
Abstract
Background
This cross-sectional study aimed to investigate how different hip abduction angles influence hip abduction torque and muscle activation of the gluteus medius (Gmed) and tensor fasciae latae (TFL) during side-lying hip abduction in individuals with Gmed weakness.
Methods
Twenty-five individuals with Gmed weakness participated in this study. Participants performed isometric hip abduction in a side-lying position at four joint angles (−15°, 0°, 15°, and 30°). Hip abduction torque was measured using an isokinetic dynamometer, while surface electromyography was used to simultaneously record Gmed and TFL muscle activities. The Gmed/TFL activity ratio was calculated to examine relative activation patterns. Hip abduction torque was normalized to body weight.
Results
Peak hip abduction torque was greatest at −15°, followed by 0°, 15°, and 30°. Electromyographic analysis showed that Gmed activity was greater at −15° and 0° than at 30°, whereas TFL activity was lowest at 30°. Although no significant pairwise differences were detected, the Gmed/TFL activity ratio tended to increase with increasing hip abduction angle, reaching its highest value at 30°.
Conclusion
Hip abduction angle influences hip abduction torque and muscle activation during side-lying hip abduction in individuals with Gmed weakness. A more adducted starting position was associated with greater torque, whereas a more abducted position showed lower TFL activity and higher Gmed/TFL ratios; thus, hip abduction angle may be considered in rehabilitation, with caution.
Introduction
The gluteus medius (Gmed) is a key hip abductor that plays a critical role in pelvic stabilization during unilateral weight-bearing activities. 1 It functions eccentrically to control hip adduction and internal rotation, thereby preventing excessive pelvic drop.2,3 In particular, the Gmed contributes to maintaining pelvic stability by regulating hip motion during dynamic tasks such as walking and running. 1 Weakness of the Gmed is often accompanied by compensatory overactivation of the tensor fasciae latae (TFL), leading to altered biomechanics such as increased hip internal rotation and knee valgus. 4 These maladaptive movement patterns are associated with a higher risk of iliotibial band syndrome, 5 patellofemoral pain, 6 and anterior cruciate ligament injuries. 4 Consequently, in clinical and rehabilitative settings, it is important to implement exercise interventions that promote preferential activation of the Gmed relative to the TFL, while limiting excessive TFL activation that may contribute to undesirable hip internal rotation, to improve movement control and functional outcomes. 7 Accordingly, rehabilitation programs commonly incorporate targeted hip abductor exercises aimed at restoring Gmed function before progressing to more demanding weight-bearing functional tasks, such as walking, running, single-limb squatting, and landing activities. 4
Side-lying hip abduction is widely used in rehabilitation to promote selective activation of the Gmed while minimizing compensatory activation of the TFL. 8 This exercise allows for biomechanical modifications that can optimize Gmed recruitment. For example, performing the movement with slight hip extension positions the TFL at a mechanical disadvantage while facilitating activation of the posterior fibers of the Gmed. 7 Similarly, adopting a position of hip internal rotation has been shown to increase Gmed activation and improve the Gmed/TFL activation ratio. 9 In addition, maintaining a neutral pelvic position is critical for limiting compensatory activation of surrounding muscles, such as the TFL and quadratus lumborum, thereby enhancing selective Gmed activation. 10 Collectively, these biomechanical conditions make side-lying hip abduction a useful exercise for targeting the Gmed and support its frequent use in rehabilitation settings, particularly in individuals with Gmed weakness.
Among these factors, hip abduction angle has been suggested as an important variable affecting muscle activation patterns. 7 Previous studies using magnetic resonance imaging have demonstrated that the activation levels of the superficial and deep layers of the gluteus medius vary depending on the hip abduction angle maintained during isometric contractions. 11 In addition, variability in electromyographic findings across studies has been partly attributed to differences in testing positions, including the angle of hip abduction. 12 From a biomechanical perspective, such variations may be explained by changes in the length–tension relationship of the hip abductor muscles, which can influence their relative contributions. 13 Accordingly, certain abduction angles may place the Gmed at a mechanical advantage, whereas others may facilitate greater involvement of the TFL. However, few studies have directly compared the relative activation of the Gmed and TFL across different hip abduction angles.
This issue may be particularly relevant in individuals with Gmed weakness, who are more prone to compensatory activation of the TFL, resulting in altered movement patterns and impaired pelvic control. 5 In such cases, side-lying hip abduction is frequently used to facilitate Gmed activation while minimizing compensatory strategies and restoring proper hip joint control. 8 However, the effects of hip abduction angle on muscle activation patterns, including functional outcomes such as torque production, in this population remain unclear. Therefore, the purpose of this study is to examine the effect of different isometric hip abduction angles on hip abduction torque, Gmed and TFL muscle activity, and the Gmed/TFL activation ratio during side-lying hip abduction in individuals with Gmed weakness.
Patients and methods
Patients
This cross-sectional study was conducted between July 2024 and February 2025. Participants were recruited from the university community. The inclusion criteria were: (1) males aged 20–39 years and (2) the presence of gluteus medius weakness defined as a manual muscle testing (MMT) grade ≤3 according to the Hislop and Montgomery scale. 14 A total of 37 participants were initially recruited for screening. Both lower limbs were screened for Gmed weakness using MMT, and when both limbs met the inclusion criteria, the limb with the lower MMT score was selected for testing. If both limbs had the same MMT grade, the preferred limb (i.e., the leg used to kick a ball) was selected. Of the initially recruited participants, 25 met the inclusion criteria and were included in the final analysis. All participants were classified as recreationally active (Tier 1) according to an established participant classification framework and current physical activity guidelines. 15 Individuals with inflammatory arthritis, lower extremity injury, current low back pain or a history of lumbar spine disorders diagnosed by a healthcare professional, or an inability to maintain isometric hip abduction for at least five seconds in a side-lying position were excluded. 16 All participants provided written informed consent prior to study participation, and the study protocol was approved by the Institutional Review Board(Approval No. 1041386-202403-HR-37-02).
Assessment of Gmed weakness
The Gmed manual muscle test was performed using a manual break test as described by Hislop and Montgomery. 17 Participants were positioned in a side-lying position with the tested hip abducted and slightly extended, the pelvis rotated slightly forward, and the lower extremity on the bottom side flexed for stabilization, while the tested leg remains aligned with the trunk. 1 Manual resistance is applied at the ankle in the direction of hip adduction. Prior to testing, participants are instructed to avoid hip flexion, internal rotation, or compensatory pelvic movements involving the quadratus lumborum or TFL muscle. To further minimize compensatory actions, the trunk and pelvis are secured with a strap. After a familiarization trial, a 3-min rest period is provided before the test. Muscle strength is graded on a 0–5 scale according to Hislop and Montgomery, 17 with grades ≤3 classified as weak and grades ≥4 classified as strong. 18
Peak torque across side-lying hip abduction angles
Hip abduction peak torque in the side-lying position was measured using a Biodex dynamometer (Biodex Systems 4 Pro, Biodex Medical Systems, Shirley, NY). Participants were positioned in a side-lying position with their back facing the dynamometer, in accordance with the manufacturer's instructions (Figure 1(a)). The dynamometer's axis of rotation was aligned approximately 3–4 cm above the midpoint between the greater trochanter of the femur and the pubis. 19 For comfort and stability, a standard belt was applied, and the contralateral hip and knee joints were flexed. The initial hip abduction angle was set to 0° based on the isokinetic dynamometer. Testing was then conducted at −15° (15° of adduction), 0°, 15°, and 30° of hip abduction. During each trial, participants were instructed to maintain the test position without hip flexion, external rotation, or compensatory pelvic movements. At each angle, maximal voluntary isometric contraction was performed three times for 5 s per trial, with 30 s of rest between trials and 5 min between angle conditions. 20 Hip abductor torque was normalized to body weight (peak torque/body weight, PT/BW; unit: Nm/kg), and the mean value from the three repetitions at each angle was used for analysis. To minimize fatigue and learning effects, the order of testing angles was randomized using Excel-generated random numbers. All measurements were performed by the same examiner, and participants received standardized verbal encouragement throughout testing. 19
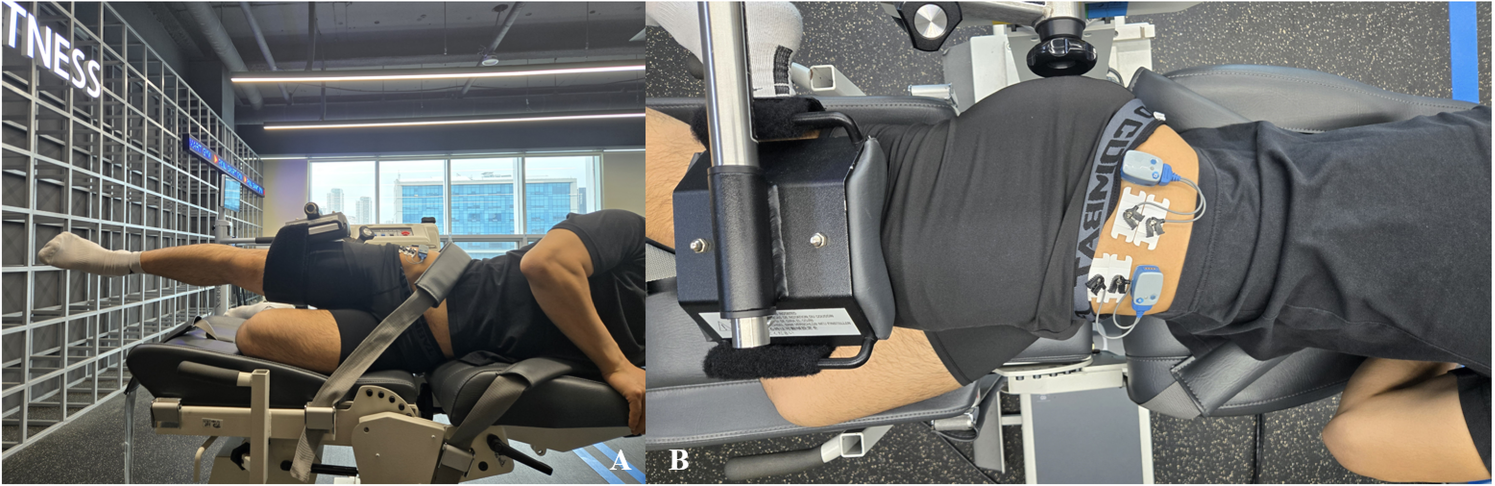
Experimental setup for side-lying hip abduction torque and EMG recording. (a) Participant positioning and dynamometer alignment during isometric side-lying hip abduction testing at 0°. (b) Surface EMG electrode placement for the gluteus medius (Gmed) and tensor fasciae latae (TFL) based on anatomical landmarks.
The muscle activities of Gmed and TFL during side-lying hip abduction were recorded simultaneously with peak torque measurements using a two-channel wireless surface electromyography (EMG) system (Ultium EMG System, Noraxon, USA). EMG and torque signals were recorded simultaneously, and the EMG system was synchronized with the dynamometer to ensure that both signals corresponded to the same contraction period. To minimize skin–electrode impedance, hair at the electrode sites was removed with a razor, and the skin was cleaned with medical alcohol swabs before attaching disposable Ag/AgCl surface electrodes (10-mm conductive area) with an interelectrode distance of 20 mm (1). For the Gmed, electrodes were placed at the midpoint between the uppermost aspect of the iliac crest and the greater trochanter, and for the TFL, electrodes were positioned at one-sixth of the distance from the anterior superior iliac spine to the greater trochanter, according to previously published recommendations for hip abductor EMG recording 19 (Figure 1(b)). EMG measurements were obtained while participants exerted maximal voluntary isometric contractions against the dynamometer at four hip abduction angles (−15°, 0°, 15°, and 30°) in the side-lying position. Each condition was performed three times for 5 s, with the first and last seconds discarded; only the middle 3 s of data were analyzed. EMG signals were sampled at 2000 Hz, band-pass filtered at 20–450 Hz, and notch-filtered at 60 Hz. 1 Processed data were converted to root mean square (RMS) values (unit: mV) using a 100-ms moving window in Noraxon MyoResearch Master Edition 1.08 XP software (Noraxon, Inc., Scottsdale, AZ, USA). 19 Because measurements were obtained during maximal voluntary isometric contractions under consistent electrode placement and testing conditions, RMS amplitudes were analyzed in mV to examine angle-dependent changes within each muscle. The RMS values obtained from the three trials at each hip abduction angle were averaged and used for statistical analysis. The Gmed/TFL ratio (unit: %) was calculated by dividing Gmed RMS amplitude by TFL RMS amplitude and multiplying by 100 to describe relative activation patterns.
Statistical analyses
All statistical analyses were performed using R software (version 4.5.2; R Foundation for Statistical Computing, Vienna, Austria). Normality of the data was confirmed prior to analysis, and parametric statistical procedures were therefore applied. A one-way repeated-measures analysis of variance (ANOVA) was used to compare isometric hip abduction peak torque and the Gmed/TFL activation ratio across four hip abduction angles (−15°, 0°, 15°, and 30°). To further examine muscle-specific responses to hip abduction angle, an additional two-way repeated-measures ANOVA with angle (−15°, 0°, 15°, and 30°) and muscle (Gmed and TFL) as within-subject factors was conducted for electromyographic activity. When significant main or interaction effects were identified, pairwise comparisons were conducted with Bonferroni adjustment. Greenhouse–Geisser corrections were applied where appropriate, and effect sizes were reported as partial eta squared (ηp2). Statistical significance was set at α = 0.05.
Results
A total of 25 male participants with gluteus medius weakness were included in this study. The participants’ mean (±standard deviation) age, height, weight, and body mass index (BMI) were 24.96 ± 2.56 years, 175.84 ± 5.23 cm, 79.28 ± 8.58 kg, and 25.61 ± 2.31 kg/m2, respectively. According to the Hislop and Montgomery manual muscle testing scale, 7 participants (28.0%) had grade 1, 10 (40.0%) had grade 2, and 8 (32.0%) had grade 3 gluteus medius weakness (Table 1).
Participant characteristics.

Participant characteristics.
BMI, body mass index; Gmed, Gluteus medius; MMT, manual muscle test.
Values are presented as mean ± standard deviation for Age, Height, Weight, and BMI, and as counts (percentages) for Gmed MMT grade.
First, body weight–normalized peak hip abduction torque differed significantly across hip abduction angles (F(2.22, 53.24) = 241.13, p < 0.001, ηp2 = 0.91). Bonferroni-adjusted post hoc comparisons revealed that peak hip abduction torque at −15° was significantly greater than at 0° (mean difference = 36.16 Nm/kg, p < 0.001), 15° (mean difference = 59.30 Nm/kg, p < 0.001), and 30° (mean difference = 82.48 Nm/kg, p < 0.001). In addition, torque at 0° was significantly greater than at 15° (mean difference = 23.14 Nm/kg, p < 0.001) and 30° (mean difference = 46.32 Nm/kg, p < 0.001), and torque at 15° was significantly greater than at 30° (mean difference = 23.18 Nm/kg, p < 0.001). Overall, peak hip abduction torque progressively decreased as hip abduction angle increased (Figure 2).
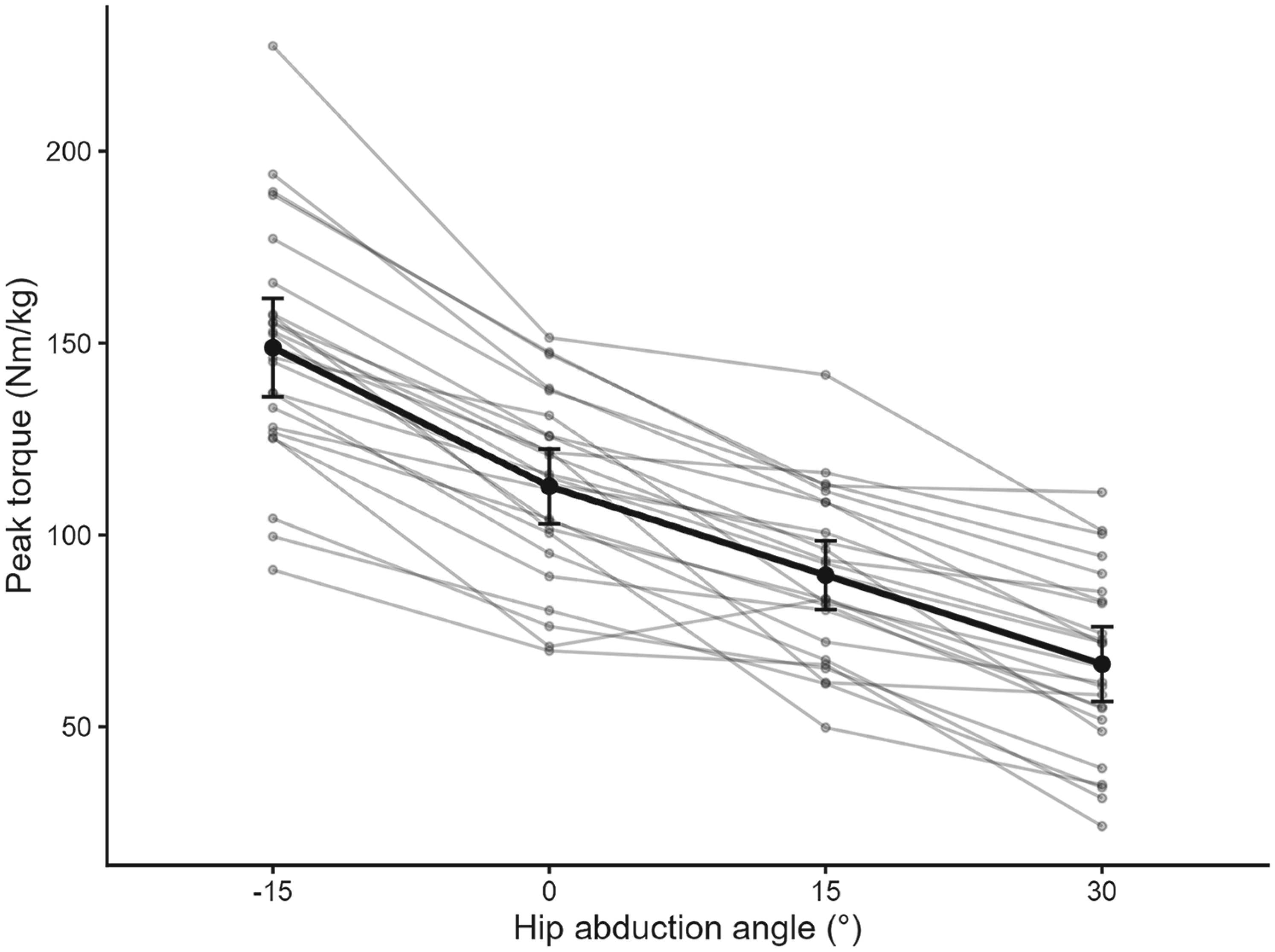
Peak hip abduction torque across hip abduction angles. Individual participant data are shown as thin gray lines, and group means are shown as black circles connected by a solid line. Error bars represent 95% confidence intervals. A significant main effect of hip abduction angle was observed (p < 0.001), with peak torque progressively decreasing as hip abduction angle increased.
Next, electromyographic activity demonstrated muscle-specific responses across hip abduction angles (Figure 3). Significant main effects of hip abduction angle and muscle were observed, along with a significant angle × muscle interaction (F(2.48, 59.59) = 11.48, p < 0.001, ηp2 = 0.32; TableS1). Bonferroni-adjusted post hoc analyses showed that Gmed activity at −15° was significantly greater than at 15° (mean difference = 14.20 mV, p = 0.032) and 30° (mean difference = 31.01 mV, p < 0.001), and Gmed activity at 0° was significantly greater than at 30° (mean difference = 27.00 mV, p < 0.001). In contrast, TFL activity did not differ significantly among −15°, 0°, and 15° (all p > 0.05), but was significantly lower at 30° compared with −15° (mean difference = 74.48 mV, p < 0.001), 0° (mean difference = 60.68 mV, p < 0.001), and 15° (mean difference = 43.15 mV, p = 0.011).
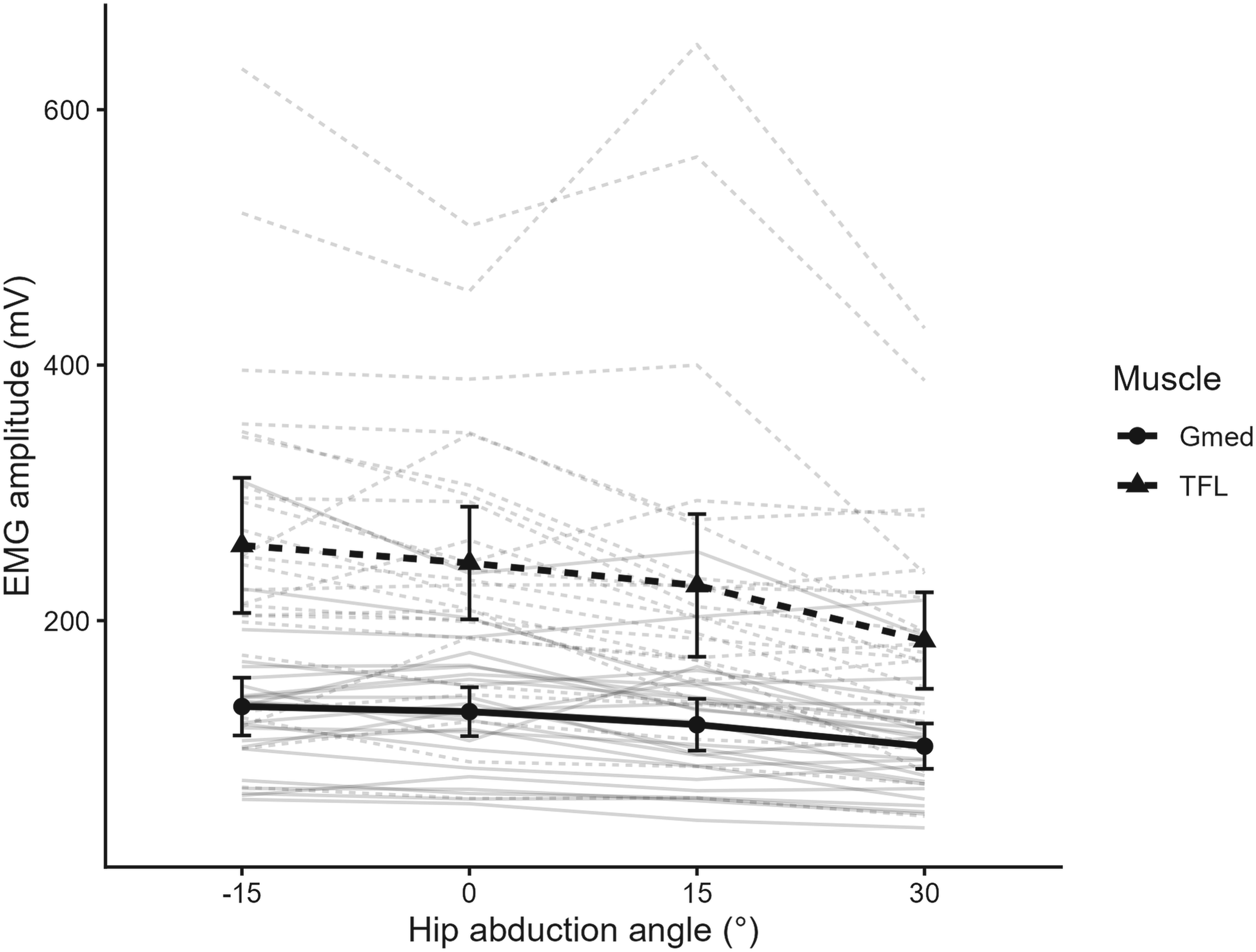
Electromyographic activity of the gluteus medius (Gmed) and tensor fasciae latae (TFL) across hip abduction angles during side-lying hip abduction. Thin gray lines represent individual participant data, and bold lines with symbols represent group means. Error bars indicate ± 95% confidence intervals. A significant angle × muscle interaction was observed (p < 0.001), indicating distinct, angle-dependent activation patterns of the Gmed and TFL.
Finally, the Gmed/TFL muscle activity ratio showed a significant main effect of hip abduction angle (F(2.00, 48.12) = 3.46, p = 0.039, ηp2 = 0.13; Figure 4). Bonferroni-adjusted post hoc comparisons did not reveal significant pairwise differences between angles (all p > 0.05); however, the mean Gmed/TFL ratio tended to increase with increasing hip abduction angle, with the highest mean value observed at 30° (62.23 ± 30.19%) compared with −15° (57.52 ± 25.26%).
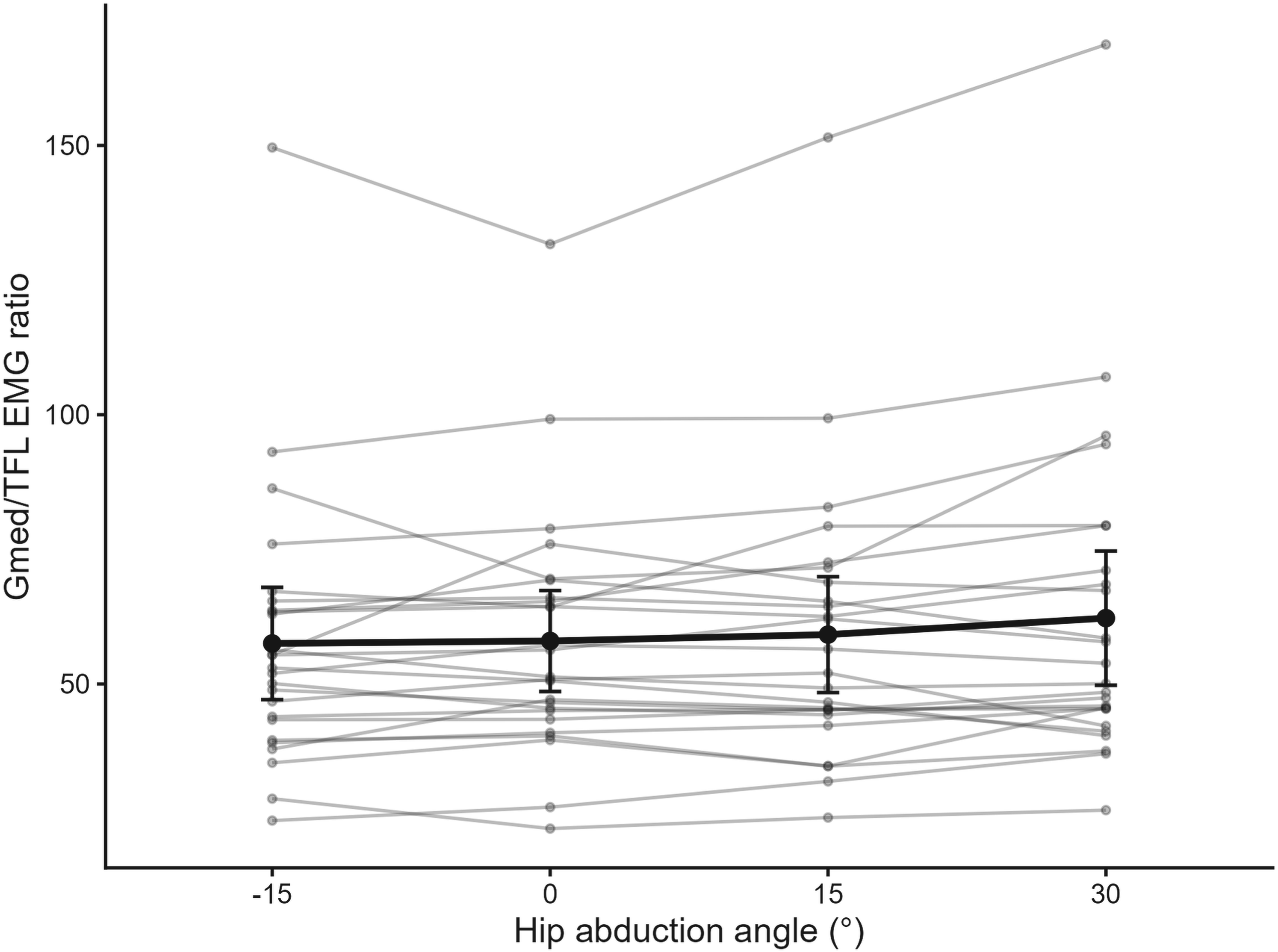
Ratio of gluteus medius (Gmed) to tensor fasciae latae (TFL) electromyographic activity across hip abduction angles during side-lying hip abduction. Thin gray lines represent individual participant data, and bold black lines with symbols represent group means. Error bars indicate ± 95% confidence intervals. The Gmed/TFL ratio showed an overall effect of hip abduction angle, with a tendency toward higher values at larger abduction angles.
This study investigated the effects of varying isometric side-lying hip abduction angles (−15°, 0°, 15°, and 30°) on hip abduction torque, Gmed and TFL muscle activities, and the Gmed/TFL activity ratio in individuals with Gmed weakness. The findings demonstrated clear angle-dependent differences in hip abduction torque and muscle activation. Peak hip abduction torque and absolute EMG activities of both the Gmed and TFL were greater at lower abduction angles, whereas the Gmed/TFL activity ratio tended to increase at higher abduction angles. Collectively, these results suggest that hip abduction angle influences both force production and activation patterns during isometric side-lying hip abduction. Notably, the Gmed and TFL showed angle-dependent changes in activation, indicating that joint position may influence the activation of hip abductor muscles during this task.
The muscle length–tension relationship influences muscle torque, as joint angle changes alter muscle length, resulting in reduced torque at the extremes of motion and maximal torque at mid-lengths corresponding to functional demand.1,3,20 This principle also applies to side-lying hip abduction, where changes in abduction angle modify the lengths of the hip abductors. 3 Kindel and Challis 20 demonstrated a negative slope in the hip abduction torque–angle curve (−0.014 Nm/kg/degree), showing decreasing torque with increasing abduction angle in healthy adults. Similarly, another study using a portable dynamometer confirmed that torque decreased progressively from −10° (87.7 Nm) to 40° (45.2 Nm) of abduction. 21 Consistent with these findings, our results showed that hip abduction torque decreased as the abduction angle increased from −15° (148.81 ± 31.05 Nm/kg) to 0° (112.64 ± 23.58 Nm/kg), 15° (89.51 ± 21.77 Nm/kg), 30° (66.32 ± 23.64 Nm/kg). These results suggest that neutral or adducted positions, rather than the commonly used 30° position in side-lying hip abduction exercise, allow the length–tension relationship to optimize hip abduction torque generation.20,21 Importantly, because participants with Gmed weakness showed patterns similar to those of healthy individuals, adopting a neutral or adducted hip position may provide a favorable mechanical condition for hip abductor strengthening in this population.
The internal torque generated by a muscle is influenced by both the muscle length–tension relationship and its moment arm (MA).22–24 Although an increased MA theoretically enhances torque production, 25 our findings, consistent with previous studies, showed greater hip abductor torque in neutral and adducted positions, where the MA is reduced.20,21 This suggests that torque production is driven more by the length–tension relationship than by MA alone, particularly in positions that reflect functional demands such as walking. 3 In support of this, our results demonstrated progressively greater absolute EMG activity of the Gmed and TFL as the hip abduction angle decreased, with the highest activity observed at −15°. This may reflect both active and passive contributions from the iliotibial band in this position. Similarly, previous work has shown that optimizing Gmed length results in approximately 12% higher activity compared with a shortened position, 1 reinforcing the role of muscle length–tension dynamics. Given that most prior studies examined hip abduction torque and Gmed strengthening at 30°,8,26,27 the present findings suggest that neutral and adducted positions in the coronal plane may provide favorable conditions for torque assessment and hip abductor exercise in individuals with Gmed weakness.
In individuals with Gmed weakness, identifying the posture and hip abduction angle that generate greater torque and favorable activation of the hip abductors is clinically relevant, as it may help minimize compensatory activation of the TFL and facilitate more selective recruitment of the Gmed. 10 In addition, the relationship between Gmed and TFL activation may be important because excessive TFL activity has been associated with lower-extremity disorders such as osteoarthritis, patellofemoral pain, and iliotibial band syndrome.1,28 In our study, the Gmed/TFL activity ratio during side-lying hip abduction ranged from 0.80% to 1.21%, which was lower than values previously reported in individuals without Gmed weakness (1.13–1.46), suggesting relatively greater TFL activation in this population.1,9,26,29 Although both Gmed and TFL activities were lowest at 30° compared with other angles, the Gmed/TFL ratio tended to increase with greater abduction angles (−15°: 57.52%, 0°: 57.98%, 15°: 59.16%, and 30°: 62.23%). This pattern reflects a relatively larger reduction in TFL activity (29%) than in Gmed activity (24%) from −15° to 30°, which may be related to reduced passive tension in the iliotibial band at higher abduction angles. 3 Although the 30° position did not maximize torque generation or Gmed activation, it showed a tendency toward higher Gmed/TFL ratios. These findings suggest that hip abduction angle may influence the relative activation patterns of the Gmed and TFL during side-lying hip abduction. To our knowledge, no previous studies have examined the Gmed/TFL activity ratio according to hip abduction angle during side-lying exercise, limiting direct comparisons with other work. Nevertheless, the present findings suggest that hip abduction angle selection may be adjusted according to rehabilitation goals, such as emphasizing torque generation or considering relative activation patterns during exercise.
From a clinical perspective, the present findings suggest that hip abduction angle may be a factor to consider when selecting exercise conditions based on rehabilitation goals. Lower abduction angles were associated with greater torque production, which may be beneficial when the primary goal is to enhance hip abductor torque. In contrast, higher abduction angles showed a tendency toward higher Gmed/TFL ratios; however, given the limitations related to Gmed/TFL activation, this finding should be interpreted with caution and may have limited applicability when considering activation patterns during early-stage rehabilitation exercises.
This study has several limitations. First, because it employed a cross-sectional design, we cannot determine the long-term effects of hip abduction angle on hip abduction torque or on Gmed and TFL muscle activities. Second, the participants were limited to young adults (20–39 years), and the relatively small sample size may further limit the generalizability of the findings to other age groups and populations, including older adults, females, and clinical populations with hip pathology. Third, the study examined only isometric contractions in a controlled side-lying position, which may not fully reflect the dynamics of functional tasks such as gait, single-leg stance, or sport-specific movements. In addition, we did not include kinetic or kinematic analyses that could have provided complementary insights into hip joint mechanics. Fourth, only one limb was tested in each participant, which prevented comparison with the contralateral limb that could potentially serve as an internal control. Finally, EMG amplitudes were analyzed as RMS values (mV) rather than normalized to a separate reference contraction for each muscle; therefore, comparisons between the Gmed and TFL and interpretation of the Gmed/TFL ratio should be made with caution. Future research should therefore extend these findings by including broader and more diverse populations, investigating dynamic and functional tasks, and examining long-term training adaptations to angle-specific hip abduction exercise. Moreover, studies integrating musculoskeletal modeling or imaging could further clarify the relationships between muscle length–tension properties, moment arms, and muscle activation patterns.
Conclusion
This study demonstrated that hip abduction angle influences hip abduction torque and the relative activation of the Gmed and TFL in individuals with Gmed weakness. Performing hip abduction from a more adducted starting position relative to neutral (e.g., −15°) resulted in greater torque and higher EMG activity of both muscles, whereas a more abducted starting position (e.g., 30°) was associated with lower TFL activity and a tendency toward higher Gmed/TFL ratios. Accordingly, hip abduction angle may be considered when selecting exercise conditions in rehabilitation settings; however, these findings should be interpreted with caution given the limitations related to Gmed/TFL activation.
Supplemental Material
sj-docx-1-iso-10.1177_09593020261456715 - Supplemental material for Impact of isometric hip abduction angle on isolated hip abductor muscle work in gluteus medius weakness
Supplemental material, sj-docx-1-iso-10.1177_09593020261456715 for Impact of isometric hip abduction angle on isolated hip abductor muscle work in gluteus medius weakness by Na-Dan Lim, Tae-Gyu Kim, Il-Young Yu, Gi-Bin Kim, Hao Ren and Hokyung Choi in Isokinetics and Exercise Science
Footnotes
Acknowledgements
The authors thank all participants for their commitment to this study and the staff of the biomechanics laboratory for their technical support. We also acknowledge the contributions of colleagues who provided helpful comments during the development of this manuscript.
Ethical approval and informed consent statements
Institutional review board of Pukyong National University (No. 1041386-21080710-HR-023-03).
Authors contributions
ND Lim and HK Choi was responsible for the study conception and design, data collection, statistical analysis, and manuscript drafting. TG Kim contributed to the interpretation of the data, critical revision of the manuscript, and supervision. IY Yu, GB Kim, and H Ren contributed to data collection and manuscript review. All authors approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Global Joint Research Program funded by the Pukyong National University (Grant No. 202412370001).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data are not publicly available due to ethical restrictions and the protection of participants’ privacy but are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.