
Abstract
Background
Ankle sprains are common in Taekwondo athletes and early first aid (EFA) is often overlooked.
Objective
To analyze the effect of EFA intervention on rehabilitation outcomes in young Taekwondo athletes with acute ankle sprains.
Methods
Data from 46 adolescent male Taekwondo athletes with acute ankle sprains were retrospectively analyzed. Participants underwent a 6-week standardized rehabilitation program and were divided into two groups: the EFA group received first aid within 24 h of injury, while the delayed first aid (DFA) group received first aid after 24 h. Primary outcomes included dorsiflexion range of motion (DFROM), Foot and Ankle Outcome Score (FAOS), Y-balance test (YBT) and isokinetic ankle plantarflexion and dorsiflexion strength measured at baseline and post-rehabilitation.
Results
Both groups showed significant improvements in DFROM, FAOS, YBT, and isokinetic ankle strength (p < 0.05). The EFA group exhibited significantly greater improvements in DFROM, FAOS Symptoms subscale, and YBT anterior reach distance (p < 0.05). No between-group differences were observed in isokinetic ankle strength.
Conclusions
Early first aid intervention significantly enhances specific rehabilitation outcomes, including dorsiflexion, dynamic balance, and symptom relief, following acute ankle sprains. These findings highlight the critical role of prompt first aid in optimizing recovery and minimizing complications.
Introduction
Taekwondo is a popular international sport that involves intense movements such as kicking, spinning, stepping, hopping, jumping, and landing. 1 Active movements are inherently associated with a risk of injury. Young taekwondo athletes are particularly susceptible to musculoskeletal injuries due to differences in growth rates between bone, muscle, and tendon attachments during critical developmental stages, such as rapid growth and maturation. Moreover, these risks may be further exacerbated by biomechanical factors, including decreased flexibility, coordination, and balance, which often occur during the adolescent growth spurt. 2
Especially, lateral ankle sprain (LAS) is one of the most common musculoskeletal injuries in adolescent sports, accounting for up to 40% of sports medicine clinic visits within this population. 3 Young athletes are particularly vulnerable to LAS during their developmental years, as their musculoskeletal systems are not yet fully mature. 4 In a meta-analysis, Doherty et al. 4 reported LAS incidence rates of 2.85 per 1000 exposures in children, 1.94 in adolescents, and 0.72 in adults. Supporting these findings, a Korean study revealed that 17% of young Taekwondo athletes experienced an ankle injury. 5
The higher incidence of LAS in young athletes may be attributed to several factors. First, the trend of participating in competitive sports from an early age exposes athletes to repetitive stress and overuse, inherently increasing the risk of ankle trauma. 6 Second, the ongoing physical development in young athletes, including imbalances in strength and coordination related to muscle and tendon growth, may further contribute to their vulnerability to such injuries. 7 Given the high prevalence and risk of LAS in this population, prompt and effective management of such injuries is essential to mitigate symptoms and facilitate recovery. Immediate first aid is known to play a pivotal role in reducing the severity of injury outcomes. 8 However, despite the established effectiveness of early intervention, a lack of awareness about the importance of prompt first aid persists among young athletes, particularly in school sports settings. 9 Factors such as limited knowledge among coaches, inadequate access to medical personnel or resources, and underestimation of injury severity by the athletes themselves contribute to this problem. These oversights can result in prolonged recovery times, increased discomfort, and a higher likelihood of subsequent re-injury. 10
Range of motion (ROM), strength, and dynamic balance are critical factors in the rehabilitation of acute ankle sprains, as they directly influence functional recovery and an athlete's ability to return to play. Reduced ROM may limit joint mobility, impairing performance and increasing susceptibility to further injury. 11 Strength deficits in the muscles surrounding the ankle compromise joint stability and proprioception, potentially delaying recovery and increasing the risk of re-injury. 12 Dynamic balance, which requires the integration of flexibility, strength, and coordination, is vital for maintaining postural stability during sports activities and preventing subsequent injuries. 13 Understanding how early first aid intervention impacts these rehabilitation outcomes can provide valuable insights into optimizing recovery protocols.
Considering the impact of LAS and the critical window for effective treatment, it is necessary to investigate how early first aid affects recovery outcomes. While previous studies have emphasized the importance of post-LAS management, most have focused on the recovery process and the effects of interventional rehabilitation. However, the outcomes of timely implementation of first aid protocols immediately after injury remain underexplored.14,15 While the PRICE (Protection, Rest, Ice, Compression, Elevation) protocol is widely recommended for acute injury care, its impact on rehabilitation outcomes in young athletes remains unclear. 16 Moreover, the growing trend of early sports specialization has led to an increased risk of LAS in young athletes due to the repetitive stress and biomechanical challenges associated with their developmental stage. 17 Addressing this gap is critical to optimizing recovery and preventing long-term complications in this vulnerable population.
Therefore, this study investigates the effects of early first aid intervention on rehabilitation outcomes in adolescent Taekwondo athletes with acute ankle sprains. Specifically, it compares early first aid (EFA) and delayed first aid (DFA) groups in terms of ankle ROM, subjective symptom scores, dynamic balance, and isokinetic ankle strength, providing insights into the importance of timely intervention for optimal recovery. By specifically targeting the acute phase of LAS, this study addresses a critical gap in sports medicine research and advances the understanding of how the timing of first aid influences rehabilitation outcomes, unlike prior research that emphasizes general rehabilitation strategies.
Materials and methods
Participants
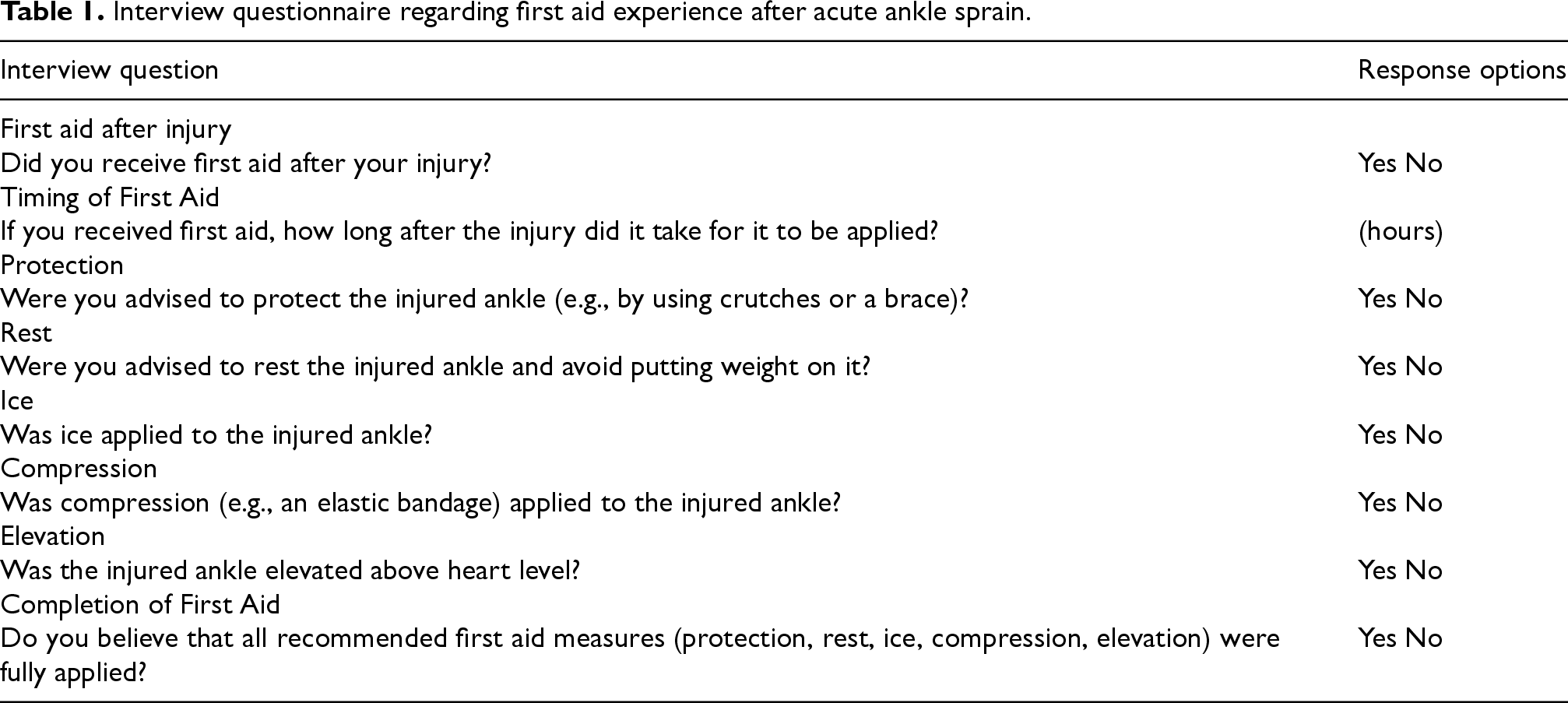
The sample size for the study was determined using the G*power analysis program (G*power 3.1.9.4, University of Düsseldorf, Düsseldorf, Germany). The number of participants required was calculated to be 46 when the effect size was 0.25 and power was 90%. The data selected were adolescent male Taekwondo athletes aged 15 to 18 years who returned to play after 6 weeks of rehabilitation due to ankle sprain. They visited a sports rehabilitation center and received physical examinations and radiological examinations by an orthopedic specialist. The exclusion criteria included previous ankle surgery, a history of ankle sprain within the previous 6 months, fractures, and other lower extremity injuries that could impact rehabilitation outcomes. The first aid experiences of participants were thoroughly investigated through interviews to determine whether and when they were provided first aid. The questionnaire assessed whether or not participants had received first aid services, the time elapsed before receiving first aid after the injury, and the specific details of the first aid administered (Table 1).
Interview questionnaire regarding first aid experience after acute ankle sprain.
Interview questionnaire regarding first aid experience after acute ankle sprain.
Participants were retrospectively categorized based on whether they received first aid following the PRICE protocol after their initial injury. This protocol is widely recommended as the standard first aid treatment for LAS, aiming to reduce swelling, relieve pain, and promote healing during the acute phase. 16 Patients were classified to the EFA group (n = 23) if they were provided first aid that fully complied with the PRICE protocol within 24-h after experiencing an ankle sprain. Participants who had at least one component of the PRICE protocol implemented more than 24-h after the injury were classified to the DFA (n = 23). Although it is ideal to apply first aid immediately (within the first hour after injury), the present study sought to adopt a pragmatic approach in classifying early and delayed intervention. For this purpose, immediate first aid was defined as intervention within 24-h after injury, when the acute inflammatory response peaks. 18 All participants in the EFA and DFA groups followed an identical 6-week rehabilitation program and were retrospectively analyzed after returning to play. This study complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Gangneung-Wonju National University (2024–66).
The ankle dorsiflexion range of motion (DFROM) of participants was measured using a universal goniometer (Baseline® Model 12-1000, Fabrication Enterprises Inc., White Plains, NY, USA) and a weight-bearing lunge test (WBLT) (Figure 1A). The ROM was measured using the goniometer by placing the stationary arm parallel to the floor, and aligning the moving arm with the fibula, while the fulcrum was placed at the center of the lateral malleolus. The WBLT was performed with the participant in a standing position, ensuring that the heel remained in full contact with the floor throughout the test. The participant's knee was aligned with the index (second) toe, and the hallux (big toe) was positioned 10 cm from the wall. Participants were instructed to slowly lunge forward, directing the knee toward the wall until it contacted the wall. The participant's foot was moved 1 cm further away from the wall at a time, and the lunge was repeated until the knee could no longer reach the wall without lifting the heel off the ground. The assessor monitored heel contact by lightly placing a finger on the heel to detect subtle movements and visually inspecting for heel lift. ROM was measured using the goniometer at the final lunge position when maximal ankle dorsiflexion was achieved. To minimize variability, the assessment was conducted under standardized conditions in a quiet laboratory environment, with consistent lighting and minimal external distractions. Participants were allowed three practice trials to familiarize themselves with the procedure before testing. During the measurement phase, three consecutive tests were performed, with the participant returning to a neutral standing position between each test. The average of the three measurements was used in the analysis to ensure reliability. The goniometer was calibrated prior to each session to confirm accurate readings. Participants performed the test barefoot to prevent any external influence from footwear. The testing area was marked to ensure consistency in foot positioning across trials. All measurements were performed by the same trained examiner to reduce inter-rater variability.
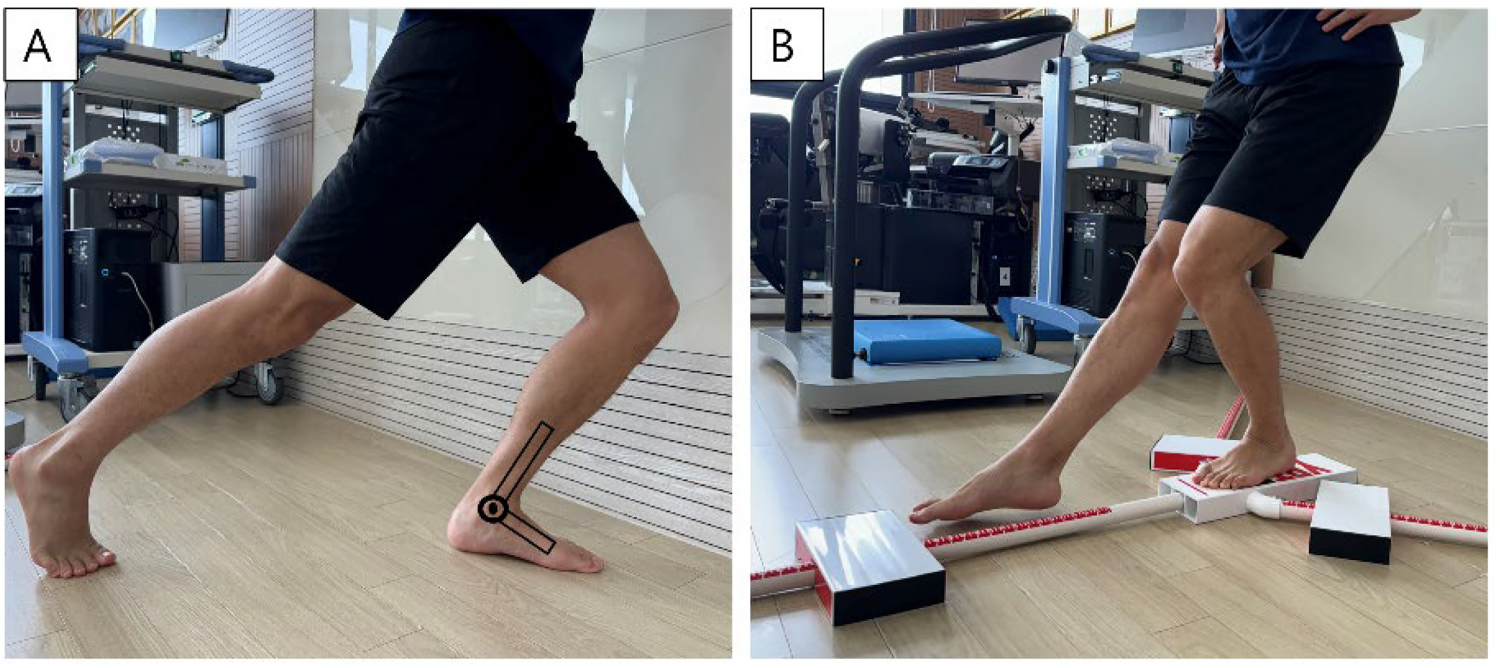
Ankle tests. A, Ankle dorsiflexion range of motion; B, Dynamic balance test.
The Foot and Ankle Outcome Score (FAOS) was used to assess the subjective symptoms and functions of the participants. 19 The FAOS is a clinical questionnaire designed for subjective self-assessment by physically active patients with symptoms and functional limitations of the foot and ankle. Its wide applicability to foot and ankle pathology has been verified in various studies.19,20 The FAOS is subdivided into 42 items comprising five subscales: Symptoms, Pain, Activities of daily living (ADL), Sport and recreation function, and Quality of life (QOL). Each item is scored on a 5-point Likert scale from 0 to 4, and the scores for each subscale are normalized to a percentage. A high score indicates no symptoms or functional limitations in the foot and ankle, and no restrictions on activities and sports. During the data collection process, the examiner explained the purpose and content of the FAOS to the participants and provided them with a pen and a questionnaire. The participants were given sufficient time and a private setting to complete the assessment independently. The examiner ensured that participants fully understood each question by providing clarifications when needed, without influencing their responses. All participants completed the questionnaire in a quiet room to minimize distractions, and responses were collected immediately after completion to ensure data integrity. The questionnaires were reviewed by the examiner for completeness before participants left the testing area.
Dynamic balance
To evaluate postural stability, dynamic balance was measured using the Y-balance test (YBT) kit (Y Balance Test™, Move2Perform, Evansville, IN, USA) (Figure 1B). The YBT is a dynamic balance test that requires flexibility, strength, stability, and proprioception of the lower extremities, including the ankle. 21 After a skilled examiner demonstrated the correct test posture and movement sequence, sufficient practice time was provided to the participants. After completing the practice, the participants stood upright with one foot on the stance plate at the center of the device and performed a one-legged stance. Subsequently, while maintaining balance, the participants extended the opposite leg as far as possible, and sequentially pushed the indicator box in the anterior, posteromedial, and posterolateral directions with the tip of their toes. During the measurement, if the foot pushing the indicator box touched the ground or the heel of the standing foot came off the stance plate, remeasurement was performed. After measuring the continuous reaching movements in the three directions twice on each leg, the better record for each leg was used for analysis. The absolute reach distance measured in each direction was recorded in centimeters and normalized to a relative reach distance as a percentage by applying leg length. The participant's leg length was measured in centimeters as the distance between the anterior-superior iliac spine of the pelvis and the medial malleolus of the ankle. All measurements were conducted in a quiet laboratory environment to minimize external distractions. The examiner ensured consistent verbal instructions were provided before each measurement. Participants were instructed to wear tight-fitting clothing and remove shoes to avoid measurement interference. Before each trial, the stance foot position was marked on the stance plate to ensure consistency across measurements. Any deviations in body posture or compensatory movements were noted by the examiner, and trials were repeated if necessary. The normalized reach distances were calculated using the formula: (reach distance/leg length) × 100%.
Isokinetic ankle strength
To assess the isokinetic ankle plantarflexion and dorsiflexion strength of the participants, an isokinetic dynamometer (Humac Norm, Stoughton, MA, USA) was used. The participant lay on an examination chair in a supine position, the foot was fitted with an ankle joint examination adapter and fixed using a cross strap. The distal thigh was placed on a support and secured with a strap. The ROM of the ankle joint was set to relative to the neutral position, and 40° for plantarflexion, and −20° for dorsiflexion (a total 60°). An experienced examiner demonstrated the test method to the participants, and sufficient practice was allowed. After two practice runs for each measurement, the participants performed the main test four times. To ensure the reliability of the test results, the muscle strength of the uninvolved ankle was measured first, followed by the muscle strength of the involved ankle. The measured peak moment values were recorded in Nm. All measurements were conducted in a quiet laboratory environment to minimize external variables. The examiner provided standardized verbal instructions before each trial, including cues to encourage maximal effort while avoiding compensatory movements. Participants were instructed to avoid vigorous physical activity for 24 h prior to testing to ensure consistent baseline conditions. The test chair and dynamometer settings, including seat height and ankle attachment alignment, were individually adjusted and documented for each participant to ensure consistency across trials. Any deviations in posture or incorrect movements during testing were noted by the examiner, and the trial was repeated if necessary. Torque values were automatically calculated and stored by the dynamometer software for subsequent analysis.
Rehabilitation program
The rehabilitation program followed the same protocol for both the EFA and DFA groups (Table 2) and was developed based on evidence-based guidelines for ankle sprain management and recovery to optimize functional outcomes and reduce the risk of re-injury. 22 This structured approach incorporates progressive weight-bearing, range of motion exercises, and functional training tailored to the healing phases of the injury. After the ankle joint was immobilized using a splint, the participant performed partial weight-bearing using crutches for 2 weeks after the injury. From the third week, a soft brace was worn, and participants gradually transitioned to full weight-bearing as tolerated. From the fifth week, the soft brace was removed, and light jogging was allowed. Sessions were held three times per week over the 6-week period, with warm-up and cool-down of 20 min per session and the main exercises for 40 min, accounting for a total of 60 min. The warm-up and cool-down consisted of aerobic exercises for 10 min each, and the rehabilitation protocol gradually progressed to stationary biking, ellipticals, and treadmill running. Considering the tissue healing process during the subacute period, ankle ROM exercises were performed for 2 weeks except for inversion, and ROM in all planes was allowed from the third week. Isometric exercises were performed in all planes for 2 weeks to minimize muscle weakness. From the third week, isotonic exercises using elastic bands were allowed, and balance exercises were performed progressively from stable to unstable surfaces. From the fifth week, practice-based hopping and ladder drills were performed in multiple directions at varying speeds to prepare for return to sports. To ensure consistency, exercise intensity and progression were standardized. Isometric exercises were held for 5 s per repetition, with 10 repetitions performed in three sets per session. For isotonic strengthening exercises, elastic bands with a resistance of 1.7–2.1 kg at 100% elongation (2x original length) were used. Resistance was adjusted progressively within this range over the course of the program to match each participant's capacity and recovery phase. Balance exercises included single-leg stances on stable surfaces for 30 s per leg, progressing to dynamic movements on unstable surfaces (e.g., balance boards). Ladder drills incorporated linear and lateral movements, with participants performing three sets of 10 repetitions per direction. All sessions were supervised by a trained physical therapist to ensure proper technique and minimize the risk of re-injury. Each participant's progress was documented using an individualized exercise log, which recorded the intensity, duration, and feedback from each session. Modifications were made if participants reported pain or discomfort, and resistance or exercise difficulty was adjusted accordingly. These measures ensure the reproducibility and safety of the rehabilitation protocol.
Rehabilitation protocol.

Rehabilitation protocol.
* AROM, active range of motion; AAROM, active assisted range of motion; EV, eversion; IV, inversion; PF, plantarflexion; DF, dorsiflexion.
Data analysis was conducted using SPSS Statistics version 25.0 for Windows (IBM Corp., Armonk, NY, USA). Continuous variables are presented as means and standard deviations, and categorical variables are presented as numbers and percentages. The Kolmogorov–Smirnov test was used to determine normality of the main variables. For the general characteristics of the participants, independent t-test (age, height, weight, BMI, career, and time to first aid) and chi-square test (involved side, and dominant side) were performed. The major analysis according to the theme of this study was conducted by two-way repeated measures analysis of variance (ANOVA) to confirm the main effect and interaction effect between time and group. In addition, the difference (%) was calculated to observe the change rate between baseline and 6 weeks. The significance level was set at p < 0.05.
Results
General characteristics of participants
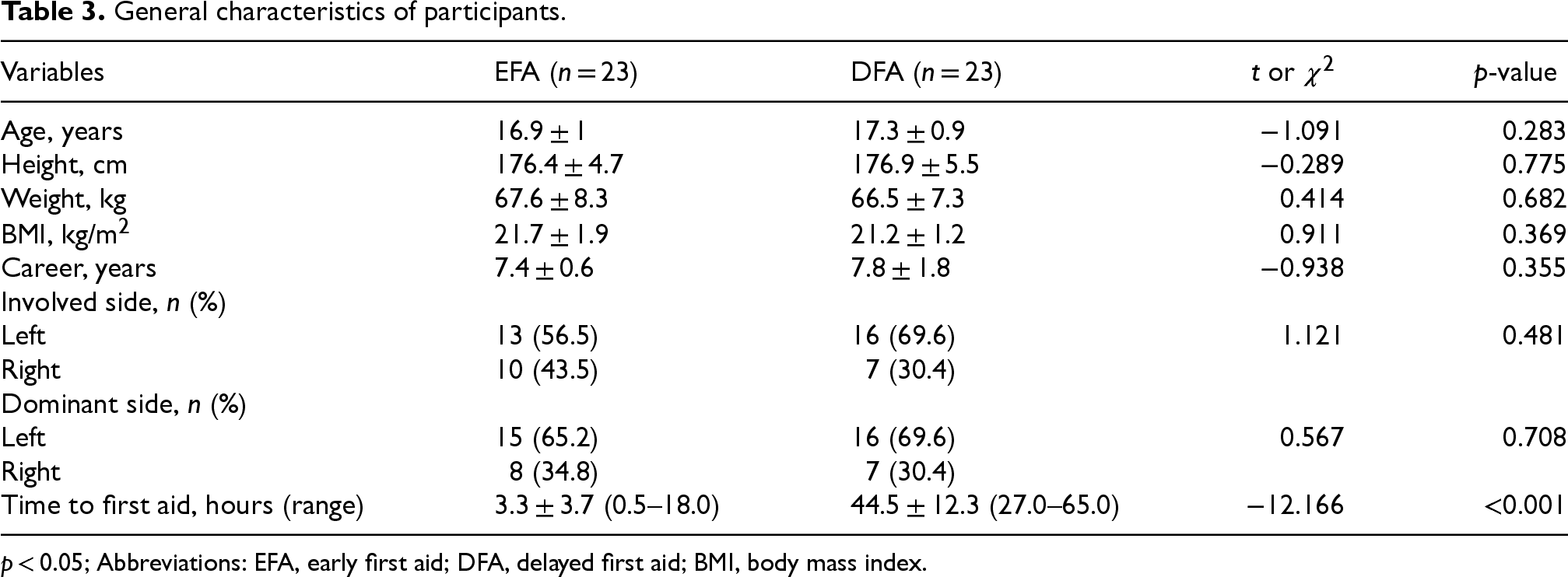
Table 3 presents the general characteristics of the participants, who were classified into the EFA and DFA groups. There were no statistically significant differences between the two groups in age, height, weight, or body mass index (p > 0.05). An independent t-test analysis was performed to compare the time taken to receive first aid after injury, and there was a significant difference between EFA and DFA (p < 0.001).
General characteristics of participants.
General characteristics of participants.
p < 0.05; Abbreviations: EFA, early first aid; DFA, delayed first aid; BMI, body mass index.
Table 4 presents the results of the WBLT for ankle DFROM. The interaction effect by time and group was significant (p < 0.05), indicating that changes in DFROM over time differed between the EFA and DFA groups. The main effects were also significant for both time and group. These results indicate that the EFA group showed significantly greater improvement in DFROM than the DFA group after 6 weeks of rehabilitation (p < 0.05), suggesting the benefits of early first aid intervention on ankle ROM.
Change of weight-bearing lunge based on groups (unit: degree).

Change of weight-bearing lunge based on groups (unit: degree).
p < 0.05; Abbreviations: EFA, early first aid; DFA, delayed first aid, ROM, range of motion.
Table 5 presents the results of the FAOS evaluations for subjective ankle scores. A significant interaction effect between time and group was observed in the Symptoms (p < 0.05), indicating that changes in Symptoms scores over time differed between the EFA and DFA groups. Main effects analysis revealed that both the EFA and DFA groups demonstrated significant improvements across all five FAOS subscales (Symptoms, Pain, ADL, Sport and Recreation Function, QOL) after 6 weeks of rehabilitation (p < 0.05). However, the EFA group achieved significantly higher scores in the Symptoms compared to the DFA group (p < 0.05).
Change of the foot and ankle outcome score based on group (unit: score).

Change of the foot and ankle outcome score based on group (unit: score).
p < 0.05; Abbreviations: EFA, early first aid; DFA, delayed first aid.
Table 6 presents the results of the YBT for dynamic balance. A significant interaction effect between time and group was observed in the anterior reach distance (p < 0.05), indicating that EFA group showed significantly greater improvement in the anterior reach distance compared to the DFA group (p < 0.05). The main effect analysis results showed that there was a significant difference in time, but not in group.
Change of dynamic balance based on groups (unit: cm).

Change of dynamic balance based on groups (unit: cm).
p < 0.05; Abbreviations: EFA, early first aid; DFA, delayed first aid.
Table 7 presents the results of isokinetic ankle strength measurements, including pre- and post-rehabilitation changes and between-group differences. Both the EFA and DFA groups demonstrated increases in the isokinetic strength of the plantarflexion, and dorsiflexion after 6 weeks of rehabilitation. Thus, the main effect results were significant for time (p < 0.05), but there was no difference between groups (p > 0.05). Accordingly, in this study, no interaction effect by group and time was observed for plantarflexion and dorsiflexion muscle strength. These findings suggest that the timing of first aid intervention does not differentially affect isokinetic strength outcomes.
Change of isokinetic ankle strength based on groups (unit: nm).

Change of isokinetic ankle strength based on groups (unit: nm).
p < 0.05; Abbreviations: EFA, early first aid; DFA, delayed first aid; Nm, Newton meter.
Ankle sprains are prevalent among Taekwondo athletes due to the sport's dynamic movements. 23 This study highlights the critical role of timely first aid intervention in improving rehabilitation outcomes following such injuries.
The results of our study demonstrate significant improvements in ankle dorsiflexion after 6 weeks of rehabilitation in both the EFA and DFA groups. However, the EFA group, which received PRICE immediately after injury, showed more pronounced improvement. These findings align with the umbrella review by Gaddi et al. 16 that emphasized the effectiveness of early first aid protocols, such as PRICE, in controlling inflammation, preventing secondary complications, and accelerating recovery to enhance functional outcomes. Collectively, the evidence underscores the critical role of timely first aid in mitigating inflammatory responses, facilitating comprehensive functional recovery, and enabling a quicker return to pre-injury activities.24,25 The PRICE components, particularly the prompt application of ice and compression, play a crucial role in controlling acute inflammation associated with ankle sprains. 26 By effectively managing these symptoms, timely first aid not only supports earlier participation in rehabilitation activities, such as ROM exercises and strength training, but also helps prevent complications like tissue adhesions and joint stiffness.24,25
However, while these interpretations align with prior study, 16 further research is necessary to establish the causal mechanisms and long-term effects of early intervention. Ankle dorsiflexion plays a critical role in functional recovery following LAS because it directly impacts the ability to perform tasks involving the lower leg. During the midstance and terminal stance phases of gait, the tibia rolls over the supporting foot and dorsiflexes the ankle joint by approximately 10°, which in turn contributes to forward movement of the body 27 . Therefore, dorsiflexion is essential for normal gait, especially during the stance phase of walking and running, enables proper heel strike and weight distribution through the foot. 28 However, alterations in biomechanics after injury increase the risk of re-injury due to compensatory movements. 11
The greater improvement in DFROM in the EFA group suggests that rapid first-aid intervention may facilitate a faster return to normal activities and reduce the risk of compensatory movements that may lead to further injury. All subscale scores of the FAOS used to assess subjective ankle scores significantly improved after 6 weeks of rehabilitation in both the EFA and DFA groups. 19 In particular, the EFA group exhibited better results in the subscales related to ankle symptoms. These findings suggest that timely first aid intervention effectively mitigates acute inflammatory responses, reducing mechanical and sensory restrictions on the joint. The symptom-related subscales of the FAOS include questions related to swelling, joint noises (like grinding or clicking), catching or hanging, and restrictions on movements that fully straighten or bend the ankle. 19 The greater improvement in symptom-related subjective ankle scores observed in the EFA group provides meaningful insight into the subjective experiences of athletes during rehabilitation after acute ankle sprains. The improved scores related to swelling suggest more effective edema management in the EFA group, which may be a result of timely first aid intervention to minimize the acute inflammatory response. Swelling is closely related to joint mobility, including DFROM, as it can mechanically limit joint movement by increasing stiffness and pain. 29 The reduction of mechanical restrictions to ankle joint movement may result in smoother and more coordinated movements during activities and reduce the perception of grinding, clicking, or other noises associated with joint movement. 30 The fact that the EFA group achieved significantly better results in these areas reinforces the notion that early first aid intervention after LAS may result in better subjective outcomes.
Dynamic balance is critical for various daily activities and sports, and requires coordinated motor response and stabilization in various aspects. 31 The findings of this study demonstrate significant improvements in maximal reach distances across all three directions of the YBT, reflecting enhanced dynamic balance in both the EFA and DFA groups after 6 weeks of rehabilitation. These results underscore the effectiveness of the rehabilitation protocol in promoting overall balance and stability. Notably, the EFA group exhibited significantly greater improvement in the anterior reach distance, highlighting the potential advantages of timely first aid intervention in addressing mechanical restrictions and optimizing balance-related performance. This better performance emphasizes the benefit of immediate and comprehensive first aid in improving dynamic balance in the anterior reach direction. In a previous study, Gabriner et al. 32 investigated the factors contributing to YBT performance in 40 individuals with chronic ankle instability, and reported that the anterior reach distance was more affected by mechanical restrictions and sensory deficits of the ankle complex, whereas the posteromedial and posterolateral reach directions were more dependent on muscle strength and postural control. This suggests that the anterior reach is closely related to the ability of the foot standing on the support to control the center of gravity of the body while the contralateral lower extremity is propelled forward. Terada et al. 33 emphasized the importance of ankle dorsiflexion for effective anterior reach in dynamic balance assessment. Since the anterior reach direction mainly performs the movement in the sagittal plane while the tibia translates above the foot, any mechanical restriction of dorsiflexion significantly impairs performance 11 . In the aforementioned study on ankle dorsiflexion, the EFA group exhibited greater improvement in DFROM than the DFA group, which may have contributed to maintaining ankle mobility and function and improving dynamic balance.32,33
In the present study, both the EFA and DFA groups demonstrated significant improvements in isokinetic strength (plantarflexion, and dorsiflexion) after 6 weeks of rehabilitation. However, no significant differences were observed between the groups. This finding suggests that the standardized rehabilitation protocol was effective in restoring ankle muscle strength, regardless of the timing of first aid. The observed improvements likely reflect the structured progression of resistance training, which promotes hypertrophy and neuromuscular adaptation through consistent application. 34 Previous research has consistently highlighted muscle weakness around the ankle joint as a critical consequence of acute ankle sprains. Perron et al. 35 examined the maximal torque of the muscles surrounding the ankle joint in 36 soldiers diagnosed with LAS and reported significant strength deficit in the plantarflexion that persisted for up to 6 months after injury. Similarly, Cho et al. 36 identified a significant association between peroneal strength deficits and functional ankle instability in 42 patients undergoing surgical reconstruction of the lateral ligaments. Chronic ankle instability, characterized by recurrent sprains, discomfort, and instability, is often linked to unresolved strength deficits. 12 In contrast to these findings, our study demonstrates that a structured rehabilitation protocol can effectively restore ankle muscle strength within 6 weeks, thereby reducing the risk of long-term functional deficits. However, the lack of group differences indicates that early first aid does not appear to provide an additional benefit for isokinetic strength outcomes. This result may suggest that the primary benefits of timely first aid lie in mitigating inflammatory responses and facilitating recovery in other domains, such as range of motion and dynamic balance.
Despite the important findings, this study has several limitations. The relatively small sample size impedes generalization of the results to a broader demographic of young athletes, especially considering potential variability in age, gender, and skill level among the target population. Additionally, the reliance on self-reported data regarding the timing and application of first aid may have introduced potential bias, as participants’ recollections might not always accurately reflect actual practices. Furthermore, the use of subjective measures such as the FAOS may be influenced by individual perception and reporting bias, highlighting the need for complementary objective measures to validate subjective outcomes. The study defined the timing of early first aid as within 24-h after injury, which may not have captured the subtle effects of very early intervention (e.g., within the first hour) and later interventions. Moreover, the severity of symptoms was not taken into account. Perhaps, it cannot be ruled out that the EFA group had severe pain and requested active medical assistance. This limitation restricts a comprehensive understanding of the time-dependent efficacy of first aid interventions. Therefore, future studies should address these limitations and investigate more subtle time intervals of first aid intervention to provide clearer guidance on the specific components and optimal timing of implementing first aid after injury.
Conclusion
This study highlights the importance of timely first aid intervention, particularly the implementation of the PRICE protocol, in improving rehabilitation outcomes following LAS in adolescent Taekwondo athletes. The findings demonstrate that early intervention not only enhances ankle dorsiflexion but also contributes to better dynamic balance and subjective ankle scores, suggesting its comprehensive benefits in both functional and symptomatic recovery. Both EFA and DFA groups benefited from the structured rehabilitation protocol, but the additional gains observed in the EFA group emphasize the critical role of mitigating acute inflammation through immediate care. While these results underscore the effectiveness of the PRICE protocol in the acute phase of LAS recovery, the study also identifies areas for further investigation. Future research should explore variations in the timing of first aid and its impact on long-term outcomes, as well as the specific mechanisms through which early intervention accelerates recovery. Furthermore, coaches, trainers, and other sports-related staff should be proficient and equipped to promptly provide first aid to injured athletes, as their actions are critical to ensuring effective acute injury management.
Footnotes
Abbreviations
Acknowledgements
We would like to thank Gangneung-Wonju national university for editing and administrative support. All authors agreed on this content.
Ethical considerations
This study was approved by the Research Ethics Committee of the Gangneung-Wonju National University (2024-66). Informed consent was obtained from all the participants and their legal guardians.
Author contributions/CRediT
YK and YP—conceptualization, revision writing, supervision. HW and MC—methodology, formal analysis. HW—investigation. HW and YK and MC—original draft writing. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
Funding
This research did not receive any funding.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data presented in this study are available on request from the corresponding author.