
Abstract
Background
Glenohumeral internal rotation range of motion deficit (GIRD) is linked to shoulder strength in the glenohumeral (GH) joint and to increased risk of throwing-related injuries. In adolescent overhead athletes, GIRD ≥25° has been associated with a four-fold higher risk of upper-extremity injury. However, from a functional perspective relevant to overhead throwing, the extent to which GIRD is related to the dynamic strength of the shoulder rotators has not been investigated.
Objective
This study compared internal rotation (IR) and external rotation (ER) torque between adolescent baseball athletes with and without GIRD, and examined factors associated with concentric and eccentric IR/ER torque, including GH joint range of motion (ROM).
Method
Eighty male adolescent baseball athletes participated. IR, ER, total rotational ROM, and GIRD were measured. Concentric and eccentric torque of IR and ER, as well as functional strength ratios, were assessed. Group differences were analyzed with independent t-tests, correlations with Pearson's coefficients, and predictors with Stepwise multiple regression analysis.
Results
Concentric IR and ER torques were significantly lower in the GIRD group than in the non-GIRD group (mean differences: 4.6% and 6.9% body weight, respectively; p < 0.05). Concentric torques showed poor to fair correlations with GH joint rotational ROM, particularly reduced IR ROM and increased GIRD. Eccentric torques did not differ significantly between groups. Regression analysis identified IR ROM and GIRD as significant predictors of concentric torque, while antagonist exhibited the greatest relative influence on the agonist.
Conclusions
Concentric shoulder strength (IR and ER torques) is reduced in adolescent baseball athletes with GIRD and is significantly associated with IR ROM loss. IR ROM and GIRD were key predictors of concentric torque, while antagonist strength exerted the greatest relative influence on agonist function. In contrast, eccentric torques showed no group differences or meaningful correlation with GH joint ROM.
Keywords
Introduction
Shoulder pain is the most prevalent concern among overhead athletes, with more than 50% of adolescent baseball players experiencing shoulder pain.1,2 Recent epidemiological studies have reported a notable prevalence of shoulder and elbow injuries in youth and high school baseball players.3,4 The glenohumeral (GH) joint is particularly susceptible to microtrauma due to repetitive throwing. Internal rotation (IR) velocities of approximately 7000–7900°/s and torques of up to 90 Nm have been reported.1,5,6 Consequently, distractive forces and eccentric stress increase on the soft tissues of the posterior shoulder, including the posterior deltoid, rotator cuff, and posteroinferior capsule.7–9 In addition, the excessive external rotation (ER) motion required during the late cocking phase leads to posterior–superior humeral head translation, thereby further increasing mechanical stress on the GH joint.7,10,11 Recent imaging and clinical reviews have confirmed that repetitive posteroinferior capsular contracture, scapular dysfunction, and microinstability exacerbate posterosuperior internal impingement and predispose throwers to SLAP lesions and rotator cuff pathology.6,11
These biomechanical features of overhead throwing may induce adaptive changes in the soft tissues. Glenohumeral internal rotation deficit (GIRD), defined as a reduction in IR range of motion (ROM) of the throwing shoulder, is considered a representative adaptive response to repetitive throwing-induced soft tissue stress.7,12 Typically, an IR ROM reduction of more than 20° in the throwing shoulder compared to the non-throwing shoulders is the suggested criterion for GIRD.13–15 Some studies, however, have proposed that a GIRD of up to 15° may be considered within the normal range in overhead athletes.16,17 Importantly, GIRD exceeding 20° is closely associated with throwing-related injuries,15,18–20 with reports indicating approximately a four-fold increase in upper-extremity injury risk in adolescent overhead athletes presenting with GIRD of ≥25°. 19 Complementing these findings, a systematic review and meta-analysis across multiple overhead sports further suggested that athletes with GIRD tend to show an increased risk of shoulder and elbow injuries, particularly in association with total rotational motion deficits and excessive ER gain, 21 which may represent a compensatory mechanism to maintain functional performance despite a reduced total rotational arc.14,22
Furthermore, GIRD is associated with alterations in shoulder muscle strength, as decreased ROM affects muscle-length tension relationships and subsequently influences force generation. 23 In addition, GIRD shifts the GH rotation center posterosuperiorly, increasing distractive forces on the posterior GH structures.7,13 These biomechanical alterations contribute to imbalances in the shoulder rotator muscles, 7 and previous studies have demonstrated significant differences in IR and ER strength, rotator thickness, and strength ratios in adolescent and adult overhead athletes with GIRD.20,24–26 During throwing, the GH joint experiences maximal stress owing to repetitive concentric contractions of the ER and IR agonists, particularly from the late cocking to deceleration phases.9,27,28 Therefore, eccentric antagonist control is essential to prevent GH joint overload.29,30
The functional strength ratio (FSR), defined as the ratio of eccentric antagonist strength to concentric agonist strength, has been proposed as an indicator of shoulder stability.31–34 Supporting this concept, Guney et al. 26 found that adolescent overhead athletes with GIRD showed reduced FSR, while recent scoping reviews of isokinetic dynamometry in youth athletes, including baseball players, have consistently reported ER/IR strength imbalances, particularly reduced eccentric ER (ECC ER) to concentric IR (CON IR) ratios. 35 A lower ECC ER/CON IR ratio has been suggested as a predisposing factor for throwing-related injuries in overhead athletes.22,35,36 Although some assumptions posit that GH joint rotational ROM and GIRD influence shoulder muscle strength,7,13,23 few studies have explore how GH rotational ROM affects the concentric and eccentric torques of the IR and ER muscles, which reflect the functional characteristics required for throwing.
Previous investigations have primarily relied on isometric strength assessments, which may not adequately capture the dynamic demands of overhead throwing.20,24,25 Evidence from adolescent athletes indicates that isokinetic dynamometry can be reliably applied in youth athletes, with reliability confirmed in adolescent athletes 37 (ICCs 0.72–0.99, CVs 3.9–17.4%) and further studies profiling isokinetic strength characteristics in adolescent and junior overhead athletes,26,33 together with a recent scoping review that examined its broader application in youth athletes. 35 However, comprehensive evaluation of shoulder rotational strength in adolescent overhead athletes remains scarce, with, to our knowledge, only one investigation directly examining isokinetic strength in relation to GIRD. 26 By contrast, scoping reviews have systematically mapped and synthesized existing evidence on ER/IR strength characteristics in youth overhead athletes, yet these reviews did not specifically evaluate their relevance to GIRD. 35 Therefore, this study aimed to investigate differences in the concentric and eccentric torques of the IR and ER muscles and the FSR according to GIRD status in adolescent baseball players, and to examine potential factors associated with CON and ECC IR and ER torque, including GH joint ROM.
Materials and methods
Subjects
Sample size was estimated using G*Power (v3.1.2; University of Kiel, Germany). A pilot study with 30 male adolescent baseball athletes was conducted, and correlation analyses were performed between IR ROM and concentric/eccentric IR and ER torques. The lowest correlation coefficient observed was between IR ROM and ECC IR torque (r = −0.186), which was used as the effect size for the sample size estimation. Based on this value, a priori power analysis (correlation: bivariate normal model, α = 0.05, power = 0.95) indicated that a minimum of 53 participants was required. Accordingly, 80 male adolescent baseball players who were able to train and compete without pain were recruited. Inclusion criteria required a Kerlan-Jobe Orthopedic Clinic (KJOC) score ≥70, which is above the pain threshold of 68.6. 38 Demographic data are presented in Table 1. Participants with a history of shoulder surgery, dysfunction, or upper- extremity injuries were excluded. Informed consent was obtained from all parents or guardians, and consent for participation was obtained for all study participants. The study was approved by the Bioethics Committee of Pukyong National University (Approval No: 1041386-202310-HR-118-02) and registered with the Clinical Research Information Service (KCT0009349).
Demographic and clinical characteristics of participants (n = 80).
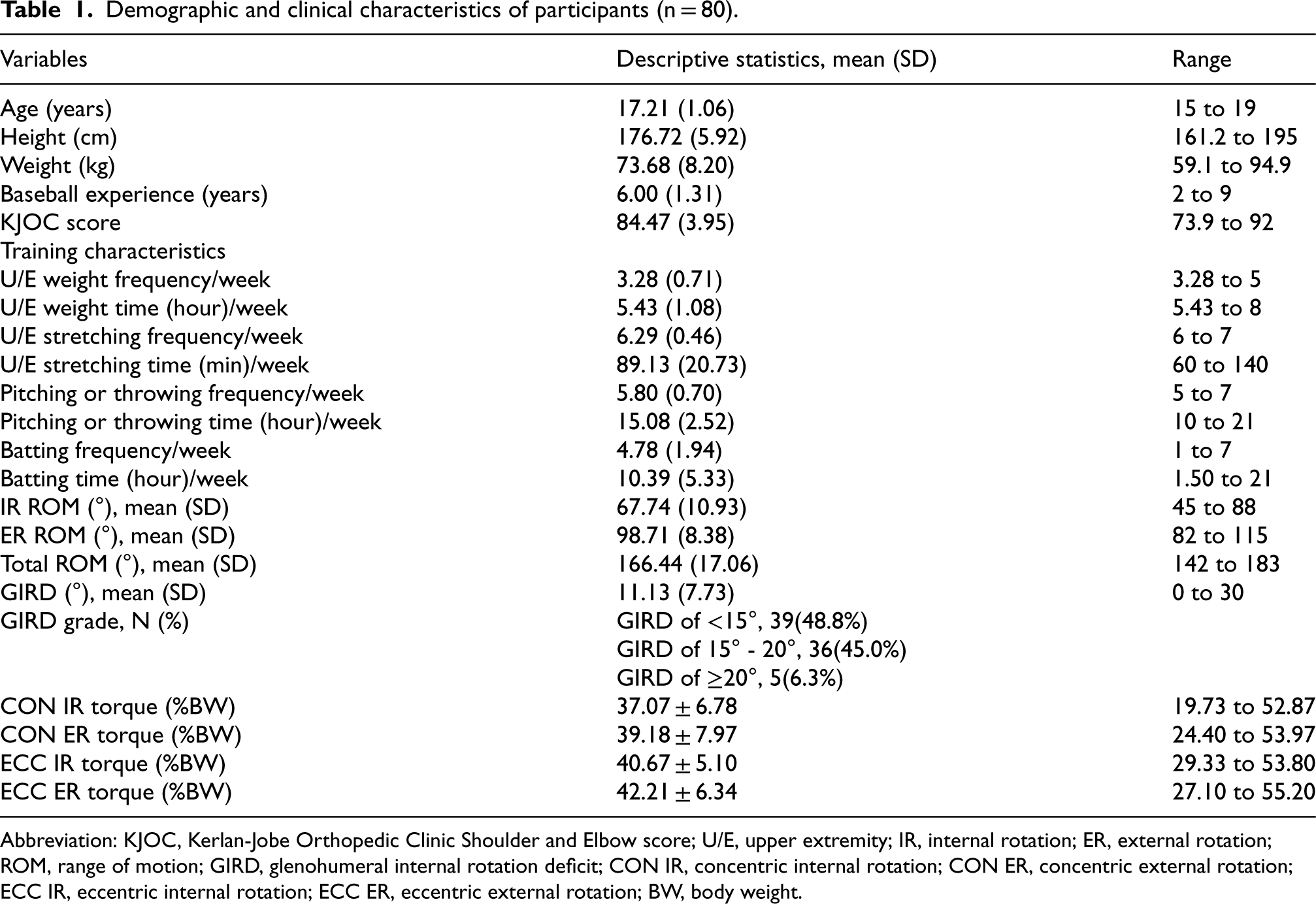
Demographic and clinical characteristics of participants (n = 80).
Abbreviation: KJOC, Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow score; U/E, upper extremity; IR, internal rotation; ER, external rotation; ROM, range of motion; GIRD, glenohumeral internal rotation deficit; CON IR, concentric internal rotation; CON ER, concentric external rotation; ECC IR, eccentric internal rotation; ECC ER, eccentric external rotation; BW, body weight.
GH joint ROM was assessed through IR, ER, total rotational ROM, and GIRD. IR and ER were passively measured at 90° shoulder abduction using a bubble goniometer by two examiners, one stabilizing the scapula and the other recording ROM.15,39,40 The goniometer axis was aligned with the olecranon process; the stationary arm was positioned perpendicular to the floor, and the movable arm was aligned parallel to the ulna's styloid process (Figure 1). GIRD was calculated as the difference in IR between throwing and non-throwing shoulders, while total rotation was defined as the sum of IR and ER of the throwing shoulder. Intra-rater reliability was assessed using ICC (3,1) according to COSMIN guidelines. The same examiner performed repeated ROM measurements twice, separated by a 5-day interval, under identical testing conditions. The results demonstrated high reliability for IR (ICC = 0.925, 95% CI = 0.886–0.951, SEM = 3.0, p < .001) and ER (ICC = 0.926, 95% CI = 0.887–0.952, SEM = 2.3, p < .001). Participants with GIRD ≥15° were assigned to the GIRD group (n = 41), and those with <15° were assigned to the non-GIRD group (n = 39).
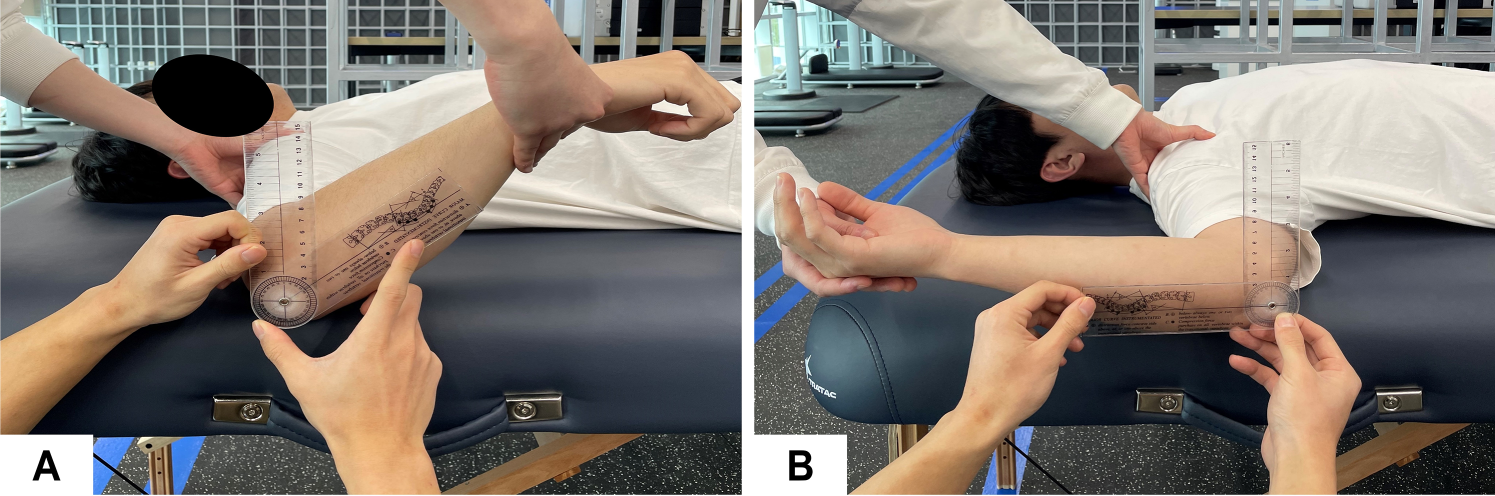
Measurement of internal and external rotation ROM in the glenohumeral joint. (a) Internal rotation, (b) external rotation.
The isokinetic concentric and eccentric torques of IR and ER were assessed using the Biodex System 4 (Biodex Corp., Shirley, NY). Participants completed 3–5 submaximal warm-up contractions under standardized conditions. All measurements were conducted in the supine position, which provides stability, facilitates ROM assessment, and minimizes compensatory movements.41,42 Participants were positioned with 90° shoulder abduction, 0° rotation, and 90° elbow flexion in forearm pronation. The shoulder axis was aligned with the dynamometer, and straps were used to secure the trunk and shoulder girdle (Figure 2). Torque was measured across IR 60° to ER 90°31,32 at a velocity of 120°/s.30,43 Each participant performed five repetitions, and peak torque values were normalized to body weight (%BW). FSRs were calculated using ECC IR/CON ER and ECC ER/CON IR ratios to reflect the dynamic balance between agonist and antagonist rotator muscles. Two types of ratios were considered: (1) ECC IR/CON ER, representing the functional demand during the cocking phase; and (2) ECC ER/CON IR, representing the functional demand during the deceleration phase. These ratios have been described in previous studies as important indicators of dynamic stability in athletes, including overhead athletes.34,44 A 5-min rest interval was provided between tests. Gravity correction was omitted because torque was generated in the direction of gravity regardless of contraction type.32,45

Measurement of internal and external rotation ROM in the glenohumeral joint. (a) Internal rotation, (b) external rotation.
Data were analyzed using SPSS version 21.0. The normality of all variables was assessed using Kolmogorov-Smirnov test (p > 0.05). For group comparisons, independent t-tests were performed separately for each dependent variable (concentric and eccentric IR/ER torque and FSR). Each dependent variable was tested only once between the two groups (GIRD vs. non-GIRD). Pearson's correlation coefficients were used to examine relationships between torque values, GH joint ROM, and other variables (e.g., physical characteristics, experience, and upper limb training and practice routines). Finally, stepwise multiple regression analysis were conducted to identify significant predictors of concentric and eccentric IR/ER torque.
Results
Difference in concentric and eccentric torques of the IR and ER, and FSR between GIRD and non-GIRD
Table 2 presents torque comparisons between GIRD and non-GIRD groups. CON IR torque was significantly lower in the GIRD group (mean difference: 4.61 PT/BW, effect size [ES]: 0.72), as was CON ER torque (mean difference: 6.88 PT/BW, ES: 0.95). The ECC IR/CON ER ratio was significantly higher in the GIRD group (mean difference: −0.19, ES: 0.70). No significant differences were observed in eccentric torques or in the ECC ER/CON IR ratio.
Difference in concentric and eccentric torques of IR and ER, and FSR between GIRD and non-GIRD groups.
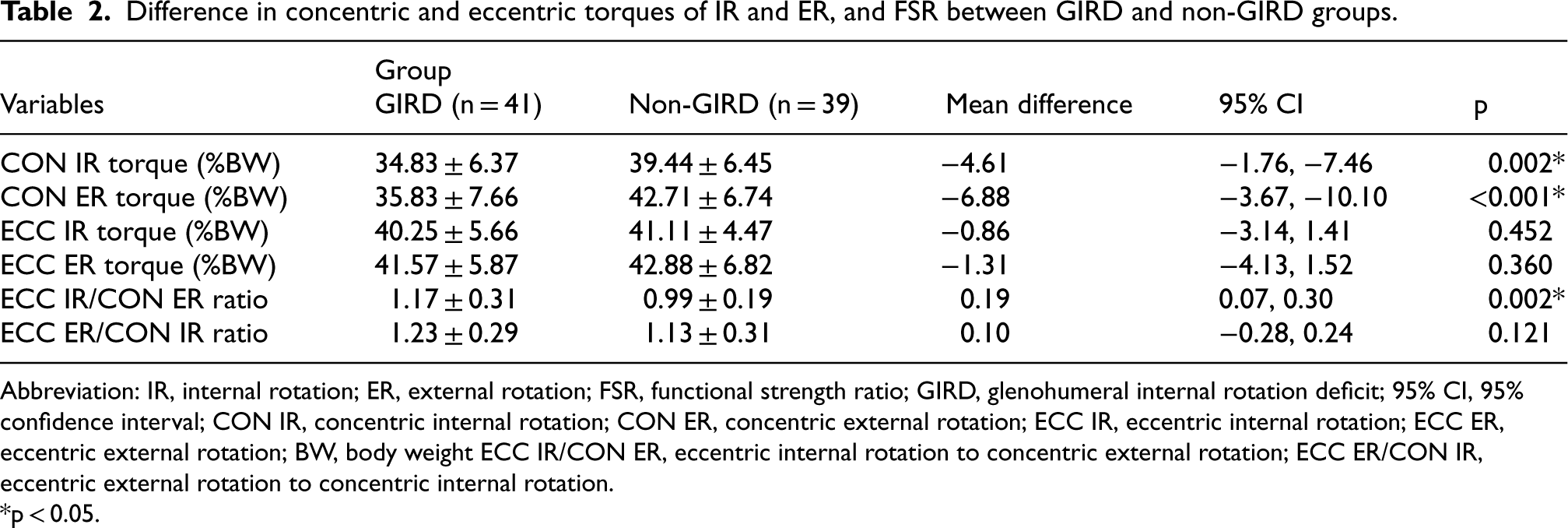
Difference in concentric and eccentric torques of IR and ER, and FSR between GIRD and non-GIRD groups.
Abbreviation: IR, internal rotation; ER, external rotation; FSR, functional strength ratio; GIRD, glenohumeral internal rotation deficit; 95% CI, 95% confidence interval; CON IR, concentric internal rotation; CON ER, concentric external rotation; ECC IR, eccentric internal rotation; ECC ER, eccentric external rotation; BW, body weight ECC IR/CON ER, eccentric internal rotation to concentric external rotation; ECC ER/CON IR, eccentric external rotation to concentric internal rotation.
*p < 0.05.
Table 3 summarizes the correlation results. CON IR torque demonstrated fair positive correlations with IR ROM (r = 0.417) and total rotation ROM (r = 0.239), and fair negative correlations with ER ROM (r = −0.306) and GIRD (r = −0.444). It also showed a fair positive correlation with CON ER torque (r = 0.619). CON ER torque showed a fair positive correlation with IR ROM (r = 0.390), and fair negative correlations with ER ROM (r = −0.418) and GIRD (r = −0.510). Additionally, CON ER torque demonstrated a poor positive correlation with baseball experience (r = 0.231), as well as fair positive correlations with CON IR (r = 0.619) and ECC ER torque (r = 0.433). ECC IR and ECC ER torques showed no significant correlations with GH joint ROM variables. ECC IR torque demonstrated poor negative correlations with height (r = −0.248) and weight (r = −0.291), and a fair positive correlation with ECC ER torque (r = 0.454). ECC ER torque also showed fair positive correlations with CON ER torque (r = 0.433) and ECC IR torque (r = 0.454).
Pearson correlation coefficients (r) among variables (n = 80).
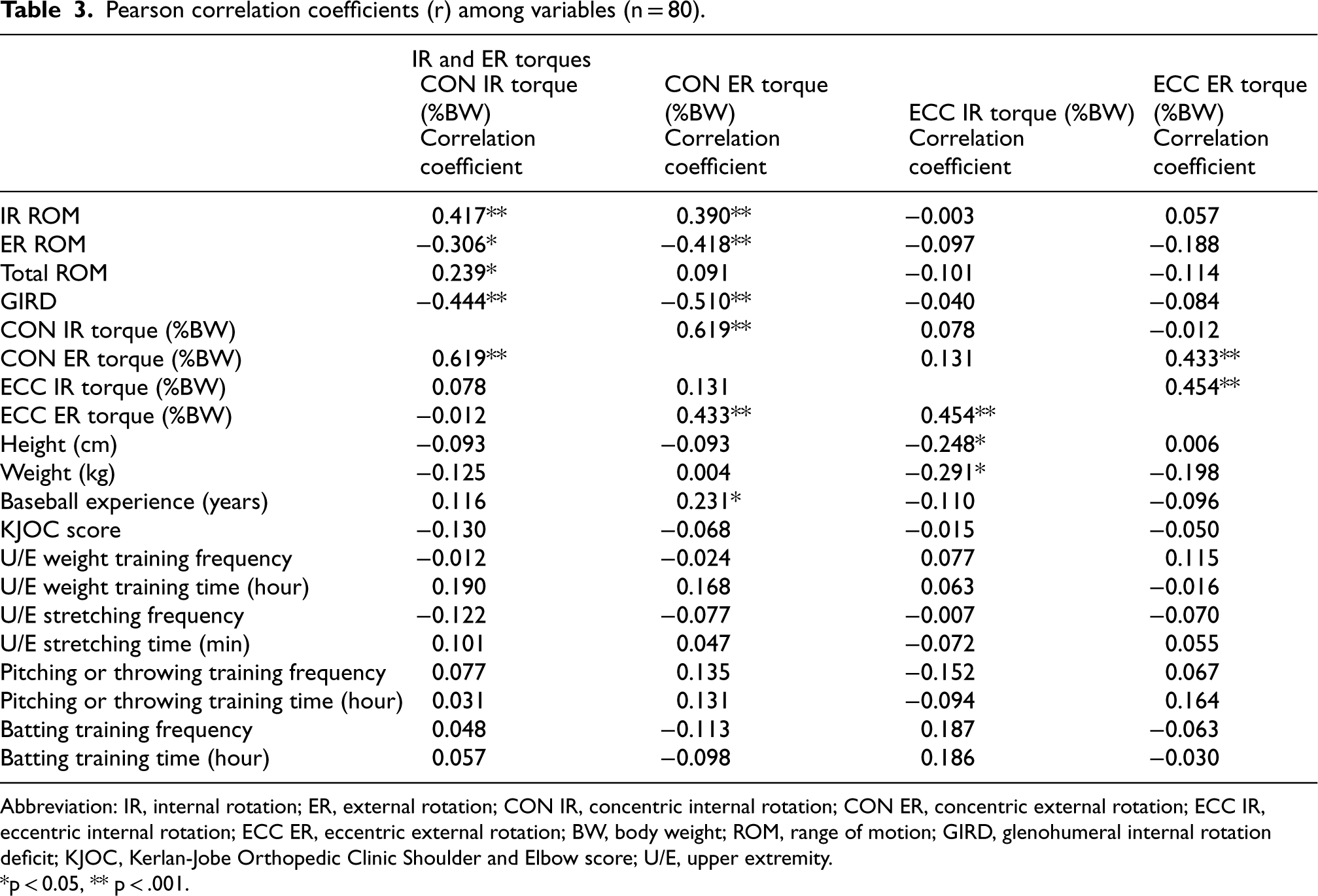
Pearson correlation coefficients (r) among variables (n = 80).
Abbreviation: IR, internal rotation; ER, external rotation; CON IR, concentric internal rotation; CON ER, concentric external rotation; ECC IR, eccentric internal rotation; ECC ER, eccentric external rotation; BW, body weight; ROM, range of motion; GIRD, glenohumeral internal rotation deficit; KJOC, Kerlan-Jobe Orthopedic Clinic Shoulder and Elbow score; U/E, upper extremity.
*p < 0.05, ** p < .001.
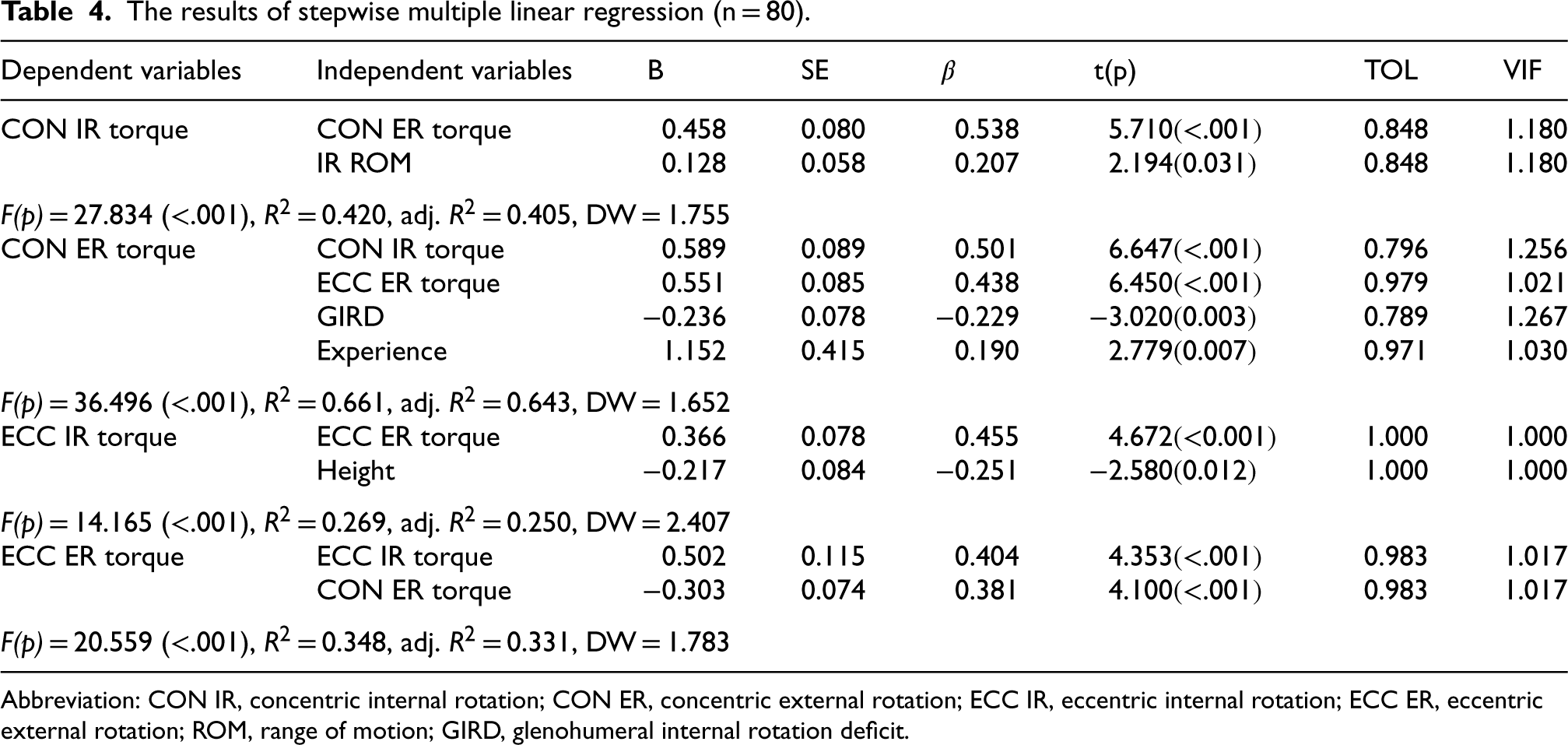
Table 4 presents the results of stepwise regression analyses identifying significant predictors of CON and ECC IR and ER torques, based on variables identified through Pearson correlation analysis.
The results of stepwise multiple linear regression (n = 80).
The results of stepwise multiple linear regression (n = 80).
Abbreviation: CON IR, concentric internal rotation; CON ER, concentric external rotation; ECC IR, eccentric internal rotation; ECC ER, eccentric external rotation; ROM, range of motion; GIRD, glenohumeral internal rotation deficit.
The model for CON IR torque was significant (F = 27.834, p < .001), explaining 40.5% of variance (adj. R2 = 0.405). CON ER torque (β = 0.538) and IR ROM (β = 0.207) were significant predictors, with CON ER torque exerting the stronger influence (Table 4).
CON ER torque
The regression model for CON ER torque was significant (F = 36.496, p < .001), explaining 64.3% of the variance (adj. R2 = 0.643). Significant predictors included CON IR torque (β = 0.501), ECC ER torque (β = 0.438), GIRD (β = −0.229), and baseball experience (β = 0.190), with CON IR torque showing the strongest association (Table 4).
ECC IR torque
The model for ECC IR torque was significant (F = 14.165, p < .001), explaining 25.0% of variance (adj. R2 = 0.250). ECC ER torque (β = 0.455) and height (β = −0.251) were significant predictors, with ECC ER torque demonstrating the greater influence (Table 4).
ECC ER torque
The regression model for ECC ER torque was significant (F = 20.559, p < .001), explaining 33.1% of the variance (adj. R2 = 0.331). Significant predictors included ECC IR torque (β = 0.404) and CON ER torque (β = 0.381), with ECC IR torque showing the stronger influence (Table 4).
Discussion
This study revealed that adolescent baseball players with GIRD exhibited significantly lower CON IR and ER torques, along with an increased ECC IR/CON ER ratio, compared to those without GIRD. Concentric torque values had moderate associations with GH joint rotational ROM, particularly IR ROM and the presence of GIRD, which were identified as key influencing factors. Among these variables, CON ER torque demonstrated the strongest association with CON IR torque and was also correlated with baseball experience and GIRD. In contrast, eccentric torque values were not significantly associated with GH joint ROM. However, ECC IR torque was influenced by ECC ER torque and participant height, whereas ECC ER torque was affected by both ECC IR and CON ER torques. These findings imply that shoulder rotational ROM and the balance between agonist and antagonist muscle groups are critical determinants of torque production in adolescent baseball players.
The GIRD group exhibited concentric torque values of approximately 34.8%BW for IR and 35.83%BW for ER, which were about 5%BW and 7%BW lower, respectively, than those observed in the non-GIRD group. This indicates an insufficient IR ROM may affect the IR and ER muscle force generation, particularly during concentric contraction. A plausible explanation for this reduced concentric torque in the GIRD group is diminished muscle strength resulting from limited ROM.23,46 Restricted IR ROM, i.e., 60.7° in the GIRD group compared to 75.1° in non-GIRD group, and a 6° reduction in total rotation may impaired optimal muscle length and joint mechanics, thereby reducing force generation in both IR and ER. These findings are supported by the observed poor-to-fair correlations between GH joint rotation ROM and concentric torque variables. Regression analysis also revealed a positive association between IR ROM and CON IR torque (β = 0.207), and a negative association between GIRD and CON ER torque (β = −0.229). These results support the hypothesis that limited ROM and shortened muscle length impair force production. Prior studies suggest that increased muscle length enhances energy absorption during eccentric contraction, thereby facilitating greater concentric force output.47,48 Thus, reduced IR and total rotation ROM in the GIRD group may have limited eccentric energy absorption, resulting in decreased concentric torque in both IR and ER muscles. While these reductions in torque are consistent with the proposed mechanism, their relatively small magnitude requires cautious interpretation, as they may overlap with measurement precision. Hill et al. 42 demonstrated ICC values between 0.73 and 0.93 in the supine position, supporting the reproducibility of this protocol and reinforcing the appropriateness of our measurement approach. However, Forthomme et al. 41 reported SEM values ranging from 2.2 to 6.7 N·m and SDD values between 6.2 and 18.6 N·m across different testing positions, indicating that small torque differences may fall within the bounds of measurement error. The effect sizes calculated in our study (ES = 0.72 for IR and ES = 0.95 for ER) nevertheless suggest moderate-to-large magnitudes, and diminished rotator strength has been linked to increased injury risk. 20 Taken together, the torque differences observed in our study may have clinical implications related to performance and injury risk, but they should be interpreted with caution in light of measurement precision.
Eccentric overload of posterior shoulder soft tissues has been linked to inflammatory responses and morphological changes that reduce muscle strength.7–9,49 GIRD is associated with stiffness and inflexibility caused by repetitive overhead throwing, leading to connective tissue damage, inflammation, and external rotator weakness.14,24,26 Guney et al. 26 reported lower eccentric ER torque (GIRD: 0.43 vs. non-GIRD: 0.75) and ECC ER/CON IR ratio in individuals with GIRD (GIRD: 0.55 vs. non-GIRD: 0.83), attributing this to a posterior-superior shift of the GH rotation axis. Previous studies have identified GIRD as a risk factor for throwing-related injuries with IR ROM differences of 18° 15 and a fourfold increase in injury risk when GIRD exceeds 25°. 19 Structural and strength alterations in rotator cuff muscles have also been documented in athletes with GIRD,20,25 including reduced ER strength and decreased supraspinatus and infraspinatus thickness. Yamaura et al. 25 reported a higher isometric IR strength ratio and a lower ER strength ratio of the throwing shoulder compared to the non-throwing shoulder in professional baseball players with GIRD, and further demonstrated reduced supraspinatus and infraspinatus muscle thickness in the GIRD group. Tyler et al. 20 reported that 57% of overhead athletes with a history of injury had a GIRD of more than 20°, and athletes with moderate injuries exhibited weakened isometric supraspinatus strength. Despite these previous findings, the present study found no significant differences in ECC IR or ER torque between groups, and no association between eccentric torque and GH joint ROM. Interestingly, the ECC ER/CON IR ratio showed a tendency to be higher in the GIRD group, which contrasts with prior reports of decreased ratios. Guney et al., 26 who examined adolescent volleyball and basketball athletes, found lower ECC ER torque and reduced ECC ER/CON IR ratios in the GIRD group (0.43 Nm) than the non-GRID group (0.75 Nm), but no significant differences in CON IR torque (GIRD: 0.81 Nm vs. non-GRID: 0.82 Nm). In contrast, our study did not observe differences in ECC ER torque between groups (GIRD: 41.6%BW vs. non-GIRD: 42.9%BW). Instead, we found a significant reduction in CON ER torque in the GIRD group. These distinct results likely contributed to the relatively higher ECC ER/CON IR ratio observed in our study. Regression analysis further indicated that ROM limitations may impair concentric torque generation, supporting the interpretation that reduced CON ER torque in the GIRD group was influenced by restricted mobility. Previous authors have suggested that eccentric overload of posterior shoulder soft tissues contributes to inflammatory responses and morphological changes that reduce muscle strength.7–9,49 Because our study included healthy adolescent baseball players without pain or prior injury, eccentric strength including ECC ER torque may not have been affected. This may explain why eccentric torque differences were not observed. Future studies should investigate how structural and pathological changes in posterior shoulder tissues influence eccentric torque generation. Methodological differences such as testing velocity (Our study: 120°/s vs. Guney et al. 26 : 90°/s) and testing position (Our study: supine vs. Guney et al. 26 : seated) may also have influenced torque outcomes. In our study, isokinetic torque was measured at a relatively higher angular velocity (120°/s), which, according to the force–velocity relationship, may have contributed to reduced concentric torque values, as concentric torque decreases with increasing velocity while eccentric torque tends to increase.50,51 In addition, eccentric torque measurements are known to be less reproducible and more susceptible to the influence of non-contractile tissue properties.52,53 Therefore, eccentric torque otucomes should be interpreted with caution, taking measurement reliability into consideration.
In this study, IR and ER torques demonstrated fair positive correlations with their respective antagonists in both concentric (r = 0.619) and eccentric (r = 0.454) contractions. Regression analysis revealed standardized coefficients of 0.538 for CON ER torque and 0.501 for CON IR torque, indicating mutual influence. For ECC IR torque, ECC ER torque exerted the greatest relative impact (β = 0.455), and similarly, ECC IR torque was the strongest predictor of ECC ER torque (β = 0.404). These findings imply that antagonist torque plays a significant role in agonist torque generation across both contraction types. In other words, higher antagonist torque was associated with greater agonist torque. Additionally, reciprocal influence was observed between concentric and eccentric ER torques. CON ER torque was the second strongest predictor of ECC ER torque (β = 0.381), while ECC ER torque was the second strongest predictor of CON ER torque (β = 0.438). These results suggest that strengthening antagonist muscles should be considered alongside IR and ER agonists when designing muscle training programs. Moreover, these results highlight the necessity of incorporating balanced training strategies that address both concentric and eccentric contractions for ER muscles. However, theoretical evidence explaining the mechanisms through which antagonist torque influences agonist torque remains limited. This relationship may not directly reflect physiological factors, such as muscle cross-sectional area, motor unit recruitment, firing rate, or energy metabolism. Although these are key determinants of muscle strength and power, their contributions were not confirmed in this study. Therefore, further research is warranted to elucidate the interactions between these physiological factors and torque generation. In addition to these strength-related findings, regression analysis emphasized the critical role of joint mobility in concentric torque generation. Specifically, IR ROM (β = 0.207) and the presence of GIRD (β = −0.229) were significant contributors to concentric torque production, indicating that mobility parameters complement muscular strength in determining shoulder performance. Accordingly, effective athlete management should encompass both the strengthening of agonist and antagonist muscles and targeted interventions to improve IR ROM, such as posterior shoulder stretching. Taken together, these strategies may help prevent shoulder dysfunction and support performance enhancement in adolescent baseball players with GIRD.
There are several limitations of this study. First, the physiological length characteristics of intramuscular soft tissue were not directly investigated. Examining correlations that incorporate additional factors influencing muscle strength, such as changes in muscle length at the musculotendinous junction, will be necessary to clarify further the relationship between GH joint ROM alterations and muscle torque. Second, we did not investigate concentric and eccentric torque in relation to other potential contributing factors, including risk factors for throwing-related injuries or scapular kinetics and kinematics. Therefore, future studies are needed to determine more clearly the causal relationship among the factors contributing to CON and ECC IR and ER muscle strength by accounting for these additional variables.
Conclusion
This study found that CON IR and ER torques were significantly reduced in athletes with GIRD compared to those without GIRD, and were closely associated with GH joint rotational ROM. IR ROM and the presence of GIRD emerged as key factors influencing concentric torque generation. Additionally, both concentric and eccentric torque production demonstrated strong interdependence between agonist and antagonist muscles, underscoring the role of the antagonist in supporting agonist strength. In contrast, ECC IR and ER torques did not differ significantly between groups and showed no meaningful correlation with GH joint ROM. These findings imply that evaluating IR ROM loss and GIRD, together with management strategies such as posterior shoulder stretching to improve IR ROM, may be essential for enhancing concentric IR and ER strength. Importantly, strengthen antagonist muscles within the same contraction type should be incorporated for both IR and ER, while the reciprocal influence observed between concentric and eccentric ER torques highlights the necessity of balanced training across both contraction modes. This integrated approach may provide a comprehensive strategy to optimize shoulder function in adolescent baseball players with GIRD.
Footnotes
Acknowledgements
We would like to thank everyone who contributed to this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Global Joint Research Program funded by the Pukyong National University (202412370001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.