
Abstract
Background
Although an imbalance between the thoracic and lumbar erector spinae muscle activity is known to contribute to spinal dysfunction, the factors influencing this muscle balance, particularly thoracic extension mobility, remain unclear.
Objectives
This study investigated the associations of thoracic kyphosis and thoracic extension mobility with erector spinae muscle activity and muscle balance.
Method
Ninety-four healthy participants underwent measurements of thoracic kyphosis angle, thoracic extension angle, and erector spinae muscle activity (longissimus thoracis, iliocostalis lumborum pars thoracis, and iliocostalis lumborum pars lumborum). Muscle balance was assessed using the ratios of longissimus thoracis to iliocostalis lumborum pars lumborum and iliocostalis lumborum pars thoracis to iliocostalis lumborum pars lumborum. Regression analyses were conducted with erector spinae muscle activities and their ratios as independent variables, and thoracic kyphosis and thoracic extension as dependent variables.
Results
Regression analyses showed that the ratio of longissimus thoracis to iliocostalis lumborum pars lumborum and the activity of the iliocostalis lumborum pars thoracis significantly predicted thoracic extension mobility (adjusted R2 = 0.14, p < 0.001), while the activity of the iliocostalis lumborum pars lumborum significantly predicted thoracic kyphosis (adjusted R2 = 0.04, p = 0.026).
Conclusions
These findings suggest that the assessment and intervention of thoracic extension mobility may be significantly associated with the erector spinae muscle balance during trunk extension exercises.
Keywords
Introduction
Increased thoracic kyphosis caused by repeated prolonged slouched postures or hypomobility of the thoracic spine in sedentary life may pose significant health problems.1–5 Prone trunk extension exercises are recommended for improving thoracic kyphosis.6,7 However, when performing prone trunk extension exercises, individuals with an imbalance between the thoracic and lumbar extensors of the erector spinae exhibit compensatory lumbar hyperextension, resulting in abnormal load distribution and potential spinal dysfunction such as low back pain.8,9 Park et al. 9 reported that, during prone trunk extension exercises, individuals with thoracic hyperkyphosis showed increased thoracic kyphosis angle and lumbar lordotic curve, accompanied by a reduced balance between thoracic and lumbar extensor activity.
The ratio of activity between the thoracic and lumbar extensors has been used as an index of selective recruitment balance.1,9–11 In healthy individuals, values have been reported to range approximately 0.77–0.98,10,12 whereas in individuals with thoracic hyperkyphosis or reduced thoracic extension mobility, ratios closer to 0.51–0.78 have been observed, indicating relative hypoactivity of the thoracic extensors and hyperactivity of the lumbar extensors during prone trunk extension.1,9,10,13 Hyperactivity of the lumbar extensors causes hyperextension of the lumbar spine during prone trunk extension, which can cause low back pain. 14 An imbalance of the thoracic and lumbar extensors is frequently observed in individuals with impaired spinal alignment, particularly those with thoracic flexion syndrome or thoracic hyperkyphosis.7,9 Thoracic hyperkyphosis increases the relative length of the thoracic extensors, making it difficult to activate them during trunk extension because of the length and tension relationship, and lumbar extensors are overused.7,9,15 However, most previous studies have focused on static postural measures, and the role of spinal mobility in muscle activation patterns remains less understood.
Since thoracic hyperkyphosis affects the imbalance of the thoracic and lumbar extensors, therapeutic approaches addressing both thoracic alignment and mobility have been investigated.8,9,16 Jung et al. 8 reported that thoracic mobilization not only improved thoracic kyphosis but also improved the thoracic extension range and decreased the activity of the thoracic extensor. The improvement in thoracic kyphosis due to thoracic mobilization may have altered the activity of the thoracic extensors because there is a correlation between the erector spinae and thoracic kyphosis.8,9,17 However, the relationship between the changes in erector spinae activity and thoracic mobility remains unclear.
Muscle activity increases when movement is performed in a static posture; the activity of the thoracic extensor of the erector spinae increases when the thoracic spine is extended.18,19 Previous studies have mainly examined the association between thoracic kyphosis angle (a static alignment parameter) and extensor activity.18,19 However, because extensor activity occurs during movement, it may be more closely related to thoracic extension mobility than to static kyphosis. Therefore, in this study we included both thoracic kyphosis and thoracic extension to clarify their respective associations with erector spinae activity. This study aimed to determine the relationship between the erector spinae muscle activity (longissimus thoracis, iliocostalis lumborum pars thoracis, iliocostalis lumborum pars lumborum, and the ratio of the erector spinae muscles) and thoracic spine parameters (thoracic kyphosis and thoracic extension mobility).
Methods
Participants
Ninety-four healthy participants (male = 63, female = 31) who self-perceived an increase in thoracic kyphosis were recruited through internet advertisements (Table 1). Participants with a history of spinal column fractures, scoliosis, spinal tumors and related malignancies, cancer, congenital spinal anomalies, or rheumatoid arthritis were excluded from the study. This study was approved by the Yonsei University Wonju Institutional Review Board (1041849-202101-BM-009-01).
Demographic data.

Demographic data.
The thoracic kyphosis angle and thoracic extension mobility were measured using a Spinal Mouse device (CH6604, Idiag AG, Zurich, Switzerland). The Spinal Mouse, a handheld and computer-based electromechanical device, was used to measure spinal curvature. This device has accelerometers that measure changes in the angle and intersegmental distance of the vertebra. The device contains two rolling wheels that follow the spinous processes of the spine. The data were transferred from the device to Spinal Mouse software (sampling frequency of approximately 150 Hz). These data were calculated as the total angle of the sagittal plane using the Spinal Mouse Software (G6, Ver. 6.4.2, Idiag AG, Zurich, Switzerland). The reliability and validity of the Spinal Mouse for assessing spinal curvature and mobility have been demonstrated in previous studies.20,21
Thoracic kyphosis and thoracic extension were measured in the sagittal plane. The participants were instructed to stand comfortably in a crossarm position with the shoulders flexed at 70°, and thoracic kyphosis was measured in this position.8,22 To measure thoracic extension, participants stood comfortably with their hands placed behind their heads.2,8,23 They were instructed to extend the thoracic spine toward the ceiling while maintaining a neutral lumbar posture, and the thoracic angle at the end of the extension was recorded using the same kyphosis measurement protocol as in the baseline assessment.1,2,8,23 Because this angle reflects the curvature of the thoracic spine on a kyphosis scale, lower or more negative values indicate a greater degree of thoracic extension. To minimize breathing-related artifacts, participants briefly held their breath at end-range extension.
Muscle activity of the erector spinae
The muscle activities of the longissimus thoracis (LT), iliocostalis lumborum pars thoracis (ICT), and iliocostalis lumborum pars lumborum (ICL) were measured using surface electromyography (sEMG) with the Noraxon Ultium ESP System (Noraxon USA, Inc., Scottsdale, AZ, USA), as according to Criswell. 18 To reduce skin impedance, excess body hair was shaved and, if necessary, the skin was gently abraded with fine-grade sandpaper. After these procedures, the skin was cleaned with alcohol swabs for hygienic purposes. Bipolar Ag/AgCl electrodes were used with an inter-electrode distance of 20 mm and a common-mode rejection ratio greater than 100 dB. Signals were collected using MyoMuscle™ MR3 3.14.52 (Noraxon USA, Inc., Scottsdale, AZ, USA). The EMG signals were band-pass filtered (20–450 Hz) and the root mean square (RMS) values were calculated using a 50-ms window. For RMS calculation, the middle 3 s of each 5-s measurement (excluding the first and last 1 s) was analyzed. The RMS value was calculated separately for each repetition, and the mean of the two repetitions was used as the representative value for analysis. The data were recorded at a sampling rate of 2000 Hz.
Muscle activity of the erector spinae was measured during the prone thoracic extension exercise because this task reflects active recruitment of the thoracic extensors, which we intended to compare with standing thoracic extension mobility as a structural parameter. 8 At the end of the table, the participants aligned the xiphoid process and were in thoracic flexion with their arms crossed in front of their chest (initial position). The lower extremities (hip, knee, and ankle joints) were fixed using a nonelastic belt. The participants were then instructed to extend their spines parallel to the floor. The target bar was located at the T6 level, in a position where the participants extended their spine parallel to the floor. To measure the muscle activity of the erector spinae, the participants extended their spines to the target bar and held that position for 5 s (test position, Figure 1). The muscle activity of the erector spinae was measured twice and expressed as the average value.

Prone thoracic extension in test position.
The activities of the LT, ICT, and ICL muscles were calculated as the percentage of maximum voluntary isometric contraction (MVIC). To obtain MVC, participants performed a prone back extension against the examiner's manual resistance at the upper thoracic region, following a previously described procedure. 8 Each contraction was held for 5 s and repeated twice with rest in between. The ratios of LT to ICL (LT:ICL = LT/ICL activity) and ICT to ICL (ICT:ICL = ICT/ICL activity) were calculated to indicate the balance between the thoracic and lumbar extensors.
Statistical analyses were performed using SPSS ver. 20.0 (SPSS Inc., Chicago, IL, USA). The normality of residuals was assessed using the Kolmogorov–Smirnov test. All residuals met the assumption of normality (p = 0.200). Pearson's correlation analysis was used to examine the bivariate relationships between thoracic spine variables (kyphosis, extension) and EMG outcomes (LT, ICT, ICL, LT:ICL, and ICT:ICL), as a preliminary step before regression. Multiple regression analyses with stepwise selection were then performed using LT, ICT, ICL, LT:ICL, and ICT:ICL as independent variables, with thoracic kyphosis and thoracic extension as dependent variables. Stepwise selection was applied in an exploratory manner to identify the most significant predictors among the thoracic spine parameters. The assumptions of regression analysis, including normality, linearity, homoscedasticity, independence of residuals (Durbin–Watson range = 1.29–1.87), and multicollinearity (all VIFs < 2), were evaluated and met. Differences were considered statistically significant at P < 0.05.
Results
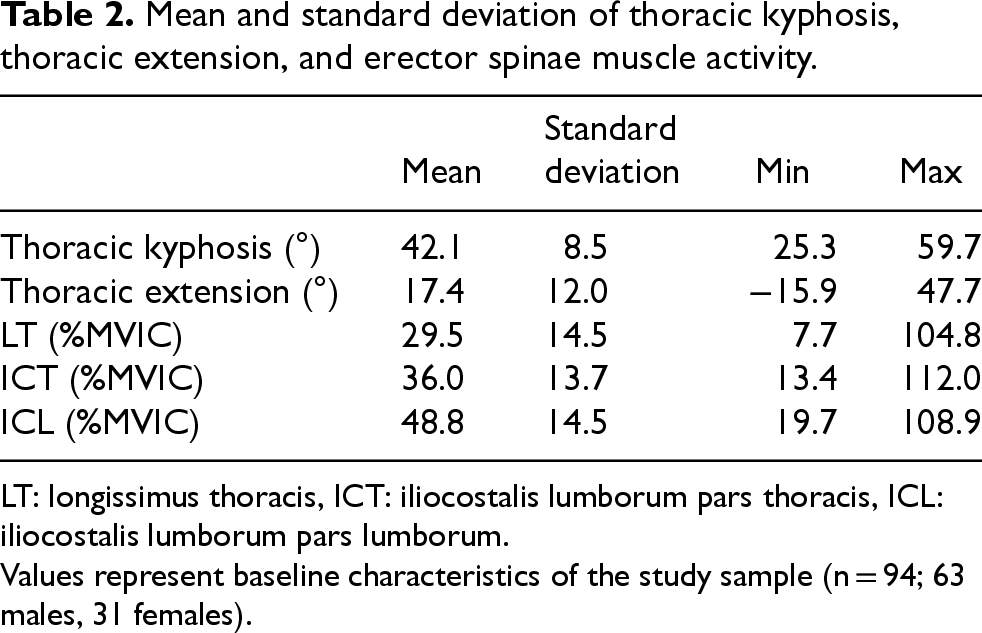
Thoracic kyphosis ranged from 25.3° to 59.7° (mean 42.1° ± 8.5°), and thoracic extension ranged from −15.9° to 47.7° (mean 17.4° ± 12.0°). The mean muscle activities were 29.5%MVIC for LT, 36.0%MVIC for ICT, and 48.8%MVIC for ICL (Table 2).
Mean and standard deviation of thoracic kyphosis, thoracic extension, and erector spinae muscle activity.
Mean and standard deviation of thoracic kyphosis, thoracic extension, and erector spinae muscle activity.
LT: longissimus thoracis, ICT: iliocostalis lumborum pars thoracis, ICL: iliocostalis lumborum pars lumborum.
Values represent baseline characteristics of the study sample (n = 94; 63 males, 31 females).
Pearson's correlation analysis showed that thoracic kyphosis was positively correlated with ICL activity (r92 = 0.23, p = 0.026), while thoracic extension was positively correlated with ICL activity (r92 = 0.23, p = 0.029) and negatively correlated with the LT:ICL ratio (r92 = -0.33, p = 0.001) (Table 3, Figure 2). No significant correlations were observed for ICT or the ICT:ICL ratio.

Scatterplot showing the relationship between LT/ICL ratio and thoracic extension, color-coded by thoracic kyphosis.
Pearson's correlation between thoracic kyphosis, thoracic extension, and erector spinae muscle activity.
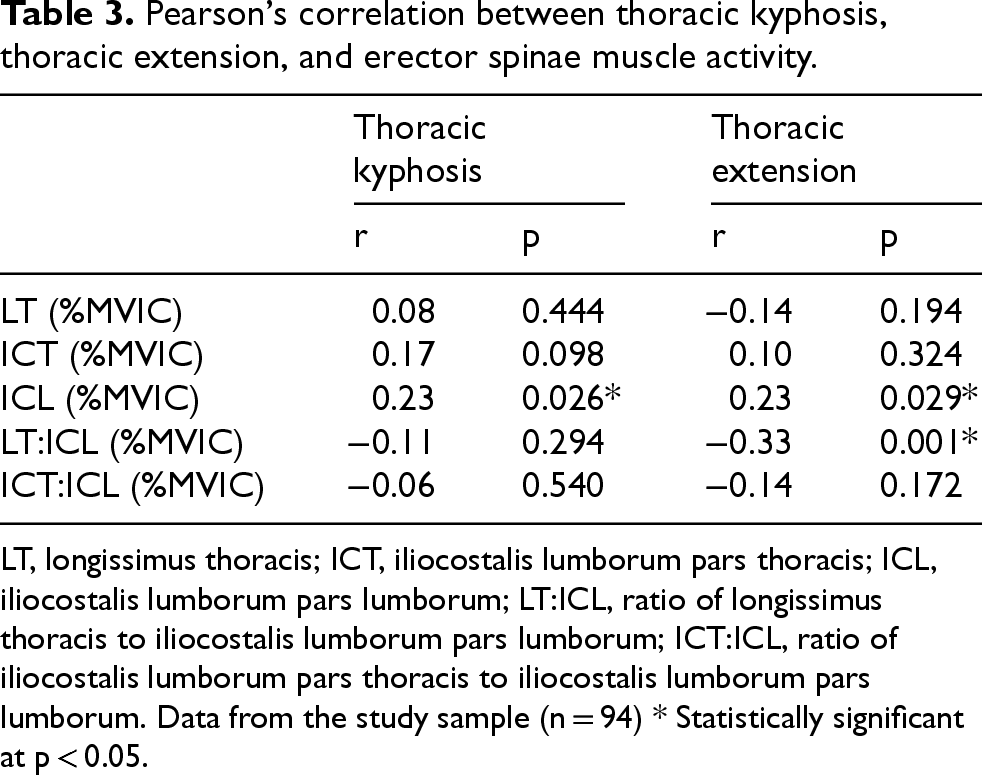
LT, longissimus thoracis; ICT, iliocostalis lumborum pars thoracis; ICL, iliocostalis lumborum pars lumborum; LT:ICL, ratio of longissimus thoracis to iliocostalis lumborum pars lumborum; ICT:ICL, ratio of iliocostalis lumborum pars thoracis to iliocostalis lumborum pars lumborum. Data from the study sample (n = 94) * Statistically significant at p < 0.05.
In the regression analysis, the LT:ICL ratio significantly predicted thoracic extension (adjusted R2 = 0.097, F = 11.02, p = 0.001), and the model further improved when ICT activity was added (final adjusted R2 = 0.137, F = 8.37, p < 0.001, Durbin–Watson = 1.29), while ICL activity significantly predicted thoracic kyphosis (adjusted R2 = 0.043, F = 5.14, p = 0.026, Durbin–Watson = 1.87).
This study aimed to clarify how thoracic kyphosis and thoracic extension are associated with erector spinae muscle activity and muscle balance during trunk extension. Although thoracic spine mobility influences erector spinae activation, previous studies have focused on the relationship between thoracic kyphosis and muscle activity. A recent study reported that a group with low thoracic spine extension mobility had lower LT muscle activity and LT: ICL ratio than a group with high thoracic spine extension mobility. 1 However, evidence directly examining the association between thoracic extension mobility and erector spinae muscle activity remains limited, highlighting the need for further investigation. In the present study, thoracic extension mobility was significantly predicted by the LT:ICL ratio and ICT activity (14% of the variance), whereas thoracic kyphosis was predicted by ICL activity, explaining only 4% of the variance. This indicates that mobility may be more critical for the balance of erector spinae activity than kyphosis.
The closer the LT: ICL ratio is to 1, the better the balance between the thoracic and lumbar regions of the erector spinae.1,9 If the ratio is low, that is, if the imbalance increases, it can cause lower back pain. Park et al. 9 reported a difference in the LT:ICL ratio between individuals with and without hyperkyphosis; however, in this study, there was no correlation between the LT: ICL ratio and thoracic kyphosis. Instead, the significant correlation (r92 = -0.33, p = 0.001) between thoracic extension and this ratio suggests that individuals with better thoracic mobility demonstrate more balanced erector spinae activation patterns. This correlation strength indicates that approximately 14% of the variance in muscle balance can be attributed to thoracic mobility, which has practical implications for exercise prescription. There are two possible reasons why the LT: ICL ratio correlates with thoracic extension. First, because the activity of the erector spinae occurs during trunk extension mobility, the activity of the LT may be more related to thoracic extension mobility than to thoracic kyphosis, which is a static posture. Second, limited thoracic extension mobility causes compensatory lumbar hyperextension to reach the target position during prone trunk extension.7,9 This compensatory mechanism may directly influence the LT/ICL ratio by altering the relative contribution of thoracic versus lumbar extensors.
Lumbar hyperextension has been observed in individuals with thoracic hyperkyphosis during prone trunk extension, which may lead to lumbar extensor hyperactivity. 9 Jung et al. 8 reported that improvements in thoracic hyperkyphosis may reduce lumbar extensor activity. In our study, there was a significant positive correlation (r92 = 0.23, df = 93, p = 0.026) between thoracic kyphosis and ICL activity. ICL activity was entered as a predictor in the regression model of thoracic kyphosis, which supports the results of previous studies.8,9 Similarly, our findings demonstrated that thoracic extension was positively correlated with ICL activity (r92 = 0.23, p = 0.029) and the LT:ICL ratio served as a predictor in the regression model for thoracic extension. While improving thoracic kyphosis reduces excessive lumbar extensor activity, enhancing thoracic extension mobility increases thoracic extensor recruitment. These complementary findings suggest that optimal erector spinae muscle balance can be achieved by addressing both static postural deformities and dynamic mobility limitations.
This study had several limitations. First, in our study, subjects aged 20–50 years participated (35.1 ± 6.7). Therefore, the results of our study cannot be generalized to older populations. Second, body composition was not assessed, and greater subcutaneous adipose tissue may have affected the accuracy of surface EMG signal detection, representing a potential confounding factor. Third, only thoracic spine kinematics were measured. As there is a high correlation between the kinematics of the thoracic and lumbar spines, analysis of the lumbar spine may also be meaningful due to its clinical relevance to low back pain. Fourth, because surface EMG was used to measure muscle activity in this study, the activity of the transversospinalis muscles, such as the multifidus, was not measured; only the activity of the erector spinae was measured. Fifth, thoracic extension mobility was assessed in a standing posture, whereas muscle activity was measured during prone trunk extension, which may have introduced differences due to posture. Sixth, EMG activity was recorded during a static hold rather than dynamic movement, so the findings may not fully represent functional activities. Finally, although statistically significant associations were observed, the explained variance of the regression models was small. Thus, the practical implications of these findings may be limited and should be interpreted with caution.
Conclusion
Our findings indicate that thoracic extension and, to a lesser extent, thoracic kyphosis are associated with variations in erector spinae activity and muscle balance. We found no correlation between the LT: ICL ratio and thoracic kyphosis; however, the LT: ICL ratio was significantly correlated with thoracic extension. The LT:ICL ratio emerged as a significant predictor of thoracic extension, highlighting its role in determining the balance of erector spinae muscle activity. This suggests that the mobility of the thoracic spine should be considered to improve the activity of the thoracic spine and the ratio between the thoracic and lumbar extensors when applying a thoracic intervention.
Footnotes
Acknowledgments
We would like to thank the assistant researcher at the KEMA station for their helpful assistance in the preparation of this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (NRF-2020R1A6A3A01099963).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.