
Abstract
Background
Athletes widely consume caffeine to enhance exercise performance due to its potential effects on metabolism and the central nervous system. While moderate-to-high doses of caffeine (≥5 mg·kg−1) have been extensively studied, research on the acute impact of low-dose caffeine intake (≤3 mg·kg−1), particularly in coffee form, on isokinetic strength performance remains limited.
Objective
The current study aimed to examine the acute effects of low-dose caffeine consumption (1.5 mg·kg−1 and 3 mg·kg−1) in coffee form on isokinetic knee strength performance in physically active males.
Methods
Thirteen physically active male university students (age: 20.75 ± 0.96 years; height: 177.08 ± 4.07 cm; body mass: 69.91 ± 5.56 kg) participated in a double-blind, randomized, crossover study. Participants consumed either 1.5 mg·kg−1 or 3 mg·kg−1 of caffeine in coffee form or a placebo (decaffeinated coffee) 60 min before testing attempts. Single-leg isokinetic knee strength was assessed at two angular velocities (60°/s and 180°/s) using an IsoMed 2000 dynamometer. Peak moment, total work, and rate of perceived exertion (RPE) were recorded and analyzed.
Results
No statistically significant differences were observed between the caffeine and placebo conditions in terms of peak moment or total work at either angular velocity (p > 0.05). Effect sizes were small (
Conclusion
Acute low-dose caffeine supplementation in coffee form does not significantly enhance isokinetic knee strength or alter perceived exertion in physically active males.
Introduction
Caffeine and caffeine-containing products are widely used by athletes to enhance performance during competitions or training, stemming from the belief that caffeine intake may influence energy metabolism1–3 and mitigate pain perception by affecting adenosine-related neural transmission processes in the central nervous system (CNS).2,4–6 In addition to its metabolic and CNS effects, caffeine has been investigated for its role in enhancing various physiological and psychological parameters that contribute to athletic performance. Research indicates that caffeine enhances various cognitive functions, including attention, vigilance, and reaction time—key factors in high-intensity competitive environments.7,8 Furthermore, it may mitigate the sensation of exertion, enabling athletes to sustain peak performance levels for extended periods.9–11
Some studies have shown that the effect of caffeine intake on physical performance may vary depending on individual dose-dependent responses,11–13 as well as factors such as sex differences and habitual caffeine consumption. 14 To date, most of the literature has focused on examining the effects of caffeine on aerobic15–17 and anaerobic performance.18–20 However, recent publications regarding its impact on muscle strength and power output remains unclear, with studies yielding controversial results.11–13,21 The majority of studies in the literature have focused on the effects of moderate-to-high doses of caffeine supplementation (5–13 mg·kg−1) on physical performance.22,23 In contrast, research examining the impact of low-dose caffeine (≤3 mg·kg−1) consumed in coffee form remains limited.24,25 A meta-analysis of published studies indicates that improvements in isokinetic strength performance have typically observed with caffeine doses ranging from 3 to 6 mg·kg−1. 26 However, no studies have investigated the effects of acute caffeine supplementation in coffee form at a dose of 1.5 mg·kg−1.
Low-dose caffeine supplementation was chosen in this study due to the potential gastrointestinal distress associated with moderate and high doses. Additionally, caffeine administration in coffee form was preferred for its practical applicability to athletes and support personnel. Accordingly, two different caffeine doses—1.5 mg·kg−1 and 3 mg·kg−1—were administered. This study hypothesized that acute low-dose caffeine supplementation in coffee form would be sufficient to induce a dose-dependent improvement in single-leg isokinetic strength performance in physically active males.
Methods
Participants
Thirteen physically active male university students (age, 20.75 ± 0.96 years; height, 177.08 ± 4.07 cm; bod mass, 69.91 ± 5.56 kg) participated in the study voluntarily. The study protocol was approved by the Ethics Committee of Trabzon University (2024-11/2.1) and conducted in a double-blind, randomized, crossover repeated measures study design. All the procedures were implemented in compliance with the Declaration of Helsinki.
A priori power analysis was conducted using G*Power 3.1 to determine the required sample size for detecting statistically significant differences in isokinetic strength performance following caffeine supplementation. Based on previous studies examining the effects of caffeine on strength performance, an effect size (f) of 0.25 (moderate) was assumed, with an alpha level of 0.05, a power (1-β) of 0.80, and a within-subject design (repeated measures ANOVA, three conditions: 1.5 mg·kg−1, 3 mg·kg−1, placebo). The analysis estimated that a minimum of 12 participants was necessary to achieve adequate statistical power. The inclusion criteria for the study were defined as; being over the age of 18, engaging in a minimum of 4 h of exercise/training per week on at least 3 days, having no musculoskeletal injuries in the past 6 months, not using any medication, and having no chronic disease. All participants were convened 15 days before the commencement of the tests, during which they were provided with detailed information about the study. After the necessary explanations were given, participants were asked to read and sign the informed consent form to provide their consent. Participants were informed that they should refrain from consuming any nutritional ergogenic aids and caffeinated beverages from the day of the meeting until the end of the research period. Additionally, participants were instructed to avoid strenuous physical activity for 48 h before each test, refrain from consuming alcoholic beverages within 24 h, and avoid any food or beverage other than water for 12 h before the test. All tests were conducted with each participant tested at the same time on each testing day to avoid diurnal variations. The participants’ height and body weight were measured during their first visit, conducted for familiarization purposes.
One participant left the study because of an upper respiratory tract infection before the second visit to the laboratory. Therefore, statistical data analysis was performed for twelve participants.
Procedure
Caffeine and placebo supplementation
Studies in the literature on caffeine intake generally focus on isolated caffeine supplementation. The current study aimed to evaluate the acute effect of caffeine, consumed in coffee form, on physical performance. Grgic et al. 11 also recommended caffeine intake in coffee form with a matched dose for caffeine supplementation up to 9 mg·kg−1 60 min before exercise or testing. Following the laboratory analysis findings reported by Karayiğit et al., 13 the caffeinated and decaffeinated coffee supplements were prepared accordingly. Nescafé Gold was used for the 3 mg/kg intervention, while the 1.5 mg/kg intervention involved a blend of 1.5 mg Nescafé Gold and 1.5 mg Decaf Nescafé Gold to ensure the same taste. For the placebo group, a dose of 3 mg Decaf Nescafé Gold per kilogram of body weight was calculated and administered. In the present study, participants consumed doses of 1.5 and 3 mg·kg−1 caffeine in coffee form or decaffeinated coffee as a placebo mixed with 300 ml hot water, within ten minutes, 1-h before the testing sessions. Participants were scheduled for test days using a randomized crossover study design, receiving either 1.5 mg·kg−1, 3 mg·kg−1, or a placebo. A dietitian, independent from the study, determined the appropriate doses based on each participant's body weight and prepared them in coded, anonymized packages to ensure blinded administration during the test days.
Single-leg isokinetic strength test
The IsoMed 2000 dynamometer (D&R Ferstl GmbH, Hemau, Germany) was used to measure single-leg isokinetic knee flexion and extension strength for the dominant leg. The data obtained from the tests were processed and recorded using the device's proprietary software interface. The results of each test were exported in “.CSV” format and organized for analysis. All participants were invited to the laboratory 72 h before the first test, and their profiles were created for each participant in the device interface. The familiarization process was completed, allowing participants to perform two test trials at two different angular velocities (60°/s and 180°/s) following a ten-minute of standardized warm-up on a cycle ergometer. Each participant's individual device settings were recorded to ensure consistency during the tests.
Participants were seated on the dynamometer chair with a hip joint angle of 75° for full knee extension. The tested leg was carefully positioned so that the popliteal fossa aligned with the front edge of the chair. Depending on the tested leg, the femur, hip, shoulders, and chest were stabilized using the device's pads and straps to ensure proper positioning and minimize movement during testing. The dynamometer lever arm was positioned to 90° to align with knee flexion movement, and the lateral femoral epicondyle landmark was properly adjusted to fix the anatomical axis of rotation in accordance with the manufacturer's guidelines. The single-leg isokinetic test protocol included two angular velocities (60°/s, and 180°/s), for knee flexion and extension. In the initial phase of the test protocols, participants performed three repetitions of submaximal knee flexion and extension movements at %60 submaximal effort to familiarize themselves with the movements and complete a warm-up. After the warm-up, participants performed five maximal repetitions at 60°/s and 5 maximal repetitions at 180°/s to assess isokinetic knee muscle strength. Participants rested for 30 s after the warm-up and for 3 min between the two angular velocities. Verbal and visual encouragement was provided during the test to maximize effort. The tests were performed with a minimum of 48 h between the testing sessions. The intervention period and testing sessions have been demonstrated in Figure 1.
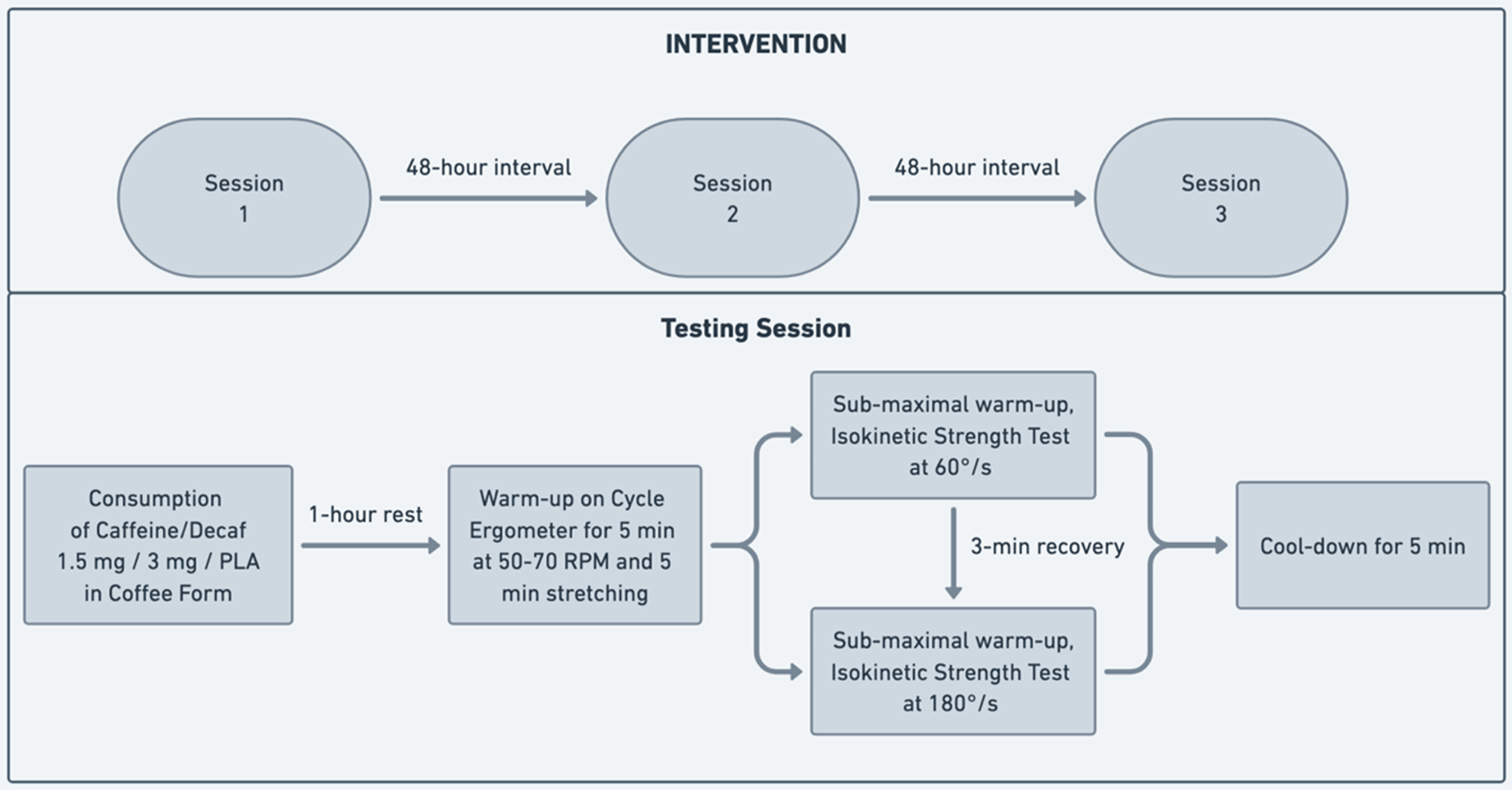
Illustration of intervention and testing session.
Participants’ knee muscle performance at two different angular velocities (60°/s and 180°/s) was assessed by measured peak moment and total work values separately. The rate of perceived exertion (RPE) was recorded end at the end of each angular velocity during the testing sessions.
Statistical analyses were conducted using SPSS 26. The normality of the data was assessed with the Shapiro-Wilk test. For variables that met the normality assumption, one-way repeated measures ANOVA was used, while the Friedman Test was applied to those that did not. In the one-way repeated measures ANOVA results, the p-value, and partial eta squared (effect sizes: small = 0.01 < η² < 0.06, medium = 0.06 < η² < 0.14, large = η² > 0.14) were calculated and reported. The threshold for statistical significance was established at p < 0.05, and the data were reported as mean ± standard deviation (SD).
Results
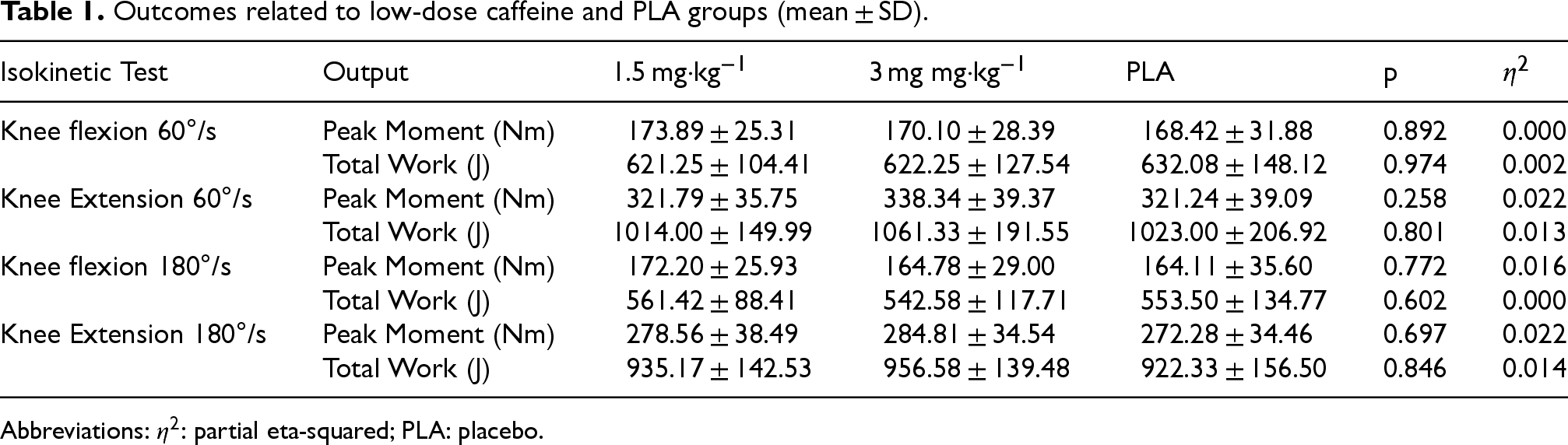
The one-way repeated measures ANOVA results showed no statistically significant differences in peak moment and total work values between the 1.5 mg, 3 mg, and PLA interventions at either angular velocity during flexion and extension.
The single-leg isokinetic test results indicated that the effects of different doses were generally very small or small in terms of effect size (η2). For knee flexion at 60°/s, the effect size for peak moment was η2 = 0.000, p = 0.892, and for total work, it was η2 = 0.002, p = 0.974, indicating no significant effect of the doses on these parameters. For knee extension at 60°/s, the effect size for peak moment was η2 = 0.022, p = 0.258, and for total work, η2 = 0.013, p = 0.801, suggesting that the effect remained small for these parameters as well.
For knee flexion at 180°/s, the effect size for peak moment was η2 = 0.016, p = 0.772, and for total work, η2 = 0.000, p = 0.602, indicating almost no observable effect, particularly for total work. Similarly, for knee extension at 180°/s, the effect size for peak moment was η2 = 0.022, p = 0.697, and for total work (J), η2 = 0.014, p = 0.846, suggesting a small effect of the doses on these parameters.
Overall, the effect size values across all parameters indicate that low-dose caffeine in coffee form did not produce a statistically significant effect on isokinetic strength outputs (Table 1).
Outcomes related to low-dose caffeine and PLA groups (mean ± SD).
Outcomes related to low-dose caffeine and PLA groups (mean ± SD).
Abbreviations:
The RPE values were 14.83 ± 0.83 for the 1.5 mg·kg−1 attempt, 14.66 ± 0.88 for the 3 mg·kg−1 attempt, and 14.91 ± 1.37 for the placebo (PLA) attempt at an angular velocity of 60°/s. Statistical analysis revealed no significant differences among these conditions (p = 0.843), with a negligible effect size (η2 = 0.010).
Similarly, at an angular velocity of 180°/s, the RPE values were 13.41 ± 0.79, 13.25 ± 0.75, and 13.58 ± 0.79 for the 1.5 mg·kg−1, 3 mg·kg−1, and placebo conditions, respectively. Again, no significant differences were observed (p = 0.583), with a small effect size (
These findings revealed that neither different doses of the interventions (1.5 mg·kg−1 or 3 mg·kg−1) resulted in a meaningful change in RPE during isokinetic exercise, regardless of the angular velocity tested (Table 2).
Rating of perceived exertion values in low-dose caffeine and PLA groups.

Abbreviations:
In the present study, two low doses of caffeine in coffee form were examined using a crossover study design. The outcomes revealed that low-dose caffeine supplementation had no impact on single-leg isokinetic strength or RPE at either angular velocities. However, a slight increase in knee extension moment and total work at the angular velocity of 180°/s was observed, though it was not statistically significant. The findings showed that low-dose acute caffeine intake was insufficient to enhance single-leg isokinetic strength production or reduce perceived exertion in physically active males.
Contrary to the findings of the present study, the literature suggests that caffeine consumption enhances sports performance through multiple mechanisms, primarily by acting as an adenosine receptor antagonist in the CNS. This action reduces adenosine's inhibitory effects on neurotransmission, excitation, and pain perception.27–29 In the present study, caffeine's effect on single-leg isokinetic strength was assessed in physically active males using two angular velocities with a 5-repetition protocol for each. The inclusion of two angular velocities enabled the evaluation of caffeine's impact across different contraction speeds, addressing its potential velocity-dependent ergogenic effects. The 5-repetition protocol prioritized maximal effort over fatigue resistance, aligning with strength-focused outcomes. However, the limited repetition range may not fully represent muscular endurance and muscular pain-related perceived exertion. Studies examining the effects of caffeine on isokinetic strength performance indicate that positive changes in isokinetic strength metrics, perceived exertion, and muscle soreness typically occur at doses above ≥3 mg·kg−1.11,12 Some studies examining the effects of caffeine ingestion on isokinetic strength indices at angular velocities of 60°/s30,31 and 180°/s 31 have reported statistically significant performance improvements with a 6 mg·kg−1 dose. 31 Another research, similar to the present study, tested two different caffeine doses (2 mg·kg−1 and 5 mg·kg−1) showed that only the 5 mg·kg−1 dose led to an increase in isokinetic strength metrics (magnitude of %5–8), while no improvements were observed with the 2 mg·kg−1 dose at an angular velocity of 180°/s. 32 These results indicate that low-dose caffeine ingestion is insufficient to provoke enhancement on isokinetic strength performance. A position stand on caffeine and exercise performance stated that while a slight ergogenic effect can be observed with doses as low as 2 mg·kg−1, the clear positive effects are generally observed within the 3–6 mg·kg−1 range. Additionally, it highlights that caffeine's effectiveness varies based on individual differences, training level, exercise type, as well as exercise intensity and duration. 33 In parallel with these results, the present study, which evaluated the two different caffeine doses (≤3 mg·kg−1), showed no statistically significant changes in single-leg isokinetic strength or RPE. The outcomes suggest that the caffeine doses used in this study did not produce an ergogenic effect.
On the other hand, in placebo-controlled crossover studies evaluating the ergogenic effect of caffeine consumption in terms of isokinetic strength metrics, it has been observed that as the dose increases, both the magnitude of the effect and the percentage improvement in performance also increase, with strength gains occurring particularly during the extension phase. 26 Consistent with the literature, the present study found that at a dose of 3 mg·kg−1, the peak moment and total work produced during the extension phase (magnitude of %2–5) were higher compared to both the placebo and the 1.5 mg·kg−1 dose.
The literature indicates that studies investigating the effect of caffeine ingestion on knee isokinetic strength using a placebo-controlled crossover design are very limited, particularly for doses below 3 mg·kg−1. Given its accessibility to athletes, this study focused on caffeine intake in the form of coffee. While previous research has primarily examined higher doses, there remains a gap in understanding the potential benefits of lower doses, especially in practical, real-world scenarios. The ergogenic effect of caffeine is also known to vary based on dose-dependent mechanisms26,33 and genetic variations. 34 Therefore, further research is needed on low-dose caffeine intake, incorporating various sports disciplines, training levels, consumption habits, caffeine forms, and the simultaneous investigation of different doses.
Conclusion
This study examined the effects of commercially available coffee, which is widely accessible and may provide time and cost advantages for athletes and coaches. However, the findings indicated that acute low-dose caffeine intake in coffee form does not significantly enhance single-leg isokinetic knee strength production or alter perceived exertion in physically active males. Therefore, future studies incorporating varying caffeine doses in individuals with different training levels, exercise intensities, and exercise modalities may contribute to the literature and improve understanding of the effects of low-dose caffeine on exercise performance.
Footnotes
Acknowledgments
Thanks to participants for their efforts.
Ethical considerations
The study protocol was approved by the Ethics Committee of Trabzon University (2024-11/2.1). Informed consent form were signed by all participants and the procedures implemented in compliance with the Declaration of Helsinki.
Author contributions
CONCEPTION: Abdulkadir Birol, Erkan Tortu. PERFORMANCE OF WORK: Abdulkadir Birol, Erkan Tortu. INTERPRETATION OR ANALYSIS OF DATA: Erkan Tortu, Abdulkadir Birol. PREPARATION OF THE MANUSCRIPT: Abdulkadir Birol, Erkan Tortu. REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Abdulkadir Birol. SUPERVISION: Abdulkadir Birol.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.