
Abstract
Background
Static stretching (SS) is effective in increasing flexibility and neuromuscular function, leading to changes in postural control.
Objective
This study aimed to examine the acute effects of SS on ankle plantar flexors and dynamic postural control during a maximum forward-leaning task in young and older adults.
Methods
Twenty-eight university students and 22 community-dwelling older adults were included in this study. The participants performed 5 sets of 1-min SS for the ankle plantar flexors of both legs with standing on a stretching board. Ankle dorsiflexion range of motion (ROM) and center of pressure (COP) during the maximum forward-leaning task, the COP area, and the anterior limit of stability were assessed before and after SS.
Results
SS increased ankle dorsiflexion ROM, COP velocity, and anterior limit of stability, whereas changes in the COP area were not significant after SS. Furthermore, there were no differences in the changes in postural control between young and older adults, whereas ROM increase was greater in older adults than in young adults.
Conclusions
These findings suggest that SS can improve postural control and can serve as a simple, low-risk intervention to reduce the risk of falls in older, at-risk adult populations.
Introduction
Postural control for activities of daily living involves the neuromuscular, vestibular, visual, and somatosensory systems.
1
Joint flexibility decreases in older adults,2,3 which is associated with reduced postural control and the occurrence of falls.4–6 Falls and related injuries can cause disability, hospitalization, loss of independence, and increased mortality.
7
Moreover, fall-related injuries lead to activity restriction, further decline in physical function, and loss of quality of life.8,9 Therefore, increased flexibility and postural control may reduce the risk of falls, leading to improved health and social conditions in older adults.
Comparison of the percent changes in ROM and COP parameters between young and older adults. (a): ROM; (b): LOS; (c) COP velocity; (d): COP area. * indicates a significant difference between young and older adults.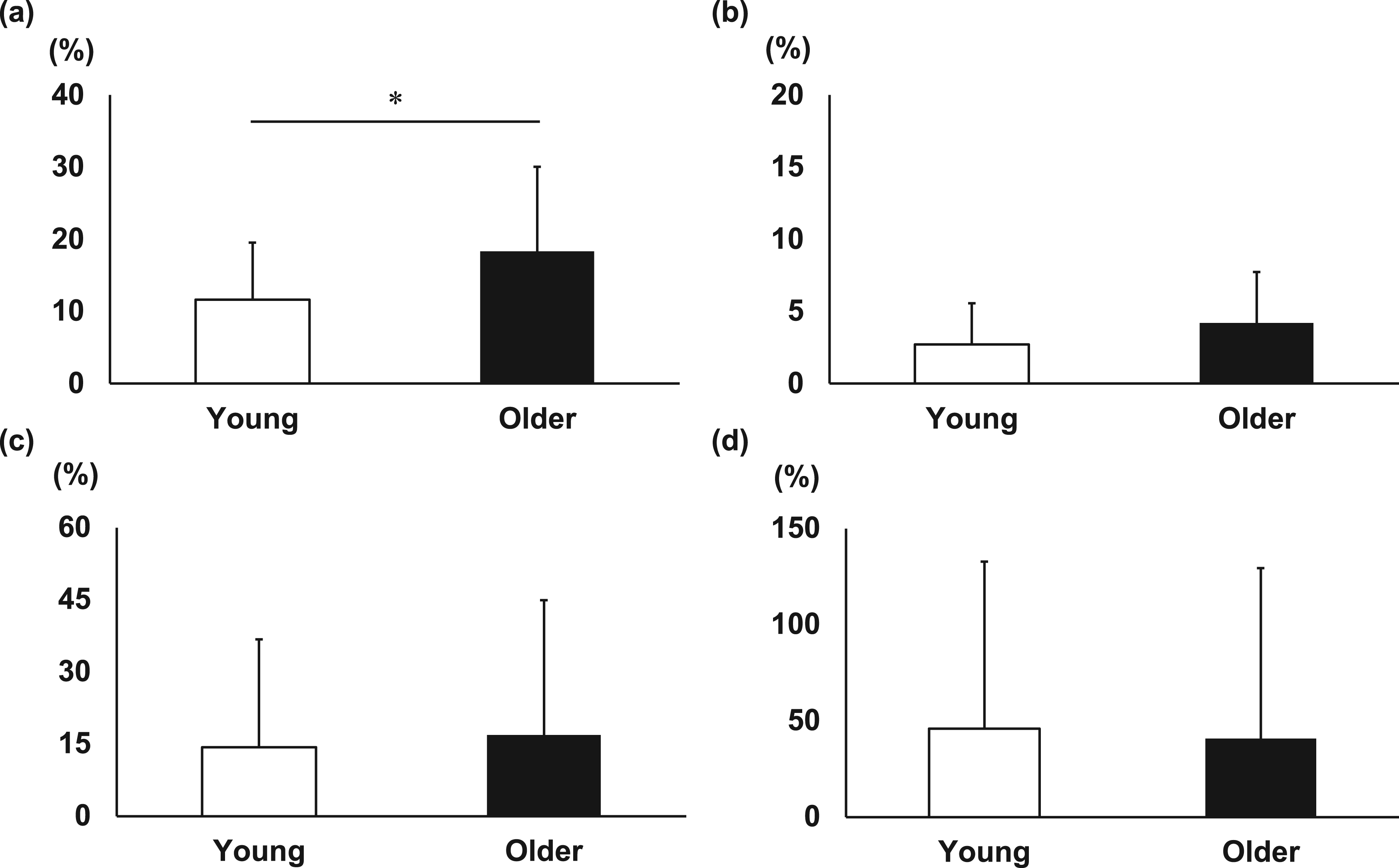
Static stretching (SS) has been commonly used as a preparation exercise in sports. It is typically beneficial in increasing the range of motion (ROM) and decreasing the musculotendinous stiffness.10–12 Notably, older adults often exhibit decreased ROM and increased musculotendinous stiffness.11,12 SS induces mechanical and neural adaptations in the musculotendinous complex, which affects force transmission and the proprioceptive feedback system.13–18 Thus, SS results in the change of postural control. Age-related increases in musculotendinous stiffness have been linked to impairments in postural control among older adults. 19 Previous studies report that older adults experience greater improvements in ROM and reductions in musculotendinous stiffness following SS compared to young adults.11,12 Consequently, postural control changes due to SS may differ between younger and older adults.
The center of pressure (COP) has been used to obtain quantitative outcomes of postural control during standing tasks. 20 The COP position indicates the position to maintain the posture within the base of support, while COP velocity determines the extent of sway velocity and COP area reflects sway area, which represents the ability to stabilize posture in response to self-initiated or externally induced disturbances. 21 Nagano et al. 22 reported that SS to ankle plantar flexors in young adults significantly increased anteroposterior (AP) COP range and COP velocity during double-leg standing. SS to unilateral ankle plantar flexors in young adults also reportedly increased the COP area during one-leg standing, indicating decreased postural stability. 23 In contrast, Martínez-Jiménez et al. 24 reported that SS of the ankle plantar flexors in young adults decreased the COP area and improved postural stability during double-leg standing. Thus, reports on the effects of SS on postural control in static balance tasks (i.e., one-leg standing and double-leg standing) among young adults are conflicting. Moreover, postural control during balance tasks involving weight shift has not been thoroughly examined in previous studies despite the necessity of a smooth COP shift for transferring or shifting body weight during daily activities. A recent study 21 showed that SS to the bilateral ankle plantar flexors in young adults did not change the COP area during a maximum forward-leaning task, but allowed the COP to shift more forward during the maximum forward-leaning task. The maximum voluntary COP excursion in the base of support is defined as the limit of stability (LOS) and reflects dynamic postural control. 25 Thus, the SS of the ankle plantar flexors in young adults increases the anterior LOS while maintaining sway area and improves postural control. 21 The maximum forward-leaning task is considered an important screening tool for older adults because anterior LOS is correlated with the dynamic balance score and gait performance in older adults.26,27 However, it remains unclear whether SS improves postural control during maximal forward leaning tasks among older adults and, whether the postural control response to SS differs between older and young adults. Demonstrating the effects of aging on changes in postural control through SS would allow stretching programs to be tailored to individuals and their specific needs.
The present study aimed to examine the acute effects of SS on ankle plantar flexors and postural control during a maximum forward-leaning task in young and older adults. We hypothesized that both young and older adults would demonstrate increased flexibility and anterior LOS, with older adults showing greater improvements in flexibility and anterior LOS than young adults.
Participants
Twenty-eight young male adults (age 21.4 ± 1.2 years; height 171.8 ± 5.6 cm; body mass 63.9 ± 7.5 kg) and 22 community-dwelling older adults (4 males and 18 females; age 73.9 ± 5.5 years; height 151.8 ± 6.1 cm; body mass 54.9 ± 8.0 kg) participated in this study. Only young male adults were recruited to avoid the potential confounding effects of the menstrual cycle on stretching effects in females.28,29 Older adults who volunteered to participate in the present study were included from city council exercise classes. None of the participants had current lower-limb injuries, neuromuscular diseases, ophthalmologic diseases, or vestibular disorders that affected postural control assessment. For older adults, participants who had a significant decline in cognitive function were excluded. Written informed consent was obtained from each participant after sufficient explanation of this study.
Postural control assessment
All participants performed the maximum forward-leaning task as a dynamic balance assessment, with COP displacement before and after SS. The COP X-Y positions were measured and recorded using a force plate (FDM-S ver. 1.2.0, Zebris Medical GmbH, Germany) at 100 Hz. The participants stood barefoot with arms crossed over their chests and feet 10 cm apart on a force plate, with their foot position marked using tape. They were instructed to look straight ahead for 2 m at their eye level. After the standing posture stabilized, the maximum forward-leaning task was performed. The participants were instructed to move their COP forward as far as possible for 3 s and maintain their posture without bending both hips and knees or raising their heels from the floor for 30 s. 21 Several practice trials were conducted to confirm movements of the maximum forward-leaning task while minimizing the learning effect. If inadequate motions were observed (e.g., trunk rotation, knee and/or hip flexion, or heels rising from the floor), participants were instructed to stop and repeat the test. This task was performed twice. The COP X-Y position during the maximum forward-leaning task was recorded using WinFDM software (Zebris Medical GmbH, Germany) and processed offline using MATLAB software (MathWorks, Natick, MA, USA). To clarify the postural control change, the mean anteroposterior COP (COPAP) position, mean COP velocity, and COP area were determined. 21 We analyzed 10-s durations starting from 2 s after reaching the peak COPAP position because the timing of peak COPAP is considered as the transition phase from double-leg standing to maximum forward leaning. 21 The distance between the heel and the mean COPAP position was normalized using the foot length of each participant, which was indicated as a percentage of the heel and anterior LOS. The sway speed of the COP velocity was divided by the total COP length for 10 s. COP area was estimated by the 95% confidence ellipse area. 30 The COP velocity and COP area were standardized by foot length.
Range of motion measurement of ankle dorsiflexion
Before and after SS, the maximum ankle dorsiflexion ROM was determined using a digital inclinometer (DL-155 V; STS, Japan) based on a previous study. 21 The measurement of ankle dorsiflexion ROM using an inclinometer has been validated in previous study. 31 Participants were instructed to put one leg backward as far as possible, with the knee fully extended, and the heel kept in contact with the ground. The midpoint between the first and second toes and the calcaneus was placed on the vertical line on the wall to prevent any movement of the subtalar joint with ankle dorsiflexion. The contralateral side was tested first, and the hands were permitted to touch the wall to preserve balance. The tibial inclination was measured for ankle dorsiflexion ROM 15 cm distal to the tibial tuberosity. 31 The measurements were retested when the heel was displaced from the ground. The measurement was repeated three times on both sides, and the average tibial inclination was defined as the ROM. To ensure the test–retest reliability of ROM, the ROM measurement of ankle dorsiflexion was repeated two times in a pilot study (n = 26), and the intraclass correlation coefficients (ICC) were calculated. ICC was 0.97 [95% CI: 0.93 − 0.99] for ankle dorsiflexion ROM measurement.
Static stretching
The participants performed SS for the ankle plantar flexors of both legs while standing on a stretching board (Toei Light Co., Ltd, Tokyo, Japan) 21 under the supervision of the Ohta Moeka (O.M.) or Oka Izumi (I.O.). The participants were instructed to stand looking straight forward with their backs leaning against the wall. The stretch intensity was defined as the point of discomfort but not pain, 28 and the angle of the stretching board was adjusted by 1˚. A 60-s SS was performed five times on both legs, with a rest interval of 30-s. The angle of the stretching board was adjusted between every stretch interval to maintain the intensity. Many previous studies reported that SS for a total of 5-min increased ROM and decreased musculotendinous stiffness.32,33
Statistical analysis
All statistical analyses were performed using the SPSS software ver. 21.0 (SPSS Inc., Chicago, Illinois, USA). The Shapiro-Wilk test was used to evaluate the normality of demographic data, ROM, and COP parameters. Depending on normality, differences between the young and older adults for demographic data and baseline value of ROM and COP parameters were evaluated using the unpaired t-tests or Mann-Whitney U tests. Differences between before and after SS for ROM and COP parameters were assessed using the unpaired t-tests or Wilcoxon signed rank sum tests. The percent change in each parameter before and after SS was calculated. The unpaired t-tests or Mann-Whitney U tests were used to compare the percent change in ROM and COP parameters among young and older adults. To determine associations between percent change in ankle dorsiflexion ROM and anterior LOS, Pearson correlation analysis or Spearman's rank correlation tests were conducted. The significance level was set at p < 0.05, and all data are presented as the mean ± SD.
Results
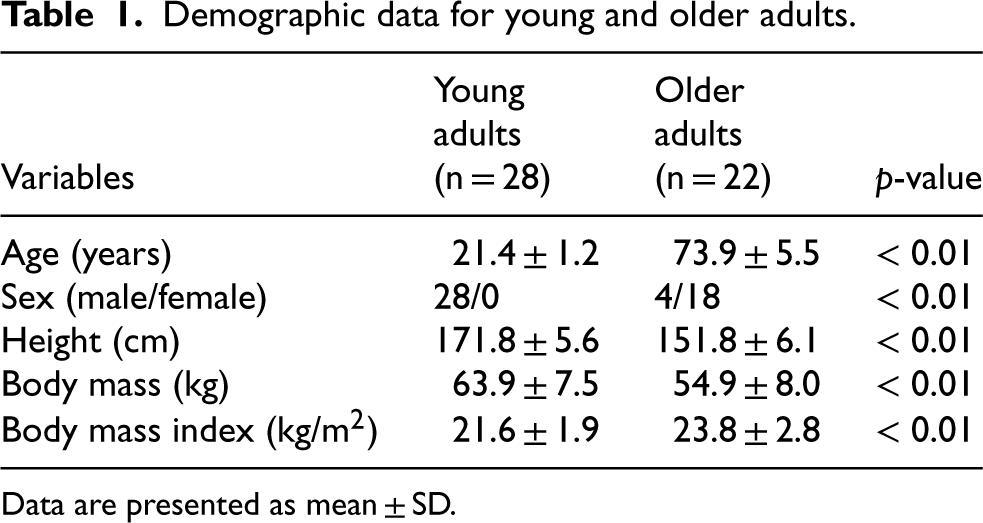
Table 1 shows demographic data for young and older adults. Significant differences in age, height, body mass, BMI, and sex proportion were observed.
Demographic data for young and older adults.
Demographic data for young and older adults.
Data are presented as mean ± SD.
The baseline value of ROM in both young and older adults is presented in Table 2. Young adults show significantly greater ROM than older adults (p < 0.01). After SS, ROM in both young and older adults significantly increased (young p < 0.01; older p < 0.01), and the percent change of ROM in older adults was significantly higher than in young adults (p = 0.04) (Figure 1).
ROM and COP parameters before and after stretching.

Data are presented as mean ± SD.
ROM: range of motion; LOS: limit of stability; COP: center of pressure; FL: foot length. CI: confidence interval.
*indicates a significant difference between Pre and Post stretching.
#indicates a significant difference between young and older adults.
The baseline value of COP parameters in both young and older adults is presented in Table 2. Young adults show significantly greater LOS (p < 0.01), whereas no significant difference in COP velocity (p = 0.11) and COP area (p = 0.053) among young and older adults. SS significantly increased LOS (young p < 0.01; older p < 0.01) and COP velocity (young p < 0.01; older p < 0.05) in both young and older adults. However, there was no significant change in COP area (young p = 0.14; older p = 0.28) in both young and older adults after SS. Furthermore, no significant difference in the percent change of COP parameters between young and older adults (LOS p = 0.12; COP velocity p = 0.51; COP area p = 0.91) (Figure 1).
No significant correlation was found between the percent change in ankle dorsiflexion ROM and anterior LOS in both young (r = −0.26, p = 0.19) and older (r = −0.19, p = 0.39) groups.
This study investigated the acute effects of SS on ankle plantar flexors and COP during maximum forward-leaning tasks in young and older adults. The results showed that SS increased ankle dorsiflexion ROM, anterior LOS, and COP velocity during the maximum forward-leaning task in both young and older adults. However, the COP area remained unchanged after SS in both the young and older adult groups. The percent change in ROM increases was significantly greater in older adults than in young adults, while no significant difference in COP parameters was observed between the young and older adults. These findings revealed that SS improved anterior LOS while maintaining postural stability, indicating the improvement of dynamic postural control; there were no differences in stretching effects on postural control between young and older adults.
The maximum forward-leaning task is known to ascertain the anterior LOS within the base of support, which indicates dynamic postural balance. 25 This study revealed that SS increased the forward shift of the COP during the maximum trunk forward-leaning task in both young and older adults, increasing LOS and improving dynamic postural balance. Thus, it is evident that SS is also effective in improving postural control among older adults. In previous studies,34–36 significant positive correlations were found between the maximal ankle dorsiflexion ROM and dynamic balance scores (e.g., functional reach test, Star Excursion Balance Test, and forward-leaning balance task). Moreover, SS in young adults increases the forward shift of COP during the maximum forward-leaning task with an improvement in ankle dorsiflexion ROM. 21 However, the present study also revealed no significant positive correlation between the increase in ROM and anterior LOS in both young and older adults. Consequently, these findings suggest that the increase in anterior LOS during the maximum forward-leaning task may be attributed to neuromuscular adaptation rather than an increase in joint flexibility resulting from SS. Furthermore, the COP area did not change during the maximum forward-leaning task in both young and older adults, indicating that the sway area was maintained following SS. A previous study also found that SS improved postural control by suppressing the stretch reflex for postural displacement on an unstable surface. 37 In this study, a larger anterior LOS following SS would allow a more forward COP shift during the maximum forward-leaning task. Thus, the participants had to maintain unstable postures as the LOS was getting closer to the edge of the base of support, and more torque adjustment to the ankle joint was required. Therefore, the present results indicate that SS suppressed the stretch reflex to postural displacement and improved ankle torque adjustments, which would adapt the COP velocity and maintain sway area even though the anterior LOS was increased.
SS in older adults induced a greater increase in ROM, a decrease in musculotendinous stiffness, and a smaller reduction in muscle strength and muscle activity compared to young adults.11,12 We hypothesized that postural control changes after SS could differ between young and older adults. However, there was no significant difference in COP change between young and older adults after SS, although ROM increase was greater in older adults than in young adults. As previously mentioned, the lack of association between increased LOS and increased ROM suggests that factors other than joint flexibility, such as neuromuscular properties (i.e., changes in reflex activities and central neural drive),13,15 are involved in the changes in postural control induced by SS. While not measured in this study, it is conceivable that differences in muscle activity between young and older adults could be detected. In the future, muscle activity should be examined to elucidate the postural control changes resulting from stretching in greater detail.
In clinical practice, SS is commonly performed to prevent sports injuries. Decreased ROM in older adults is associated with gait performance, balance, and fall risk.4–6,38 Anterior LOS is correlated with the dynamic balance score and gait performance in older adults.26,27 In the present study, after SS for 5-min, young and older adults had similar improvement in anterior LOS, although the ankle dorsiflexion ROM and postural control baselines were different. Consequently, SS could be beneficial in improving flexibility and postural control in both young and older adults, even though older adults have decreased flexibility and postural control. Therefore, SS is a simple and low-intensity exercise, and SS for 5-min is appropriate for the prevention of falls and injuries.
This study has several methodological limitations. First, only males participated in the young adult group. In contrast, the older adult group had a higher proportion of females though the participants were recruited irrespective of sex. Thus, there was a significant difference in the sex distribution between the younger and older groups. A recent meta-analysis revealed that sex did not lead to stretch-induced changes in ROM. 39 Furthermore, in our older adult group, there were no significant differences between males and females in the changes of all outcomes (ankle dorsiflexion ROM: p = 0.27; anterior LOS: p = 0.19; COP velocity: p = 0.67; COP area: p = 0.84). Therefore, the influences of the sex differences of the younger and older groups are considered negligible on the present results. Second, the exercise habits of each participant were not assessed. Exercise habits and training background have been shown to influence stretch-induced ROM increase. 40 Older adults who participated in this study may have been active because they were recruited in city council exercise classes. Third, this study did not examine the muscle activity during the maximum forward-leaning task. A possible difference in muscle activity could be observed during maximum forward leaning among young and older adults with SS. Future studies should assess muscle activity to clarify postural control differences between young and older adults after SS. Fourth, only the maximum trunk forward-leaning task was used to assess postural balance. Single-leg standing stability and postural control against unexpected disturbances are also important in activities of daily living.
Conclusion
This study investigated the acute effects of SS on the ankle plantar flexors and postural control during the maximum forward-leaning task in young and older adults. SS increased ankle ROM, anterior LOS, and COP velocity, whereas the COP area was unchanged in both young and older adults. Furthermore, SS showed no difference in the changes in postural control between young and older adults. These findings suggest that SS improves postural control in both young and older adults and that it could be recommended for the prevention of falls.
Footnotes
Acknowledgements
We would like to thank all the participants.
Ethical approval
The institutional review board of the Faculty of Health Sciences at Hokkaido University approved the present study (number: 18–64; date: Dec. 6th, 2018). All the experimental procedures were performed in accordance with the principles of the Declaration of Helsinki.
Informed consent
Informed consent was obtained from all individual participants included in the study
Author contributions
Conception: Kensuke Oba, Mina Samukawa, Moeka Ohata, Izumi Oka, Satoshi Kasahara, Teppei Suzuki, and Katsuhiko Ogasawara.
Performance of work: Kensuke Oba, Moeka Ohata, and Izumi Oka.
Interpretation or analysis of data: Kensuke Oba, Moeka Ohata, and Izumi Oka.
Preparation of the manuscript: Kensuke Oba.
Revision for important intellectual content: Mina Samukawa, Satoshi Kasahara, Teppei Suzuki, and Katsuhiko Ogasawara.
Supervision: Mina Samukawa and Katsuhiko Ogasawara.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.