
Abstract
This study aimed to investigate the relationship between the break-point angle (BPA) measured with the Nordic Angle app and absolute and relative eccentric knee flexion peak torques. Twenty-one male participants performed Nordic hamstring exercise (NHE) trials to determine their BPA, followed by absolute eccentric knee flexion strength testing. Absolute eccentric knee flexion peak torque was divided by body weight to calculate relative eccentric knee flexion peak torque. No Pearson correlation was observed between BPA and absolute eccentric knee flexion peak torque (rp = −0.05, p = 0.85). Conversely, the Pearson correlation between BPA and relative eccentric knee flexion peak torque was significant (rp = −0.54, p < 0.05). BPA measured with the Nordic Angle application was associated with relative eccentric knee flexor peak torque. As this study did not include a clinical population nor investigate hamstring injury incidence, clinical implications should be interpreted cautiously, and future research is required to determine whether BPA can predict hamstring injury risk.
Introduction
Hamstring injuries are common in track and field, 1 soccer, 2 rugby, 3 and baseball. 4 Notably, returning to play takes an average of 15–105 days for professional rugby players. 3 Because return–to–play duration varies substantially depending on injury severity, injury type, and other study–specific factors, briefly acknowledging this variability helps avoid oversimplification. When these injuries occur close to a competition, athletes may lose the opportunity to perform. Therefore, hamstring injury prevention through conditioning is crucial.
The Nordic hamstring exercise (NHE) is a conditioning method used to prevent hamstring injuries. 5 Specifically, it imposes an eccentric load on the hamstring muscles by leaning the upper body forward from a kneeling position. The point at which hamstring strength can no longer resist the eccentric load associated with forward upper body lean is termed the break-point angle.6–9 Specifically, in the present study, the break–point angle (BPA) was operationally defined as the knee joint angle at which knee extension velocity exceeded 10–20°/s, following previous studies that used heterogeneous velocity thresholds.6–8 In addition, BPA was calculated as the mean angle ± 2 standard deviations (SDs) across trials for each participant. 9 Previous studies reported moderate to very large correlations (rp = 0.49–0.88, p < 0.001) between absolute eccentric knee flexion peak torque and BPA.6–8 Nevertheless, a previous study reported no correlation between absolute eccentric knee flexion peak torque and BPA. 9 However, differences in methodological approaches—such as the operational definition of BPA, measurement instrumentation, and loading conditions—make direct comparison across studies difficult. Thus, rather than indicating clear disagreement, the current evidence reflects methodological inconsistency, and a consensus regarding the relationship between absolute eccentric knee flexion peak torque and BPA has yet to be established.
Eccentric knee flexion peak torque relative to body mass (relative eccentric knee flexion strength) at 30–60°/s can predict the risk of hamstring injury.10,11 Although these velocities are higher than those typically observed during the NHE, they are widely used to assess maximal eccentric hamstring capacity under standardized and reliable conditions. Because BPA during the NHE reflects an individual's ability to tolerate eccentric loading, comparing it with isokinetic eccentric peak torque at these velocities provides a meaningful reference for evaluating overall eccentric hamstring function, even if the movement speeds differ. For instance, Lee et al. conducted a prospective study of 146 professional male soccer players to investigate whether relative eccentric knee flexion peak torque predicted future hamstring injury risk, 11 and demonstrated the hamstring injury risk increased by 5.6-fold when the relative eccentric knee flexion peak torque was below 2.4 Nm/kg. Importantly, if BPA during NHE can predict relative eccentric knee flexion peak torque, it may offer benefits to athletes. Nevertheless, studies examining the relationship between BPA and relative eccentric knee flexion peak torque are lacking. Because peak knee flexion force during the NHE may depend on body mass,12,13 BPA during the NHE may be less informative in individuals with high absolute eccentric knee flexion peak torque but low body mass because BPA may approach the floor/ceiling constraint at 0° (0° indicates full knee extension). To achieve true absolute knee flexion peak torque in participants with BPA values near 0° during the NHE, an external load is likely necessary. 14 Moreover, adding an external load reportedly increases BPA. 15 Conceptually, because the NHE is a body–weight exercise, the torque demand at the knee is inherently scaled to body mass; thus, BPA reflects the point at which an individual's eccentric knee flexor capacity is exceeded relative to their body mass. Therefore, BPA may correlate with relative rather than absolute eccentric knee flexion peak torque. 9
Recently, the Nordic Angle application was developed to enable BPA measurements during NHE on iOS devices. Soga et al. examined BPA validity with the Nordic Angle application and reported it was valid.16,17 However, no study reported the relationship between BPA measured using the Nordic Angle application and relative eccentric knee flexion peak torque measured with an isokinetic dynamometer. Therefore, this study aimed to investigate the relationship between BPA measured using the Nordic Angle application and absolute and relative eccentric knee flexion peak torques. We hypothesized that BPA would show a negative correlation with relative, rather than absolute, eccentric knee flexor peak torque.
Methods
Experimental approach to the problem
This study adopted a single-visit cross-sectional design. The participants performed an NHE trial followed by an eccentric knee flexion trial. BPA measurements during the NHE were performed using the Nordic Angle app. Eccentric knee flexion peak torque was measured using an isokinetic dynamometer. This study investigated the relationship between the BPA and absolute and relative eccentric knee flexion peak torques.
Subjects
G Power (version 3.1.9.7; Heinrich Heine Universität, Düsseldorf, Germany) was used to estimate required sample sizes. Sample sizes were a priori calculated based on the parameters of Pearson's correlation coefficient analysis (correlation ρ H1 = 0.6, alpha = 0.05, and power = 0.8).6–8 The required sample size was determined to be 19 participants.
Twenty-one male participants (21.5 ± 2.9 years, 171.3 ± 5.6 cm, and 70.2 ± 12.6 kg) majoring in sports science were recruited. Twenty participants reported using their right leg as the dominant leg for kicking, whereas only one participant reported using their left. The inclusion criteria required participants to be healthy males aged 18–35 years engaged in physical activity without musculoskeletal pain, while the only exclusion criterion was the inability to perform NHE due to a current injury. One participant had a right-leg anterior cruciate ligament injury three years prior but was asymptomatic, had fully returned to sport, and demonstrated no strength asymmetry greater than 15%. The remaining participants had no history of hamstring or anterior cruciate ligament injuries. The Ethics Committee of [blinded] approved the experimental protocol (approval number: [blinded]). All procedures were performed in accordance with the Declaration of Helsinki. The study purpose and procedures were explained to the participants, and informed consent was obtained. Prior to data collection, all participants were informed of the study purpose, procedures, potential risks, and their right to withdraw at any time. Written informed consent was obtained from all participants.
Procedures
The participants initially performed a static hamstring stretch (standing hamstring stretch on one leg) with a 20–s hold on each leg as a warm–up. After the warm–up, the participants performed three consecutive repetitions of the NHE at 20%, 50%, and 80% of perceived maximal effort, with no external feedback provided (e.g., no verbal cues or visual feedback regarding force output). Once the participants were ready, an initial NHE trial was conducted with maximum effort. Three NHE trials were conducted, with a 3-min rest period between them. The participants assumed a kneeling position on a step box with their elbows bent and hands open in front of them (Figure 1). Moreover, a non-elastic strap with a cushion pad was wrapped around the lateral malleolus. 6 Participants leaned forward slowly while maintaining a straight posture from the knees to the head.

The screen on the Nordic angle app. θ1 indicates the knee flexion angle. θ2 indicates the knee flexion angle. Hip angle at break-point indicates the hip flexion angle at break-point.
Approximately 10 min after the NHE trials, participants completed a familiarization set for eccentric knee flexion measurements, consisting of two sets of three repetitions at submaximal effort. In the first set, participants maintained an effort level of 20% of perceived maximal effort. In the second set, the effort was progressively increased to 20%, 50%, and 80% of perceived maximal effort, with no external feedback provided (e.g., no verbal cues or visual feedback regarding force output). After this familiarization set, the participants performed two sets of three consecutive repetitions with maximum effort. The rest period between the familiarization and trial sets was 1 min. Eccentric knee flexor peak torque was measured in a randomized order for both the right and left legs.
Kinematic data
An iPhone camera (iPhone 15, Apple Inc., USA) was set to 60 fps and positioned approximately 3 m from the right side of the participant at a height of approximately 0.6 m. The Nordic Angle application was used to calculate the BPA and hip flexion angle at the BPA (HFA-BPA) during the NHE (Figure 1).16,17 A successful trial was defined as an HFA-BPA < 30° (<24.7° in this study). 18 The knee and hip flexion angles were measured anatomically, with 0° indicating fully extended knees and hips. The BPA values from three NHE trials were averaged.
Eccentric knee flexion peak torque
Eccentric knee flexion peak torque was measured using an isokinetic dynamometer (Biodex System 4; Biodex Medical Systems). The examiner informed participants about the characteristics of the dynamometer. During the trials, the participants were seated with their hips flexed at 85° (0° represents a fully extended hip). The rotational axis of the dynamometer was aligned with the lateral epicondyle of the femur, and the shin pad of the lever arm was placed above the medial malleolus. To ensure stability, straps were tightened around the chest, pelvis, and thighs. The range of motion for testing was set at 20°–90° of knee flexion (0° representing a fully extended knee), while the angular velocity was set at 60°/s. Participants were instructed to hold the dynamometer bars with both hands during testing and received consistent verbal encouragement throughout the test. For each leg, peak torque was obtained for every set and then averaged within that leg. The average peak torque values of the right and left legs were then combined to calculate a bilateral mean value. Relative eccentric knee flexion peak torque (Nm/kg) was calculated by normalizing this bilateral average to body mass.
Statistical analysis
Values are expressed as mean ± SD. Intraclass correlation coefficients (ICCs) (1,1) were calculated to assess reliability. The Shapiro-Wilk test was used to assess normality. Inter–leg differences in eccentric knee flexion peak torque were analyzed using the Wilcoxon signed–rank test. The validity of the BPA of the Nordic Angle application was examined using Pearson's correlation test (rp) for consistency with the relative and absolute eccentric knee flexion peak torque. The magnitude of the correlation was established based on the following criteria: rp = 1, perfect correlation; 1 ≥ rp ≥ 0.9, nearly perfect; 0.9 ≥ rp ≥ 0.7, very large; 0.7 ≥ rp ≥ 0.5, large; 0.5 ≥ rp ≥ 0.3, moderate; 0.3 ≥ rp ≥ 0.1, small; and 0.1 ≤ rp, trivial. 19 All the statistical analyses were performed using SPSS version 29 (IBM Corp., Armonk, NY, USA). The significance level was set at p < 0.05.
Results
Reliability
The ICC was calculated to assess reliability. The ICC values for BPA measured by the Nordic Angle app and for absolute eccentric knee flexion peak torque on the right and left were 0.75 (95% confidence interval [CI]: 0.56–0.88), 0.95 (95% CI: 0.89–0.98), and 0.94 (95% CI: 0.86–0.98), respectively.
Inter–leg differences
The eccentric knee flexion peak torque of the right leg (173.1 ± 40.7 Nm) was significantly higher than that of the left leg (165.2 ± 46.6 Nm) (rp = 0.49, p < 0.05).
Relationship between BPA and absolute eccentric knee flexion peak torque
Figure 2 displays the correlation between the BPA and absolute eccentric knee flexion peak torque. No Pearson correlation was observed between BPA and absolute eccentric knee flexion peak torque (rp = −0.05, p = 0.85).
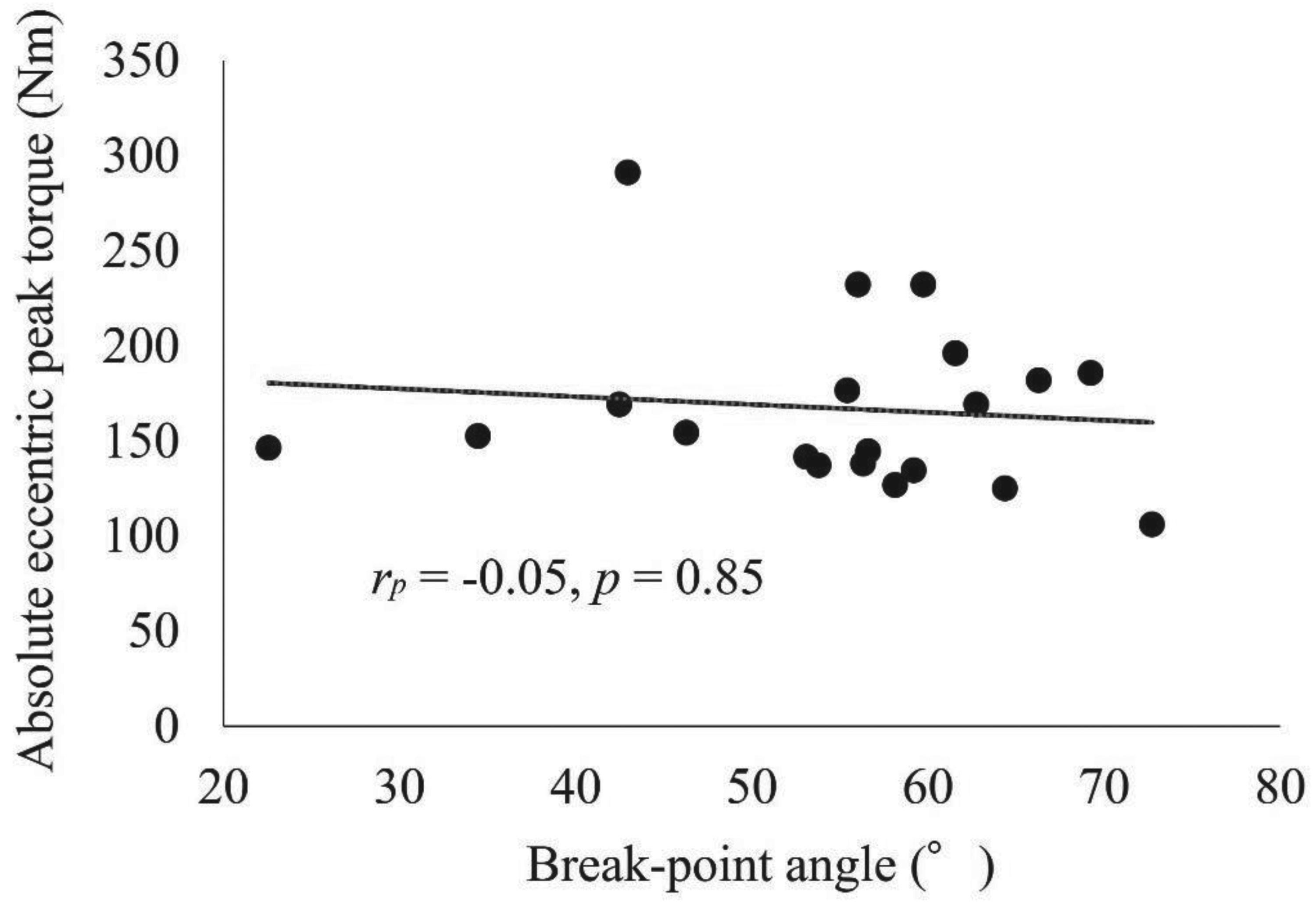
The correlation between the BPA and absolute eccentric knee flexion peak torque.
Relationship between BPA and relative eccentric knee flexion peak torque
Figure 3 demonstrates the correlation between BPA and relative eccentric knee flexion peak torque. The Pearson correlation between BPA and relative eccentric knee flexion peak torque was significant (rp = −0.54, p < 0.05).
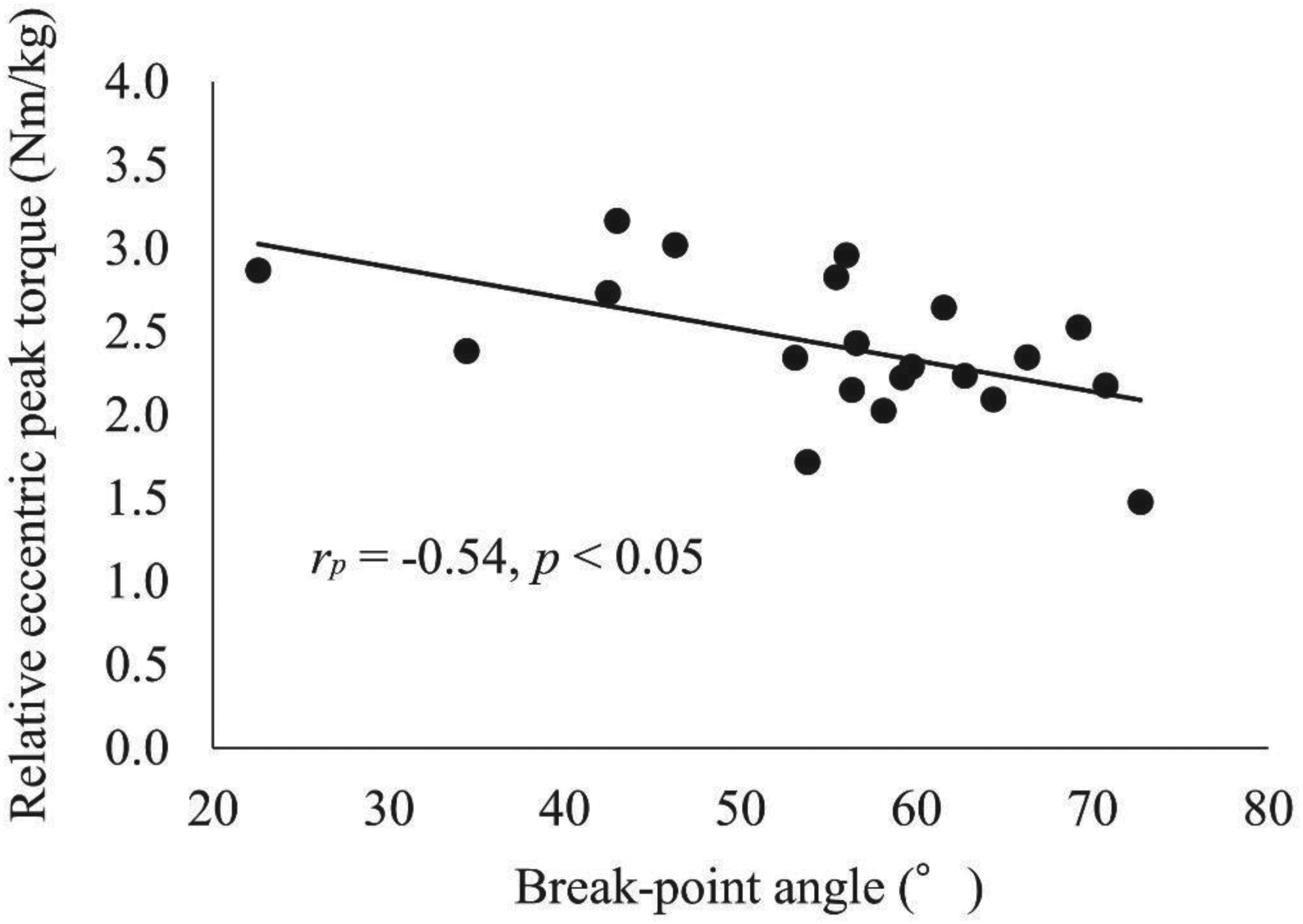
The correlation between the BPA and relative eccentric knee flexion peak torque.
Discussion
This study aimed to investigate the relationship between BPA measured using the Nordic Angle application, as well as absolute and relative eccentric knee flexion peak torques. We demonstrated BPA was significantly correlated to relative rather than absolute eccentric knee flexor peak torque. Therefore, our findings supported our hypotheses. To our knowledge, this is the first study to investigate and demonstrate an association between BPA measured using the Nordic Angle application and relative eccentric knee flexion peak torque.
Previous studies reported moderate to very strong correlations (rp = 0.49–0.88, p < 0.001) between absolute eccentric knee flexion peak torque and BPA.6–8 Specifically, Lee et al. investigated the correlation between absolute eccentric knee flexion peak torque and BPA in 30 elite male soccer players. 7 Using a BPA threshold defined as a knee extension velocity >10°/s, they reported a large positive correlation between absolute eccentric knee flexion peak torque and BPA (R2 = 0.34, rp = 0.58, p < 0.001). Additionally, Lee et al. from the same research group investigated the correlation between absolute eccentric knee flexion peak torque and BPA measured using a smartphone application (SensorLog) in 25 male professional soccer players. 6 Using a BPA threshold defined as a knee extension velocity >10°/s, they reported a very strong positive correlation between absolute eccentric knee flexion peak torque and BPA (R2 = 0.77, rp = 0.88, p < 0.001). Furthermore, Miralles-Iborra et al. investigated the correlation between absolute eccentric knee flexion peak torque and BPA, measured using two–dimensional software, in 46 volunteers (33 men and 13 women). 8 Using a BPA threshold defined as a knee extension velocity >20°/s, they reported a moderate positive correlation between absolute eccentric knee flexion peak torque and BPA (rp = 0.49, p < 0.001). Nevertheless, one study found no correlation between absolute eccentric knee flexion peak torque and BPA. 9 Nishida et al. investigated the correlation between absolute eccentric knee flexion peak torque and BPA, measured with an electrogoniometer, in 16 male university students. 9 Using a BPA threshold defined as knee extension velocity exceeding the average ± 2SD, they reported no meaningful correlation between absolute eccentric knee flexion peak torque and BPA (rp = −0.03, p = 0.92). Here, no correlation was found between absolute eccentric knee flexion peak torque and BPA measured using the Nordic Angle application (Figure 2). Because peak knee flexion force during the NHE may depend on body mass and because the NHE is a multi–joint task involving hip extension and trunk muscle activation, BPA may not purely reflect isolated knee flexor strength. Rather, individuals with higher body mass experience a greater forward gravitational moment during the NHE, requiring proportionally higher relative knee flexor torque to delay forward fall. Therefore, BPA reflects the ability to resist gravitational torque relative to body mass, rather than absolute peak torque production alone. Sex–related biomechanical factors may also influence BPA. Women generally differ from men in body mass distribution, hamstring strength relative to body mass, and trunk–pelvis control during the NHE, all of which can alter the forward gravitational moment and the relative torque required to delay forward fall. Therefore, sex differences may affect the interpretation of BPA. Additionally, the BPA threshold of 30°/s used in the Nordic Angle application16,17 differs from the thresholds reported in previous studies,6–9 which did not include female participants 8 and used different measurement equipment.6–9 Such methodological discrepancies may have influenced the present findings.
As previously discussed, because the maximum knee flexion force during NHE may depend on body weight,12,13 the BPA during NHE may not be particularly meaningful when absolute eccentric knee flexion peak torque is high and body weight is low. Therefore, as hypothesized, BPA was associated only with relative eccentric knee flexor peak torque (rp = −0.54, p < 0.05) (Figure 3), indicating a negative relationship in which individuals with greater relative strength tend to reach a smaller BPA. The negative correlation indicates that individuals with greater relative eccentric knee flexor peak torque tend to reach a smaller BPA, meaning they can resist forward gravitational torque for longer before the onset of forward fall. Thus, a lower BPA reflects higher relative peak torque, resulting in the observed negative association. Lee et al. demonstrated when the relative eccentric knee flexion peak torque was below 2.4 Nm/kg, the risk of hamstring injury increased by 5.6-fold. 11 Although previous studies have not discussed this factor in detail, 11 the incidence of sports injuries may increase with body mass gain. 20 Thus, hamstring injury risk likely increases when absolute eccentric knee flexor peak torque is insufficient relative to body mass. Notably, although this study suggested BPA measured using the Nordic Angle application may provide an estimate of relative eccentric knee flexion peak torque, the coefficient of determination was 29%, which is modest. Nishida et al. examined the correlation between peak force during NHE and one-repetition maximum (1RM) deadlift in 49 rugby players, 21 and reported a significant weak correlation between peak force during NHE and deadlift 1RM (rs = 0.34–0.37, p < 0.05). During NHE, not only knee flexion torque but also hip extension torque is generated. 22 Furthermore, NHE induces trunk muscle activity (erector spine and internal oblique). 23 Because the NHE is a multi–joint task that requires not only knee flexor strength but also hip extension strength and trunk stability, BPA inherently reflects contributions from multiple muscle groups rather than isolated knee flexor capacity. These multi–joint demands constrain the extent to which BPA can represent knee flexor strength alone. Nevertheless, BPA measurements may have the potential to provide a rough indication of relative eccentric knee flexion peak torque magnitude. However, because this study did not assess hamstring injury incidence, BPA should not be interpreted as a predictor of hamstring injury risk. Further studies are required to determine whether regular BPA measurements can predict hamstring injury risk.
This study has two limitations. First, statistical power was slightly low. Although a significant correlation was confirmed between relative eccentric knee flexion peak torque and BPA, statistical power was 0.75. Future studies should use larger sample sizes and include women. 8 Second, unilateral eccentric knee flexor peak torque was assessed using an isokinetic dynamometer, whereas the NHE is a bilateral task. This mismatch in task specificity may have influenced the observed correlations. Unilateral strength testing can elicit greater supraspinal neural drive to a single limb compared with bilateral actions, potentially resulting in higher peak torque values and reducing the specificity of the comparison with bilateral NHE performance. 24 Finally, because this study did not assess hamstring injury incidence, no conclusions can be drawn regarding whether BPA predicts hamstring injuries.
Conclusions
BPA measured using the Nordic Angle application was associated with relative eccentric knee flexor peak torque. However, because this study did not assess hamstring injury incidence, BPA cannot be interpreted as a predictor of hamstring injury risk. Future research is warranted to determine whether BPA can predict hamstring injuries.
Practical applications
Although BPA should not be used to predict hamstring injury risk, it may serve as a practical field–based indicator of relative eccentric knee flexor peak torque. For athletes with BPA values approaching 0°, holding weight plates or medicine balls can increase BPA values, 14 suggesting a simple method to further challenge and potentially enhance relative eccentric knee flexor peak torque. Future studies are needed to determine whether BPA–based training adjustments translate to reduced hamstring injury risk.
Footnotes
Acknowledgments
The authors acknowledge the facilities and assistance provided by the [blinded]. This study was supported by [blinded] (Grant Number: [blinded]).
ORCID iDs
Author contributions
All the authors contributed to the study design. Material preparation, data collection, and analysis were performed by TS, TK, PI, and PR. The first draft of the manuscript was written by TS, and all authors commented on the previous versions. All the authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (grant number: JP25K21055).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available, but can be obtained from the corresponding author who organized the study.