed in the male group during left leg concentric contractions and those in the female group during right leg eccentric contractions exhibited some variability. Despite this variation, the statistical significance after the experiment was interpreted as not being present. In terms of the developmental aspects of neuromuscular function, it can be inferred that various factors, such as injury history and the timing of the initiation of rehabilitation programmes after injury, may have influenced the differences observed between genders. On the other hand, it was confirmed that the development of neuromuscular function simultaneously improved isokinetic moments in the GE group using ILG. Specifically, the PT and WR derived from the right and left legs significantly decreased in the CON group, which did not perform ILG, while they significantly improved in the GE group, allowing for the observation of statistical differences between the groups. However, in terms of isokinetic moment characteristics, the ILG used in this study showed more pronounced results in WR compared to PT, and it exhibited clearer statistical outcomes in males compared to females. Ultimately, the development of neuromuscular function and the improvement of isokinetic moments through ILG were observed to reduce PTSD and anxiety. Notably, when examining the total PTSD scores, a significant reduction effect was evident in both males and females. However, regarding the anxiety scores, a significant change was only observed in the male group. This discrepancy is considered to be influenced by the previously mentioned differences in injury duration between males and females. In addition, these findings appear to be somewhat consistent with the report by McLean and colleagues, 43 which stated that anxiety disorders were associated with a greater illness burden in women than in men. Indeed, PTSD or anxiety is frequently encountered and is characterized by severe debilitation, 29 with a low rate of successful treatment outcomes. 42 However, it is also a widely accepted view that psychological disorders can lead to faster physical responses and adaptations when interventions incorporate elements that are friendly and somewhat engaging. In this context, Payne et al. 44 emphasised the importance of considering instinctive and physical -based protective responses when addressing stress and trauma, highlighting that body-based approaches can positively influence proprioception and motor sensations, aiding in the recovery of the central nervous system. These research findings suggest that rehabilitation programs that target somatic function and incorporate psychological activation may be effective in overcoming PTSD or anxiety related to musculoskeletal injuries. Based on previous research findings and the results of this study, it can be inferred that a gamified protocol designed for patients with knee injuries could promote the development of isokinetic moments through the enhancement of neuromuscular function, thereby effectively helping to alleviate PTSD and anxiety. However, it is important to acknowledge the limitations of our research. First, the sample size was relatively small. Second, while there are various types of gamified exercise programs aimed at improving a neuromuscular function, this study focused on a specific ILG protocol. Given these limitations, further research is recommended to explore the effects of different types of gamified exercise protocols with a larger and more diverse participant pool.
Conclusions
This study indicates that a gamified protocol designed for patients with knee injuries could promote the development of isokinetic moments through the enhancement of neuromuscular function, thereby effectively helping to alleviate PTSD and anxiety. Specifically, it showed more pronounced results in WR compared to PT, with clearer statistical outcomes in males than in females.
Footnotes
Acknowledgements
We gratefully acknowledge all the participants who took part in this study and their support.
Author contributions
CONCEPTION: Yong-Seok Jee; Dong-Hyun Yoo
PERFORMANCE OF WORK: Yong-Seok Jee; Dong-Hyun Yoo; Sang-Geun Jo; Jaehyun Yoo
INTERPRETATION OR ANALYSIS OF DATA: Yong-Seok Jee; Jaehyun Yoo
PREPARATION OF THE MANUSCRIPT: Yong-Seok Jee; Dong-Hyun Yoo; Sang-Geun Jo
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Yong-Seok Jee; Jaehyun Yoo
SUPERVISION: Yong-Seok Jee
Funding
This research was not supported by any external agency.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.