
Abstract
This paper aims to highlight the potential contribution of the arguments developed in Burman’s Deconstructing Developmental Psychology for exploring the implications of discourses around development for the practice of family therapy with children. Through the analysis of one brief systemic therapy with a stepfamily, formed following the mother’s death, this paper examined how discourses from developmental psychology, including representations of children, father, mother, stepmother and family, are implicated in the construction of the problem and in the positioning of the participants. The diverse ways in which the family members made sense of their difficulties and the positions they assumed were shown to be intimately linked with culturally dominant representations of the biological nuclear family ideal and with representations of parents as responsible for their children’s difficulties. The position of stepmother in particular was shown to be characterised by conflict and ambiguity, reflecting discourses that idealise motherhood and vilify stepmothers. Moreover, the children were found to be positioned as ‘half-members’ at several points in the conversation, whilst at other points they themselves resisted calls to a more equal positioning, particularly when disagreeing with the adults’ talk. Family therapy, as an institutional practice, was shown to be intimately linked with developmental psychology accounts about childhood, family life and parenthood and Deconstructing Developmental Psychology was shown to provide valuable insights in researching family therapy with children. Based on the analysis, it is argued that paying attention to the social, ideological and cultural context in which family therapy takes place opens up novel ways of conceptualising and researching the process of therapy and allows the exploration of taken-for-granted assumptions about childhood, adulthood, parenthood and the family.
Keywords
In this paper, I approach Erica Burman’s book Deconstructing Developmental Psychology from a particular standpoint. This standpoint reflects my involvement in both clinical work and in researching therapy process; it explores the interface between discursive and deconstructive approaches to psychotherapy and the actual practice of therapy. More specifically, I aim to highlight how some of the ideas developed in Deconstructing Developmental Psychology can help investigate the processes implicated in family therapy with children. It is worth noting that, despite family therapy’s commitment to systemic principles, children’s involvement in family therapy is limited in practice (Miller & McLeod, 2001). There is relatively little research on children in family therapy and the majority of studies focus on children’s experience of family therapy through individual or family interviews (Lobatto, 2002; Moore & Seu, 2011; Stith, Rosen, McCollum, Coleman, & Herman, 1996; Strickland-Clark, Campbell, & Dallos, 2000). This study assumes a different perspective and examines how family therapy with children is actually practiced, in line with the trend of language-based, constructionist research of psychotherapy process. Through the discursive analysis of one case of family therapy, I explore how discourses from developmental psychology, including representations of ‘children’, ‘father’, ‘mother’, ‘stepmother’ and ‘nuclear family’, set the context for the positioning of participants in the clinical conversation and for the construction of the problem.
A brief description of discursive research on family therapy is initially presented, with a focus on the notion of subject positioning. This is followed by a discussion of the effects on participants’ positioning of dominant representations of children and development and of gendered discourses about parenting, within the context of developmental psychology.
Discursive approaches to psychotherapy
Over the last decades, social constructionist, narrative and discursive approaches have fuelled important developments in psychotherapy theory, practice and research. Broadly, discursive approaches to therapy focus on the constructive and functional aspects of language-in-use; accordingly, discursive research on psychotherapy often examines the processes of construction of psychological problems and the negotiation of the clients’ subjectivity through the clinical dialogue (e.g. Avdi & Georgaca, 2007, 2009). Psychotherapy talk typically revolves around ‘problems’. Given that talk about problems implies ideas about their cause(s) and about possible (and preferred) solutions (Buttny, 2004), studying problem constructions in therapy also entails examining the clients’ subjectivity, as speakers position themselves and others with regards to the problem and in this way negotiate issues of responsibility, accountability, blame and agency. In family therapy, the construction of the problem and the participants’ positioning is often contested and lies at the center of complex negotiations around clienthood (with questions around what the problem is and who the client is) as well as blame and responsibility.
Subject positions refer to the identities made relevant through specific ways of talking and it is a notion that emphasises the location of the person in discourse and within a moral order (e.g. Avdi & Georgaca, 2009). It is argued that whenever we speak, we assume a specific position and invite the other to take up a particular position; the other can in turn accept, resist, challenge or change this invitation, and through his or her response he or she positions us, and so on (Drewery, 2005). It is important to note that these exchanges are context-dependent and imbued with power, in the sense that in some contexts some participants have more ‘say’ in positioning others, while some positions may be harder to resist. Within the context of psychotherapy, the therapist is typically represented as possessing expertise, authority and knowledge, a position realised through the therapist asking the questions, managing turn-taking, selecting topics for discussion and offering reformulations and interpretations of the clients’ talk. Accordingly, the client is positioned as knowable within the framework of psychotherapy, malleable and deferring towards the therapist’s understanding (Guilfoyle, 2005).
Family therapy is an institutional practice where the ‘family’ is talked into being and where speakers negotiate their positioning with regard to different category memberships. Family therapy conversations often involve issues that are associated with age-related (e.g. adult, child, teenager) and gendered relationship categories (father, mother, wife, husband, son, daughter, etc.). Moreover, family therapy is a complex interactional setting, with multiple participants, who may have diverse – and even competing – agendas, exhibit different levels of engagement in, and consent to, therapy, have different access to the conversational floor and hold different power to make decisions about therapy. Although research on this issue is limited, there is evidence that parents and children often do not agree about the problem the child faces, and that therapists tend to align themselves with the parents’ perspective (Hawley & Weisz, 2003). Moreover, parents often construct their reasons for attending family therapy as relating to problems in the child and, in this way, position the child as the client (O’Reilly, 2013). Furthermore, children’s positioning in family therapy occurs in the context of specific cultural representations surrounding childhood, as well as gendered representations around parenthood and ‘appropriate’ adult–child interactions. In the next sections, I discuss research that highlights some of the ways in which discourses from developmental psychology are implicated in children’s and parents’ positioning and their participation in family therapy.
Representations of children and family therapy
Developmental psychology is a discipline that produces much of the knowledge surrounding children and their needs. A major critique of developmental psychology, cogently developed in Deconstructing Developmental Psychology, is that it promotes a decontextualized and universalising perspective on childhood and development: development is generally represented as a natural process, fuelled by an intrinsic, biologically driven motivation, a uniform and universal process of orderly progression towards competence, maturity and autonomy. Furthermore, childhood is typically represented as a time of dependence, innocence, proximity to nature and to the ‘authentic self’; accordingly children are positioned as dependent, needy and vulnerable, and thus requiring protection and education by appropriate adults (Burman, 2008).
This positioning of children in discourse is arguably reflected in their interactions with adults, where children are typically treated as ‘half members’, i.e. not fully competent members (Shakespeare, 1998). For example, it has been shown that children, and especially young children, are routinely excluded from the main talk in interactions with professionals, such as paediatric consultations (O’Reilly, 2006), and that they are not always able to participate actively in adult-led therapy (Lobatto, 2002). When children are positioned by their parents as the problem in therapy, they tend to align themselves with such accounts and often do not respond to therapists’ invitations to voice their view about them (Lobatto, 2002). There is also evidence that children and adults are not treated equally within family therapy sessions. For example, it is much more likely for parents to talk ‘for’ the child than the reverse, even in situations where the therapist directly addresses the child, and therapists tend to accept such responses (Hutchby & O’Reilly, 2010). Moreover, children’s attempted interruptions are usually ignored by the adults and, if they persist in their attempt to interrupt, children typically receive a negative response (O’Reilly, 2006). When therapists interrupt parents, they tend to either apologize or otherwise orient to the interruption; this is not, however, the case when therapists interrupt a child, in which case the interruption is generally not acknowledged (O’Reilly, 2008). In addition, in family therapy, children are often represented as needing protection from hearing talk about specific issues (notably sex), although this protection may be in itself problematic (O’Reilly & Parker, 2014; Wilson, 1998). These common interactional processes function to position the child as a ‘half member’ in the conversation and to construct the child’s talk as somehow less important than that of adults. This is the case, despite the emphasis on equality of participation as a key value in family therapy.
Parenting, gender and family therapy
As argued by Burman (2008), representations of children are intimately bound with those of other age and status categories, and primarily those of adult, father and mother. Moreover, much of the knowledge-base of developmental psychology concerns those aspects of the child’s environment that are considered to set the context for optimal development. These accounts are deeply gendered, as they reflect – and further promote – assumptions about women’s central role in fostering children’s development. In most instances, a child’s ‘environment’ is equated with ‘the mother’: ‘the primary focal object of developmental psychological interventions (and its associated panoply of practices) has historically been not children, but mothers – or rather “the mother”’ (Burman, 2008, p. 176). In the majority of the developmental psychology literature, mothers are positioned as the main object and source of child’s affections, as both the originators and monitors of their child’s development, and as ultimately responsible for it. Assumptions about the characteristics of the optimal environment change with time and place, and are shaped by – and in turn have significant implications for – women’s employment and position in the family (Burman, 2008). At the same time, the social construction of motherhood is concealed and motherhood is represented as a woman’s ultimate natural fulfilment; maternal love is described as natural, as reflected in the absorption of a woman’s identity into that of mother (Phoenix, 1991). Moreover, modern motherhood is associated with dependence on professional experts for advice, rather than relying on oral sources of knowledge, which are generally devalued and represented as uninformed or old fashioned (Marshall, 1991).
In contemporary developmental psychology literature, fatherhood is far less studied and regulated than motherhood. Pre-modern family narratives position the father as spiritual guide, advisor, guardian and disciplinarian. A divided model of fathering has been recently described, in which fathers are either accorded mothering qualities, a representation intertwined with the image of vulnerable masculinity, or are pathologized as violent or abusive (Burman, 2008).
Within discourses about child development, any deviation from the expected developmental course is framed in terms of inferiority or abnormality, and parents are generally held responsible for it (Avdi, Griffin, & Brough, 2000; Urwin, 1985). The culturally prevalent view is that children’s difficulties reflect some form of parental failure or fault, whilst the social and material context of children’s life, as well as that of their families, is often sidestepped (Billington, 1996). In line with this, there is some evidence that parents who attend family therapy attempt to accomplish a delicate balance between convincing experts of the reality of the problem, in order to legitimize access to services, whilst at the same time refuting any possible accusations of blame for the child’s problems (Avdi, 2005).
In sum, family therapy can be approached as an institutional practice, which both relies upon and informs developmental psychology accounts about family life, parenting and childhood. In family therapy, children are generally positioned as half-members whilst parents are typically positioned as potentially responsible for the problem, which is seen to be located within the child. This study examines therapy process in a naturalistic setting and uses discursive analysis to study how family therapy with children takes place in clinical practice, with a focus on how the children are involved in the conversation. This is considered useful both for better understanding family therapy process, which in itself can contribute to therapist reflexivity, and for exploring taken for granted assumptions about childhood, adulthood, parenthood and the family.
The family
The material for this study consisted of video-recordings and verbatim transcripts of a brief family therapy, conducted at a training institute in systemic therapy in Greece,1 which offers specialised family and couple therapy services, free of charge. The researcher requested access to videotapes of one completed family therapy for the purposes of this study. The therapy was selected by members of the training institute and the criteria for selection were, firstly, that at least one child should have participated in the therapy and, secondly, that all participants gave their consent for access to the material.
The family attended four sessions, at fortnightly intervals, following referral by a community mental health centre, which the female partner had approached. All sessions were videotaped, in line with the institute’s usual practice, and the videos were transcribed verbatim. Two female mental health professionals training in family therapy were the primary therapists and live supervision was offered through telephone contact and a one-way mirror by a team, which consisted of a senior family therapist and trainees in family therapy.
The family consists of Costas, his two sons: Andreas aged nine and Petros aged 14 and his partner, Katia. Costas’s wife, Vera, died of cancer approximately 18 months prior to the start of therapy, following a protracted period of illness. Costas and Katia attended the first and fourth sessions alone; the children participated in the second and third sessions, following the therapists’ invitation. Before turning to the analysis per se, an outline of the main issues discussed in the sessions is briefly presented. In the first session, the discussion focused on the couple’s struggle to define and manage their ‘new family’, a process described as complicated by the children’s grief and by tensions with Costas’s in-laws who did not approve of their relationship. Also, Costas talked about his struggles with ‘finding himself’, following his wife’s death. In the second and third sessions, the main issues concerned the children’s and Costas’s experience of loss and mourning, as well as each member’s place in their new life together. Strong emotions were expressed and delicate issues, concerning loss, betrayal, family ties and loyalty, were explored. In the last session, the couple’s thoughts and hopes about their shared future were discussed. Through the sessions, the family’s difficulties were reconstructed in terms of transition to a new family setting and the problems they experienced were reformulated in terms of mourning, adaptation in the face of loss and a move towards a new life. In narrative terms, a shift was observed from a narrative of lack (a ‘problem family’) to a narrative of resilience and transition.
Analysis
The sessions were examined using discourse analysis (Georgaca & Avdi, 2011) with a focus on the implications of developmental psychology discourses for the construction of the problem and for the participants’ positioning. The analysis presented focuses primarily on the family member’s constructions of their difficulties rather than on the processes of reformulation of these constructions through therapy. As with other discourse analytic studies, all sessions were examined in detail for the analysis but only brief extracts are used to illustrate the main arguments.
As already mentioned, the main issues discussed in the therapy centred on mourning and on the family’s transition to a stepfamily status. It is proposed that these highly personal and emotive issues take place in the backdrop of normative assumptions about the nuclear family, stepfamilies, parenthood and childhood, and the ‘problem talk’ could be understood in terms of negotiating the moral order of this family (Kurri & Wahlström, 2005), as discussed below.
Problem formulations and the conflicts around stepfamilies


Katia further develops the perspective of a non-normative family that needs professional help, as she describes Costas and the children as in need of psychological support and professional involvement. In underlining the importance of psychological support, she positions Costas and the children as emotionally vulnerable, whilst she assumes a maternal position of carer and nurturer, interested in and engaged with the family’s emotional needs. The shift in the verbs Katia uses to describe her role in initiating the referral (I encouraged, I suggested, I persuaded) is also interesting, as these denote a gradual increase in control and engagement, which may be seen to reflect her shifting position with regard to her place and role in the family. Research on stepfamilies has shown that a key issue relates to the negotiation of the stepparent’s place and role in family and this seems to be more ambiguous for stepmothers than stepfathers (Weaver & Coleman, 2005).

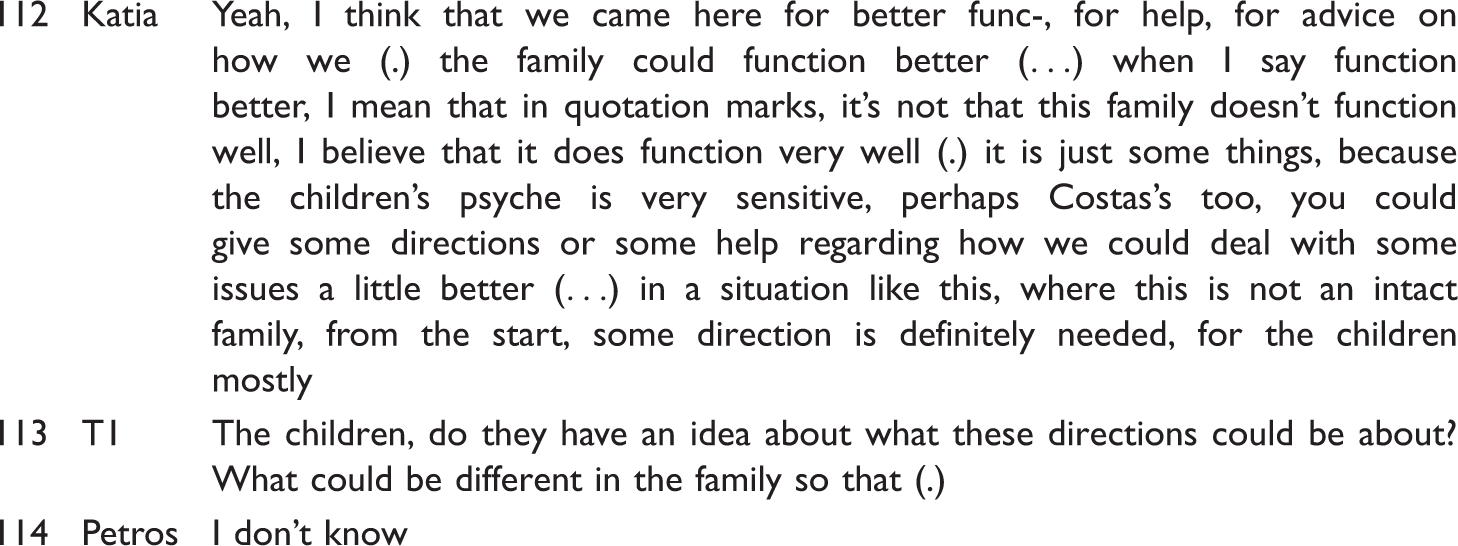
In the extract above, the problem is represented as associated primarily with the children’s vulnerability and sensitivity; Katia describes their family as ‘not intact’, a term with associations of damage and lack. She is careful to assert that this is a vulnerable and needy rather than a dysfunctional family. The therapist subtly subverts the description of children as vulnerable, by asking them about the directions they would consider relevant, and thus positions them as knowledgeable concerning their family’s needs and resourceful; the children, however, do not accept this position call.
Based on the above, in the couple’s initial formulations, the problem is primarily constructed in terms of the status of a new (step-)family, which is non-intact and lacking, presumably in comparison to the norm of the biological nuclear family. Within developmental psychology ‘the family’ is represented as universal, common and unchanging structure, despite the great diversity in family organisation. The nuclear family, prototypically consisting of a heterosexual couple and their genetic children, is represented as the optimal model of family organisation and the optimal environment for children’s development (Burman, 2008). It has been argued that the ideal of the nuclear family persists, despite significant changes in household constitutions over the last few decades. This might be more so in Greece, where household constitution is generally more traditional than in northern European countries. Greece has the lowest rate of live births outside marriage in Europe and a comparatively low divorce rate (European Commission, 2013), whilst ties with the extended family are prominent and valued. The power of the nuclear family ideal is arguably felt most acutely by those who fail to conform to its requirements; there is evidence that stepfamilies are represented as deviating from the ideal of the biological nuclear family, a deviation that often functions as the basis for stigmatisation (Gosselin & Rousseau, 2012; Roper & Capdevila, 2010).
Constructing the problem and managing blame

In the extract above, Costas defines the problem as relating to his temper; both children interrupt the therapist’s next turn, Petros interjects and links Costas’s temper with their mother’s death, thus locating the problem in the context of loss. Moreover, in the children’s narrative, their mother is described as the one who used ‘to shout about details’ (e.g. tidying the house), a description which is in line with the traditional gendered division of labour in the family. This account functions as a justification for Costas’s temper, which is rendered justifiable in the context of the loss of the ‘most important person in his life’; the extreme case formulation used functions to increase the plausibility of the account. Costas interrupts and ‘corrects’ him by asserting that the boys themselves are the most important people in his life, thus producing a version that reinforces his identity as a committed and loyal father.
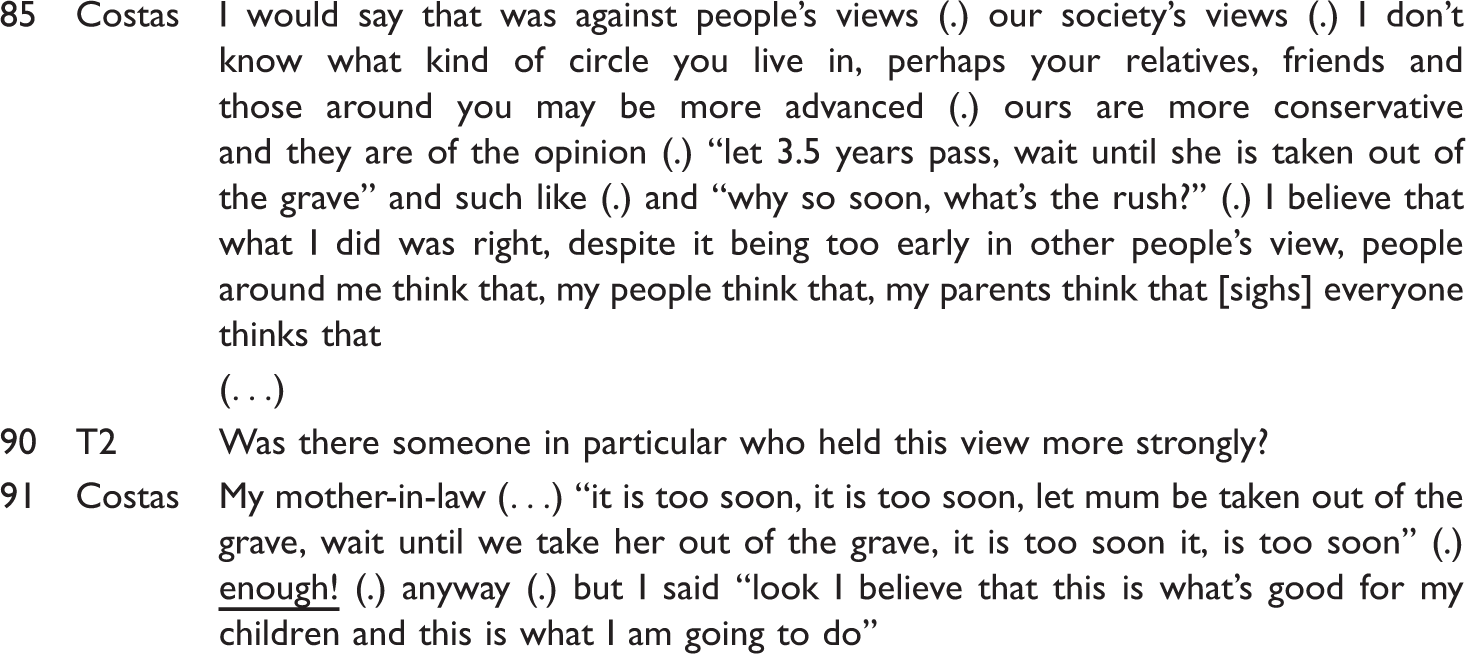
Next (turn 74), Petros expands this formulation to account for Costas’s ‘irrational’ and ‘irresponsible’ reactions following their mother’s death. In Petros’s account, Costas’s ‘bad parenting’ in the past is justified as he is represented as having ‘lost it’, and therefore not fully responsible for his actions, as he was overwhelmed by powerful emotions. Emotions are generally assumed to be involuntary experiences, closely associated to one’s ‘authentic self’ (Godwin, 2004) and so accounts based on emotions have privileged explanatory power. Attributing one’s actions to strong emotions functions to disclaim one’s agency, refute blame and maintain a positive identity. This sequence of blame management can be understood both in its situated context (that is as a response to the extended family’s disapproval of Costas’s parenting) and within the broader cultural context of parental culpability. Furthermore, there are gendered aspects in these constructions, which highlight important differences in the ways in which paternal and maternal roles are represented. More specifically, Costas is excused from not adequately attending to parenting while Vera was alive, because that is accepted as woman’s work; there are several references in the sessions where Costas is reported to have been absent from family life prior to Vera’s illness, due to his work commitments. He is excused from being absent from the family during his wife’s illness, as he is supporting her and is thus represented as a loyal spouse. Finally, he is excused for poor parenting following Vera’s death because he is in mourning. Meanwhile, Katia takes on the caring role, both in terms of household chores and in terms of attending to the family’s emotional needs, but this is apparently seen by the extended family as problematic, as discussed in the next section.
Constructing step-mothering

In Costas’s description, Katia is in an impossible position: she is always compared to the children’s mother, a comparison she can neither avoid nor win. Moreover, on several occasions in the sessions Katia states her priorities and describes herself as someone who puts others’ needs before and above her own. This description is in line with dominant narratives of idealised motherhood, in which mother is constructed as biologically geared to be selfless, nurturing and subsuming her own needs to attend to her children’s (Craig & O’Dell, 2010). It is as if Katia needs to assert her position as caring, selfless and good, despite being a stepmother. Although the research on the experiences of stepparents is limited, parenting children is reported as more difficult by stepmothers than stepfathers; this finding has been interpreted as reflecting a pervasive cultural intolerance of there being more than one ‘type’ of mother (Gosselin & Rousseau, 2012). Furthermore, in stepmother families, increased ambiguity has been reported regarding family boundaries (i.e. who belongs in a family) as well as regarding role definition (Weaver & Coleman, 2005). These issues are arguably particularly complex in this family, as issues of loyalty and betrayal are intensified because of the biological mother’s death and the extended family’s disapproval. In other words, this family’s efforts to establish itself in the context of mourning, are arguably further complicated by the idealisation of motherhood and the cultural prejudice against stepmothers.
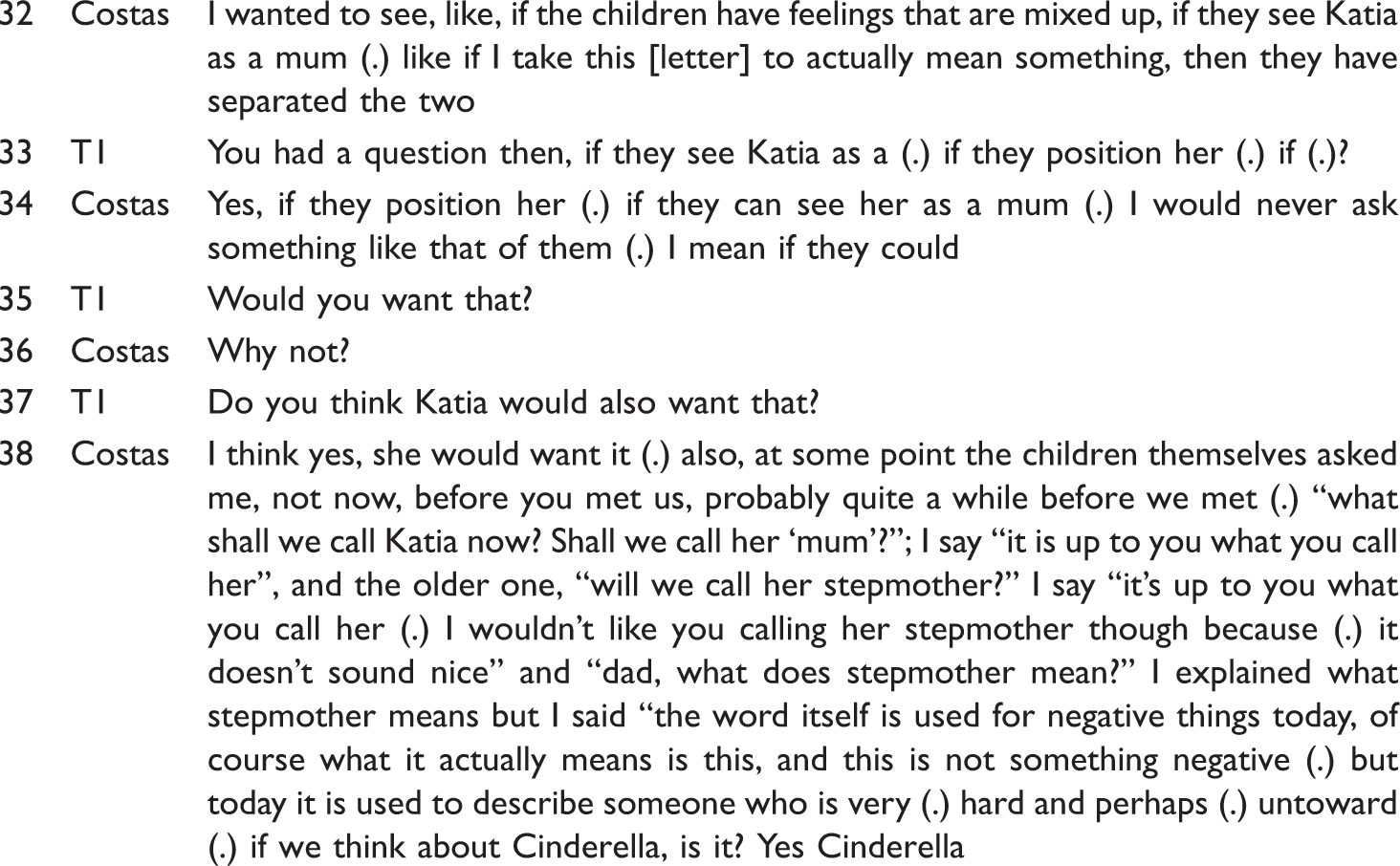
It has been argued that the position of stepmother is intimately implicated with the wicked stepmother myth, a dominant cultural narrative, which is invoked in the above extract through reference to Cinderella. In our collective cultural narratives, stepmothers are cruel, jealous and murderous, in sharp contrast to idealised mothers. Such representations stigmatise stepfamilies and marginalise stepmothers in particular (Roper & Capdevila, 2010).
Children’s participation around delicate issues
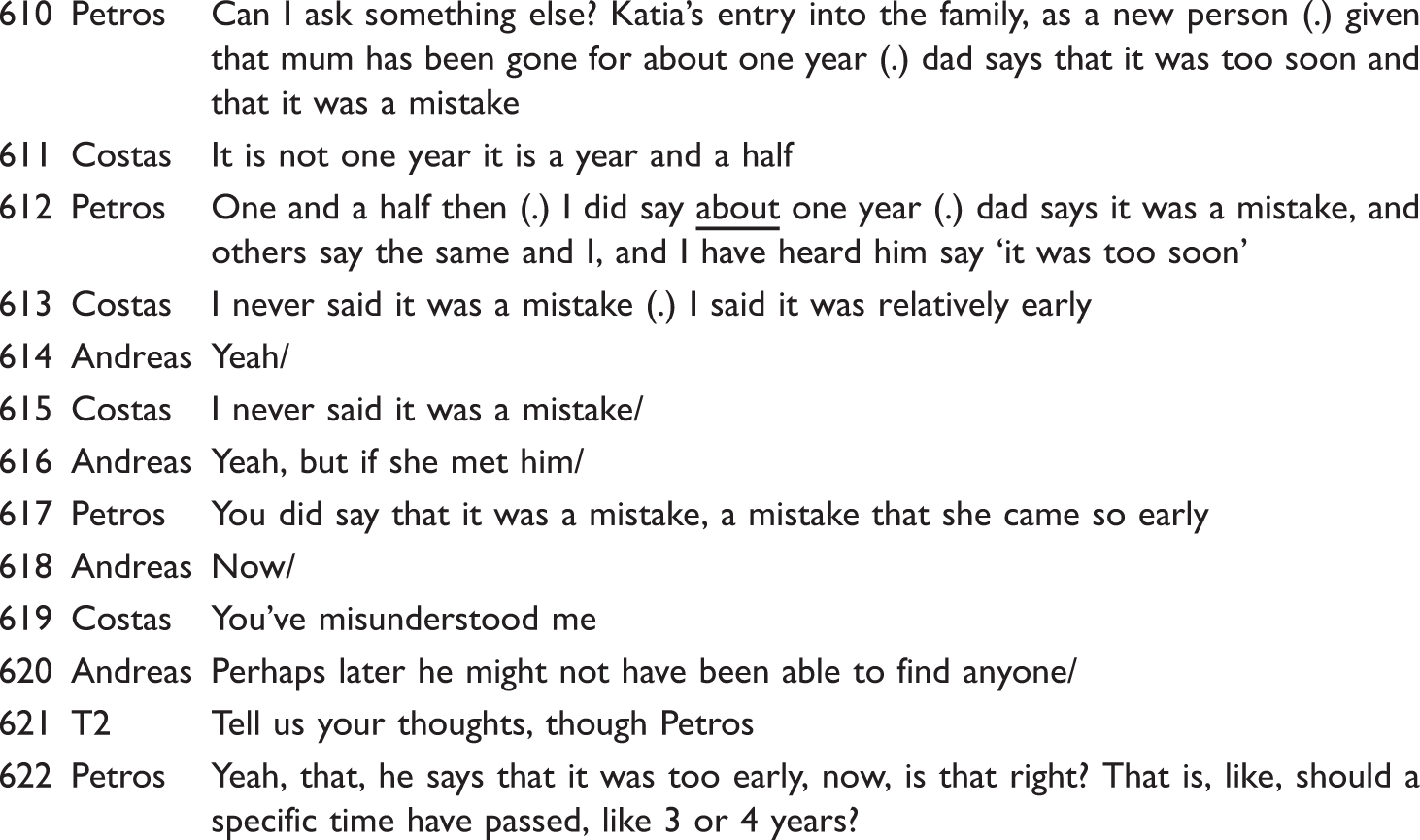
As is evident in the extract above, this is a delicate issue; it is one of the few cases where Costas interrupts either of the children’s talk and persists in correcting what he frames as Petros’s misunderstanding, which reduces the validity of his account and positions Petros as limited in conversational competence. The therapist does not answer Petros’s question, but rather states that the same issue may be seen differently by each person and marks it as important.


The interaction described above illustrates some of the tensions and difficulties surrounding the establishment of this stepfamily and, at the same time, shows some of the tensions involved in children’s participation in family therapy. As already mentioned, equality of participation is an important systemic principle; in this therapy, children were found to have been addressed on a more equal footing than that reported in other studies (e.g. O’Reilly, 2006, 2008). This positioning, however, was sometimes resisted by the children, as in the sequence described above, in which they were in a situation of disagreeing with adults around a very sensitive topic. In family therapy, there is often a tension between speaking and not speaking, especially about issues that may feel too unsafe or too potentially disturbing for others (Rober, 2002). Parental loss and the creation of a new family following such a loss can be seen as a topic which evokes such tensions. Moreover, Petros’s statement is delicate as he challenges a fundamental assumption in representations of the family, that is that a family and children necessarily need mothers.
Discussion
The analysis presented highlighted the potential contribution of the arguments developed in Burman’s Deconstructing Developmental Psychology for examining the implications of discourses around development in the construction of one family’s difficulties and, more broadly, for the practice of family therapy with children. Based on the analysis, it was argued that one of the main issues this family faced was associated with their status as a stepfamily, formed following the death of the children’s mother. The diverse ways in which the family members made sense of their difficulties and the positions they assumed were shown to be intimately linked with culturally dominant representations of the biological nuclear family ideal. Related to this, the female partner’s position as stepmother was shown to be characterised by tensions and ambiguity and discussions around her place in the family were seen to be delicate. Again, the cultural representations that idealise motherhood and demonise stepmothers were shown to be implicated in her positioning as stepmother, in the context of their lived situation, which involves experiences of maternal and partner loss, the need to support the children in their grief and to deal with the extended family’s disapproval. A further issue explored focused on the tensions involved with regard to children’s participation in family therapy, in the context of the principle of equal participation. Children were found to be positioned as less than full members at some points in the conversation, whilst at other points they themselves resisted calls to a more equal positioning, particularly when disagreeing with the adults’ talk. This is an interesting issue both from a clinical and a theoretical perspective, as it illustrates the complex dynamics of positioning in family life, as well as the tensions involved in promoting the participation of children in family therapy.
Drawing upon the above, family therapy was studied as an institutional practice, which is intimately linked with developmental psychology accounts about childhood, family life and parenthood. Deconstructing Developmental Psychology was found to provide valuable insights in conceptualising how discourses around development, the family, gender and the positioning of adults and children set the context for the way in which problems are constructed and reconstructed within family therapy and for the participants’ positioning in the interaction. It is argued that paying attention to the social, ideological and cultural context in which family therapy takes place both opens up new ways of conceptualising and researching the process of therapy, in ways that promote clinician reflexivity, and allows the exploration of taken-for-granted assumptions about childhood, adulthood, parenthood and the family.
Footnotes
Notes
Acknowledgement
I would like to thank participants as well as the staff at the Institute of Systemic Thought and Psychotherapy for providing access to the material.