
Abstract
This paper explores the experiences of young LGBTQ+ people with mental health services in Finland. Drawing on collaboratively created focus group data, we apply minority stress theory and an intersectional lens to shed light on how LGBTQ+ young people's subjective and collective experiences with mental health services are shaped by various interlocking systems of oppression, including cisheteronormativity, ableism and racism. We analysed the data using reflexive thematic analysis, identifying four themes: expectations, experiences, outcomes and demands. Together, these themes illustrate how shortcomings in mental health services feed into minority stress, often resulting in inadequate mental healthcare for LGBTQ+ young people. However, our analysis also illuminates the agentic stance that participants adopted in demanding improvements to existing mental health provision. We conclude by emphasising the importance of developing intersectional sensitivity and increased awareness of the specific needs of sexual and gender minority young people, and the challenges they face when seeking help for mental distress.
Keywords
Although the heightened risk of LGBTQ+ young people encountering mental health challenges has been demonstrated in various studies (Rees et al., 2021), relatively few have qualitatively explored their experiences with mental health services (MHS). Furthermore, while minority stress theory (Meyer, 2003) is widely used as a framework for making sense of the nature and depth of LGBTQ+ young people's mental distress, its application is not always accompanied by theoretical engagement with underlying macro-level systems of oppression. This reflects the relative lack of engagement in queer psychology with decolonial and intersectional perspectives, as seen in extant studies’ continued emphasis on data and narratives about Western, White, cisgender, LGB, middle- or upper to middle-class, highly educated, nondisabled people (Freeman-Coppadge & Langroudi, 2021).
In this article, we build on and contribute to recent efforts in critical psychology (e.g., Ferguson, 2021; Metzger et al., 2023) to understand the interlinkages between experiences of mental distress and discrimination in MHS among minoritised people, and structural inequalities shaped by the sociopolitical context. We complement minority stress theory with insights from intersectional theorisation to analyse LGBTQ+ young people's experiences with MHS, aiming to shed light on current challenges and discriminatory patterns in MHS provision, as well as opportunities to develop such services to better cater to the needs of minoritised young people.
Experiences of LGBTQ+ Young People With MHS, Minority Stress and Intersectionality
As mentioned above, qualitative research on the experiences of LGBTQ+ young people with MHS is fairly sparse, reflecting a wider gap in studies on LGBTQ+ young people's own views and experiences (Metzger et al., 2023). In a study focusing specifically on LGBTQ+ young people and MHS in the UK, McDermott et al. (2024) showed that they often refrain from using MHS due to poor previous experiences, including a lack of understanding of intersectionality in LGBTQ+ lives. A review of qualitative studies by Rees et al. (2021; not focused solely on young people), conducted to identify mental health needs in LGBTQ+ communities and their experiences of accessing mental healthcare, corroborated these findings. The review showed that LGBTQ+ clients had not only been pathologised and undertreated for their primary mental health problems, resulting in experiences of helplessness and vulnerability, but they also felt that practitioners imposed their knowledge during these encounters. Quantitative and mixed methods studies with adults (e.g., McCann & Sharek, 2014) and youth (Fraser et al., 2022) have supported these findings by showing that LGBTQ+ people highlight practitioners’ lack of knowledge, and thus the need for increased education across varied geographical locations.
Our study makes a valuable contribution to this underresearched field by shedding light on LGBTQ+ young people's experiences with MHS through qualitative, collaboratively produced focus group discussions, which provided in-depth knowledge of the lived inequalities that shape LGBTQ+ young people's MHS encounters. Theoretically, our work has been guided, firstly, by the conceptualisation of cisheteronormativity. Stemming from queer theory, cisheteronormativity enables an understanding of how bodies become intelligible only in relation to a set of norms that favour an idealised White, cisheterosexual, middle-class, young, able and successful body (Riggs & Treharne, 2017). Secondly, we draw on minority stress theory, a widely used conceptual framework designed to explain mental health differences between LGBTQ+ and heterosexual people, later extended to understanding differences between transgender and cisgender people (Meyer, 2003; Velez et al., 2021). Minority stress theory operates on two foundational principles: it acknowledges that prejudice and stigma targeted at LGBTQ+ individuals create distinct stressors, and recognises that these stressors contribute to negative health consequences, encompassing both mental and physical distress (Frost et al., 2015). Therefore, the minority stress model elucidates how environmental factors, particularly those linked to stigma and prejudice, can generate stressors that persist throughout the lives of LGBTQ+ individuals and thus contribute to the higher prevalence of mental health issues among LGBTQ+ individuals compared to heterosexual and cisgender people (Meyer, 2015; Velez et al., 2021).
Meyer (2003) outlined four processes of minority stress: (a) experiences of discrimination, including differential treatment, derogation, harassment or victimisation based on one's sexual or gender minority identity; (b) anticipation of rejection, where individuals expect to encounter discrimination, leading to heightened vigilance; (c) internalised heterosexism or transphobia, referring to the acceptance of negative attitudes or beliefs about LGBTQ+ identities; and (d) identity concealment, which involves the stress associated with deciding whether to reveal one's sexual or gender identity. Integral to the minority stress model is the idea that these processes shape each other cyclically. Therefore, the theory illuminates how cumulative negative experiences with mental health and other services can have increasingly dire consequences, including deepened mental distress and potentially a pattern of refraining from help-seeking.
While the minority stress model is crucial for understanding the specific stressors faced by gender- and sexuality-minoritised people, it must be complemented with an intersectional lens to fully grasp their life experiences and to more robustly consider the structural determinants of discrimination experiences, including within mental health counselling contexts (McDermott et al., 2024; Moradi & Grzanka, 2017; Tan et al., 2020). Intersectional theorisation originates from Black feminists’ efforts to understand the particularities of Black women's experiences in the United States (US) at the intersections of racism and sexism (e.g., Crenshaw, 1989). It has since expanded into a variety of applications, with different emphases in different geographical locations. Intersectionality is a theoretical framework, perspective and praxis that shifts the focus away from ‘single axis’ thinking (such as attending exclusively to race, gender or sexuality) towards a ‘matrix’ perspective that underscores the inseparability of systems of oppression and privilege – such as cisheterosexism, racism and capitalism – in shaping people's possibilities in life (Collins, 2019).
As intersectionality is increasingly applied to an ever-expanding array of intersections and in studies with broadly varied background assumptions, concerns have been raised that such applications may erase its rootedness in Black women's experiences. Bilge (2020), for instance, has emphasised the importance of ensuring that intersectionality travels ‘with Black women’, and has contended that ‘a racialized habitus is not an optional but a constitutive component of intersectionality’ (2020, p. 2310). Others, such as Jennifer Nash (2019), have emphasised the benefits of intersectionality's expanding usage, suggesting that it should ‘move with figures beyond “Black woman”’ (2019, p. 104). Regardless of differences in viewpoints, there is broad agreement on the risks of erasing the experiences and viewpoints of Black women as the basis for intersectional theorisation. Therefore, as White, highly educated researchers residing in a Western European country, we find it important to reflect on how to draw on intersectionality in a responsible manner that seeks to avoid its negligent appropriation and distortion (Moradi & Grzanka, 2017). In this article, using data from focus groups with LGBTQ+ young people, we foreground cisheteronormativity while paying somewhat less attention to other systems of oppression such as racism. However, our analysis shows that cisheteronormativity does not shape our participants’ experiences in isolation from other systems of oppression, but rather co-operates with them in creating a sense of otherness and exclusion. Furthermore, the analysis shows that intersectionality served as an important tool for participants to make sense of their experiences of discrimination and of services’ lack of attentiveness to structural inequalities and lived differences.
Patricia Hill Collin's (2019) intersectional theorisation on the interlinkages between experience, knowledge and social action holds particular significance for us, also regarding the epistemological and ontological assumptions that drive our inquiry. Collins (2019) has foregrounded the importance of both experience and social action for critical theorising and, by extension, for epistemology. As she states, since ‘experiences occur in the social world, they are windows to that world’ (2019, p. 13). Oppositional knowledge based on experiences of oppression is central in Collins's thought for achieving social change. For us, these notions form an important basis for attending to minoritised young people's own understandings of MHS and the best ways to make them more inclusive. More specifically, they help us consider how young people's resistant knowledge can disrupt patterns of minoritisation in MHS and the knowledge practices of practitioners. Accordingly, our analysis seeks to answer these research questions: 1. How do LGBTQ+ young people make sense of their experiences with MHS? 2. What kind of patterns of exclusion do they identify? 3. How do they envision inclusivity in these services?
Materials and Methods
Context
Our data originate from Finland, where the current right-wing government's stance raises concerns regarding the rights of LGBTQ+ people and other minoritised groups. At present, these concerns coincide with the so-called youth mental health crisis due to increased mental distress symptoms among young people (Kurki & Rask, 2025). The particularly vulnerable position of LGBTQ+ young people has rarely been considered in public discourse despite surveys consistently reporting that the average well-being level of LGBTQ+ young people in Finland is lower than that of heterosexual and cisgender young people, including fewer experiences of social inclusion and perceived opportunities to seek help for well-being issues (Lehtonen et al., 2024). The well-being of LGBTQ+ children and young people has, however, entered public discourse in the context of debate surrounding the recent Act on Legal Recognition of Gender, which entered into force on April 3, 2023. While the Act enhanced the realisation of trans rights by removing medical examinations, diagnoses or infertility from the eligibility criteria for legal gender recognition, it does not extend to people under 18 (Ministry of Social Affairs and Health, 2023). The exclusion of children from the Act has been widely criticised by medical and welfare institutions, experts and LGBTQ+ rights advocates.
Data Collection and Participants
Our study is part of a larger project focused on inclusion and equity in low-threshold MHS targeting young people in Finland, which received ethical approval from the University of Helsinki. Our project group consisted of both junior and senior researchers, with the former working from insider positions based on their identification with our target group, LGBTQ+ young people. As a diverse group, we worked across perspectives and differences in power (Collins, 2019, p. 144), with a goal to promote mutual learning and to foreground the junior researchers’ insider knowledge in our knowledge generation process. We collaboratively designed our data collection approach, drawing partial yet meaningful inspiration from methodological literature on participatory approaches. These approaches emphasise the inclusion of marginalised groups in research concerning them, and aim to conduct research in a less hierarchical and more responsible and collaborative manner (Fine et al., 2021; Kulmala et al., 2024). While our ability to draw on such principles in the context of the larger project was limited, we made a specific effort to work beyond traditional power relations. To this end, we developed a tailored version of peer-led focus groups, carefully designed to foster a sense of safety and peerhood. Peer-led means here that the facilitators and participants shared identification as LGBTQ+ young people, and that to disrupt the emergence of a hierarchy between researcher and participants, the facilitator would equally contribute to the discussion as one of the participants while being careful not to take the lead but rather to allow the discussion flow organically.
This article draws on data from two focus groups, with eight participants aged 19–29: four in one group (FG1) and three in the other (FG2) plus the facilitator, considered here as a researcher-participant. The focus groups were held in the autumn of 2023, and participants were recruited through university channels, social media and personal networks. The invitation was extended to young (under 30) current or former students at the University of Helsinki who identified as queer. Although everyone related to the word ‘queer’ in some way and responded to the invitation using that term, not all identified with it. Following Fine et al. (2021), we asked participants to self-identify anonymously using one or more words. This was the only background information we collected, as we wished to highlight the identities that the young people themselves considered important in this context. As a result, each participant used between one and five of the following words: queer (five), woman (four), nonbinary (three), trans (two), lesbian (two), transmasculine (one), polyamorous (one), 19-year-old Finn (one), pansexual (one), homo (one) and activist (one). In addition, several participants brought up personal experiences of racism during the focus group discussions, which we discuss in the Analysis section. Considering the diversity of identifications, we use the blanket term LGBTQ+ when referring to participants in this paper.
The focus groups began with a discussion about safer space policies, accompanied by the standard procedures for providing information about the study and obtaining signed consent. The focus groups loosely followed a predefined set of questions, but the participants had the freedom to steer the conversation to topics they deemed important – and this is what they did. The questions focused on participants’ knowledge of mental health, the accessibility of MHS and their views on improving these services. Participants were also asked for their thoughts on a specific intervention targeting university students, although these parts of the discussion largely fall outside the scope of our analysis. Moreover, one of the prompt questions invited participants to consider the importance of intersectionality by asking how attitudes linked to, or fear of, racism and other forms of discrimination due to differences in language skills or cultural background, or stemming from ableism, transphobia or homophobia might influence help-seeking for mental health problems.
Our commitment to safer space policies and having a peer facilitator proved important in creating a space where participants openly shared their experiences and felt supported and connected. There were several shared laughs and frequent nods from participants, suggesting that many of the shared experiences resonated collectively. Participants also gave feedback in which they expressed gratitude for having had the chance to ‘vent’. The facilitator who acted as a participant-researcher, and who is one of the authors of this paper, shared this feeling and perceived the groups as successful in enabling mutual learning and peer support. The groups were held in Finnish, and the recordings were transcribed verbatim and analysed in the same language. The focus groups lasted 125 and 88 min, respectively. The transcribed material consists of 115 pages of text (Times New Roman, font size 12, double-spaced). The extracts presented in this paper have been translated by the authors.
Analytical Method
Our analysis drew on reflexive thematic analysis (RTA; Braun & Clarke, 2006; Clarke & Braun, 2017), which was well suited to our aim of conducting reflexive and open-ended inquiry. Accordingly, we followed the six steps proposed by Braun and Clarke (2006): (a) familiarising ourselves with the data, (b) generating initial codes, (c) searching for themes, (d) reviewing themes, (e) defining themes and (f) producing the report. We used ATLAS.ti 24 for coding. Although the dataset and number of participants were relatively small, the data were rich and enabled us to identify clear patterns in line with RTA.
The analysis involved cyclical listening to the audio files and reading the transcriptions, creating and revising codes and ultimately identifying potential themes, naming and renaming them until the final ones were determined. This included constructing mind maps and diagrams to clarify the relations between themes and subthemes. The focus group facilitator led the earlier stages of the analysis, while the role of the other authors was more pronounced during the later stages. Our analysis yielded four themes, outlined in the Analysis section. In presenting the analysis, we use they/them pronouns for all participants (Finnish does not have gendered third-person pronouns). The data were pseudonymised during transcription, and participants are referred to in the analysis using the codes P1–P8. To include participants’ perspectives, an initial version of the analysis was sent to them for feedback. Three participants commented and gave positive feedback, emphasising that they appreciated the approach we had adopted.
Analysis
The themes are presented in Table 1 along with their corresponding subthemes. We discuss each theme in a separate subsection.
Themes and Subthemes.
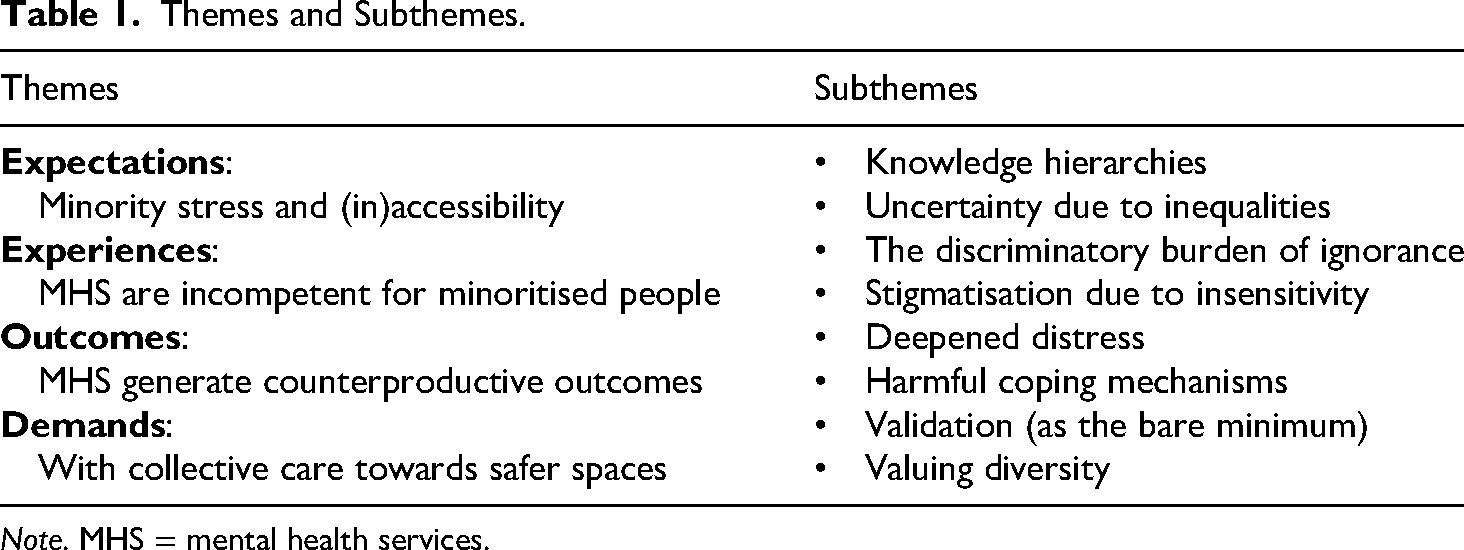
Note. MHS = mental health services.
Expectations: Minority Stress and (in)Accessibility
The first theme, ‘Expectations: Minority stress and (in)accessibility’, captures the impact of participants’ previous experiences with MHS on their current expectations regarding the accessibility of services. It has two subthemes: ‘Knowledge hierarchies’ and ‘Uncertainty due to inequalities’. In line with the minority stress cycle (Mink et al., 2014), expectations regarding MHS can be considered both a source of stress and an outcome of previous experiences, which reinforce each other. Some participants said that they had stopped going to general practitioners because their experiences had been stigmatising and counterproductive. Similar patterns have been identified in previous research on LGBTQ+ individuals’ reluctance to use healthcare services (e.g., Mereish & Taylor, 2021). For our participants, the sense of mental healthcare being inaccessible was linked to several personal and societal factors, ranging from previous experiences of practitioners misusing their knowledge power to intersectional discrimination to the Finnish transgender law. The subtheme ‘Knowledge hierarchies’ captures participants’ experiences of encounters with healthcare professionals (through whom MHS can be accessed) who had ignored their self-knowledge, leading them to refrain from help-seeking: Yeah, and I have this experience, especially with older doctors, which is why I very rarely seek help from general practitioners … because I often feel that my self-awareness and knowledge of my own body aren’t taken seriously. It's kind of like it's a zero factor, like it doesn’t matter at all, and then it's as if it's completely disregarded … so it's rare to find doctors who listen or approach the situation humbly with the assumption that, ‘Hey, maybe there's something here that I don’t know’. (P2, Focus Group [FG] 1)
The second subtheme, ‘Uncertainty due to inequalities’, specifically highlights the role of intersecting inequalities in participants’ expectations regarding MHS. In line with previous research (see Noyola et al., 2020), participants were aware of their status as a minority group, while some also mentioned their privileged status in other respects, thus pointing to the complexity of the intersectional dynamics of oppression and privilege. Class and wealth differences, for instance, were discussed as being highly relevant in shaping access to MHS. P2, among others, stated that ‘if you’re both low-income and have minority identities, then it's almost impossible to get good treatment’. Furthermore, in both focus groups, racism was mentioned as a key factor impeding help-seeking. In the following extract from FG2, in response to the facilitator's question prompting intersectional thinking, P2 described how racism had shaped their expectations regarding accessibility of MHS to a greater extent than cisheteronormativity or other bases for discrimination. Facilitator (F): Yes, so regarding the previous question, how do you think racism, language skills, cultural issues or attitudes affect… P2: Seeking help? F: Yes. P2: Yeah, well, at least for me, more than those mentioned earlier because I’ve encountered a lot of racism in healthcare, and that has perhaps prevented me even more from seeking help for those issues [mental-health-related symptoms], or, like, the fear of racism, in addition to those [transphobia and homophobia]. P3: Yeah, but it's true that racism probably, sort of, comes up faster than the other issues. P1: Yeah.
Several participants also linked their perception of the inaccessibility of MHS to ableism, which they discussed through the lens of neurodiversity and experienced, for instance, when applying for publicly funded therapy. This process absorbs a considerable amount of time and energy, involving extensive paperwork in which one is required to clearly articulate and justify one's need for therapy. The following extract from FG1 demonstrates how participants contrasted, in intersectional terms, the challenges they face in accessing MHS with those of a ‘White cishetero’, with ableism intertwined with these challenges: P1: Yeah, and it's maybe like with ableism and mental health. It's like, it's so interesting that to access mental health services, you’re expected to have a certain level of functionality and meet certain criteria. And we’re assumed to be able to justify our need like two or 10 times better than someone else [laughs], like a White cishetero [someone agrees]. So yeah, ableism really affects that a lot [someone agrees], and it's intertwined with mental health [P2: ‘Yeah’], and also to a broader extent somehow. P4: Yep, and like, I was just thinking about getting a B1 therapy statement [a medical statement required for state-funded rehabilitative psychotherapy] written for myself. [P2: ‘Yeah’] It's like a skill in itself, like being able to articulate that requirement to respond to those questions [someone agrees], so there should probably be a service for that too [someone chuckles].
According to participants, whether one receives the help they need ultimately comes down to luck, which they linked to unequal opportunities. P1 described their process of getting help as: certainly a different process in many ways than it would be for a cisgender heterosexual person … but it's all really just a matter of luck, so it's about who has that stroke of luck and who doesn’t, and that's part of the inequality.
Experiences: MHS are Incompetent When it Comes to Minoritised People
The second theme is based on an emphasis on MHS’ lack of competence in catering to the needs of LGBTQ+ young people. Whether participants talked about their own experiences or second-hand stories, they all felt that their needs had not been met. Participants frequently linked this to the individualism inherent in psychotherapy, which they saw as placing the burden of distress solely on individuals, resulting in the ineffectiveness of therapy, especially for minoritised people. For instance, in relation to emphasising the importance of intersectional approaches to mental health interventions, P4 in FG1 stated that ‘it's like those approaches themselves are already individualistic, focusing on individual resources’. This individualistic emphasis was seen as particularly problematic due to its neglect of people's diverse backgrounds, support networks and community contexts.
This theme has two subthemes: Tthe discriminatory burden of ignorance’ and ‘Stigmatisation due to insensitivity’. The first subtheme connects perceived ignorance with structural inequalities, emphasising the burden this places on LGBTQ+ young people. P1 in FG2, for instance, described experiencing discrimination when seeking help for distress associated with their trans identity process, which they perceived as transphobia, and being told by mental health practitioners that they lacked the knowledge to help. Several other participants emphasised the harmful effects of encountering ignorance in MHS, which at worst created a sense of invisibility. This was accompanied by a sense of being forced to take responsibility for making LGBTQ+ lives visible to practitioners. In doing so, LGBTQ+ young people are forced to challenge discriminatory and stigmatising stereotypes. This exposes them to microaggressions, which may disrupt the therapeutic relationship (Freeman-Coppadge & Langroudi, 2021). Participants recognised the injustice and distorted reversal of responsibility that this creates. P2, for instance, stated that ‘no queer person has any obligation to explain to anyone – it's really the other person's job’.
The second subtheme, ‘Stigmatisation due to insensitivity’, underlines participants’ experiences of practitioners failing to consider the stigma associated with queerness or other minority statuses with adequate sensitivity when interacting with LGBTQ+ young people. Encounters experienced as insensitive involved practitioners making statements or asking questions that revealed implicit bias originating from a reliance on cisheteronormative assumptions. P3, for instance, described asking a therapist whether there were representatives of sexual or gender minorities in a therapy group and receiving a response that made them feel as though their sexual minority status was unspeakable: I asked the therapist how it works because I need to know that a safe space is ensured, so that I can actually benefit from it and deal with my issues at a therapy level. They explained that ‘sexuality is such a private matter that you definitely need to build trust with others for a long time before you dare to talk about it’, and then I was like, ‘well, it's not very private for me to say that I have a girlfriend in my life, it's not like a private matter’. (FG1) it's kind of like, [the professional says] ‘Let's start focusing on that, your minority membership’, instead of focusing on what you went there to address … it's like, you have a problem, you’re seeking help for it, and then it's like, ‘hmm, you’re a bit different from others, this might be a problem’. (P2, FG1) P1: I haven’t had to face it [racism] myself because I’m sort of, I have a Finnish name and Finnish is my mother tongue, and thanks to that I’ve avoided it, but I can well imagine that it's very [unclear]. P2: I could give you one example or experience. Once, probably at the student health services, when I went there for the first time about mental health issues, and talked about gender-related issues or wanted to discuss them, one of the first questions I was asked was about my religion or my parents’ religion or my family's attitude in general. So they had a lot of assumptions about my background and my parents’ background, and it wasn’t focused on the actual issue I wanted to talk about [laughs], and I found it very irrelevant … The situation changes so that it no longer feels like it's a health-related situation for me, but rather that I’m back in the outside world in a society where I’m talking to some middle-aged White person who wants to unpack my background and other such things, so it takes a lot of attention away from [the issues], and then it's hard to talk about them. (FG2)
Outcomes: MHS Generate Counterproductive Outcomes
The third theme in our analysis, ‘Outcomes: MHS generate counterproductive outcomes’, sheds light on the impacts of participants’ experiences of MHS. Many emphasised the harmful consequences of experiencing discrimination and stigmatisation in MHS. These appear to result in the failure to establish a therapeutic alliance or to provide appropriate interventions tailored to minoritised clients. P2 in FG1 described the ‘backlash’ that occurs when one feels they do not belong to the group in group therapy, noting that it is ‘really counterproductive for the overall conversation and atmosphere’. These outcomes appeared to stem from the failure of MHS to acknowledge the diverse and intersecting identities of clients and the inequalities they face, thereby neglecting significant aspects of clients’ lived experiences. This creates feelings of exclusion and invalidation, and may result in reluctance to seek help (see also Rees et al., 2021).
The ‘Outcomes’ theme has two subthemes. The first, ‘Deepened distress’, illustrates a process in which negative experiences with MHS intensify the very distress for which participants sought help. As P3 in FG2 describes, and P1 and P2 corroborate, this results from not being seen, understood or fully accepted: P3: But I think it's a pretty significant issue if you get the feeling that you’re not understood and not fully accepted for who you are, especially when gender and sexuality issues are such big topics that are really essential in, like, the therapy process. It's really sad that most people probably feel that it's a difficult thing to approach, or that they can’t get peer support from those services. P1: And it kind of feeds into itself, or as you described, when you have one bad experience and then … you seek help, you’re not understood, or just that nothing is explicitly said, but you get the feeling like, okay, they don’t really get it, and that invalidates your experience, which certainly distresses you even more and causes more problems. P2: Yeah [laughs], I second that [laughter].
The second subtheme, ‘Harmful coping mechanisms’, is intimately connected with the previous one. The distress and low expectations resulting from experiences of discrimination and minority stress activate concrete coping mechanisms that ultimately prove harmful, such as avoiding help-seeking, sidestepping relevant topics or selectively disclosing information in encounters with practitioners: So, in my opinion, we can’t talk about it as a phobia, but it's very likely that a person in that situation is simply unaware of it and then, very often, they have to develop their own coping mechanisms, either by avoiding the situation altogether, or by adapting the way they speak or disclosing things very selectively. (P4, FG1)
Demands: Collective Care Towards Safer Spaces
The participants repeatedly emphasised the urgent need for systemic change within MHS to address intersecting forms of discrimination and to provide equitable and inclusive care. They did so in an assured manner that stressed the LGBTQ+ community's right to care that meets their needs. Hence, we labelled our fourth theme ‘Demands: Collective care towards safer spaces’. Actions aimed at resisting and challenging oppression have been identified in previous research as effective strategies for coping with minority stress. For instance, sexually diverse individuals who recognise that they are not solely responsible for dismantling oppression tend to cope better with minority stress, suggesting the importance of self-care (Noyola et al., 2020). Self-care can also be understood as an element of collective care, as recognising and communicating one's needs enables communicative relationships that help healing (Tervalon & Murray-García, 1998). We therefore interpret the participants’ demands for systemic transformation as expressions of both self-care and collective care, each of which plays a crucial role in helping to maintain individual and collective mental well-being.
The emphasis on the collective dimension of mental well-being became evident in the importance participants placed on supportive peer networks for preserving mental well-being. They highlighted the unique advantages of peer-led support groups, contrasting them favourably with interventions led by adults, who were characterised as ‘moralising’ and out of touch with young people's experiences in their efforts to ‘talk to young people about young people's issues’ (P3, FG2). As in the ‘Expectations’ theme, an intersectional divide connecting age with queerness and mental health was also clearly present here. For the participants, peer-led support groups offered an antidote to older practitioners’ ignorance and the knowledge hierarchies they perpetuated. However, despite the emphasis on peer support as a means of being understood and heard, participants also acknowledged that simply by actively listening and respecting clients’ experiences and identities, practitioners can also create affirming and supportive spaces in one-on-one encounters.
The first subtheme of the ‘Demands’ theme is ‘Validation (as the bare minimum)’, which is based on participants’ emphasis on practitioners’ capacity to listen respectfully and thus validate LGBTQ+ young people's experiences. Queer and trans people often experience challenges in having their distress acknowledged, resulting in invalidation of both their distress and their identity (Cowie & Braun, 2022). For the participants in our study, validation did not necessarily require much: they discussed incorporating safer space principles, putting effort into building trust or simply refraining from voicing prejudiced assumptions: P3: Yeah, but overall, if a therapist doesn’t know much about a topic, especially if the patient belongs to a minority, I don’t think they should be like, ‘Well, I can’t help you’, but rather, they could do a little work, like googling. Because, you know, they don’t need to know everything right away when listening. Listening with acceptance is already a good start, and not many people necessarily know how to do that. P2: Yeah, or at least not making assumptions or saying them out loud [chuckles]; somehow that would be enough… P3: Yeah, yeah, just listening to the other person's experiences. I mean, you don’t necessarily need that much, just the bare minimum. P2: …and exactly what you said about how, for many, it's enough to just have validation, and something like, ‘What you’re feeling is completely okay – it's common and others feel it too’. (FG2)
Participants discussed this need for investment with an intersectional sensitivity to diversity in experiences shaped by multiple forms of discrimination and marginalisation. For instance, in FG1, P4 stated that an intersectional approach to interventions is ‘really important’ because mental health interventions are too often ‘focused on the resources of the individual’. Here, intersectionality signifies a departure from individualism towards an awareness of lived differences and inequalities.
In calling for intersectional sensitivity, participants underscored the importance of therapists possessing cultural competence, particularly regarding marginalisation shaped by racialisation and cisheteronormativity. Their suggested approach is akin to what has been termed cultural humility, wherein mental health practitioners adopt an ‘other-oriented interpersonal stance’ to avoid making assumptions about clients’ cultural identities and their significance (Hook et al., 2013). Embracing cultural humility entails a commitment to continuous learning, self-reflection and the mitigation of traditional power differentials between therapists, clients, colleagues and communities (Metzger et al., 2023).
This connects to participants’ argument that the therapist's primary goal should be to offer support, rather than to assume an authoritarian stance of knowing everything and unilaterally providing solutions. To this end, they advocated a more collaborative and connected approach between therapist and client, where the therapist acknowledges their own fallibility and works alongside the client towards shared goals. Valuing diversity appears integral to this perspective. For instance, P1 stated that, in the end, people want to be seen and heard, and framed this as a basic need of all human beings. Their accompanying suggestion is that the diversity of human beings should be a factor in enabling people to get the help they need: Yeah, and then there's the fact that, in all their diversity, people are ultimately the same; in the end, everyone just wants to be seen and heard and so on, so ignoring differences somehow removes a basic human dimension. So that's what I think we should ultimately aim for, to ensure that the differences don’t prevent you from getting help, but maybe even become an enabling factor [in getting help]. (P1, FG1) I don’t think solving this problem is solely the responsibility of these specialised centres. In my opinion, entities like the student health services have a responsibility for the well-being of all students, and the same goes for the entire public healthcare system. I don’t think it's right that LGBTQ+ young people have to search for these places. (P2, FG2) just being able to talk to someone who is queer and nonbinary themselves, it's like wow [others chuckle], is this how it's supposed to feel – you don’t have to explain anything or feel a little tense or hesitant about how to approach it.
Conclusions
Our analysis demonstrated that the experiences of LGBTQ+ young people with MHS in Finland reveal several shortcomings in the services’ ability to meet their needs. Similar to previous research (McDermott et al., 2024; Rees et al., 2021), the analysis shed light on the vicious cycle of minority stress and how previous bad experiences with MHS may result in a reluctance to seek help and thereby exacerbate LGBTQ+ youth's mental health concerns. Minority stress theory thus serves as a helpful tool for understanding the connections between participants’ previous experiences, expectations and the outcomes of poor encounters with MHS. Furthermore, our analysis shows the entanglement of intersecting societal, systemic issues with individual everyday experiences. The influence of cisheteronormativity and other intersecting systems of oppression such as racism (see also e.g., Metzger et al., 2023) turns MHS encounters into poor ones through discriminatory and stigmatising preassumptions, a lack of knowledge, the discrediting of minoritised knowledge and a lack of respect for diversity.
What our study specifically adds to existing literature is a close consideration of youth's voices and the critique of MHS they formulated in their own terms. This critique had a hopeful and agentic tone: far from seeing successful mental health encounters as an impossibility, they suggested various measures to enhance the capacity of MHS to meet the needs of LGBTQ+ young people. In alignment with recommendations made in previous studies (e.g., Czimbalmos & Rask, 2022; McDermott et al., 2024), participants specifically highlighted the importance of reflexive attentiveness to minoritised youth's own concerns and self-definitions, and pointed out that by simply listening and adopting a humble and respectful attitude, practitioners can go a long way in providing LGBTQ+ youth with validation. The participants’ recommendations also extended to addressing the structural inequalities and inadequate resourcing of MHS. Here, in particular, the conceptual tools guiding our inquiry as researchers, such as intersectionality and cisheteronormativity, also emerged as tools for the participants themselves, helping to bridge potential differences in our viewpoints. Our peer-led focus group design allowed us to ground the use of these tools in participants’ lived experiences, thereby ensuring a close fit between the conceptual tools and the participants' lived experiences and viewpoints.
While our study is limited in scope, it yielded rich data that offer valuable insights into LGBTQ+ young people's experiences with MHS in Finland. The so-called youth mental health crisis in Finland has not been adequately addressed with due consideration of systemic inequalities in service accessibility or the impact of austerity and mental health policies on health disparities (Kurki & Rask, 2025). This is despite the increasing recognition in recent years of health disparities and the impact of systemic discrimination on mental health service provision. For example, in 2023, the Finnish Ministry of Social Affairs and Health published recommendations for identifying and reducing stigma and discrimination related to mental health, along with substance abuse problems and addiction, with the overarching aims of ensuring equal access to public services and fostering cultural diversity (Strand et al., 2023). Our findings suggest that further efforts are needed to enhance inclusivity in MHS, with specific attention paid to the perspectives and needs of LGBTQ+ young people.
It is worth noting that our participants constitute a rather select group of LGBTQ+ young people – those who were comfortable speaking in a group about sensitive issues such as mental health, well-versed in queer feminism and intersectional perspectives and highly educated. While participants’ LGBTQ+ identities were somewhat diverse, none identified as gay boy, for instance. Therefore, various intersectional experiences and perspectives may be missing from our study, including those of young people for whom talking about MHS is too difficult, and for whom the services might appear even less accessible. Had their perspectives been included, the picture painted by the findings on MHS and youth mental health might have been even bleaker.
Our analysis provides further support for the claim made in previous literature (e.g., McDermott et al., 2024; Noyola et al., 2020) that intersectional sensitivity is a key route to considering the specific features of LGBTQ+ young people's experiences and circumstances. Such an approach enables a move beyond surface-level treatments to address the underlying issues that contribute to mental health challenges (Cowie & Braun, 2022). While MHS play a crucial role in alleviating the mental distress of LGBTQ+ young people, they are no substitute for a structural transformation that challenges cisheteronormativity, racism and ableism, among other systems of inequality, on a broader scale (Mereish & Taylor, 2021; Stojanovski et al., 2022). The issues we have identified are rooted in societal inequalities perpetuated by inadequate social policies, cuts to social and healthcare funding and gaps in legislation. A sustainable transformation therefore requires addressing harmful patterns at various levels, from societal discourse and policies to the education of future practitioners. In sum, our analysis suggests the need to (a) develop practitioner training in gender, sexual and cultural diversity and antiracism, (b) address implicit biases and enhance reflexivity to improve the therapeutic alliance and (c) cultivate collective care practices in mental health interventions.
Footnotes
Acknowledgements
We wish to thank all the young people who participated in this study, and the rest of our research team, particularly Kaisa Marttila, for participating in designing and implementing data collection for the project and in making sense of the topic of this paper.
Ethical Considerations
The research reported in this paper is part of a larger IMAGINE research project, which was granted ethical approval from the Research Ethics Committee in the Humanities and Social and Behavioural Sciences and the Research Ethics Committee of the Faculty of Medicine at the University of Helsinki (Statement No. 32/2023).
Consent to Participate
The study adheres to the ethical principles of obtaining informed consent from all the participants, in writing, using a consent form.
Consent for Publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was prepared as a part of the IMAGINE project, funded by the Strategic Research Council established within the Research Council of Finland (Grant No. 352700).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the data, they have not been made available for further research.