
Abstract
The revision of the Diagnostic and Statistical Manual of Mental Disorders (DSM), scheduled for publication in May 2013 by the American Psychiatric Association (APA), has created a firestorm of controversy because of questions about undue industry influence. Specifically, concerns have been raised about financial conflicts of interest between DSM-5 panel members and the pharmaceutical industry. The authors argue that current approaches to the management of these relationships, particularly transparency of them, are insufficient solutions to the problem of industry’s capture of organized psychiatry. The conceptual framework of institutional corruption is used to understand psychiatry’s dependence on the pharmaceutical industry and to identify the epistemic assumptions that ground the DSM’s biopsychiatric discourse. APA’s rationale for including premenstrual dysphoric disorder in the DSM-5 as a Mood Disorder is reviewed and discussed.
Feminists have critiqued traditional psychiatric taxonomy, codified in the American Psychiatric Association’s (hereinafter APA) Diagnostic and Statistical Manual of Mental Disorders (DSM), for more than four decades (see e.g. Caplan, 1995; Chesler, 1972; Cosgrove and Caplan, 2004; Hare-Mustin and Marecek, 1997; Kaplan, 1983; Stoppard, 1991). Early critiques focused on the problems with psychoanalytic models, the main paradigm until the late 1950s; DSM-I and DSM-II were deeply mired in that framework. The DSM-III marked an explicit shift away from the psychoanalytic framework that dominated previous versions of the DSM and toward a descriptive orientation unrestricted by the dogma of any particular theory. Unfortunately, however, the self-proclaimed atheoretical and biopsychosocial orientation of the DSM-III and DSM-III-R did not generate a more contextual approach to emotional distress. Andreasen (2007), in ‘DSM and the Death of Phenomenology,’ writes about the ways in which the DSM-III and DSM-IV mark a distinct shift in diagnostic thinking: from appreciating the importance of the specific and unique life histories of individuals to documenting symptoms. Indeed, since 1980, the DSM has consistently come under fire from feminist and other critical approaches for its biological reductionism (e.g. Caplan, 1995; Fee, 2000; Hare-Mustin and Marecek, 1992, 1997; Marecek, 1993; Potts et al., 2004; Prilleltensky, 1989, 1997; Tiefer, 2001; Ussher, 1991). Although there have been important and insightful criticisms made about the lack of transparency and rigor of the development process (Caplan, 1995); the poor inter-rater reliability and questionable validity of diagnostic categories (Kirk and Kutchins, 1992); and the failure to see how race, class, age, gender, and other forms of bias undergird many of the diagnoses (Ali, 2004; Becker, 2004; Parker et al., 1995), the criticisms typically remained inside academe, only occasionally spilling over into the public and taken up by the media (see e.g. Chrisler and Caplan, 2002; Kirk and Kutchins, 1992).
However, in the last decade there have been increasing concerns that financial conflicts of interest (FCOI) may be compromising biomedical research, teaching, and practice (including but not limited to psychiatric taxonomy guidelines). With concerns mounting about the APA’s financial ties with the pharmaceutical industry, questions have been raised by patient advocacy groups, investigative journalists, clinicians, and researchers as to whether the proposed changes for the fifth revision are evidence-based; the manual that few ever heard of 59 years ago has generated a firestorm of very public controversy including numerous reviews (e.g. Angell, 2011) and op-ed articles (e.g. Frances, 2010). The controversy has been ignited because of the impact the DSM has on a variety of domains such as jurisprudence, insurance claims, and mental health research and treatment. The appearance, let alone the reality, of industry bias has undermined its integrity and weakened public trust.
In this article, we address industry’s colonization of psychiatry, via the DSM’s profound impact on its practice, by focusing on some of the ethical and practical implications of financial conflicts of interest and why these conflicts are an important issue for feminist psychologists. We report on the financial associations between DSM-5 panel members and the pharmaceutical industry, arguing that simple transparency of financial ties is not only an insufficient solution but also a potentially dangerous one. We also suggest that the problem of undue industry influence on psychiatric taxonomy cannot be resolved by pragmatic policy interventions alone (e.g. mandatory disclosure policies). There must also be an epistemic shift that recognizes the ‘indistinguishability between measurement and description’ (Barad, 2007; Bohr, 1963, 1998; Murdoch, 1987). That is, the medical model of psychiatric illness assumes a scientific neutrality that is impossible to achieve (Prilleltensky, 2002). A paradigm shift – one that recognizes that what we measure for determines what we find – is also needed. We review the changes proposed for the DSM-5 to the diagnostic category of premenstrual dysphoric disorder (PMDD) and show, via this review, that industry relationships re-install the hegemony of the medical model and biopsychiatric discourse.
Financial ties between industry and DSM panel members: Is sunlight really the best disinfectant?
The concern that industry might affect psychiatric taxonomy was heightened when it was discovered that the APA receives substantial drug industry funding and that the most of the individuals who serve as diagnostic panel members also have drug industry ties. In 2006, it was reported that 100% of the individuals on two DSM panels, Schizophrenia and Psychotic Disorders and Mood Disorders, had financial ties (e.g. served on speakers bureaus, corporate boards, or received honoraria) with industry (Cosgrove et al., 2006). The fact that all of the members of these panels had industry ties is problematic because psychopharmacology is the standard treatment in these two categories of disorders.
The APA, to its credit, has instituted a mandatory disclosure policy: All DSM-5 panel members are required to post financial disclosure statements (www.dsm5.org), and the APA has made a commitment to better manage potential FCOI. This new disclosure requirement appeared promising, and one may have expected to see a decrease in the number of individuals serving on the DSM-5 panel who have corporate ties. As can be seen in Table 1 and as reported in the New England Journal of Medicine, despite increased transparency, industry relationships with DSM panel members persist. Of the DSM-5 task force members, who oversee the development of the manual, 69% reported having ties to the pharmaceutical industry (Cosgrove and Krimsky, 2012; Pilecki et al., 2011). This represents an increase of 21% over the proportion of DSM-IV task force members with such ties. Moreover, it is not only task force members who have financial relationships with Big Pharma; 58% of the DSM-5 panel members (the individuals who serve in specialized groups tasked with making the revisions), reported financial relationships – hardly an improvement over the 56% of DSM-IV members who were found to have such industry relationships (Cosgrove et al., 2009). Most of the DSM-5 panels still have the majority of members with industry ties. It is also noteworthy that, as with the DSM-IV, the panels with the highest number of members with FCOIs are those for which pharmacological treatment is the first-line intervention (Figure 1). The type and level of financial relationships also needs to be spelled out more clearly; the APA’s disclosure policy does not require DSM panel members to report their participation on pharmaceutical companies’ advisory boards or speakers bureaus. This is a glaring omission in that it is widely recognized that speakers bureau participation constitutes a significant FCOI and is usually prohibited (e.g. for faculty in medical schools). In fact, pharmaceutical companies refer to these individuals as ‘Key Opinion Leaders’ or ‘KOLs’ because they are seen as essential to the marketing of diseases as well as drugs. In a recent article, Cosgrove and Krimsky (2012) reported that 15% of the DSM-5 panel members disclosed elsewhere that they participated on speakers bureaus and/or scientific advisory boards, indicating that these particular relationships exist with some frequency despite the lack of explicit acknowledgment in the disclosure statements.
Comparison of rates of financial conflicts of interest in DSM-IV and DSM-5 task forces and work groups. Summary of task force members and total panel members with FCOI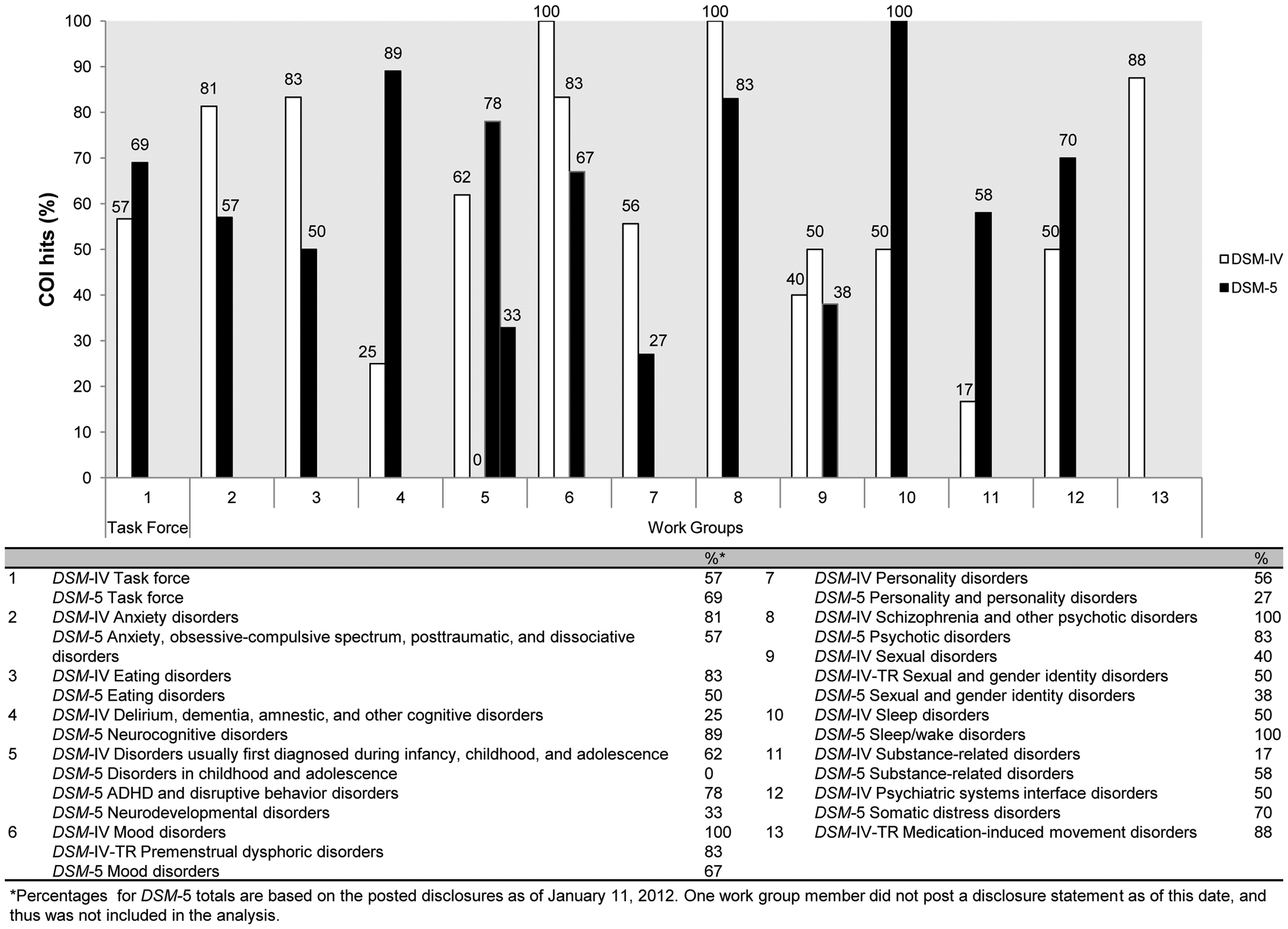

Transparency, implicit bias and institutional corruption
My point is not that everything is bad, but that everything is dangerous.
Although industry–academic relationships can result in unethical behavior that is clearly intentional, FCOI does not always translate into scientific misconduct. Industry financial relationships can also affect researchers’ and clinicians’ behavior in subtle ways that may result in implicit bias. That is, industry relationships may create ‘pro-industry … habits of thought’ (Lexchin and O’Donovan, 2010: 643) that are difficult, if not sometimes impossible, to monitor and regulate.
Bias is a ubiquitous part of the human condition. Decades of research in behavioral ethics and social psychology have shown us that we all have implicit biases (and that we remain blissfully ignorant of them). Psychiatry’s unique position as a medical subspecialty whose conditions do not have biological markers makes it especially vulnerable to industry influence, especially in terms of decisions about the criteria for and measurement of diagnoses. As Quanstrum and Hayward (2010: 1078) note, it is unrealistic to expect the guild of any service industry on its own ‘to harness its self-interest and to act [solely] according to beneficence.’ Transparency alone cannot mitigate implicit or unconscious bias.
Additionally, promoting transparency as the solution to FCOI glosses the ‘deeply normative character’ (Lexchin and O’Donovan, 2010: 646) of disclosure policies and practices. That is, these policies and practices have a constitutive element. They are not simply responses to a problem; they shape what we think of as the problem – as acceptable/unacceptable academic-industry relationships. As Foucault (1983) noted, there are always unintended (and sometimes regressive) consequences of what are assumed to be progressive solutions to problems. For example, disclosure may result in the discounting of unbiased, empirically sound research, or, conversely, it may instill an unjustified belief in whatever the industry-tied expert says (Cain et al., 2005; Licurse et al., 2010).
Thus, disclosure of FCOI is ‘dangerous’ in Foucault’s sense of the term because it has an unintended constitutive/normative aspect. We need to investigate empirically these unintended consequences (e.g. When does transparency undermine critical thinking? What are the conditions under which it animates critical thinking?). We also need to interrogate more fully the normative character of our solutions to FCOI (e.g. How does transparency shape beliefs about acceptable and unacceptable industry-academic relationships?). Additionally, we need to investigate the possibility that disclosure may open the door for subterfuge (Matheson, 2008). That is, when researchers or panel members list every affiliation that they have ever had, including funding from federal agencies, it can create a ‘signal-to-noise problem,’ thereby obscuring the truth about deeply problematic financial relationships with industry, as others have discussed (e.g. The PLoS Medicine Editors, 2012).
It is also important to note that one of the main – but unarticulated – assumptions that grounds transparency as a solution is the assumption of objectivism. Objectivism solidifies our conviction that ‘human reason can completely free itself of bias, prejudice, and tradition’ (Bernstein, 1983: 36). For example, implicit in APA’s new disclosure policy is the belief that disclosure and the restriction on current industry ties can stave off bias because a DSM panel member will then to able to ‘objectively’ use scientific facts (that are independent of the observer/researcher) when making decisions about revising symptom criteria or adding new diagnoses. Organized psychiatry’s belief that adherence to the methods of science protects against bias prevents serious consideration of the possibility that ‘disease mongering,’ or widening the boundaries of diagnostic categories (Moynihan, 2010; Moynihan et al., 2002), is a real problem and one that is exacerbated by industry–academic connections. The epistemic commitment to objectivism undermines the ability to see these financial ties as an institutional, rather than individual, problem. This unbridled belief in objectivism reinforces simple and apolitical solutions (e.g. transparency of individual financial ties to the pharmaceutical industry) to what may be a complex and socio-political problem of institutional corruption. Although there is no one definition of institutional corruption, we find Lessig’s (2009) definition robust and helpful. He differentiates institutional corruption from individual corruption by emphasizing the ‘improper dependence’ that results from the former. Institutional corruption is thus defined as a dependence that results in widespread or systematic practices that undermine the integrity of that institution or weaken public trust. In this way, institutional corruption leads to a set of practices – notably and usually legal ones – that create conflicted organizations and institutions because profit-seeking is privileged over truth-seeking.
The epistemic consequences of commercialized science
We can no longer uphold the idea of a behaviour of objects, independent of the circumstances under which the phenomena are observed.
The partnership between APA and industry occurs within a culture of inevitable – sometimes framed as desirable – commercialism (see e.g. Krimsky, 2003; Lexchin and O’Donovan, 2010). Hence, disclosure and the promise not to have current industry ties are inadequate solutions to the (institutionalized) industry capture of the DSM’s epistemic framework. This is because of psychiatry’s, and in particular the APA’s, dependence on the pharmaceutical industry, a dependence that is not just financial. The absence of biological markers for psychiatric conditions does not simply make psychiatry more vulnerable to industry influence than other medical specialties; psychiatry exists as a medical subspecialty in part because industry has been able to co-opt the lack of biological markers to its own advantage. For example, given the lack of evidence for the serotonin theory of depression, relationships between academic psychiatrists and industry are critical because these relationships sustain a belief in the neurobiological model of depression – a model which would otherwise be untenable. 1 Indeed, psychiatry is unique in its need to have industry legitimize its existence as a medical subspecialty. It is this dependence as well as the systemic nature of the financial ties that make policy-oriented interventions (e.g. disclosure policies) unable to effect meaningful change.
This dependence, and concomitantly, the colonization of psychiatry by industry, marginalizes feminist and other critical approaches to understanding emotional distress. These alternative approaches – ones which take the socio-political context of experience as their starting point – are marginalized because they pose a threat to the ontological status of psychiatric conditions. Hence, feminist challenges to the biological reductionism inherent in psychiatric taxonomy must include a re-conceptualization of the nature/culture and observer/object relationships. It will not be enough to have feminists with expertise in women’s health issues serve on DSM panels or to prohibit participation of individuals with egregious financial ties to pharmaceutical companies (although both of these changes are important). Rather, we need to understand the problem of FCOI as an institutional practice that has epistemic consequences.
Niels Bohr’s philosophy-physics may be helpful in understanding the reductionism inherent in the conceptual framework of the DSM and, by extension, how industry is able to put this reductionism to use. Specifically, Bohr’s insight that there is an ‘epistemological indistinguishability’ between measurement and description (see e.g. Barad, 1997; Bohr, 1963, 1998) is instructive here. According to Bohr, the very act of measuring an object inevitably changes its pre-measurement status; it changes what we can know about that object. That is, following Bohr, the ‘object’ can never be separated from the agencies of observation/apparatus used to measure it. He writes that ‘the essential wholeness of quantum phenomena makes it impossible to speak in any unambiguous way of attributes of the objects independent of the conditions under which they are observed’ (Bohr, 1998: 174, emphasis added). The impossibility of separating measurement and description challenges the epistemological assumption that most empirical research (and certainly research in psychiatric taxonomy) rests on: the assumption that it is possible to reveal the predetermined or objective nature of the entity being measured/observed. The failure to see the connection between measurement and description has profound consequences; to oversimplify a bit, what we measure for (or look for) does indeed determine what we find. Barad (2007: 109) astutely sums up this revolutionary insight of Bohr’s: ‘Concepts are defined by the circumstances required for their measurement’.
Applying this insight to psychiatric disorders means that we should look at the circumstances required for the identification of experience qua mental disorder. For example, as will be discussed in more detail in the next section, the acontextual ‘diagnosis-by-checklist’ (Andreasen, 2007) approach to the DSM and the serotonin theory of depression are two such ‘circumstances’ required for women to be diagnosed with PMDD. Additionally, our biopsychiatric discourse about PMDD functions to legitimize traditional constructions of femininity (Cosgrove and Riddle, 2004; Ussher et al., 2000), which in turn makes it difficult for women to experience negative affect without appealing to pathology (‘I must have PMS/PMDD’) to explain away that affect. Thus, diagnosing women’s experience as PMDD undermines an appreciation for the context of that experience.
Premenstrual dysphoric disorder and the hegemony of a biopsychiatric discourse
Measurement is a potent moment in the construction of scientific knowledge.
Barad (2007: 166)
A powerful example of industry’s capture of organized psychiatry is the medicalization of menstrual distress, reified currently as PMDD, which was first introduced in the appendix of DSM-III as ‘Late Luteal Phase Dysphoric Disorder’ (APA, 1980). The debate about the inclusion of this disorder in the manual has endured throughout the text’s subsequent revisions (see e.g. Cosgrove and Caplan, 2004) and continues with the DSM-5, as PMDD will be incorporated into the text as a mood disorder for the first time. Decades of research have failed to provide clear and consistent empirical support for PMDD as a separate disease entity, and serious methodological problems have been identified in those studies claiming that the etiology is hormonal (Callaghan et al., 2009; Di Giulio and Riessing, 2006; Gallant et al., 1992). The reliability of the diagnosis also has been a source of major criticism since there are no standardized assessments for diagnosis (Caplan, 1995; Wittchen, 2010).
Despite the questions about and challenges to the empirical basis for the validity and reliability of PMDD diagnosis, the hormonal and neurotransmitter model of this disorder has been heavily marketed and used to support treatment with SSRIs. In this way, women are encouraged to overlook the context in which their emotions are manifest and regard upsets as by-products of premenstrual hormonal changes or serotonin deficiencies. As numerous feminists have pointed out, the diagnosis of PMDD not only sustains the stereotype of women as having labile emotions, but also undermines an appreciation for the role that stress, sexual abuse, and violence play in women’s experiences of emotional distress (Caplan et al., 1992; Gallant et al., 1992; Ussher, 2003; Ussher et al., 2000). Traditional expectations of femininity are effectively hidden from view when one’s experience is labeled as PMDD (or PMS) because this label encourages women to understand conflict as an internal rather than an interpersonal phenomenon (Cosgrove and Caplan, 2004). By choosing to move PMDD into the mood disorders category, the DSM-5 mood disorders work group has marginalized the role of relational and other contextual factors in women’s experiences of emotional distress – and played handmaiden to industry.
Indeed, the biomedical orientation of the DSM-5’s mood disorders work group – 67% of whom have financial ties to industry – is evident in their rationale for including PMDD in the DSM. On the APA’s open website (www.dsm5.org), they state that ‘the prevalence statistics clearly indicate that PMDD is a condition that occurs in a minority of women.’ While the DSM-IV rates of 3–8% among American women have been replicated by other epidemiological studies that used the DSM-IV criteria, results still vary depending on the method of symptom measurement (Halbreich et al., 2003).In addition, these rates reflect criteria that have inspired criticism and challenges to their evidence base; these challenges are among the reasons why the disorder was relegated to the Appendix of the DSM-IV. Rather than justifying these criteria in this proposed revision using new evidence, the group uses the possible development of pharmacological interventions as a rationale for PMDD’s inclusion in the DSM: The inclusion of PMDD as a diagnostic category may further facilitate development of treatments that are useful for PMDD and may encourage research into the biology, prevalence, as well as consequences of PMDD … It should also be mentioned that there is already some acceptance for PMDD as an independent category from Federal regulators in that several medications have received an indication for treatment of PMDD. (http://www.dsm5.org)
When the rationale for the validity of a disorder includes what Matheson (2008: 357) astutely calls the drug narrative, or the projection into medical/scientific discourse that ‘the drug typically provides the ‘solution’ to a ‘problem,’’ one must wonder if the cart is driving the horse. Incorporating PMDD into the DSM-5 provides valuable incentives for industry (Green, 2008; Relman and Angell, 2002). As a number of researchers have noted, the classification of diseases—particularly new ones—is increasingly driven by the reported effects of drugs (see e.g. Greene, 2007; Janasoff, 2005; Lakoff, 2005; Matheson, 2008). Moreover, it is important to ask if this disorder would even exist were it not for the ‘diagnosis by checklist’ (Andreasen, 2008) approach of the DSM. Although this approach has some benefits (e.g. the potential for increased reliability of diagnosis), it is also a self-serving tool of industry. In fact, in a recent interview, Robert Spitzer, editor of the DSM-III, noted that this symptom checklist approach was a ‘gold rush’ for drug companies: ‘The pharmaceuticals were delighted’ (Ronson, 2011: 45).
Ironically, earlier additions of the DSM used a psychosocial framework and saw the boundary between mental illness and normalcy as fluid (Wilson, 1993). This psychosocial framework allowed for a contextual approach that emphasized the social nature of emotional distress (as opposed to the intra-individual focus of the disease model adopted by the DSM-III, DSM-IV, and now DSM-5). Additionally, the focus of editions of the DSM prior to DSM-III was on the meaning of a behavior or symptom (Wilson, 1993). As Wilson notes, the stakes were (and still are) high for psychiatry to adopt a disease model because the disease model could secure psychiatry’s reputation as a medical specialty at a time when its professional reputation was in question. This status continues to give psychiatry the aura of being grounded in ‘science.’ However, the cost of shifting to a scientific biopsychosocial model was great; an appreciation for an individual’s unique lived experience was undermined.
Industry has certainly benefitted from psychiatry’s embrace of a pathogenic view of the medical model; PMDD could be marketed as a ‘real’ disease entity that needed to be treated with medication. Moreover, the potential for bias in the work group due to their own conflicts of interest raises additional questions. For example, when the patent for Eli Lilly’s blockbuster drug Prozac was scheduled to expire, thereby drastically reducing the company’s profits, Lilly was able to effectively extend its patent by using the diagnosis of PMDD to justify its application for Sarafem (the formula for which is identical to Prozac) (Caplan, 2004). The repackaging of Prozac as Sarafem was undoubtedly helped by the financial relationships among APA, DSM, industry, and the FDA; the majority of the DSM-IV PMDD panel members had industry ties, and the expert opinion offered to the FDA that PMDD was a ‘real and distinct’ disorder was instrumental in getting Sarafem/Prozac approved. A decade later, despite vigorous feminist critiques regarding the validity and reliability of this psychiatric diagnosis, the industry-facilitated approval of drugs to ‘treat’ PMDD is used to justify its inclusion in the DSM-5.
Not surprisingly, financial support of both the APA and FDA by the drug industry (Green, 2008) has led critics and consumers alike to question whether these financial relationships have opened the door for ‘disease mongering.’ Indeed, the promotion of neurobiological explanation of mood disorders, together with the drug narrative, ‘readily [melds] scientific credibility and commercial imperatives’ (Matheson, 2008: 359). 2 The medicalization and subsequent pathologizing of a part of the menstrual cycle, first as LLPDD and now as PMDD-qua-mood-disorder in the DSM-5, is an example of how scientific truthfulness becomes sacrificed to corporate gain. In our current industry dominated climate, biologized diagnoses like PMDD conceal the social context and unequal power dynamics in which emotional distress is always embedded.
Conclusion
We have argued that industry creates a climate that sustains the ontological status of psychiatry and psychiatric conditions. Therefore, in order to facilitate a climate change and a more responsible practice of science, we must reconfigure ‘the relationship between knower and known, the role of measurement, questions of meaning making and concept use, [and] the conditions for the possibility of objective description’ (Barad, 2007: 31). This reconfiguring means that the problem of FCOI must be understood as an institutional problem that cannot be ‘managed’ via interventions aimed at individuals (e.g. requiring DSM panel members to disclose their industry ties over the last 3 years and to refrain from certain kinds of relationships during their tenure on the DSM). Having fewer members of DSM work groups with industry ties (or even having completely independent panels) will not create a different climate – one in which gender bias and the socio-political grounding of experience are taken as serious challenges to the medicalization of emotional distress.
Psychiatry’s discursive and paradigm shift to a classical medical model of disease opened the door for FCOI to exert an undue influence on psychiatric taxonomy. However, prohibiting industry relationships is a necessary but insufficient solution; the disease model with its reductionism and de-politicized approach also must be challenged. Radical transparency or even a prohibition on industry relationships will not shift the focus off of intra-individual factors to explain the etiology of emotional distress. There must be a concomitant re-conceptualization of psychiatric problems as ‘not truly medical but social, political [emphasis added] and legal’ (Wilson, 1993: 402). Indeed, until this epistemic shift is made, industry will continue to enjoy its colonization of psychiatry.