
Abstract
Background
Repair for total Achilles tendon ruptures is sometimes delayed, despite the recommendation for early repair.
Objective
To investigate patient recovery scores, and ankle strength and function according to the timing of Achilles tendon rupture repair.
Methods
We conducted a retrospective analysis by categorizing repair: emergency (ER, n = 38), late (LR, n = 16), and very late (VLR, n = 13). Patients were evaluated based on the Achilles Tendon Total Rupture Score (ATRS), dorsiflexion range of motion, ankle strength, hop tests, and balance.
Results
All groups showed consistent improvement in the ATRS, heel-raise, plantarflexion strength, hop tests, and balance up to 6 and 9 months post-surgery. At 3 months, the ER and LR groups had significantly better values in the ATRS, heel raise, plantarflexion strength, and single-hop test compared with the VLR group (p < 0.05); by 12 months, there were no significant between-group differences (p > 0.05). The ER group outperformed the VLR group in the crossover hop test, and in posteromedial and lateral balance at 12 months (p < 0.05).
Conclusion
Twelve months after Achilles tendon rupture repair, VLR induced similar improvement in the ATRS, and ankle strength and function compared to ER and LR. Therefore, despite being very late, the repair was significantly effective in improving ankle function.
Introduction
The Achilles tendon, among the thickest tendons in the human body, functions to transmit strength from the gastrocnemius and soleus muscles to the foot through the calcaneus, enabling ankle movements for activities.1,2 Despite its strength, the risk of Achilles tendon rupture increases in individuals engaging in vigorous physical activities. In the United States, the incidence is 2.5 per 100,000 person-years, notably higher in young men at 5.6 per 100,000 person-years. 3 Injuries typically occur during sports or recreational activities, although can also result from falls or slips. The mechanism of Achilles tendon rupture involves high-energy transmission from the calf muscles during activities such as running, jumping, or sudden changes in direction, exceeding the tendon's capacity to withstand stretching forces, leading to rupture. 4
The primary treatment for total Achilles tendon rupture is surgical repair, although conservative therapy is advocated by some specialists. 5 However, experts generally recommend performing surgery as soon as possible for Achilles tendon rupture to achieve the ultimate goal of restoring Achilles and lower extremity function through reattachment and facilitating a return to pre-injury activity levels. 6 Especially, for young, active individuals who participate in sports for leisure, surgery is typically recommended due to advantages such as improved motor function recovery and reduced re-rupture rates, as shown in a meta-analysis. 7
The timing of surgical intervention remains controversial. Ideally, surgery should be performed promptly following injury, preferably within 2 weeks. Unfortunately, approximately 20% of patients undergo delayed or late Achilles tendon repair, which is defined as surgery performed more than 14 days after injury.8,9 Delayed surgery has been associated with reduced ankle plantarflexion strength, abnormal gait, persistent weakness, and higher rates of complications. 10 Additionally, with the passage of time, surgical intervention becomes more challenging, requiring larger incisions (Figure 1) and sometimes necessitating tissue grafts from other areas.
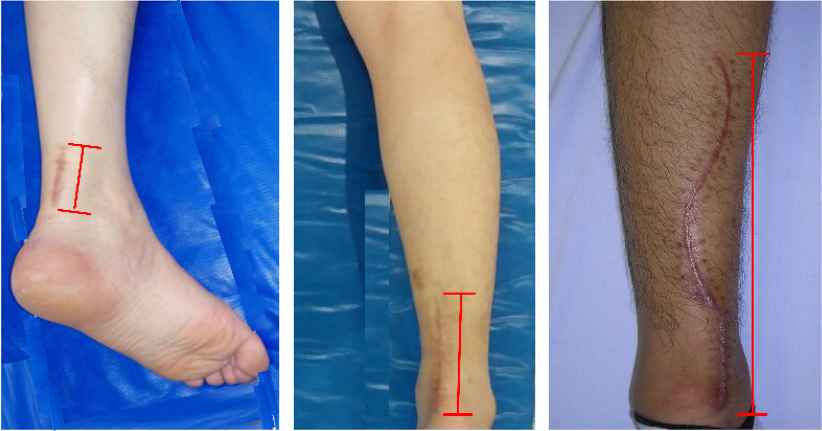
Various surgical incision sizes.
Despite these risks associated with delayed surgery, there are also viewpoints suggesting that the timing of surgery may not significantly impact its outcomes. A study comparing emergency and late repairs over a one-year period found no differences between the groups in terms of subjective assessment score, ankle angles, and heel-raise times. 8 Another study explored minimally invasive techniques akin to acute surgery, performed even for late-stage repairs (14–30 days), and similarly found no significant differences in scores and ankle angles between the groups at the one-year follow-up. 9
Despite reports of outcomes after late (14–30 days) surgery, outcomes for very late (>30 days post-injury) surgery are rare, and few studies have measured long-term changes in strength and sports-related function required for leisure activities. Therefore, the purpose of this study was to compare functional recovery outcomes based on the timing of surgery in men who experienced a total Achilles tendon rupture. We aimed to investigate the prognosis of patients who underwent delayed surgery by comparing the long-term recovery of patients who underwent delayed surgery with those who underwent early surgery. The researchers hypothesized that very late surgery would result in slower recovery than early surgery in the short term, whereas long-term recovery would be similar. The results of this study will provide useful information for understanding the recovery patterns of patients who underwent relatively late surgery, and for designing treatment and rehabilitation procedures.
Data collection and process
Between 2018 and 2023, 112 patients underwent Achilles tendon surgery by an orthopedic surgeon for complete rupture. Inclusion criteria comprised individuals under 50 years of age who sustained injuries during sports or leisure activities; exclusion criteria were those who had previously experienced partial rupture. Of these, 68 patients met the study's criteria with matched age, sex, and final data available for analysis. The groups were categorized into emergency repair (ER, n = 38), late repair (LR, n = 16), and very late repair (VLR, n = 13) groups,8,9 and 12 months of retrospective data were analyzed for this purpose (Figure 2). All patients received medical treatment and underwent rehabilitation post-surgery. Subjective Achilles tendon total rupture scores (ATRSs) using questionnaires, calf circumference, dorsiflexion range of motion (ROM), heel-raise repetition, isokinetic strength (plantarflexion and dorsiflexion), and sports-related function (hop and balance tests) were evaluated. ATRS, dorsiflexion ROM, and calf circumference were measured from 3 weeks post-surgery. For safety, strength, balance, and hop tests that transmit tension to the Achilles tendon were measured from 3 months post-surgery. Researchers also investigated the pathway of visiting the hospital and cause of the injury using open-ended questions. Although this study was a retrospective analysis, all patients were informed of the possibility of analyzing and publishing their data for future research and gave written consent.
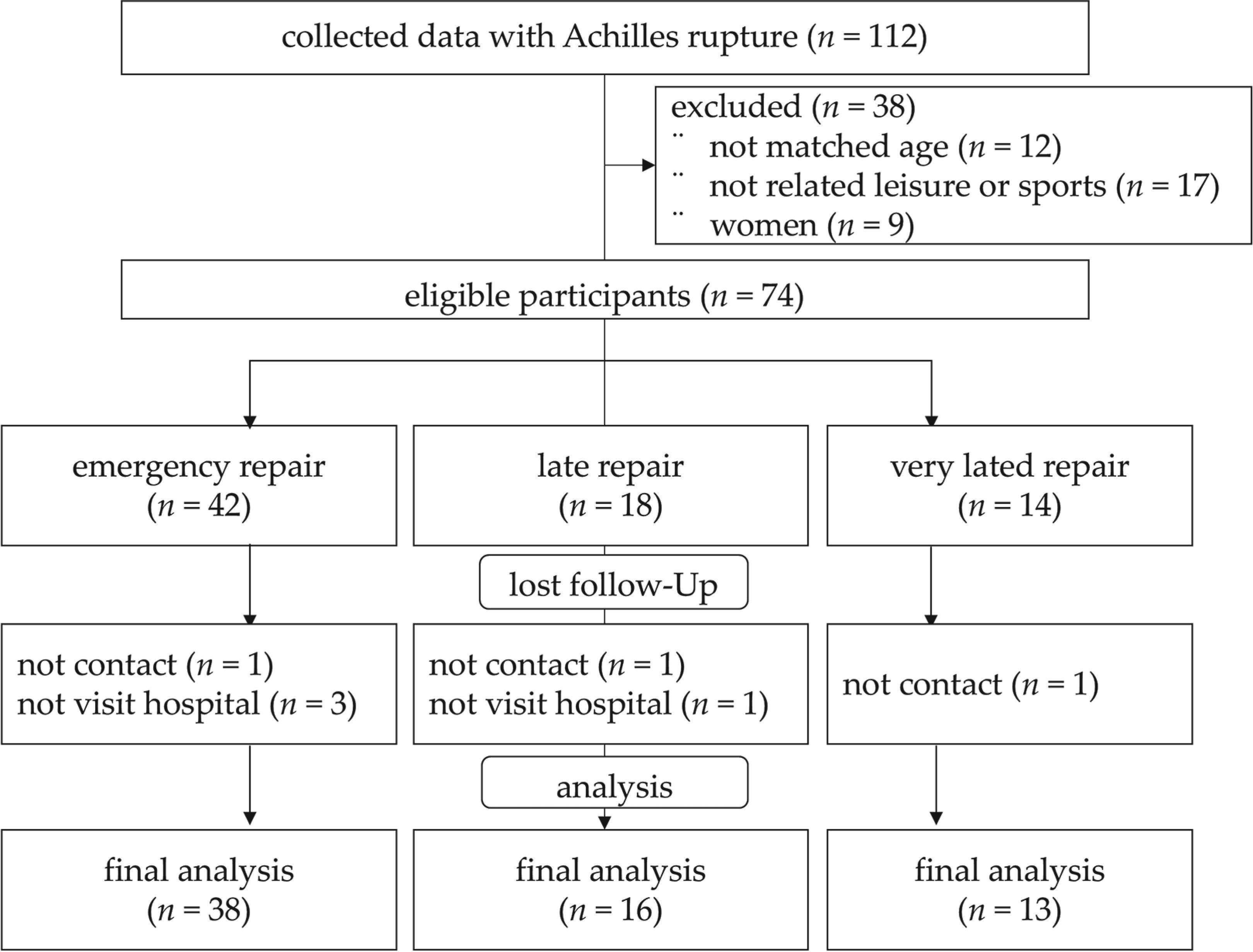
Flowchart of patient enrolment.
The ATRS questionnaire was developed to evaluate patients’ subjective outcome score. It has demonstrated high reliability and validity [intraclass correlation coefficient (ICC) = 0.84, Cronbach's alpha = 0.84], and shows a strong correlation with the ankle score system (r = 0.88). 11 In this study, measurements using the ATRS were obtained at the 3-week visit and self-reported at subsequent follow-up visits. Dorsiflexion ROM was assessed using a manual goniometer with the ankle positioned neutrally at 90°. To minimize measurement errors, all measurements were performed and recorded by the same examiner.
Strength test: Heel-raise, and isokinetic plantarflexion and dorsiflexion strength
Heel-raise test: This test involves standing on one foot and repeatedly raising and lowering the heel. It is commonly used to evaluate strength in patients with Achilles tendon rupture. 12 The examiner demonstrated and explained the test, allowing the participant to lightly place a hand on a wall or table for balance to ensure correct posture. The participant performed as many repetitions as possible, counting each time the heel was raised by more than 50% of the total angle.
Isokinetic plantarflexion and dorsiflexion strength test: An isokinetic dynamometer (Cybex Humac Norm, CSMI, Stoughton, MA, USA) was used, and the maximum strength was expressed in Nm. 13 Instructions, demonstrations, and practice sessions were provided to familiarize patients with the equipment. Measurements were taken with the patient supine on the testing table. The lateral ankle was aligned with the machine axis, and the pelvis and upper body were secured with straps to limit the influence of other body parts during testing. The patient started in a −20° dorsiflexed position and performed 50° of maximal plantarflexion on the start signal. Dorsiflexion was performed similarly, returning to the starting position. Angular velocity was measured at 30°/s, and maximum values were recorded in Nm.
Sports-related functional tests
Sports-related function tests included balance and hop tests. Balance was measured using the Y-Balance Test (YBT) equipment (Functional Movement Systems, Lynchburg, VA, USA). 14 The YBT was chosen for its high reliability in evaluating ankle stability, with ICC values ranging 0.80–0.91. 15 The Y-shaped YBT equipment helps measure balance in three directions, with the patient standing at the center. The test foot was placed on a central platform, and the patient stood on one foot. At the start signal, the patient kept the test foot centered and pushed the pad as far away as possible with the opposite foot, with the distance recorded in centimeters. This was performed three times in the anterior, posteromedial, and posterolateral directions, and the highest value was recorded.
Hop tests: Hop tests included single and crossover. For the single hop, the patient stood on one foot at the starting line and, at the examiner's signal, jumped forward as far as possible in one step. The crossover hop comprised three jumps on one leg and involved moving to the left and right sides along a long, straight line. For both tests, the distance from the starting line to the heel was recorded in centimeters. Each test was performed twice, and the higher value was recorded.
Calf circumference deficit
Calf circumference was measured using a tape measure with the patient in a relaxed prone position. The thickest part of the calf, midway between the knee and ankle, was measured horizontally. Each measurement was taken twice, and if there was a difference of more than 5 mm, the measurement was repeated. The same procedure was followed on the healthy side, and the difference in circumference to that of the affected side was recorded in millimeters.
Medical treatment and rehabilitation after surgery
Postoperative medical care and rehabilitation protocols were based on previous literature.4,16 Patients were hospitalized for 2–3 days post-surgery and discharged when there were no postoperative complications and they were confirmed to be capable of self-care. Patients were asked to use a plaster cast and crutches for 3 weeks post-surgery. Subsequently, removable braces and partial weight-bearing were allowed for up to 6 weeks. The affected area was protected with a soft brace for up to 3 months, during which time weight-bearing and ROM exercises were permitted. Active rehabilitation to regain strength began after 3 months. The overall rehabilitation process, taught by a qualified exercise specialist, is summarized in Table 1.
Standard rehabilitation and care after Achilles tendon repair.
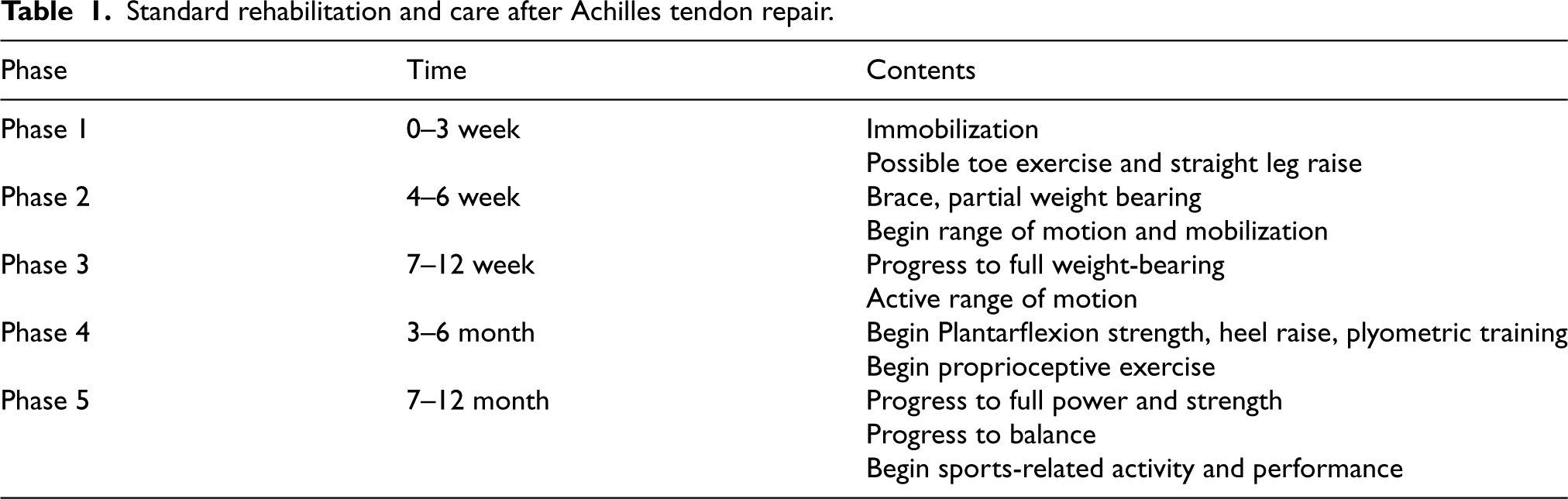
Standard rehabilitation and care after Achilles tendon repair.
IBM SPSS Statistics software version 22 (IBM Corp., Armonk, NY, USA) was used for data analysis. One-way analysis of variance (ANOVA) was used to compare continuous variables across three groups, while an independent t-test was employed to compare two groups. The chi-square test assessed categorical variables related to general characteristics between groups. To determine if there was improvement within a group, comparisons were made with previous test outcomes using a paired t-test. Finally, repeated two-way ANOVA was conducted to examine interaction effects between time and group. The significance level was set at p < 0.05.
Results
General patient information
The patients in the VLR group were older than those in the ER and LR groups, with no difference in the ruptured side between groups. In all groups, injuries to the left were more common than those to the right side, with no differences between groups. The repair time after rupture ranged widely from 1 to 153 days. There was a significant difference in the repair time after rupture between the ER and LR groups, while there was no difference in the return to play time. Meanwhile, the time until repair and return to play was delayed in the VLR group relative to the ER and LR groups (Table 2).
Patient demographic information.
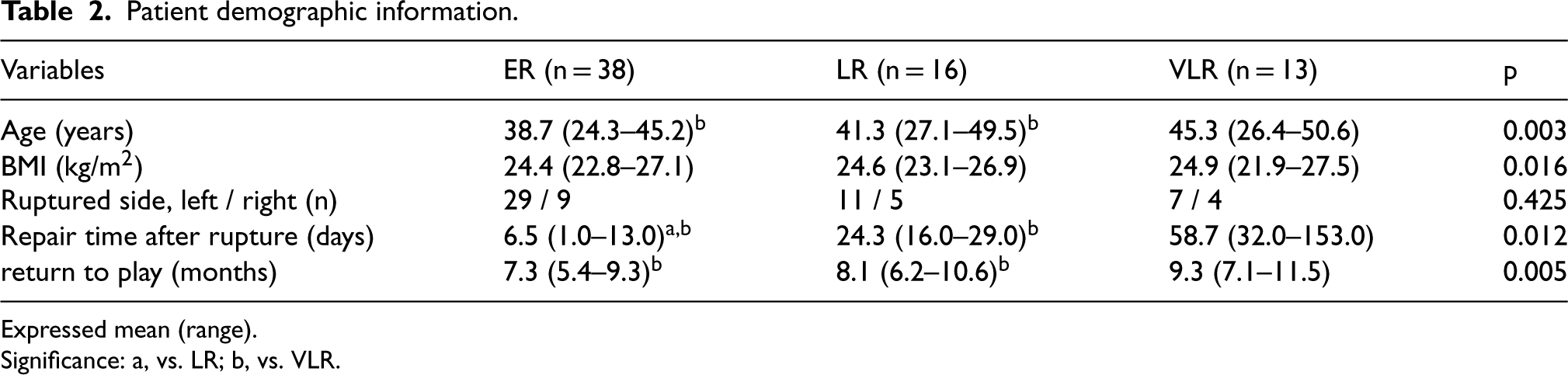
Patient demographic information.
Expressed mean (range).
Significance: a, vs. LR; b, vs. VLR.
The ATRSs of the ER and LR groups were significantly higher than those of the VLR group at both 3 weeks and 3 months post-surgery. However, there was no significant difference between the groups at 6, 9, and 12 months. All groups showed consistent improvement at each measurement time point compared to the previous one. Regarding dorsiflexion ROM, there were no differences between the groups across all measurements. Improvements in ROM were observed at 3 and 6 months, although changes were not significant until 12 months. At 12 months, there were no between-group differences in ATRSs or dorsiflexion ROM, and the interaction effects were non-significant (p > 0.05) (Figure 3).
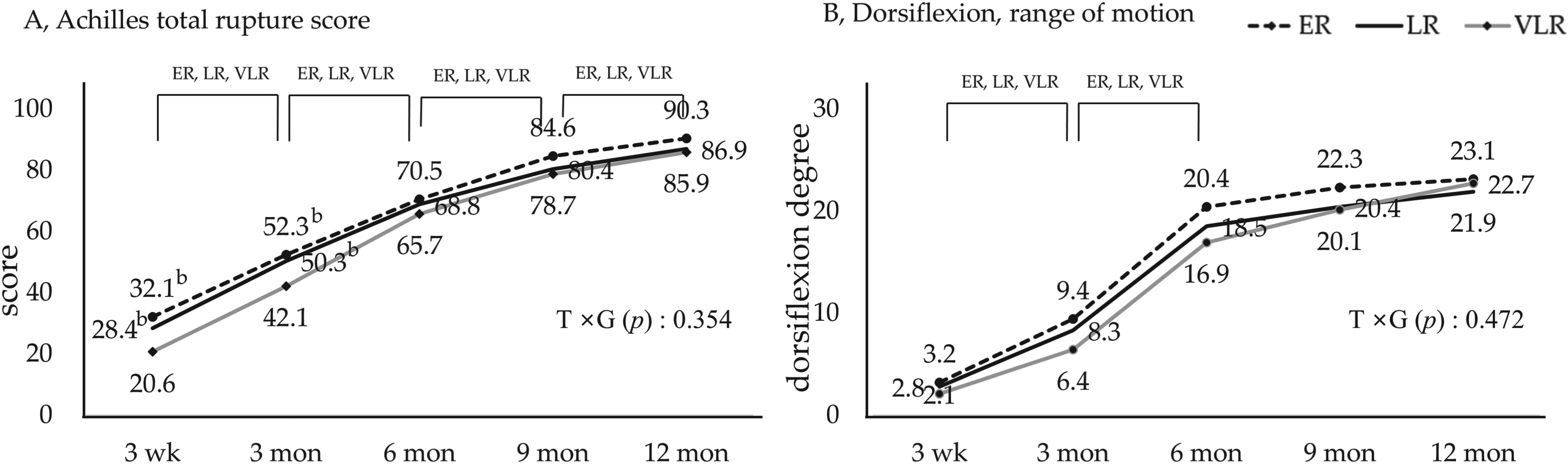
A. Achilles Tendon Total Rupture Score and B. range of motion of dorsiflexion. Abbreviations: ER, early repair; LR, late repair; VLR, very late repair; T × G, time × group.
Ankle strength assessments included heel-raise, and isokinetic plantarflexion and dorsiflexion. The ER and LR groups showed significantly higher heel-raise and plantarflexion strength values compared to the VLR group at 3 and 6 months, whereas there was no significant difference between the groups at 12 months. At 9 months, the heel-raise and plantarflexion values of the ER group were significantly higher than VLR but not the LR group. Dorsiflexion strength at all time points showed no significant differences between the groups. In the three strength-related measures, interaction effects were non-significant (p > 0.05) (Figure 4).
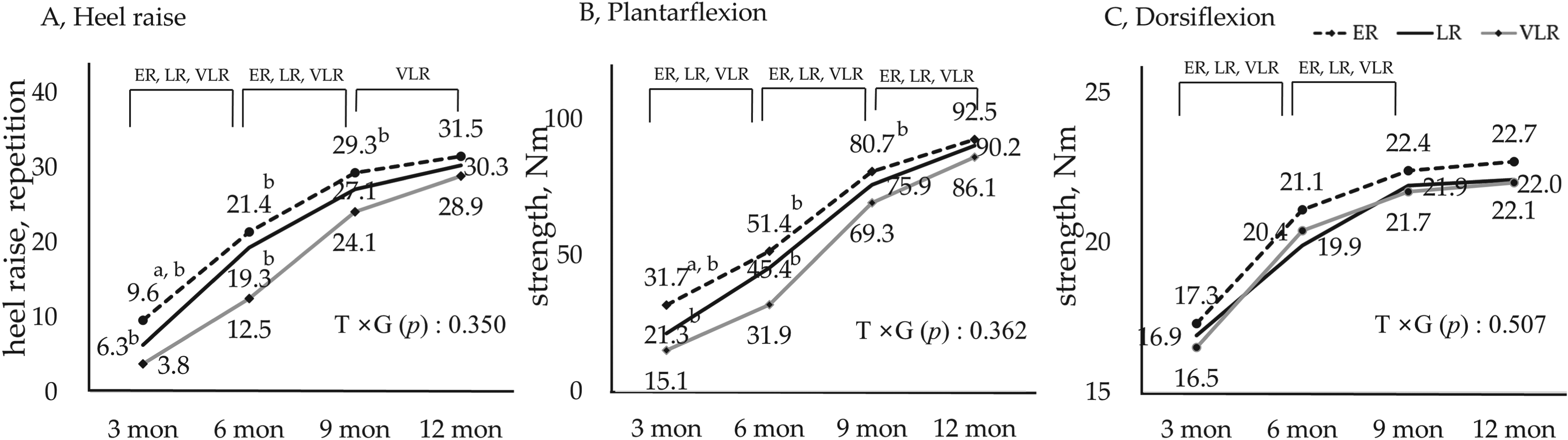
Ankle strength; A. heel raise, B. plantarflexion strength, C, dorsiflexion strength. Abbreviations: ER, emergency repair; LR, late repair; VLR, very late repair; T × G, time × group.
Exercise-related functional tests included the hop test and balance measurement. In the single-hop test, the ER and LR groups achieved a significantly greater distance than the VLR group at 3 and 6 months; there were no significant differences at 9 and 12 months. Despite continuous improvement in crossover hop performance in all groups, the ER and LR groups achieved significantly greater final distances at 12 months compared with the VLR group. A significant time × group interaction was noted for crossover hop performance (p = 0.022) (Figure 5).
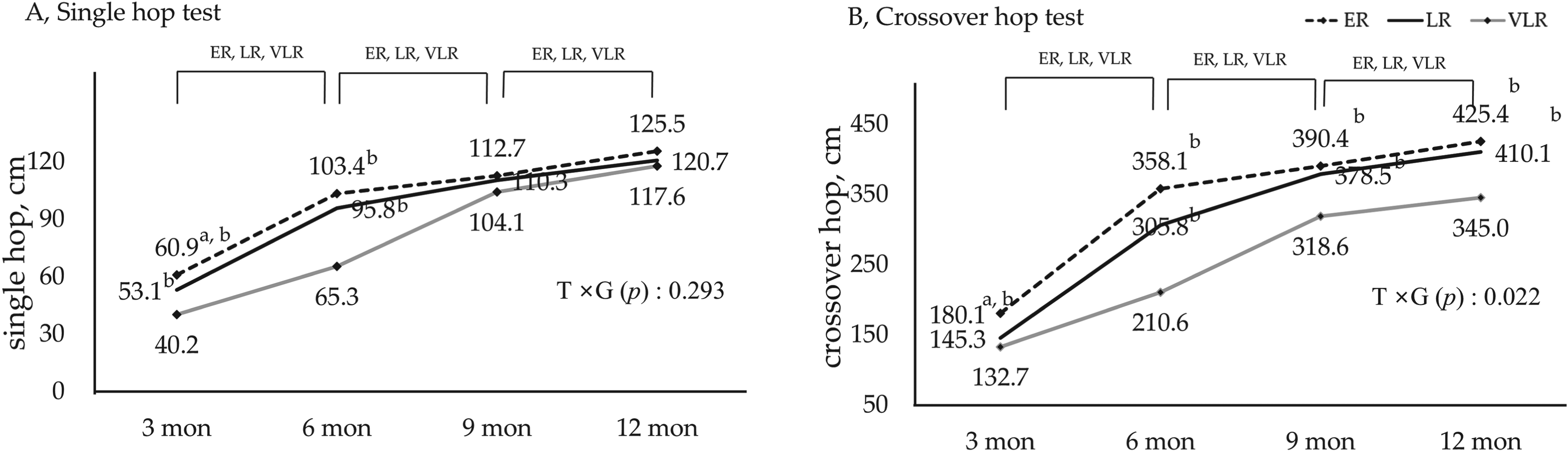
Hop tests; A. single hop, B. crossover hop test. Abbreviations: ER, emergency repair; LR, late repair; VLR, very late repair; T × G, time × group.
In the balance test, the ER group outperformed the LR and VLR groups at 3 months in all three directions, whereas at 6 and 9 months, both the ER and LR groups achieved higher distances than the VLR group in all directions. At 12 months, all three groups achieved similar values in the anterior region, whereas the ER and LR groups had superior reach distances in the posteromedial and posterolateral directions compared with the VLR group. Significant time × group interactions were noted for balance performance in the posteromedial and lateral directions (p = 0.040 and 0.043, respectively) (Figure 6).
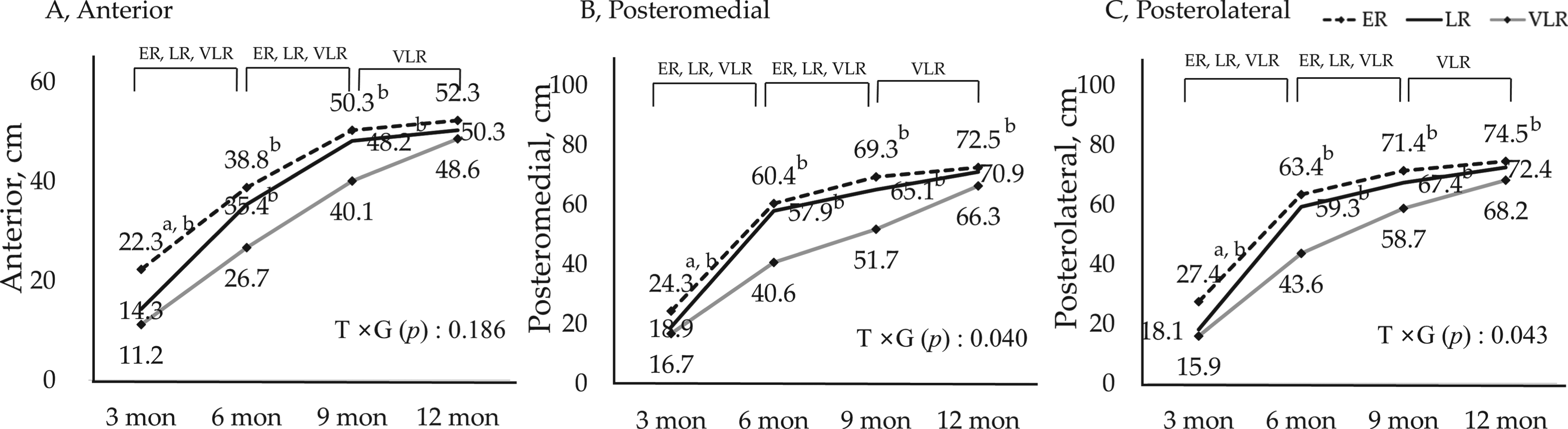
Y balance test; A. anterior, B. posteromedial, C. posterolateral. Abbreviations: ER, emergency repair; LR, late repair; VLR, very late repair; T × G, time × group.
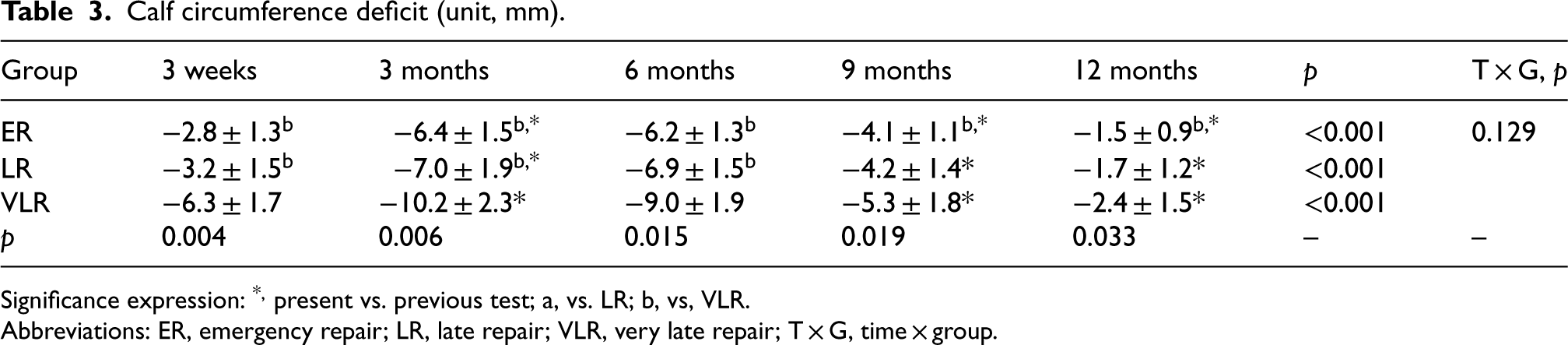
All three groups showed a temporary decrease in calf circumference at 3 months compared to at 3 weeks, and the deficit improved from 9 to 12 months. The VLR group had a greater deficit in calf circumference at 3 weeks, 3 months, and 6 months compared with the ER and LR groups. Conversely, at 12 months, the circumference deficit of the ER group significantly differed from that of the VLR but not the LR group. The interaction based on time and group was non-significant (Table 3).
Calf circumference deficit (unit, mm).
Calf circumference deficit (unit, mm).
Significance expression: *, present vs. previous test; a, vs. LR; b, vs, VLR.
Abbreviations: ER, emergency repair; LR, late repair; VLR, very late repair; T × G, time × group.
Table 4 shows the results of the survey conducted on the ER group. Most patients visited the emergency room on the same day of the injury. Some patients visited the primary hospital 1–2 days after the injury, were diagnosed with an Achilles rupture, and were referred to a hospital where surgery was possible. Alternatively, patients received physical therapy for a few days and voluntarily visited another medical institution.
Emergency room visit and repair pathway after injury.

Emergency room visit and repair pathway after injury.
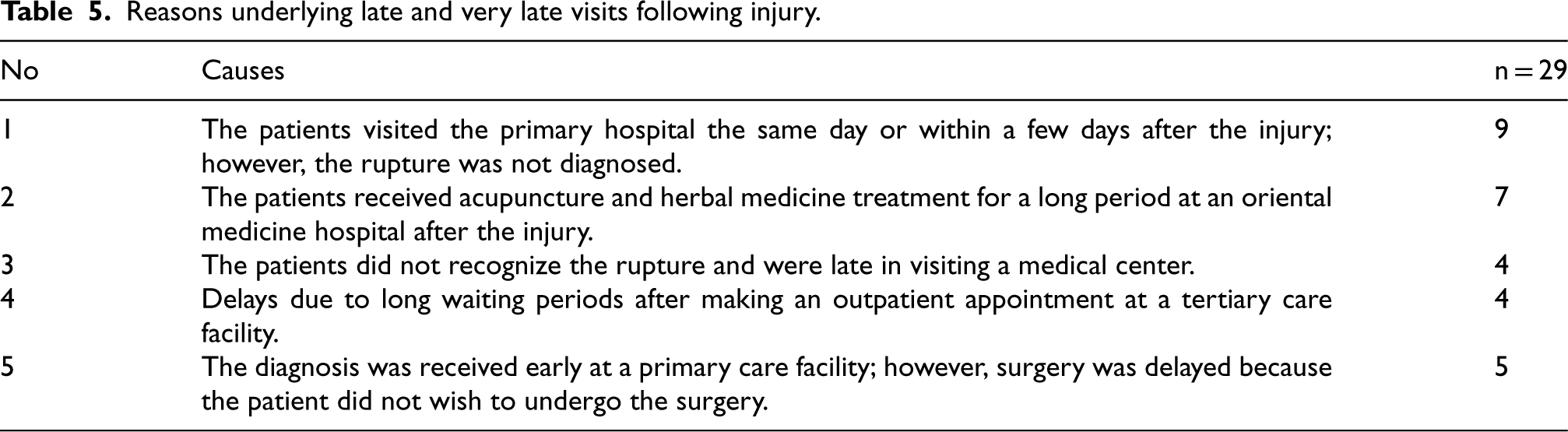
Patients in the LR and VLR groups (29 cases) were interviewed with open-ended questions about the reasons for delaying treatment. A significant number of patients had visited the hospital early but were not diagnosed with an Achilles rupture. Some patients had been receiving oriental treatments, such as acupuncture, for a long time and delayed visiting the hospital because they did not recognize the severity of their condition. In some cases, surgery was delayed due to personal reasons despite a rapid diagnosis of the rupture (Table 5).
Reasons underlying late and very late visits following injury.
This study aimed to compare strength and functional recovery outcomes based on the timing of surgery in men with total Achilles tendon rupture sustained during leisure or sports activities. Specifically, emergency surgery within 2 weeks, late repair within 2–4 weeks, and very late repair exceeding 4 weeks were distinguished, and their recovery outcomes were compared.
The first outcome of this study was that all groups showed sustained improvement in subjective, self-assessed measures using the ATRS questionnaire from 3 weeks to 12 months (Figure 3A), following a similar trend to previous studies.17,18 Repair was performed in 122 patients at a mean of 6.5 days post-injury, and the 12-month surgical outcomes showed a gradual improvement in the ATRS. 17 A study by Carmont et al. 18 compared the ATRSs of 73 patients who underwent repair and were followed for 12 months; their scores continued to improve: 42 at 3 months, 73 at 6 months, 83 at 9 months, and 89 at 12 months. In addition, patients were divided into early (48 h) and late (7 days) groups depending on the repair time after rupture, as in the present study design, and no difference in the ATRS between the early and late groups was found. 18
Achieving full dorsiflexion ROM is crucial for normal ankle function and an important indicator of progression to the next rehabilitation stage. 19 The present study revealed gradual ROM improvement over time, with no differences between groups (Figure 3B). Furthermore, at 9 months post-surgery, all three groups achieved >20° of movement, which is within the normal range. 20 Similar results were reported in a study that performed surgery to restore the ankle angle 17 ; however, while this previous study showed significant angular improvement at 3 months, the present study did not show it until 6 months. Soft tissue stiffness after repair is due to the use of a cast for 3 weeks for safety and a hard brace for up to 6 weeks to maintain a fixed angle. The delayed recovery of dorsiflexion ROM in the current study might be because active stretching was only initiated after 3 months. Considering Achilles tendon rupture occurs due to excessive lengthening, the use of a postoperative cast and slow stretching have a positive effect from the perspective of protecting the affected area. However, soft tissue tightens when in a protective cast post-surgery, leading to prolonged stiffness even after the cast is removed. 19
Several strength outcomes were evaluated in this study (Figure 4). Although the number of heel-raises and isokinetic plantarflexion strength were lower in the VLR group up to 9 months, they ultimately showed similar recovery at 12 months compared with the other groups. Some studies have compared muscle strength over 12 months of follow-up among patients with varied repair times and found similar results to the present study.8,9 Maffulli et al. classified surgery performed 14–30 days post-injury as delayed repair and compared its outcomes with an acute repair group. Plantarflexion strength was assessed, and strength recovery to 410 N in the delayed group and 421 N in the acute group was reported, 9 similar to that in the present study. In a study evaluating heel-raise performance, there was a significant difference between the acute and late groups at 6 and 9 months, but no difference at 12 months. 8 A study conducted by Park et al. also reported no differences in isokinetic strength between groups that underwent repair after 24 h, 48 hours, and 1 week. 21 Although the present study did not compare outcomes between the two sides, previous studies comparing the injured side and the non-injured side of patients reported lower strength on the injured side, even after a long recovery period post-surgery. After one year, the injured side had 12–18% lower strength,9,17 and even after 10 years, a 14.9% strength impairment was reported. 22 This information supports the need for long-term strength management.
In this study, hop and balance performance were measured as sports-related functions (Figures 5 and 6). There were no significant differences between groups in the single-hop test and anterior YBT, whereas in the crossover hop, and the posteromedial and lateral YBT, the VLR group performed worse than the ER group. Olszewski et al. analyzed factors affecting YBT performance in healthy adults from several perspectives; they concluded that ankle dorsiflexion flexibility affects balance, as measured by the leg reach distance. 23 Rafagnin et al. found a high correlation (r = 0.27–0.51) between ankle dorsiflexion ROM and YBT reach distance in futsal players. 24 In the star excursion balance test, similar to the YBT, significant correlations were found with ankle ROM in the anterior (r = 0.55) and posterolateral (r = 0.29) directions.25,26 Additionally, a study analyzing lower extremity strength and balance outcomes reported that hip extensor and knee flexor strength were positively correlated with the YBT distance. 27 In an experimental study by Francis et al., it was reported that training hip abductor muscles increased the distance of the YBT. 28
In this study, calf circumference measurements indicated a reduction in the affected side compared with the healthy side (Table 3). On the affected side, all three groups showed lower values at 3 months compared to 3 weeks, likely due to restricted calf strength exercises and movement imposed by the brace, leading to muscle atrophy. 29 Although the calf circumference improved over time, even at 12 months it remained inferior to the healthy side. Similar findings were noted in a long-term follow-up study involving 55 patients undergoing surgery post-Achilles tendon rupture, where magnetic resonance imaging comparisons revealed smaller cross-sectional areas in the soleus, mediolateral soleus, and flexor hallucis longus muscles on the affected side, alongside a reported 12–18% plantarflexion strength deficit. 30 Nonetheless, the authors emphasized that, while muscle mass correlates with strength, variations in mass may not necessarily translate to strength disparities.31,32
Finally, a notable feature of the current study was the investigation into the reasons for delayed repair through interviews, revealing delayed diagnosis at primary hospitals as a common issue (Table 5). Cases of delayed recognition of the rupture or prolonged reliance on alternative medicine were highlighted, possibly contributing to surgical complexities and potential muscle loss and weakness from disuse over time.
A debate persists over surgery and timing following Achilles tendon rupture. Surgical advocates highlight faster recovery of functionality, including improved hopping ability, strength, and endurance, as a key advantage compared to non-surgical management. 33 Furthermore, early repair is generally recommended as the optimal treatment for complete ruptures compared to delayed repair. 34
Nonetheless, the present study found no long-term differences between groups in most variables and showed that emergency surgery does not necessarily guarantee superior outcomes; even very delayed surgery can lead to similar recovery.
This study had several limitations. Considering it only included young and middle-aged men, its findings cannot be extended to women or other age groups. The rehabilitation performance status of patients, despite undergoing rehabilitation, remains unknown. Furthermore, the study did not evaluate recreational activities, making it difficult to distinguish between individuals with varying activity levels. Moreover, the study focused solely on ruptures resulting from sports and leisure activities in middle-aged men; thus, the findings may not be generalizable to patients with injuries from falls or traumatic accidents. Additionally, the outcomes for women are unclear as the current study excluded women due to insufficient numbers for meaningful analysis.
Future research should collect comprehensive data from women and different age groups, conduct case-control studies and controlled trials to identify optimal rehabilitation methods, and compare outcomes between the healthy side and injured side.
Conclusions
This study evaluated 12-month recovery outcomes following surgery for Achilles tendon rupture based on the repair time after injury. VLR induced similar recovery of ATRSs, ankle strength, dorsiflexion ROM, and single-hop distance compared with ER and LR; meanwhile, crossover hop, and posteromedial and lateral balance performance remained inferior following VLR relative to ER. Therefore, even very late repair shows the possibility of improving ankle strength and functional recovery following Achilles tendon rupture.
Footnotes
Abbreviations
Acknowledgment
We would like to thank Gangneung-Wonju National University for editing and administrative support.
All participants provided written informed consent for the examination and publication of the study. This study was approved by the Research Ethics Committee of Gangneung-Wonju National University (approval number: 202113).
The data presented in this study are available on reasonable request from the authors.
HC and YK and YP—Conceptualization; HC and YC—methodology; HC and YC and YK—formal analysis; YC and YK —investigation; HC and YK and YP—original draft writing; YC and YK and YP—review and editing; YK and YP —supervision. All authors contributed to the editorial changes in the manuscript. All the authors have read and approved the final version of the manuscript.
The authors received no financial support for the research, authorship, and/or publication of this article.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.