
Abstract
Background
The lower trapezius (LT) involves scapular depression and retraction so, the scapular depression strategy is expected to increase the LT activity during prone Y exercise.
Objective
To investigate the effects of three different strategies during prone Y exercise on the scapular muscle activities, muscle activity ratios, and scapular positions in participants with scapular dyskinesis (SD).
Results
Our results revealed that the intended scapular depression with arm lifting condition demonstrated the highest LT and MT activity along with changes in scapular positions (UHD and SDA) and exhibited significantly higher than the scapular depression with roller-assist condition (P < 0.05). Whereas, UT activity showed less in the intended scapular depression with arm lifting condition compared to the arm lifting condition (P < 0.05). Additionally, the UT/LT and UT/MT ratios were less in the intended scapular depression with arm lifting and scapular depression with roller-assist than in the arm lifting condition (P < 0.05).
Conclusions
Our results indicate the intended scapular depression with arm lifting strategy is expected to be more effective in improving LT and MT activity through the adduction and depression of the scapula in males with SD particularly.
Introduction
The scapular dyskinesis (SD) is characterized by changes in scapular kinematics caused by periscapular muscle imbalance, including decreased serratus anterior (SA) and lower trapezius (LT) activity. As well as, decreased upward rotation and posterior tilt of the scapula causing shoulder problems such as impingement syndrome.1–4 Additionally, SD affects the muscle length-tension relationship for force generation of the rotator cuff attached to the scapula, causing decreased strength and imbalance of the rotator cuff4–6 and predisposes to shoulder injuries.3,7,8 Among the periscapular muscles, LT acts as an upward rotation of the scapula through force coupling with the upper trapezius (UT) and SA, and the scapular posterior tilt.9–12 In particular, LT plays a major role in the upward rotation and posterior tilt of the scapula at the late stage in the arm elevation11,12 and prevents impingement by elevating the acromion. 13
LT weakness reduces the scapular upward rotation and increases the scapular anterior tilt,14,15 causing subacromial impingement.16,17 Additionally, excessive involvement of the UT caused by LT weakness causes an decrease activity ratio of the LT relatively to UT, as well as imbalance of the periscapular muscles, it leads to shoulder dysfunction and injuries.1–4,7,8 Therefore, LT strengthening and improving scapular muscle balances are important in rehabilitation.18,19 The prone Y exercise is known as effective for strengthening LT.20–22 Since the required arm lifting is in line with the LT fibers for performing exercise, it can represent the functional properties of the LT.11,12
However, despite the advantages of effectively strengthening LT, some studies have reported that prone Y exercise contributes to a higher increase in UT activity, with 72%–79% maximal voluntary isometric contraction (MVIC).20,23 In particular, SD type I, defined as prominence of the inferior medial border of the scapula, considered caused by representative weakness of the LT. Therefore, a strategy to minimize UT activation while selectively increasing LT activation should be considered during exercise. Some studies have investigated the effectiveness of intentional scapular motion strategies based on the function of the LT involved in scapular movement. A previous study reported that the scapular posterior tilt strategy increases LT activity by approximately 72% MVIC to 76% MVIC during prone Y exercise.24,25 Therefore, it may be expected that a strategy considering scapular movement based on LT muscle function could effectively activate the LT.
However, scapular posterior tilt requires precise motor control, if the exercise is performed without the supervision or guidance of a physiotherapists or athletic trainers, it may be difficult to perform the movement accurately due to such as compensatory movements. Furthermore, since the scapular movement must be controlled while the arm is raised, it is expected to be more difficult. Indeed, previous studies reported that UT activity showed no significant difference from the general prone Y exercise condition.24,25 LT acts not only on scapular posterior tilt but also on scapular depression and retraction9–12 so, when performing the prone Y exercise, the scapular depression strategy is expected to increase LT activity. Because scapular depression requires the inhibition of the scapular elevators including the UT along with the involvement of the LT, it is expected that more selectively activated LT while minimizing activation of the UT.
In addition, a scapular depression strategy using a foam roller that can support the arm and provide rolling assistance is expected to affect muscle activity because it may minimize external load produced by gravity and arm`s weight and assist in scapular depression. Therefore, this study aimed to determine the effects of three different exercise conditions on the activities of the LT, UT, and MT muscle, muscle activity ratios, and scapular positions during prone Y exercise in male participantss with SD.
Methods
Participants
The sample size required for this study was calculated using G*Power (version 3.1.2; Franz Faul, University of Kiel, Germany) based on a previous study that examined the changes in scapular muscle activities according to the scapular posterior tilt strategy. 24 At least seven participants were needed to identify changes in activity of the LT muscle (p = 0.05, effect size: 0.71, 95% statistical power). This study included 20 males with SD (age: 23.6 ± 4.81 years, height: 174.25 ± 4.79 cm, weight: 71.45 ± 12.00 kg). Participants who had surgery within the last six months, rotator cuff lesions, shoulder tendinitis, bursitis, or instability were excluded. 20 All participants gave informed consent after sufficient explanation for this study. The present study was approved by the Institutional Review Board of the Bioethics Committee of Pukyong National University (IRB No: 1041386-202312-HR-145-02). This study was also registered in the Clinical Research Information Service (registration number: KCT0009364).
Classification of the SD
The SD was assessed by two physical therapists with more than 10 years of experience in the field of musculoskeletal disorder and classified. 26 Participants elevated their bilateral arm three times in the scapular plane in a standing position with 1 kg dumbbells while maintaining their thumbs up. 27 The examiners observed scapular movements in behind participants and classified SD types27,28 based on described in Table 1. Participants were included in this study only when the two examiners’ assessments of the presence of SD were matched and the SD types were classified as the same. If the evaluation results of the two examiners did not match, the participants were excluded from the study. In this study, out of a total of 32 participants (24 males and 8 females), 20 male participants whose SD test results from two examiners were consistent have participated. As a result of the SD test in this study, there were no type III, and 15 and 5 participants with type I and type II were identified, respectively.
Classification criteria for SD types.

Classification criteria for SD types.
SD: scapular dyskinesis.
Participants performed the prone Y exercise in three different conditions in random order: arm lifting; intended scapular depression with arm lifting; and scapular depression with roller-assist using the foam roller. Each exercise method is described in Table 2. Prone Y exercise for each condition was performed at 125° shoulder abducted position, which is more effective in increasing LT muscle activity. 29 Shoulder abducted position and arm lifting height were controlled using a target bar (Figure 1). Participants were asked to raise their arms while maintaining contact between the target bar and the upper arm in a 125° shoulder abduction position until the distal forearm touched the target bar. The height of arm lifting during exercise was quantified as height of the foam roller. Since there was no necessary to control the arm height in the foam roller assist condition, the arm lifting height was controlled in the arm lifting and intended scapular depression with arm lifting conditions using the target bar in this study. Participants were asked to maintain an isometric contraction for 5 s at the end position of each condition. The exercise was performed three times in each exercise condition, with a 3-min rest period between exercise conditions.
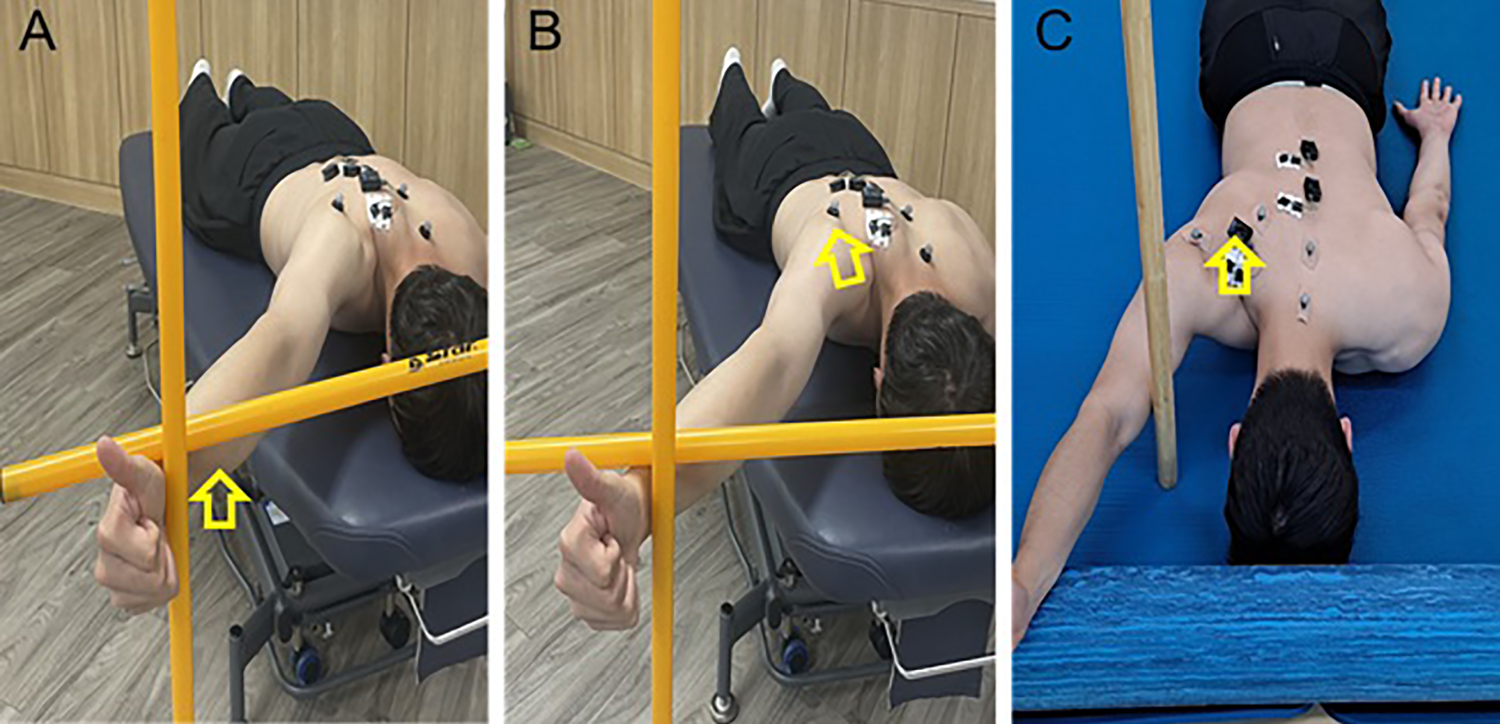
Prone Y exercise in three different conditions. A: Arm lifting condition, B: Intended scapular depression with arm lifting condition, C: Scapular depression with roller-assist condition.
Prone Y exercise for each condition.

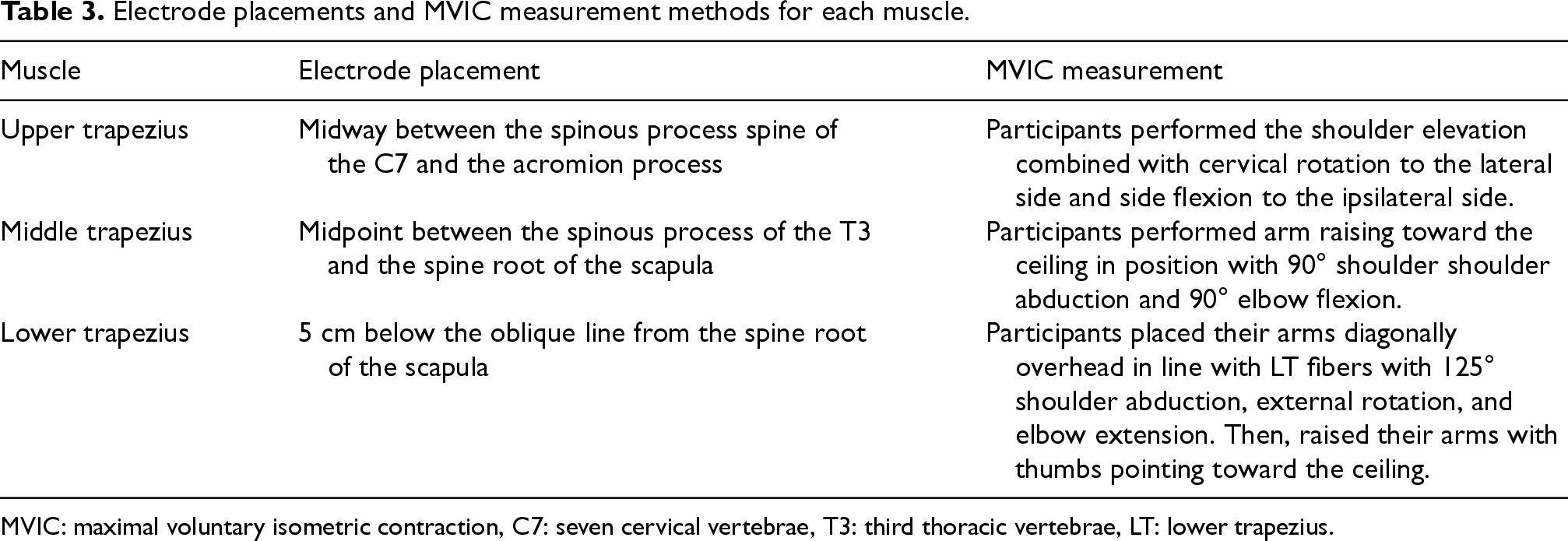
UT, MT, and LT activities were assessed in three different conditions using a surface electromyography (EMG) system (Ultium EMG system; Noraxon, Inc., Scottsdale, AZ, USA). EMG activity data were collected at 2000 Hz with a bandwidth of 10–450 Hz, were full-wave rectified, and converted to root-mean-square values with a 125-ms window length, and were analyzed using myoRESEARCH 3 software (Noraxon, Inc., Scottsdale, USA). Participants took off their shirts, and razor and alcohol swabs were used to disinfect the skin of EMG attachment sites. Electrodes consisting of two bipolar were placed 2 cm apart on each muscle fiber 30 (Table 3). Afterward, the MVIC was assessed for each muscle to normalize the data of EMG. Participants maintained maximal isometric contraction against resistance for 5 s to measure the MVIC for each muscle 31 (Table 3). MVIC was measured in three repetitions, with a 2-min rest between the trials. The average value of three repeated assessments was utilized to quantify EMG data.
Electrode placements and MVIC measurement methods for each muscle.
Electrode placements and MVIC measurement methods for each muscle.
MVIC: maximal voluntary isometric contraction, C7: seven cervical vertebrae, T3: third thoracic vertebrae, LT: lower trapezius.
The upper horizontal distance (UHD)32,33 and scapular depression angle (SDA) 34 were measured simultaneously during prone Y exercise for each condition. For measuring the UHD and SDA, photographs were taken with a smartphone in each condition. Then, images were digitized and analyzed by using an image-analyzing software Kinovea (version 0.8.15, free and open source). Before performing the prone Y exercise, reflective markers were attached to the bony landmarks of the scapular spine root, the corresponding spinous process of the thoracic vertebrae, the spinous process of the C7, and the acromion process, respectively. Then, photographs were taken with a smart phone during prone Y exercise in each condition. Once the photographs were obtained, the images were digitized and analyzed by using the image-analyzing software Kinovea. UHD was determined by measuring the distance between the spine root of the scapula and the corresponding thoracic vertebrae spinous process (Figure 2). For the SDA, was determined as the angle between the horizontal line at C7 spinous process and the line connecting C7 spinous process and the acromion (Figure 2). The intra-rater reliability of the UHD and SDA demonstrated good reliability in this study (Table 4). The difference in the UHD and SDA according to exercise conditions was analyzed using the mean value of three repeated measurements

Measurement of the scapular position. A: Upper horizontal distance, B: Scapular depression angle.
Intra-rater reliability for outcome measures of scapular upper horizontal distance and scapular depression angle.
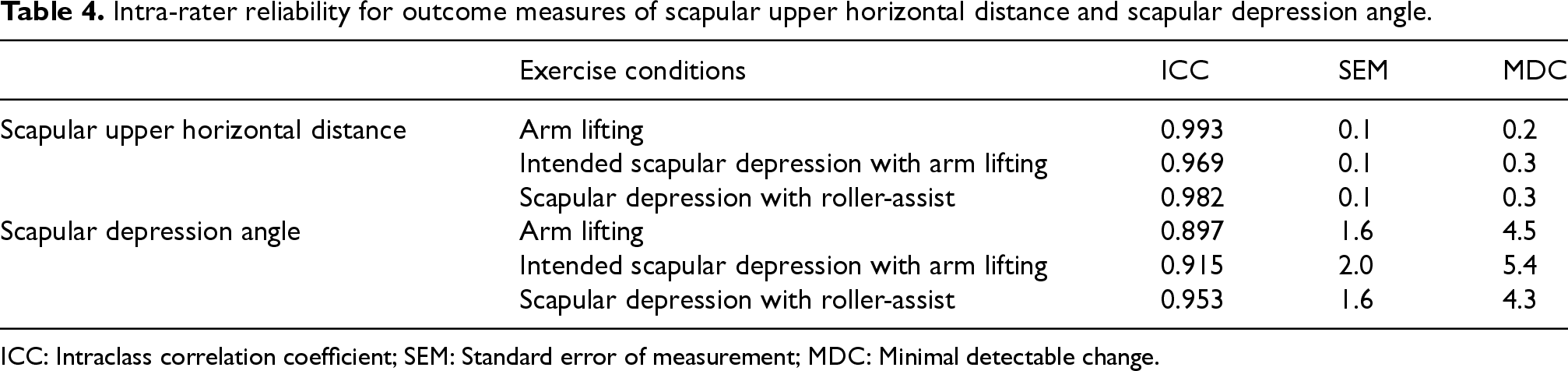
ICC: Intraclass correlation coefficient; SEM: Standard error of measurement; MDC: Minimal detectable change.
The data was analyzed using Statistical Package for the Social Sciences version 21.0 for Windows software (IBM SPSS Statistics, IBM Corporation, Armonk, NY). The Shapiro–Wilk test was conducted to check whether the data satisfied the normality. Depending on whether normality was satisfied, a One-way repeated-measures analysis of variance or Friedman test was used to determine the differences in variables between three different conditions during prone Y exercise. The Bonferroni correction and Wilcoxon signed rank test were used as a post-hoc test. The α-level was set at ≤0.05.
Results
In this study, the normality was satisfied except for UT activity and UT/LT ratio under the intended scapular depression with arm lifting condition, and UHD under the arm lifting condition.
EMG muscle activities of the scapula
EMG muscle activity of the UT
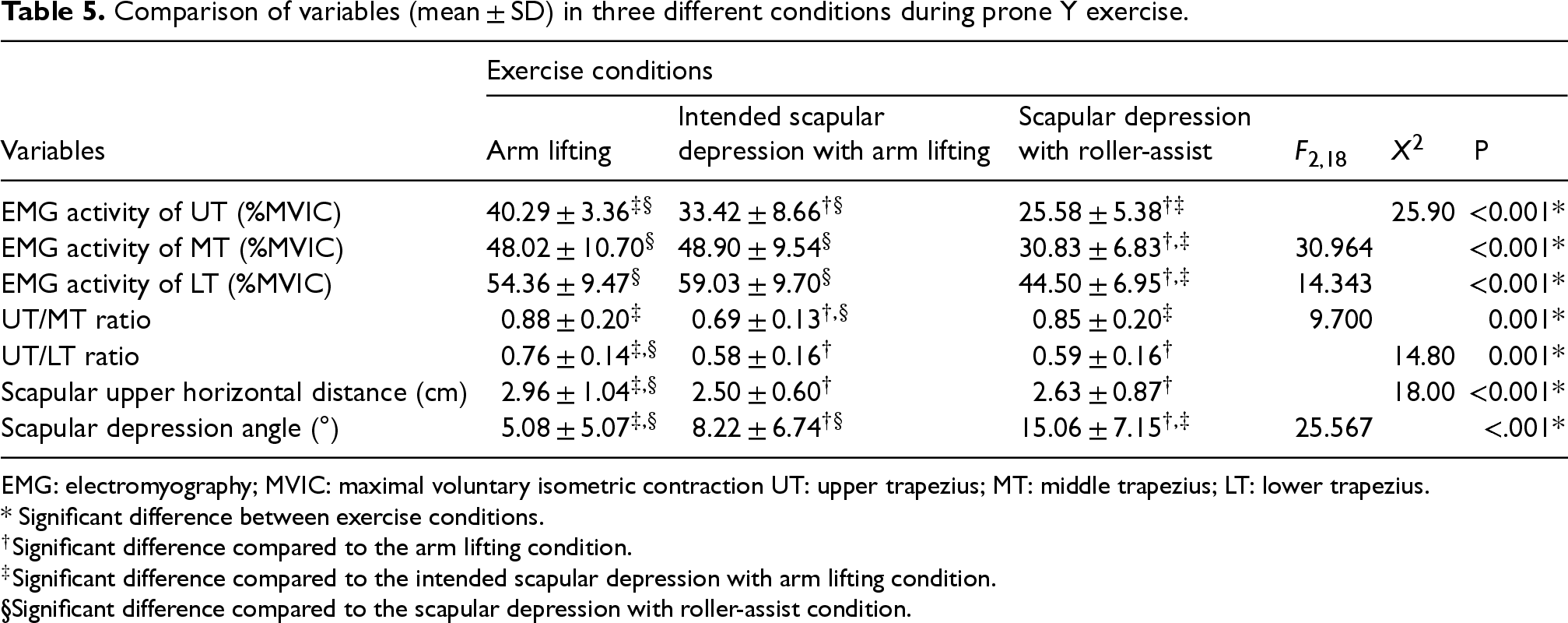
The UT activity showed significant differences between exercise conditions (x2= 25.90, p < 0.001) (Table 5). In arm lifting condition significantly increased UT activity than in both intended scapular depression with arm lifting (Z = −3.173, p = 0.002) and scapular depression with roller-assist conditions (Z = −3.920, p < .001). Also, a significantly higher in the intended scapular depression with arm lifting condition than scapular depression with roller-assist condition (Z = −2.949, p = 0.003).
Comparison of variables (mean ± SD) in three different conditions during prone Y exercise.
Comparison of variables (mean ± SD) in three different conditions during prone Y exercise.
EMG: electromyography; MVIC: maximal voluntary isometric contraction UT: upper trapezius; MT: middle trapezius; LT: lower trapezius.
* Significant difference between exercise conditions.
Significant difference compared to the arm lifting condition.
Significant difference compared to the intended scapular depression with arm lifting condition.
Significant difference compared to the scapular depression with roller-assist condition.
The MT (F2,18 = 30.964, p < 0.001) activity was significant differences between exercise conditions (Table 5). MT activity was higher in both the intended scapular depression with arm lifting (effect size [ES]: 2.12, mean difference: 18.07% MVIC, 95% CI: 12.04, 24.10; p < .001) and arm lifting conditions (ES: 1.83, mean difference: 17.18% MVIC, 95% CI: 9.61, 24.75; p < .001) than the scapular depression with roller-assist condition.
EMG muscle activity of the LT
The LT (F2,18 = 14.343, p < 0.001) activity was significant differences between exercise conditions (Table 5). LT activity was higher in the intended scapular depression with arm lifting (ES: 1.68, mean difference: 14.54% MVIC, 95% CI: 7.58, 21.49; p < .001) and arm lifting conditions (ES: 1.16, mean difference: 9.86% MVIC, 95% CI: 2.13, 17.59; p = 0.01) than the scapular depression with roller-assist condition, respectively.
UT/MT and UT/LT ratios
The UT/MT (F2,18 = 9.700, p < 0.001) and UT/LT (X2= 14.80, p < .001) ratios significantly differed among exercise conditions (Table 5). The UT/MT ratio was lower in the intended scapular depression with arm lifting condition than in the arm lifting (ES: 1.08, mean difference: −0.19, 95% CI: −0.33, −0.51; p = 0.006) and scapular depression with roller-assist conditions (ES: 0.91, mean difference: −0.16, 95% CI: −0.27, −0.06; p = 0.003). The UT/LT ratio was lower in the intended scapular depression with arm lifting (Z = −3.285, p = 0.001) and scapular depression with roller-assist conditionis (Z = −3.061, p = 0.002) than in the arm lifting condition.
Scapular positions
Significant differences in the UHD (X2= 18.00, p < 0.001) and SDA (F2,18 = 25.567, p < 0.001) among exercise conditions (Table 5). The UHD was significantly decreased in the intended scapular depression with arm lifting (Z = −3.772, p < .001) and scapular depression with roller-assist conditions (Z = −3.061, p = 0.002) than in the arm lifting condition. The SDA was significantly increased in the scapular depression with roller-assist condition than in the arm lifting (ES: 1.57, mean difference: 9.99°, 95% CI: 6.41, 13.56; p < .001) and intended scapular depression with arm lifting conditions (ES: 0.98, mean difference: 6.84°, 95% CI: 3.62, 10.07; p < .001). Also, SDA was significantly increased in the intended scapular depression with arm lifting condition than in the arm lifting condition (ES: 0.52, mean difference: 3.14°, 95% CI: 0.55, 5.74; p = 0.015).
Discussion
This study investigated the changes in trapezius muscle activities, muscle activity ratios, and scapular positions during prone Y exercise according to three different exercise conditions. Our results reveal that the intended scapular depression with arm lifting strategy increased the LT and MT activities, and SDA along with decreasing the UHD. UT/LT and UT/MT ratios were reduced in the intended scapular depression with arm lifting and scapular depression with roller-assist conditions.
The present study revealed that the LT (59% MVIC) and MT (48% MVIC) activities were highest under the intended scapular depression with arm lifting condition, and higher than the scapular depression with roller-assist condition. The UHD demonstrated the most decrease (2.5 cm) and SDA was the second greatest (8.2°) under the intended scapular depression with arm lifting condition. This result indicates that LT and MT involvement in scapular retraction and depression20,35 may have affected the increase in muscle activities under the intended scapular depression with arm lifting condition. These results are similar to previous findings, Yu and Kang 24 demonstrated that LT activity was highest as about 72% MVIC under the cues of posterior tilt of the scapula. Kim et al. 25 revealed that LT activity was highest as approximately 76% MVIC under the strategy of intended posterior tilt of the scapula. In this study, all exercises were performed combined with the shoulder external rotation. LT and MT are known to counteract the scapular destabilizing force20,36–38 and act as auxiliaries for the shoulder external rotation.20,35 Previous studies have demonstrated more increased LT and MT activities, and scapular retraction and posterior tilt during exercises accompanied by shoulder external rotation.20,23,24,36,39 In this study, LT and MT activity showed similar in arm lifting (LT activity: 54% MVIC and MT activity: 48% MVIC) and intended scapular depression with arm lifting conditions (LT activity: 59% MVIC and MT activity: 48% MVIC), and more increased than scapular depression with roller-assist condition. It is thought to be the result of the increased involvement of the LT and MT to provide scapular stability and auxiliary in both arm lifting and intended scapular depression with arm lifting conditions. Therefore, both arm lifting and intended scapular depression with arm lifting strategies are expected to effectively strengthen the LT and MT in patients with SD type I particularly, which is characterized by prominence of the inferomedial border of the scapular. However, the results of LT activity revealed a significant different between exercise conditions in this study, showed less than results of previous studies. Our study involved participants with SD, as well as arm lifting height was controlled with foam roller height but, the previous study allowed the arm to be raised as high as possible without trunk rotation and involved healthy participants without SD. Therefore, it is thought that LT activity would have differed from the previous studies.
The SDA showed a greater increase of approximately 10° and UHD lower by about 0.46 cm under the intended scapular depression with arm lifting condition compared to arm lifting condition in addition, UT activity as 33% MVIC, lower by approximately 17%. The UT hyperactivation and reduced LT activation decreased the scapular posterior tilt and upward rotation,14,15 it may cause impingement syndrome.16,17,40 A previous study by Ekstrom et al. 20 and Oyama et al., 23 demonstrated that not only LT activity but also UT activity was high during prone Y exercise, with approximately 79% MVIC and 72% MVIC, respectively. Therefore, our results suggest that intended scapular depression may be more effective in reducing UT involvement by facilitating scapular depression and retraction. Moreover, UT/LT and UT/MT ratios were significantly decreased under the intended scapular depression with arm lifting condition than the arm lifting condition by approximately 21% and 23%, respectively. In previous studies, the UT/MT ratio was found to be 0.75–0.93 and the UT/LT ratio was 0.62–1.01, during the prone Y exercise.20,22,23 These results are similar to our results in the arm lifting condition (UT/MT ratio: 0.88 and UT/LT ratio: 0.76). However, the UT/MT and UT/LT ratios were 0.69 and 0.58 in the intended scapular depression with arm lifting condition, less than the arm lifting condition. Therefore, based on our results, although LT and MT were not significantly different from the arm lifting condition, the intended scapular depression with arm lifting strategy is expected to be a more effective strategy for improving the balance of the periscapular muscles by reducing excessive UT activation and facilitating LT and MT activation in males with SD. However, since the UT/MT and UT/LT muscle activity ratios were the result of a decreased in UT activity, care must be taken not to generalize them as the result of an increase in MT and LT activity.
Among exercise conditions, the scapular depression with roller-assist revealed that the SDA was the most increased as 15.06°. This would have affected the UT activity and UT/LT ratio. The UT activity was the lowest (25% MVIC) and the UT/LT ratio was 0.59, less than in the arm lifting condition by approximately 22%. Therefore, for patients who have difficulty performing exercise or those in the early stages of rehabilitation, the scapular depression with roller-assist strategy may be expected to inhibit compensatory UT involvement and facilitate the scapular motion that is required to perform the prone Y exercise. However, in terms of strengthening the LT muscle, it is difficult to expect sufficient effect with only the scapular depression with roller assist strategy, so the LT should be strengthened gradually according to the patient's pain or exercise performance ability.
This study had some limitations. First, only the UHD and SDA were measured. Changes in other scapular kinematics, including scapular upward and downward rotation or scapular tilt angle should be considered in future research. Second, this study did not consider the results for each SD type; thus, future research is warranted to compare the differences in muscle activity and kinematics according to SD types. Finally, our results should be validated by future studies involving female participants and patients with symptomatic shoulder pathologies.
In conclusion, the intended scapular depression with arm lifting strategy is expected to LT and MT strengthening through the scapular adduction and depression in males with SD particularly. Additionally, intended scapular depression with arm lifting and scapular depression with roller-assist strategies are expected to improve the balance of the scapular muscles by decreasing ratios of the UT/MT and UT/LT.
Footnotes
Acknowledgements
We would like to thank everyone who participated in the study.
Ethical approval
The present study was approved by the Institutional Review Board of the Bioethics Committee of Pukyong National University (IRB No: 1041386-202312-HR-145-02).
Informed consent
All participants gave informed consent.
Funding
This study was supported by the Global Joint Research Program funded by the Pukyong National University (202412370001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.