
Abstract
Biobanks are essential tools for facilitating biomedical research, because they provide collections of human tissue linked with personal information. There is still little understanding of the underlying reasons why people participate in biobanking in the increasingly commercialised and internationalised biomedical research environment. This paper reports the results of an Australia-wide telephone survey. The paper analyses the types of obligations that members of the public may wish to see incorporated in biobank benefit sharing arrangements and the extent to which their views might be influenced by underlying norms of sharing behaviour. Latent class analysis of the dataset reveals three distinct classes of respondents. We link one of these with the norm of reciprocity, one with the norm of social responsibility. The third is not clearly linked with any one norm of sharing behaviour. The implications of these findings on biobank benefit sharing arrangements are discussed.
Keywords
1. Introduction
Biobanks are essential tools for facilitating biomedical research, because they provide collections of human tissue linked with personal information. A recent information paper published by the Australian National Health and Medical Research Council (NHMRC) describes the vital role of biobank resources in: “understanding the risk factors that underlie complex diseases, and translating biomedical research into real improvements in health care, especially through advances in pharmacogenomics and personalised medicine, to minimise adverse drug reactions and match drugs more effectively to the patient” (NMHRC, 2010: 6). Over the past decade, new large-scale population biobanks have been established in a number of countries. In the UK, for example, UK Biobank has been established for the purpose of providing a resource for research relating to a wide range of diseases, including cancer, heart diseases, diabetes, arthritis and forms of dementia. It has already recruited over 500,000 people aged 40–69 from “as widely generalisable a population sample as is practicable” (UK Biobank, 2007: 4).
Ethical, regulatory and social challenges associated with biobanking of human tissue and personal information have been extensively canvassed by international and national policy agencies (e.g., internationally OECD, 2005, 2009; nationally in Australia ALRC/AHEC, 2003; NHMRC, 2010), academic commentators (see Campbell, 2007; Caulfield, 2007) and biobanks themselves (e.g., UK Biobank, 2007). These and other publications recognise that access to biobank resources for research purposes should, of necessity, be facilitated, bearing in mind the need for appropriate regulation to protect participant privacy and related matters. Increasingly, attention is being turned to the need to establish networks of biobanks and frameworks for sharing of biobank resources internationally to ensure that the research potential of biobanking is fully realised (e.g., Kaye, 2009). These and other publications also recognise that success of the biobanking endeavour relies on voluntary and ongoing participation. Although public consultations have been undertaken by some biobanks during establishment processes and studies have investigated willingness to participate in biobanking (reviewed in Critchley, Nicol, Otlowski and Stranger, 2010), there is still little understanding of the underlying reasons that drive participation. In particular, the extent to which the involvement of commercial and international partners impacts on motivation to participate is unclear.
Commercial involvement
Intuitively it seems likely that commercial involvement in biobanking will cause some potential participants to question their motivation to participate, because it will be seen by them as introducing a profit motive into what is otherwise a public good activity. Public consultations conducted in the UK tend to support this proposition, suggesting that there is a general public unease about the involvement of the private sector in biobanking and biomedical research (Webster et al., 2008). This unease is likely to be heightened when commercial partners are from other countries, because of the perceived risk that the potential community benefits arising from biobank activities will be moved offshore. However, the public good focus of biobanks does not necessarily preclude involvement of commercial and international partners. In fact, fulfilment of the promise to translate research into improvements in health care will often require the involvement of commercial entities, including large multinational pharmaceutical companies, particularly for the costly and onerous clinical trials procedures required for approval of new drugs.
The language of benefit sharing is used to describe types of mechanisms that might be put in place to ensure that benefits stemming from biobanking and use of biobank resources in biomedical research are not and not perceived to be the exclusive domain of the commercial sector. Internationally, various instruments give explicit reference to benefit sharing, including the UNESCO Universal Declaration of Bioethics and Human Rights (UNESCO, 2005), the UNESCO International Declaration on Human Genetic Data (UNESCO, 2003) and the Human Genome Organisation (HUGO) Ethics Committee’s Statement on Benefit Sharing (HUGO, 2000). The recently formulated OECD Guidelines for Human Biobanks and Genetic Research Databases (OECD, 2009) include a whole section on Custodianship, Benefit-sharing and Intellectual Property, emphasising that benefits should be shared as broadly as possible (Principle 9.B). However, to date scant attention has been paid to the issue of whether to include formalised benefit sharing obligations in biobank governance and regulatory frameworks and what exact forms such obligations might take. Moreover, there is little empirical research on what types of benefit sharing arrangements members of the public may wish to see incorporated into biobank governance and regulatory frameworks. There is, however, a growing body of evidence that indicates that people fear access to benefits of biomedical research will be reduced if commercial interests are involved (e.g., Critchley, 2008). Thus, whenever there is commercial involvement in biobanking or research using biobank resources, public anxiety and distrust are likely to be aroused (German National Ethics Council, 2004: 27). This suggests that incorporation of benefit sharing obligations into regulatory frameworks may buffer an erosion in public trust in biobanks with industry links.
The current research
The research reported here addresses some of these deficits in knowledge. The data were obtained from a telephone survey of public opinion relating to biobanking and benefit sharing in Australia. Respondents were asked to consider obligations that would lead to direct sharing of benefits with biobank participants (e.g., payment for participation or preferential access to new treatments) and obligations that would lead to sharing of benefits with society more generally (e.g., open dissemination of research results and equitable access to new treatments). This reflects the types of obligations mooted in international policy literature. Some instruments focus on direct sharing of benefits with the participant or their immediate community group. HUGO Ethics Committee’s Statement on Benefit Sharing (HUGO, 2000), for example, defines benefit as: “a good that contributes to the well-being of an individual and/or a given community (e.g. by region, tribe, disease-group …).” In contrast, the UNESCO International Declaration on Human Genetic Data (2003) focuses on more general benefit sharing obligations: “benefits resulting from the use of human genetic data, human proteomic data or biological samples collected for medical and scientific research should be shared with the society as a whole and the international community” (Article 19).
The survey also examined whether attitudes to benefit sharing were affected by the type of biobank and/or user of biobank resources (commercial and non-commercial, Australian and international). It has been reported elsewhere that respondents to this survey were highly in favour of being informed about what benefit sharing obligations are in place before deciding on whether to participate in biobank research and also cared about the nature of these obligations (Nicol and Critchley, 2009). The purpose of this paper is to determine what types of obligations people wish to be incorporated in biobank benefit sharing arrangements and the extent to which these views might be influenced by underlying norms of sharing behaviour.
Norms underlying participation in biomedical research
Research indicates that different publics have different attitudes towards contributing to biomedical research. Dixon-Woods et al. (2008) found that families of children with cancer who considered themselves to be part of a research community were mostly enthusiastic about contributing to the research effort. Similarly, Madsen et al. (2002) found that non-participants in clinical cancer trials were significantly less positive about contributing to research than participants. National public opinion surveys from Sweden, Ireland, the UK, the US and Australia find a range of factors influence willingness to contribute, including: the perception that the research will be beneficial (Cousins et al., 2005; Kettis-Lindblad, Ring, Vibirth and Hansson, 2005); general support for medical or genetic research (Cousins et al., 2005; Kettis-Lindblad et al., 2005); trust in scientific actors (i.e., researchers, research organisations, biobanks) (Critchley et al., 2010; Kettis-Lindblad et al., 2005); history of blood donation (Kettis-Lindblad et al., 2005); age (Kettis-Lindblad et al., 2005; Webster et al., 2008); gender (McQuillan, Porter, Agelli and Kington, 2003); education (Cousins et al., 2005); experience with a genetic disease or medical condition (Cousins et al., 2005); and being a parent (Cousins et al., 2005). Three key themes emerge: the majority of respondents appear to take an altruistic approach to their own participation in biomedical research; they tend to expect that there should be public benefits arising from biomedical research; and they expect that new health care products should be made widely available. There is, however, no research to date that directly examines the influence of various forms of benefit sharing on public expectations towards participation in biobanking. The norm of reciprocity has been posited to explain attitudes towards and intention to participate in biomedical research (Dixon-Woods et al., 2008). We expect this norm will also guide public expectations relating to biobank participation. Furthermore, we posit that the norm of social responsibility will play a role.
The norm of reciprocity
Dixon-Woods et al. (2008: 76) argue that the norm of reciprocity plays a crucial role in determining public attitudes towards contributing to medical research. The norm of reciprocity is an expectation that individuals should help (and not harm) those who have helped or are likely to help them (Gouldner, 1960; Homans, 1961; Kanellopoulou, 2009). Research has consistently found that human beings desire reciprocity and are likely to reciprocate themselves (see Fehr and Gächter, 2000 for a review). Studies have demonstrated that expectation for reciprocity is associated with more positive attitudes towards social policies that reward those who have made a contribution than policies which reward both contributors and non-contributors (Bowles and Gintis, 1998; Haferkamp, Fetchenhauer, Belschak and Enste, 2009). Based on the norm of reciprocity, biobank policies that directly reward contribution should promote positive public attitudes, trust and in turn, a greater desire amongst members of the public to participate.
Some theorists argue that the norm of reciprocity arises from a desire to maximise self-interest, particularly in the long term (Axelrod, 1984; Fudenburg and Tirole, 1991), as giving or sharing with others is a strategy to ensure that one will receive similar benefits at a later date. Others view it as a valued end in itself, arising from a fairness heuristic, or desire for equity when distributing resources (Fetchenhauer and Dunning, 2009; Tyler, 1994). Both views argue that the norm of reciprocity prescribes a set of interrelated beliefs that expect a good deed to be returned. Members of the public who endorse this norm should therefore support the idea that biobanking should directly benefit those who contribute to the biobank. This could be in the form of a monetary fee or provision of affordable access to any treatments developed from research using biobank resources (or both). Furthermore, individuals guided by reciprocity should expect that contributors to the biobank will receive preferential access to health treatments developed from biobank research over those who have not directly contributed (whether from the general Australian community or the international community).
People guided by the norm of reciprocity should also believe that those who may benefit from accessing biobank resources (e.g., external researchers, and particularly commercial researchers) have a duty to reciprocate via the provision of a monetary fee or other in-kind payments. On this basis, if a biobank provides external researchers with access to its resources then the biobank should receive benefits in return, whether financial (e.g., payment for use of resources or share of future profits) or non-financial (e.g., return of research results). This should particularly be the case when access is requested by commercial and international research organisations that are less likely to directly benefit the local community or biobank participant than are non-profit local researchers.
The norm of social responsibility
The norm of social responsibility is the internalisation of the altruistic principle that those who are in need should be assisted (Berkowitz, 1972; Schwartz, 1975). When need varies, distributing resources to those who need them most is considered fair. Unlike the norm of reciprocity, social responsibility dictates that people should help those in need without consideration for past contributions and present or future direct benefits.
The norm of social responsibility should therefore encourage the belief that individuals should willingly and freely contribute to a biobank even if there is no prospect of future gain for them, their family or even their local community. Allied to this, individuals should not favour the distribution of health care benefits based on contribution, but rather based on need. As such, individuals guided by this norm should expect that biobanks will ensure that all people in need (regardless of whether they contributed) have access to any treatments developed from biobank activities. Moreover, this norm should encourage the belief that biobanks have a responsibility to assist all research (public or private, local or international) that could eventually lead to improved health care. On this basis, individuals should favour access policies that require biobanks to make their resources available to other researchers without discrimination, provided there are adequate guarantees that the research is scientifically valid and ethically appropriate.
While individuals guided by the norm of social responsibility should not expect biobanks to profit from the use of their resources, they may nevertheless accept the necessity of charging fees for access, if this assists in maintaining the ongoing viability of the biobank. However, they should be unsupportive of differential fee structures for commercial and non-commercial users. Notions of responsibility should also come into play when considering the obligations of external researchers to biobanks. While the norm of social responsibility should encourage the belief that external researchers should not be required to reward the biobank financially, it also suggests that there is an obligation both to return research results to the biobank and to disseminate them more publicly in the interest of more broadly facilitating research that may lead to improvements in health care.
Examining the roles of reciprocity and social responsibility in guiding attitudes towards biobanking
Public opinion research in the area of biomedical science has to date primarily taken a variable centred approach, aiming to establish relationships between different variables within an assumed homogeneous public. This study uses a person centred approach (Laursen and Hoff, 2006) to identify distinct patterns of beliefs, highlighting the presence of different publics and enabling the development of public typologies. Identifying the existence of specific patterns of benefit sharing beliefs within the community will enable us to test the hypotheses that notions of reciprocity or social responsibility guide public expectations relating to the distribution of biobank benefits.
We hypothesise that within any given community there will be different patterns of benefit sharing beliefs guided by two underlying normative belief systems: reciprocity and social responsibility. While it is not necessarily the case that either norm will operate in isolation from the other, it is posited that in any single community we are likely to find one or more publics for whom one norm exerts a dominant influence on benefit sharing beliefs and one or more other publics for whom the other norm dominates. The two norms dictate different patterns in expected benefits flowing to participants, biobanks and external researchers rather than independent differences in single beliefs. Identifying these patterns within a community will therefore enable the development of governance frameworks for biobanks that incorporate the normative expectations either of the majority of members of that community, or of members of the community who are most likely to participate in biobanking, depending on the nature of the biobank. In general, large-scale population biobanks will need to be aware of expectations of the community as a whole, whereas smaller-scale disease-specific biobanks will need to focus more attention on their target group of potential participants (e.g., those with a genetic condition).
In this study, we expected to identify two or more distinct publics (or classes of respondents) using latent class analysis. We expected that one or more class would be predominantly (but not necessarily entirely) influenced by the norm of reciprocity, represented by members of the public who strongly believe that biobank participants should receive some sort of return for participation. The type of biobank and/or user of the biobank’s resources should have a significant impact on the strength of those beliefs. We hypothesised that this class of individual should also believe that access to potential treatment developed from biobank research should be made more available to participants than to members of the general Australian public and even more than to members of the international community. This class should also strongly believe that biobanks should be rewarded (financially or in-kind, e.g., return of research results) by external researchers who access their resources, and that fees paid by commercial and international researchers should be significantly higher than those from public and Australian researchers.
We also predicted that a qualitatively different class (or classes) of respondents would exist within our sample demonstrating a pattern consistent with the norm of social responsibility. We expected that this class would tend to believe that participants should not be paid for their contribution to biobank resources (irrespective of the type of biobank) and that they should be no more entitled to access to treatments than other members of the Australian or international community. Rather, treatments should be distributed equally to all those considered in need. We expected that this class would believe that biobanks should not receive financial reward beyond cost-recovery from external users of their resources, regardless of whether those users are from a public, for-profit or international research organisation. We predicted that this class would, however, demonstrate a strong expectation that other researchers should be obliged to publicly disseminate research results.
A final aim of this study was to explore differences between classes in terms of demographic characteristics, trust in biobanks, beliefs that biobanks will lead to health care benefits, and reported intention to participate in biobank research. Because this is the first study to use a person centred approach in relation to benefit sharing beliefs, specific hypotheses were not made relating to expected class differences on these variables. Instead, differences were explored to enable a description of the classes and to guide further research investigating benefit sharing beliefs.
2. Method
Procedure
A total of 1000 Australians over the age of 18 years participated in a Computer Assisted Telephone Interview (CATI) that conformed to the ethical standards of the Australian Psychological Society. An additional 361 Tasmanians were also interviewed, but their responses were not used in the present research. A sample size of 1000 was deemed necessary to achieve an acceptable margin of error in responses (i.e., 3.1) and a confidence interval of 95% assuming a 50% split on each question (American Association for Public Opinion Research [AAPOR], 2007). A telephone survey was considered the most appropriate methodology given that a large-scale survey of a national population was needed to identify different classes or publics. As pointed out in an expanding body of literature (for example, Dixon-Woods et al., 2008; Emirbayer and Sheller, 1998; Hansson, 2009), there is no one “public” but a variety of publics. Large-scale surveys allow for analysis of differences in attitudes between different groups within society, and are more economically feasible than obtaining a national sample via focus groups or face to face interviews. Telephone surveys were also chosen because they tend to: maximise response rates (compared to mail out and online surveys; Cousins et al., 2005); increase the representativeness of the sample; ensure anonymity amongst respondents; enable the ability to randomise question presentation to avoid order effects; reduce the time involved in data collection; eliminate the need for data entry; and allow complex issues to be clarified by trained interviewers, thereby increasing confidence in the responses.
Telephone numbers were randomly selected from the electronic White Pages to represent the proportion of residents residing in each Australian State and Territory. From these, 10,682 numbers were randomly selected by the CATI software for use in the survey. A quota was used to ensure that the sample was representative of each State and Territory. Of the 10,682 phone calls, 1361 completed interviews were obtained. The minimum response rate was 19.0% (maximum = 22.9%), and the cooperation rate was 29.0% (maximum = 30.1%), taking known (e.g., refusals, under 18 years) and unknown (e.g., no answer, not working) eligibility into account. Response rates were calculated according to the AAPOR’s (2007) definitions and calculations and were typical of response rates found in other Australian social surveys (Critchley, 2008; Critchley and Nicol, 2009).
Participants
In comparison to the Australian Bureau of Statistics (ABS) Census data for 2006, the sample was representative of the Australian population in terms of state, education and occupation (i.e., no significant differences were found between the sample and ABS distributions), but was over-represented by older individuals (M = 53.31 years, SD = 16.73; Range = 18–94) and females (66%). The data were therefore weighted according to ABS (2006) proportions for gender and age groups.
A total of 22.1% of the sample had heard of the term biobank (or genetic data base). In contrast, only 7% of participants in a UK Biobank CATI survey (Webster et al., 2008) were aware of the UK Biobank. This is despite an extensive media campaign relating to that particular biobank’s establishment. In the present survey, 12.0% of the sample had previously worked in an area involving medical research. Not surprisingly this was significantly associated with awareness: those who had worked in medical research were more likely to have heard of biobanks than those who had not, χ2 (1) = 11.60, p = .001. Most participants indicated that they cared about biobanks placing conditions on the use of their resources by other researchers. When asked, “how much do you generally care about Australian university biobanks placing conditions upon the use of its resources by other researchers” the mean score on an 11-point scale (where 0 = don’t care at all and 10 = care a great deal) was 7.80 (SD = 2.41). Just over one quarter of the sample reported that they had been diagnosed with a disease that has a genetic cause (27.8%), and over half (57.5%) had a close friend, partner or family member who was diagnosed with a genetic disease. Most participants (80.3%) had between one to twelve children (M = 2.58, SD = 1.26), 19.7% having none.
Measures
Respondents were asked a series of questions relating to biobanks in general, benefit sharing and demographic information. Each construct and its measure are described below. The full survey including questions, instructions and information presented to respondents is available from the authors on request. The survey questions were guided by previous biomedical public opinion surveys (e.g., Critchley, 2008; Critchley and Nicol, 2009) that demonstrate acceptable reliability and validity, and literature discussing benefit sharing options (Nicol, 2006). All responses were accompanied by an 11-point scale (0–10) to ensure consistency and assist comprehension of the question responses. At all times respondents were allowed to respond “don’t know.” The survey was piloted on twenty randomly selected respondents to check for understandability and the ability to discriminate between respondents, resulting in a low number of “don’t know” responses for all questions (all under 3.3%), indicating the vast majority could comprehend and provide an answer to each question. An inspection of the distribution of questions revealed adequate variability suggesting the questions were able to discriminate between different respondents with different attitudes/opinions.
Trust
Trust in biobanks was assessed by asking respondents to indicate how much they trusted an Australian university biobank (0 = “do not trust at all,” 10 = “trust a great deal”). Trust relating to three other types of biobank (Australian commercial, international commercial and international university) was also assessed, and will be reported elsewhere. Prior to assessing trust, participants were presented with the following definition of biobanks: A biobank is a place where human tissue samples are stored. DNA is gathered from these samples and linked to other health information about the donors, their families and past generations. The linked information becomes a biobank resource that may help researchers identify the genetic causes of human diseases. It is hoped that biobank resources will lead to cures for a wide range of conditions, including diabetes, heart disease and cancer. Biobanks are required by law to obtain permission from participants to use their samples and to link them with other health information. They are also required by law to ensure confidentiality. Biobank resources are expected to be kept secure, so that insurers, employers and others can’t access them.
Intention to participate
Intention to participate in a government funded Australian university biobank was then assessed. Participants were asked: I would like to ask how you would feel about participating in biobank research. Imagine that you are approached by a genetic researcher from a government funded Australian university biobank. They ask for your permission to use a blood sample that was taken from you in the past for a medical procedure.
Two options followed, which were presented in a random order. The first asked participants “on a scale from 0 to 10, where 0 means ‘not at all likely’, and 10 means ‘very likely’, how likely is it that you would let the biobank use your blood sample for research purposes?” and the second, “using the same scale, how likely is it that you would let the biobank link your blood sample with your medical records?”
For the intention measure and subsequent general biobank questions, we focused on Australian public university biobanks. We expected, as outlined above, responses to significantly vary according to the type of operator. Assessing intentions as well as perceived benefits for the types of biobank identified above was not possible owing to time constraints. More importantly, our interest in this research was primarily around Australians’ reactions to Australian public university biobanks.
Perceived benefits
A series of questions was designed to capture the perceived benefits of research using biobank resources. Participants were asked their “thoughts on the benefits of research using biobank resources.” Using a scale from 0 to 10, where 0 means “not at all likely” and 10 means “very likely,” participants were asked, “how likely do you believe that government funded Australian university biobanks will lead to: better public health care for you; better public health care for your family; better public health care for Australians; and better public health care for people in third world countries?” The questions were presented in a randomised order across participants.
Benefit sharing – payment to biobank participants
Three questions were designed to assess respondents’ attitude towards paying biobank participants. Before these questions were asked the following information was read out: Research using biobank resources is aimed at developing treatments for medical conditions (for example drugs, diagnostics or therapies) which could be for the benefit of humanity. I am now interested in your thoughts about giving individual payment to the people who give permission to biobanks to store and use their tissue.
Respondents were then asked, “Using a scale from 0 to 10, where 0 means ‘disagree strongly’, 5 (the midpoint) means ‘mixed feelings’ and 10 means ‘agree strongly’, please indicate the extent to which you agree or disagree with the following:
Donors should receive payment from the biobank if their contribution is used for commercial company research
Donors should receive payment from the biobank if their contribution is used for publicly funded research
Donors should receive payment from the biobank, even if their contribution is not used in research.”
The first two questions in this series were randomised, but the third more general question was always presented last to avoid any possible contamination of answers given to questions 1 and 2. If respondents were to answer a more general question before a context-specific one (that is questions 1 and 2), any differences across contexts may be compromised.
Benefit sharing – payment to biobanks
The next set of questions was designed to assess attitudes towards researchers paying for access to resources of government funded biobanks, and whether attitudes differ across public and private, and Australian and international contexts. Respondents were first asked “Whether or not you believe that government funded biobanks should receive some payment for allowing other organisations to access their biobank resources.” Responses to all randomised options (except option 5, asking whether biobank resources should be made freely available to all legitimate research organisations, which was always presented last to avoid priming respondents) ranged from 0 to 10, where 0 = “disagree strongly,” 5 (the midpoint) = “mixed feelings” and 10 = “agree strongly.” The Statements relating to payment of biobanks were as follows:
The biobank should receive payment if their resources are to be used by an Australian commercial company
The biobank should receive payment if their resources are to be used by an international commercial company
The biobank should receive payment if their resources are to be used by a publicly funded Australian research organisation
The biobank should receive payment if their resources are to be used by a publicly funded international research organisation
Biobank resources should be made freely available to all legitimate research organisations
Benefit sharing – access to treatments
Attitudes towards access to treatments developed from biobank research were assessed via three questions, designed to assess participants’ attitudes towards companies being required to distribute new treatments developed from biobank resources to donors, developing countries and all Australians. Before the conditions were presented, respondents were presented with the following: I am now interested in your thoughts on whether or not Australian public biobanks should place conditions on the use of its resources. I am specifically interested in the situation where commercial companies want to access biobank resources so that they can develop new drugs and treatments. Again using the same scale, please indicate the extent to which you agree or disagree with the following:
Before being allowed to access biobank resources, companies must agree to make new treatments developed from biobank resources affordable to all those donors whose resources were used
Before being allowed to access biobank resources, companies must agree to make new treatments developed from biobank resources affordable to developing countries
Before being allowed to access biobank resources, companies must agree to make new treatments developed from biobank resources affordable to all Australians
Again, an 11-point scale was used where 0 = “disagree strongly,” 5 (the midpoint) = “mixed feelings” and 10 = “agree strongly.” The statements were randomised to avoid priming.
Benefit sharing – access to research results
Access to research results was measured by two questions. Respondents were asked for their “thoughts on biobanks placing conditions on the use of its resources by other legitimate researchers.” Using the same 11-point agree to disagree scale, they were asked for their level of agreement to two statements. The first was, “Before being allowed to access biobank resources, researchers must agree to give the biobank all of their research results that were found by using the biobank’s resources. By research results I mean original data files, records and reports.” The second was, “Before being allowed to access biobank resources, researchers must agree to publicly release all of their results that were found using the biobank’s resources. By research results I mean original data files, records and reports.”
3. Results
This research aimed to identify distinct publics that differ in terms of their beliefs about benefit sharing. Specifically it was expected that there would be at least two groups that would display a pattern of beliefs consistent with the norms of reciprocity and/or social responsibility. Latent class analysis (Goodman, 1974) was used to identify groups or classes that demonstrated different patterns of beliefs across the variables relating to payment to biobank participants, payment to biobanks, access to treatments and access to research results. Beliefs relating to payment to participants (three items), payment to biobanks (four items), distribution of treatments (three items) and distribution of research results (two items) were used to form the classes via Latent GOLD Version 3.0.1 (for a description of this technique see Vermunt and Magidson, 2000). Descriptive statistics for these variables are shown in Table 1.
Descriptive statistics for all benefit sharing variables.

Note: Total weighted n = 993.
Table 1 shows that the sample as a whole was opposed to payment being made to biobank participants, with all three mean scores below the midpoint of 5. Respondents were, however, significantly (p < .001) more likely to agree that biobank participants should be paid if their resources are used by a commercial research company than if they are used by a publicly funded research organisation or the biobank itself (the latter two mean comparisons were not significantly different). Payment to the biobank was preferred to payment to participants, with mean scores being above 5 for all variables. However, attitudes were significantly influenced by the type of biobank user. A 2 (public, commercial) by 2 (Australian, international) repeated measures ANOVA revealed that respondents were significantly more likely to agree that the biobank should be paid if its resources are used by a commercial company compared to a public research organisation, F(1, 1014) = 183.69, p < .001, η = .15, and if its resources were used by an international compared to Australian company, F(1, 1014) = 42.40, p < .001, η = .04. The commercialisation by location interaction was also significant, indicating that the increased agreement that biobanks should be paid if their resources are to be used by commercial compared to public organisations was stronger when the organisation was Australian compared to when it was international, F(1, 1014) = 39.02, p < .001, = .02.
Table 1 also shows that the sample was strongly in agreement that any treatments developed from research using biobank resources should be made freely available, particularly to all Australians followed by those in developing countries and biobank participants (all mean comparisons were significant at p < .001). Respondents were also likely to agree that those using biobank resources should return the research results to the biobank and make their research results public (mean scores on these two variables were significant at p < .005).
Inspection of responses to the variables in Table 1 revealed a trimodal distribution. Most participants responded at either the low or high end of the 11-point scale or at the midpoint on all variables. Thus three groups were formed to reflect the ordinal properties of the response for latent class analysis. Those scoring under 5 were considered as disagreeing, those scoring at 5 as having mixed feelings, and those at 6 and higher as agreeing. Respondents (n = 13) with more than 30% of missing responses across the 12 items were excluded, leaving a total of 987 cases. Missing values of those with less than 30% missing (n = 12) were estimated using the SPSS (Version 16) EM method.
To determine the correct number of classes, the Bayesian Information Criterion (BIC) and classification error statistics were used. As recommended by Vermunt and Magidson (2000), the simplest model with the smallest BIC value and lowest classification error was chosen to represent the number of identified classes. To account for a violation of the assumption of local independence, residuals within the participant, biobank, treatment and research results questions were free to covary. The BIC statistics suggested the presence of three classes (3-class = 15640.51; 4-class = 15651.25), as did the classification error (3-class = .07; 4-class = .13) and Entropy R2 (3-classs = .79; 4-class = .72). Figure 1 shows mean scores on variables across each class.

Mean agreement score across class.
Key features of the classes
Class 1
Figure 1 shows Class 1 is the largest, containing over half of all respondents (57.03%). The dominant features of this class are:
agreement that biobank participants should be paid for their participation when biobank resources will be used by commercial researchers, with a more equivocal response in relation to other users. A repeated measures ANOVA across the three payment to participant variables showed that this effect was significant. Respondents in this class were more likely to agree that biobank participants should be paid if their resources are to be used by a company compared to a publicly funded researcher (p < .001) or the biobank itself (p < .001);
agreement that the biobank should be paid for access to its resources, a clear distinction drawn between commercial and non-commercial users (with higher agreement that commercial users should pay) and some distinction between Australian and international users. A 2 (public, commercial) by 2 (Australian, international) repeated measures ANOVA was computed and the results revealed that respondents in this class were significantly more likely to agree that biobanks should be paid if their resources are to be used by commercial compared to public organisations (the main effect F statistic for commercialisation was significant at p < .001, = .20). The main effect of location was also significant (at p < .001, = .07), suggesting that respondents in this class were more likely to agree that biobanks should be paid if the user of their resources is not Australian;
strong agreement that new treatments should be made available across all categories, with a notably stronger positive attitude towards free access to biobank participants than for Classes 2 and 3 (all differences significant at p < .001); and
agreement that research results should be returned to the biobank and publicly disseminated.
The equivocal views about payment to biobank participants expressed by this class of respondents (except when a commercial company uses the resource, where payment is expected), combined with their high level of agreement that biobank participants should receive free treatment (significantly higher than Classes 2 and 3 at p < .001), their strong belief that biobanks should be paid across all categories of users and their differentiation between types of users all point towards a conclusion that the norm of reciprocity is exerting a significant influence. However, their strong agreement that treatments and research results should be broadly disseminated suggests that the norm of social responsibility also plays some guiding role.
Class 2
Responses in Class 2 included 28.41% of the sample and displayed the following trends:
strong disagreement that biobank participants should be paid for their participation with no user-specific differences. A repeated measures ANOVA across the payment to participant variables showed no significant differences in responses for this class. Respondents in Class 2 appeared therefore to be unaffected by commercialisation of research when expressing their views on whether biobank participants should be paid;
somewhat equivocal views on whether the biobank should be paid for access to its resources, with some distinction being drawn between commercial and non-commercial users (payment being favoured for commercial users) and less distinction made between Australian and international users. As with Class 1, results of a 2 (public, commercial) by 2 (Australian, international) repeated measures ANOVA revealed that respondents in Class 2 were significantly more likely to agree that biobanks should be paid if their resources are used by commercial compared to public organisations (the main effect for commercialisation was significant at p < .001, = .12). However, location (Australia or overseas) had no significant effect;
strong agreement that new treatments should be made available across all categories. As with Class 1, all Australians and those in developing countries were preferred over biobank participants (all differences significant at p < .001); and
essentially the same levels of agreement as for Class 1 that research results should be returned and publicly disseminated.
Respondents in Class 2 seem to be influenced rather more by the norm of social responsibility than reciprocity, especially in their strong disagreement that biobank participants should be paid and the apparent lack of distinction in their attitudes towards payment to different types of research organisations using biobank resources. The strong belief that all those in need should receive affordable access to any developed treatments (i.e., especially Australians and developing countries) also suggests an underlying norm of social responsibility amongst members of this class. However, other factors suggest that the norm of reciprocity exerts some influence in this class, particularly the difference in beliefs with regard to the obligation of commercial and public users to pay biobanks for access.
Class 3
A minority of respondents who fell into Class 3 (14.56%) displayed the following trends:
disagreement that biobank participants should be paid for their participation with slightly higher agreement that participants should be paid if their resources are to be used for commercial purposes. However, as with Class 2, a repeated measures ANOVA across the three payment to participant variables showed that there were no significant differences in responses. Thus attitudes towards payment to the participant were not influenced by commercialisation amongst this class;
equivocal views on whether the biobank should be paid for access to its resources, with some distinction being drawn between commercial and non-commercial users and Australian and international users. As with Classes 1 and 2, the results of a 2 (public, commercial) by 2 (Australian, international) repeated measures ANOVA revealed that Class 3 respondents were significantly more likely to agree that biobanks should be paid if their resources are to be used by commercial compared to public organisations (main effect for commercialisation was significant at p < .001 = .07), but as with Class 2, location had no significant effect;
the same pattern of responses as the other classes relating to the availability of new treatments and dissemination of research results, but with much lower levels of agreement (significantly different at p < .001 for all comparisons across classes).
Although it is difficult to predict the precise reasons for the pattern of responses shown by Class 3 respondents, it may be that they are not as strongly influenced by either the norm of social responsibility or the norm of reciprocity, or simply that they have not yet turned their attention to the issues presented in this study.
Common trends
Aside from the similar views between Classes 1 and 2 on dissemination of research results, there was one other notable commonality of views shared between all three classes. Figure 1 shows that on average, all three classes thought it more agreeable that treatments be made available than it was to pay biobank participants. All mean agreement scores for the payment to participant variables were significantly lower than agreement that treatments should be made freely available to the biobank participant (all three paired sample t-tests were significant at p < .001 for each class). Respondents in Classes 1 and 2 also agreed that treatments should be made more readily available to all Australians and to those in developing countries than to biobank participants (all paired t-tests comparing biobank participants with people from developing countries across these two classes were significant at p < .001). Although Class 3 agreed equally that treatments should be made available to biobank participants and people from developing countries (p > .05), they were significantly more likely to agree that all Australians rather than either biobank participants (p < .001) or people from developing countries (p < .005) should receive affordable treatments. These results further suggest that both norms tend to exert some influence across all three classes. Broad agreement as to access to treatments could be seen as having both a social responsibility component (broad sharing of benefits with those most in need) and a reciprocity component (paying back for the benefit received). It is unclear whether the preference that is given to Australians is norm-driven or perhaps a more simple display of patriotism, or whether it arises for some other unrelated reason.
Effect of group characteristics
To further explore the nature of the classes’ benefit sharing beliefs, each was compared in terms of their group characteristics, that is, trust in a publicly funded biobank, intention to participate in biobank research, beliefs in the benefits of biobank research and their demographic characteristics. One-way ANOVAs were computed for trust, benefit belief, intention to participate, and age across classes, and Chi-square statistics were computed for the categorical variables, genetic condition experienced by the self and significant others, parental status, gender and education. Table 2 shows the mean comparisons across classes for all continuous variables.
Means and standard deviations for all continuous group characteristic variables across class.
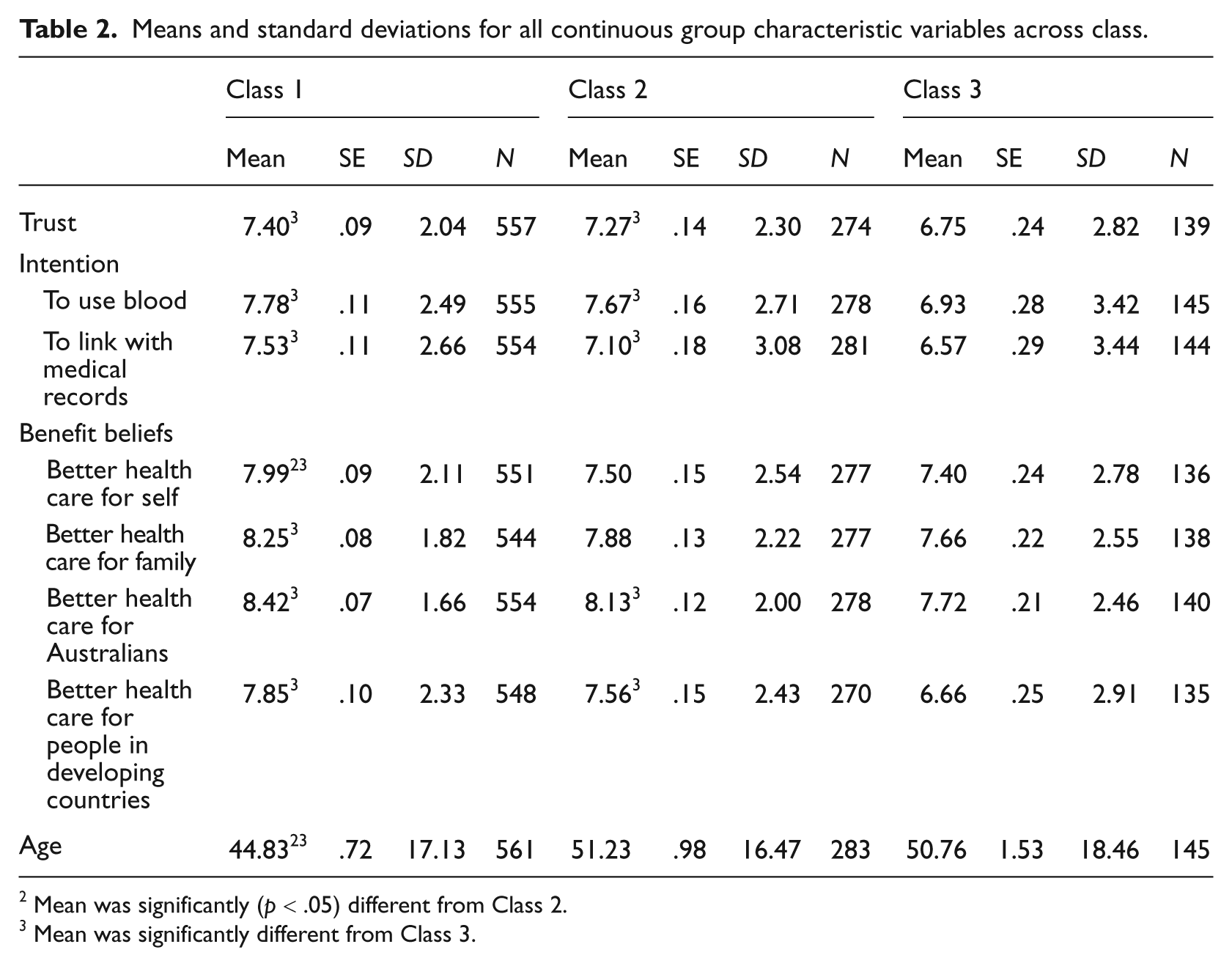
Mean was significantly (p < .05) different from Class 2.
Mean was significantly different from Class 3.
The results in Table 2 illustrate that Class 1 respondents tended to have relatively higher trust in biobanks and stronger intention to participate in biobank research than the other classes, and were more likely to believe in the benefits of biobanks, although these differences were only significant when compared with Class 3. One exception was that Class 1 respondents were significantly more likely than Class 2 respondents to believe that biobanks would result in better health care treatments for themselves. Respondents in Class 1 were still more likely to believe that all Australians and their own families would benefit more than themselves (also true for Classes 2 and 3). Table 2 shows that respondents in Class 1 were significantly younger than the other two classes.
The results of Chi-square analyses revealed that the proportion of respondents with a genetic condition (χ2(2) = 1.23, p > .05) and those who had a significant other with a genetic condition (χ2(2) = .13, p > .05) were statistically equal across classes. Parents, however, were significantly more likely to reside in Class 2 (adjusted residual = 2.0) and Class 3 (adjusted residual = 2.0), and less likely to be in Class 1 (adjusted residual = -3.4) than would be expected by chance, χ2(2) = 12.28, p < .005. Females (adjusted residual = 3.4) were also more likely to be in Class 2 than males, and less likely to be in Class 1 (adjusted residual = -2.3), χ2(2) = 11.66, p < .005. Those with a university education were more likely than those without to reside in Class 2 (adjusted residual = 2.3) and Class 3 (adjusted residual = 2.3), and less likely to be in Class 1 (adjusted residual = -3.7), χ2(2) = 14.46, p < .005.
4. Discussion
The results of the research reported here support the notion that there are multiple publics that differ in terms of their attitudes towards benefit sharing. Viewing our sample as a whole, the results suggest that both social responsibility and reciprocity influence attitudes towards benefit sharing. Equivocation about payment for participation and agreement with distribution of benefits suggest that the norm of social responsibility is influential. On the other hand, differences in attitudes relating to commercial and non-commercial and Australian and international users of biobank resources suggest that the norm of reciprocity also plays an important role.
The differences observed in this study between the three distinct publics identified are particularly clear with regard to payment to participants, but they are also reflected in responses to other questions in this survey. Evidence for the operation of two independent normative expectations was found, suggesting that while one section of the public (Class 1) would like to see biobanks operate predominantly in line with the norm of reciprocity (with the norm of social responsibility also appearing to exert some influence), another (Class 2) preferred to see benefits distributed according to the norm of social responsibility (with some influence from the norm of reciprocity), and a third (Class 3) expressed no clear preference. These results support the ideas of Dixon-Woods et al. (2008) that people expect medical research participants to be rewarded, yet they also support the notion propounded by Kettis-Lindblad et al. (2005) that contributions to medical research are, and should be, driven by altruistic motives or the desire to help those in need without the prospect of future reward. What our research adds to the existing literature is that the influence of these two norms appears to vary between different sectors of the public. We were able to identify a distinct and numerically dominant public who appeared to be primarily influenced by reciprocity (Class 1) and a public who appeared to be more influenced by social responsibility (Class 2) as well as a small minority (Class 3) who had possibly not yet formed firm views on their expectations with regard to biobanking and benefit sharing.
Norm of reciprocity
The largest “public” (Class 1) was found to primarily endorse the principle of reciprocity. Members of this class tended to expect biobank participants to be paid, especially if commercial interests were involved. They also agreed strongly that treatments developed from biobank resources should be made available to biobank participants (though not more so than for other Australians and those in developing countries), and that biobanks which provide their resources to other researchers should receive financial compensation, particularly if commercial and offshore interests are involved. Finally, this public also believed that outside organisations using biobank resources should give their research results to the biobank (and make them public). People in this group tended to be younger, less well-educated men who were likely to believe that biobank research will lead to better health care for themselves, and were highly likely to participate in biobank research. Their high levels of trust, willingness to participate and belief in the ability of biobanks to deliver health benefits (especially to themselves) provide further evidence for the operation of a reciprocity norm, given that it has previously been shown that reciprocal behaviour, particularly in the long term, is based on trust (Berg, Dickeout and McCabe, 1995) and that people tend to expect reciprocity from those who they believe are willing and capable of returning the good deed (Fehr and Gächter, 2000).
Taken together, the pattern of results for this largest group of respondents appears to support our expectations that a section of the Australian community expects benefits (both financial and health care) to be returned to those who provide their resources. The results further suggest that public expectations that affordable access to treatments will be provided to participants in return for free access to their resources are based first on beliefs that participation in biobanking will actually facilitate the development of effective treatments, and secondly on trust that these benefits will be returned to participants. If there is doubt relating to the credibility of the biobank or its ability to make future health care benefits available to the public, then individuals influenced by the reciprocity norm should be even more inclined to expect biobank participants and the biobank to be paid for their contributions. This goes some way to explaining the different attitudes observed in Class 1 between commercial and non-commercial biobank operators and users. It has consistently been found that trust is significantly lower in biotechnology research conducted by for-profit compared to public research organisations (Critchley and Nicol, 2009). Moreover, a significant reason for the reduction in trust is a belief that private organisations will reduce the affordability and accessibility of new health treatments arising from their research (Critchley, 2008). Thus, if the norm of reciprocity is in operation, people should favour payment for participation especially if the biobank is owned by a for-profit entity, or when a for-profit entity is allowed access to the biobank’s resources for research purposes. This is precisely the pattern of findings here, providing further support for the idea that, for a large section of the public, attitudes towards benefit sharing are driven, at least in part, by the norm of reciprocity. It should be pointed out, however, that not all of the findings were precisely in line with our expectations about the operation of the norm of reciprocity, particularly with regard to attitudes towards access to treatments.
The fact that Class 1 respondents were more likely than those in Class 2 to believe that biobanks would result in better health care treatments for themselves tends to suggest that self-interest may play a role in their attitudes. However, other evidence tends to point away from this conclusion. We posit that if the norm of reciprocity arises from self-interest, it should be particularly strong for those who are most likely to benefit from biobank research, such as those who have experience with a genetic condition, those who have children who may need treatment in the future, and perhaps older people who are more vulnerable to illness. Yet the results of this study show those who had experienced a genetic condition (themselves or their family or friends) were equally likely to be found in all classes. Also parents and older respondents were significantly less likely to occur in Class 1 suggesting that this form of self-interest (as well as parental interest in the welfare of offspring) may not be responsible for the influence exerted by the norm of reciprocity, at least in this sample. Instead, these results tend to concur with the notion of reciprocity arising from a fairness heuristic, that is, a strong desire for fairness or being seen as fair (Fetchenhauer and Dunning, 2009; Tyler, 1994). On this basis, reciprocal behaviour can be viewed as a desired end in itself as a fair method of distributing resources. Those sharing their resources (i.e., biobank participants and biobanks themselves) should receive something back (especially if their contribution is to be commercialised for profit) simply because it is considered the fair thing to do.
Norm of social responsibility
Fairness is also closely linked with the notion of social responsibility. People participate in biomedical research because it is the right and fair thing to do (Kettis-Lindblad et al., 2005). The major difference in views between the “reciprocity” group (Class 1) and the class who appear to be most influenced by the norm of social responsibility in this study (Class 2) relates to attitudes towards payment for participation. The highly negative views towards payment expressed by the “social responsibility” group appear to reflect the long-held assumption that people generally participate in biomedical research for purely altruistic reasons, because of the likely benefit that such research could bring to society as a whole. However, various commentators are starting to question whether it is reasonable for researchers to continue to expect altruism to be the driver for participation, particularly when there are commercial partners (Campbell, 2007; Laurie and Hunter, 2004).
In the increasingly commercialised research environment, some argue that free access to biomedical resources for research purposes in exchange for the promise of future health care developments is not enough and that participants should be paid a fair price for use of their material (for example, Bear, 2004). However, this view is not widely supported in the academic and policy literature. On the contrary, in addition to the potential for this to impact on the cost of doing biomedical research, there is concern that it could lead to coercion to participate (Irish Council for Bioethics, 2005: 62). Moreover, although some research participants are paid for their participation in biomedical research (for example, in some clinical trials), as a general rule payment is rarely considered to be a serious option, because of long-standing concerns about the commodification of human tissue (Andrews and Nelkin, 1998). However, given the views expressed by the majority “reciprocity” group in this study, it may be timely to revisit this debate about payment for participation.
Limitations
It should be noted that more empirical evidence is needed before we conclude that the majority of the Australian public expect biobank participants to be compensated for their contribution. This is the first study to specifically assess public expectations relating to benefit sharing, thus the measures used here need further testing in relation to their reliability and validity. While the low number of unsure responses and the generally expected relationships found between measures (and with previous research) hint that the measures were valid, the extent to which knowledge about biobanks may have influenced the results has not been tested. Biobanks and the issues surrounding them are relatively new in Australia and internationally, and as a consequence responses to questions about them may be influenced by a range of factors including the structure of survey questions. Future research should therefore also employ qualitative methods to obtain attitudes and expectations amongst members of the public who are not aware of biobanks or biomedical research.
Implications for benefit sharing
Despite its limitations, this research clearly illustrates that open dissemination of research results and broad access to treatments created using biobank resources are critical considerations for biobanks in establishing benefit sharing frameworks. Solving the payment conundrum will be more challenging, given the marked divergence of views between the “reciprocity” and “social responsibility” groups in this study, together with general lack of support for payment in the policy and academic literature. Given that attitudes in the “reciprocity” group are apparently influenced by the type of biobank and type of researchers accessing the biobank resources, ultimately each biobank will need to consider how to create appropriate benefit sharing arrangements, taking into account its own funding arrangements and the way it intends to provide access to other researchers.
One further matter that warrants attention is that this study revealed few obvious differences in responses between groups of respondents based on demographic characteristics, including involvement with a genetic condition and parenthood. This suggests that differences between biobanks and the populations from which they recruit (disease-specific or population-wide) should have little bearing on types of benefit sharing arrangement. It seems that group-specific attitudes should only bear on benefit sharing arrangements if recruitment is specifically targeted to young, less well-educated males (which seems unlikely). In such circumstances, views expressed by the “reciprocity” group should be given precedence. More generally, biobanks will need to consider the likelihood that they will be recruiting from two or more publics with fundamentally different views on some aspects of benefit sharing. This emphasises the complexities involved in dealing with benefit sharing, but it should not deter biobanks and policy makers from addressing this challenge.
Footnotes
Acknowledgements
This research was supported by Australian Research Council Discovery Project DP0559760. The authors would like to thank Professor Margaret Otlowski and Dr Mark Stranger for assistance with survey design and for constructive feedback on earlier drafts of this paper, the staff at the Swinburne University CATI facility for their efforts in conducting this survey, and all those participants who kindly gave their time to be interviewed. Thanks are also due to Gordana Bruce for assisting with data collection.
Notes
Author Biographies
Dianne Nicol is a Law Professor at the University of Tasmania and a Deputy Director of the Centre for Law and Genetics. The broad theme of her research is the regulation of biotechnology and human genetics, with particular interest in the commercialisation of genetic knowledge and patenting of genetic inventions as well as the specific regulatory issues associated with genetic, cloning and stem cell technology and biobanking.
Christine Critchley is a Social Psychologist and Senior Lecturer in the Department of Psychology at Swinburne University in Melbourne, Australia. Her research interests include public opinion, attitudes towards controversial scientific research and trust in scientific actors. She has designed and conducted eight Swinburne National Science and Technology Monitors (SNSTM), an annual national telephone survey designed to gauge public reaction to science and emerging technologies.