
Abstract
This study’s objective was to examine residents’ attitudes toward and factors associated with an ongoing, real genome cohort study based on a community in Japan. After the genome cohort study’s launch in 2007, in November and December 2009, a self-administered questionnaire survey was conducted with 2500 randomly sampled residents aged 30–74 years, living in Nagahama, Japan. Responses were received from 1363 people (response rate = 54.5%), of whom 187 respondents had already participated in the study. Although the local government and researchers disseminated information through leaflets and citizen-information papers to every household, sent notices by personalized letter, and held symposia and other meetings, 65.7% of males and 47.2% of females first became aware of the study when they received our questionnaire. Among all respondents, 81.2% of those who knew that the genome cohort study had begun and 68.6% of those who did not know had a positive attitude toward the study. Their attitudes were significantly associated with high health consciousness and the desire for an extensive health check-up. Although for males there were no particular negative aspects of the genome study, for females, positive aspects were associated with participating in community activities and desiring an extensive health check-up. Although promoting a community-based genome cohort study requires huge effort, it is essential to popularize it. Actions are vital both for monitoring public awareness and attitudes at a community level and for keeping communication channels open.
1. Introduction
After the completion of human genome sequencing in 2003, several large-scale biobanks for genome epidemiology were established to examine relationships between phenotypes and genotypes (Artene et al., 2013). Development of biobanks has shifted such studies from medical institutions to communities. Past genetic studies based on information from clinics mainly analyzed target single nucleotide polymorphisms (SNPs) to prevent, diagnose, and treat specific diseases for patients or individuals suspected of having a disease. In contrast, studies based on communities where participants’ genetic information is collected and stored, along with information on their lifestyle habits and medical histories, are premised on analyzing genes, as yet unrevealed, through genome-wide association studies of the healthy general public. Such data might be shared and used by many researchers around the world. Therefore, biobanks based on communities require further efforts for recruitment of the healthy public, informed consent, assurance of personal information remaining secure, and so on (Haga and Beskow, 2008; Kerath et al., 2013). In addition, individuals’ geographic origins to an accuracy of a few 100 kilometers can be uncovered, thanks to the recent enhancement of SNP databases (Novembre et al., 2008). This means that inherited characteristics not only of biobanks’ participants and their kin but also of neighbors might be inferred from data. Therefore, community-based biobanks have accountability for neighborhood residents.
In December 2005, the Kyoto University Graduate School of Medicine and the city of Nagahama, Shiga Prefecture, finalized an agreement on the development of a health promotion project: The Nagahama Zero (0)-ji Prevention Cohort Project (N0PCP) aimed to facilitate biomedical research, including genome epidemiology, and to promote the health of Nagahama residents. Following the pilot study in 2007, the complete study began in November 2008. Eventually, 10,084 citizens (14% of those eligible) participated in the N0PCP program.
For researchers, comprehending the public’s awareness of a study and their willingness to participate in it is important for efficient management of projects involving genetics and biobanks (Bates et al., 2005; Cunningham-Burley, 2006). Genetic studies based on biobanks depend on the general public volunteering to provide sensitive information on their genetics, lifestyle habits, and medical histories (Masui and Takada, 2003; Yonemoto, 2007). Two types of studies examine public awareness and attitudes about genome studies (Sterling et al., 2006). The first shows people a hypothetical scenario and inquires about their willingness to participate in such a study (Ikeda, 2008; Ishiyama et al., 2008; Kettis-Lindblad et al., 2006; Wang et al., 2001; Wong et al., 2004). The other type asks participants about their perceptions of genome studies added to real and common medical studies (McCarty et al., 2008; McQuillan et al., 2003; Matsui et al., 2005; Mezuk et al., 2008).
According to hypothetical studies, a relatively low rate, that is, 49% of respondents in a Singapore study (Wong et al., 2004), and a relatively high rate, that is, 86% of respondents in a Swedish study (Kettis-Lindblad et al., 2006), were willing to participate in a genetic study. The factors associated with positive attitudes toward genetic studies are awareness of their benefits (Ikeda, 2008; Ishiyama et al., 2008; Wong et al., 2004), knowledge of and interest in such studies (Ikeda, 2008; Ishiyama et al., 2008; Wang et al., 2001), trust in experts and the implementing agency (Kettis-Lindblad et al., 2006; Trindad et al., 2010), and altruism (Kettis-Lindblad et al., 2006; Trindad et al., 2010; Wong et al., 2004). However, Kerath et al. (2013) reported no association between awareness of genetic research’s importance and willingness to participate. According to Etchegary et al. (2010), participants tended to have critical attitudes toward certain aspects of genetic testing and the use of genetic information. Arguments about public willingness to participate in genome studies and their associated factors are not without complications.
According to reports from add-on genome studies, more than 80% of participants in each study revealed positive willingness toward the study. With regard to demographic factors associated with willingness to participate in genetic studies, a study by McQuillan et al. (2003) suggested that females and black participants were less likely to consent to genetic research. In contrast, a study by Mezuk et al. (2008) suggested that age, but not race, gender, or education, was associated with consent to genetic testing. Additionally, race, but not age, gender, or education, was associated with consent to storage of biological samples. It seems that no concrete evidence exists about willingness to participate in genome studies and associated factors in add-on genome studies.
As indicated above, willingness to participate in genome studies and their associated factors depend on regional characteristics and contexts. Moreover, very few reports exist on general residents’ attitudes about ongoing studies in their own communities. Therefore, we investigated general residents’ awareness and attitudes in a community where a genome cohort study was in progress and determined the factors that influence their opinions. Our goal was to collect and provide information for constructing sustainable relationships among the community, residents, local government, and researchers to pursue a desirable community-based genome cohort study.
2. Method
Background
The N0PCP was organized by two boards: The Project Design Board consisted of 19 members who were Nagahama City staff members and Kyoto University researchers, and the Making the Nagahama Rule Board consisted of 15 members who were Nagahama city staff members, Kyoto University researchers, bioethicists, lawyers, and citizens selected from among applicants. Each board held 15 meetings over 2 years. The Project Design Board considered creating the project with (1) both a severe protection of individual information and usable data for researchers; (2) concise, to-the-point test items; and (3) friendships among citizens and researchers. Making the Nagahama Rule Board legislated the first ordinance, the “Nagahama Rule,” about the community-based genome cohort study in Japan. Their mission was to prioritize citizens’ dignity.
Outreach and recruitment activities
Kyoto University researchers held 13 lecture meetings on contemporary medical issues, such as genomes, lifestyle-related diseases, sleep disorders, information disclosure, and hospital evaluation for residents or high school students, including five symposia and five “science café” talks from November 2006 to November 2009. For recruitment, the Nagahama City Health Promotion section leafleted all houses through residents’ associations and placed reports in Nagahama public information sites and newspapers. All males and females in their 30s and subjects aged 40–74 years in the national health check-up program in Japan were notified by personalized mail.
Participants and setting
This study was conducted as part of the health/lifestyle survey of the Nagahama City Health Promotion section, to examine the health consciousness of Nagahama’s residents and to provide effective health services. Data were collected using an anonymous self-administered postal questionnaire. Of the 2500 subjects in the 30–74 years age bracket, selected by random sampling from the basic Resident Resister in compliance with local regulations, 1900 received mailed surveys. Responses from 600 subjects were collected by community health promoters who received municipality-organized training in November and December 2009.
The study protocol was approved by the Kyoto University Graduate School and Faculty of Medicine Ethics Committee.
Measures
The study’s questionnaire was developed on the basis of a preliminary survey conducted during the N0PCP (Tomoda, 2008) and the nationwide survey on public attitudes toward genetic studies in Japan (Ishiyama et al., 2008). Revisions were made according to advice from public health researchers and staff members of the Nagahama City Health Promotion section.
Survey items included the following. For “Awareness of the N0PCP,” participants were asked whether they were aware of the N0PCP before the survey, and if so, their source of information. For “Attitude toward the N0PCP,” participants were asked about its favorable and the unfavorable aspects. Multiple answers were allowed (see online Appendix at http://pus.sagepub.com). For “Willingness to participate in the N0PCP,” participants were asked whether they had participated in the N0PCP, and if not, whether they wanted to participate in the future. Furthermore, those who had already participated and who wanted to participate were asked about their positive reasons for such willingness. Those who did not intend to participate in the N0PCP were asked about their respective reasons. Multiple answers were allowed (see online Appendix). For “Understanding the N0PCP,” we asked subjects whether they knew about five aspects of the N0PCP (see online Appendix). In addition to survey items, participants were asked to provide their socio-demographic characteristics (age, gender, and employment status) and other factors (participation in community activities, health consciousness, and self-rated health).
Analyses
Chi-square tests were used to examine associations between items. Logistic regression analyses were used to identify factors associated with attitudes toward the N0PCP.
3. Results
Respondents’ characteristics
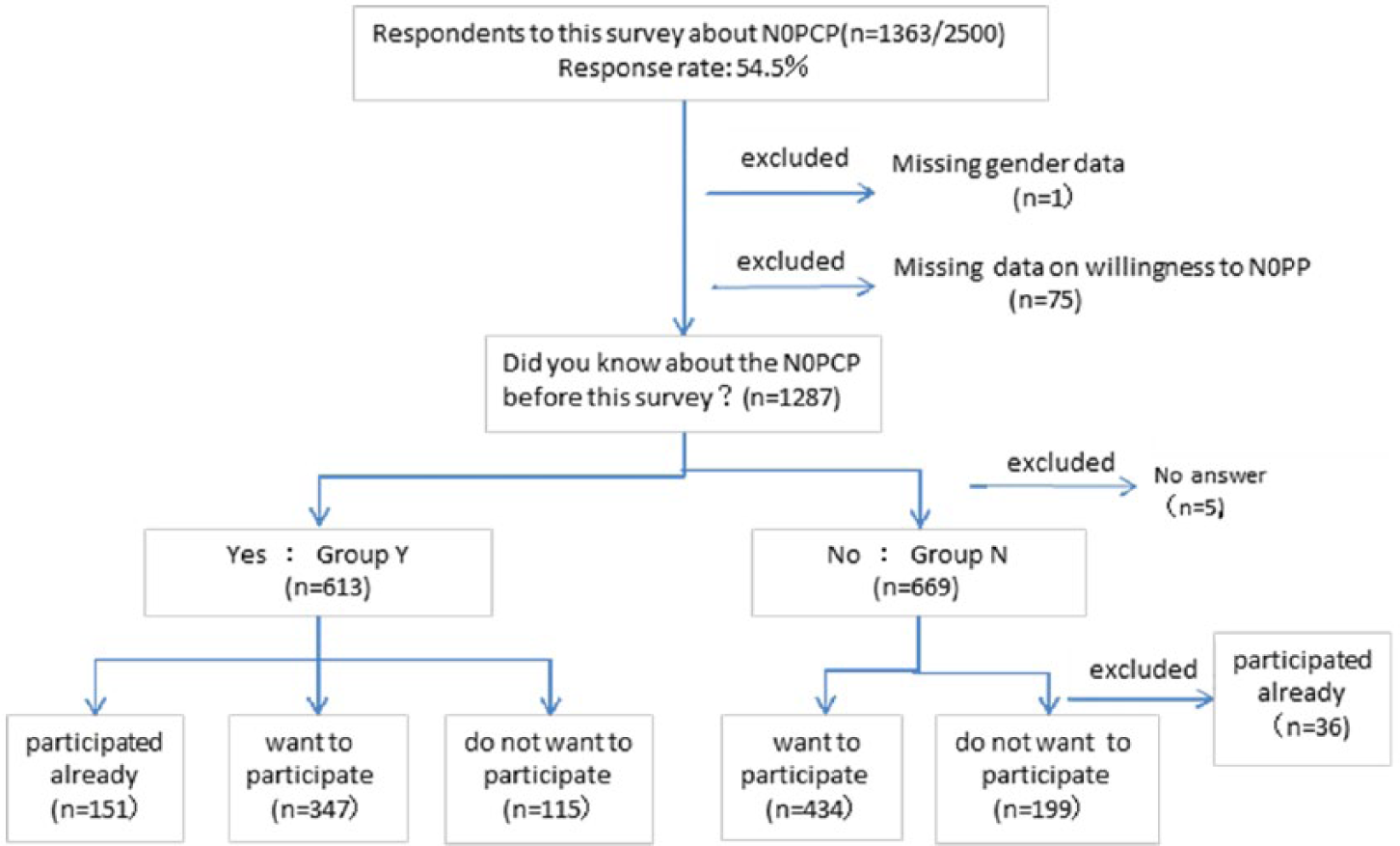
Of the 2500 questionnaires distributed, 1363 were returned (54.5% response rate), 47.4% (595/1254) for males and 61.6% (767/1246) for females. One person of unknown gender was excluded from later analyses. For all respondents, demographic and other individual factors (i.e. intention to participate in the N0PCP, awareness of the project, participation in community activities, health consciousness, and self-rated health) are presented in Table 1. Overall, males (especially in their 30s) were underrepresented (14.0%), whereas those in their 60s were overrepresented (33.6%). Of the 1362 respondents, 75 who gave no answer regarding their intention to participate in the N0PCP and 5 who gave no answer regarding awareness of the N0PCP were excluded from analysis. The remaining respondents were divided into 613 who knew about the N0PCP (group Y) and 669 who did not know about the N0PCP before the survey (group N). These groups were analyzed separately because for group N, this survey is hypothetical. Furthermore, 36 who did not know about the N0PCP before the present survey, in spite of having previously participated in the study, were excluded from analyses (Figure 1).
Demographic and other factors that affect attitudes toward Nagahama Zero (0)-ji Prevention Cohort Project (N0PCP).
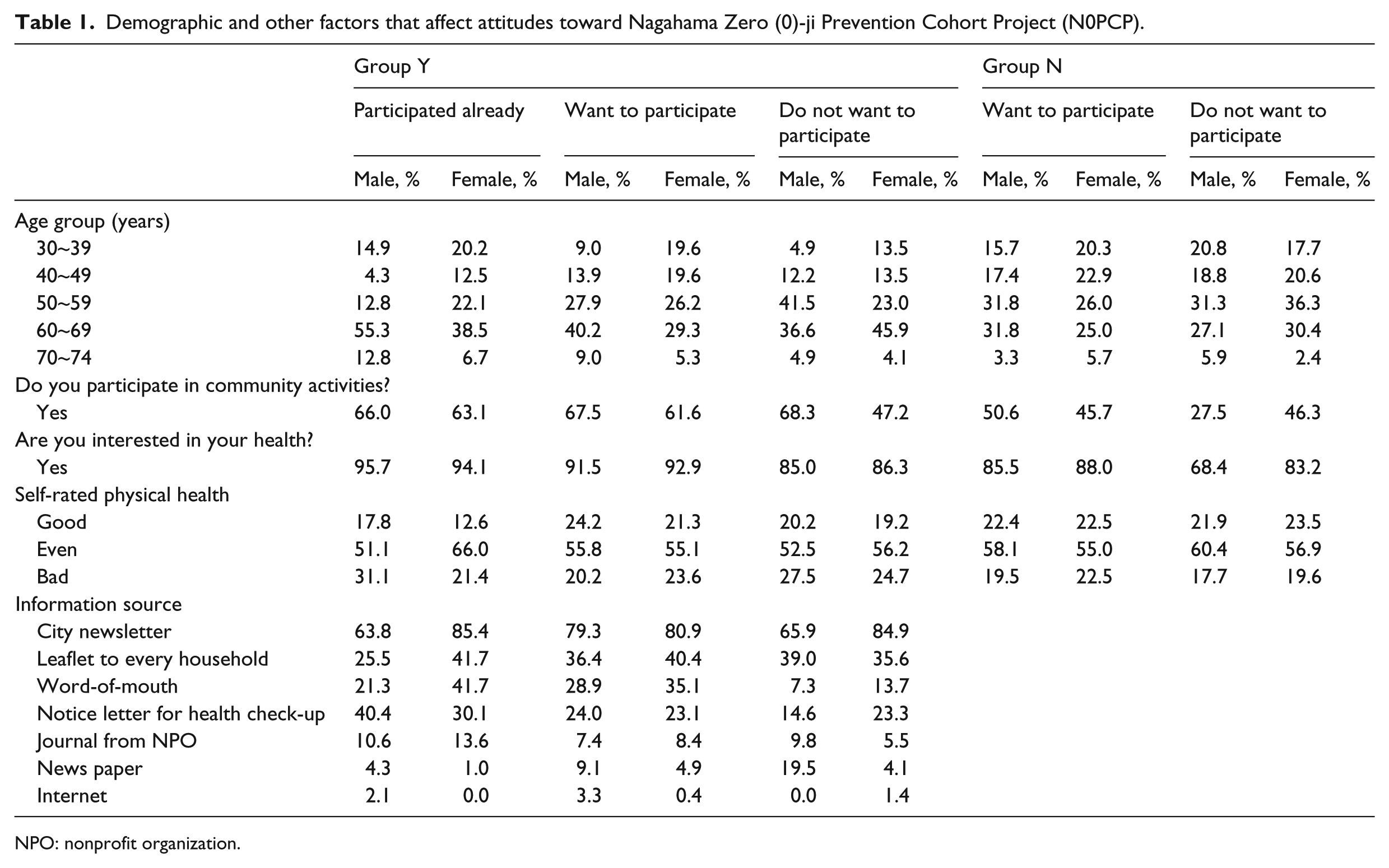
NPO: nonprofit organization.
Attitudes toward the Nagahama Zero (0)-ji Prevention Cohort Project (N0PCP) of respondents.
Awareness of the N0PCP
Overall, 34.3% of males and 52.8% of females were aware of the N0PCP, with females being significantly more aware than males (p < .001). For both males and females, the most common means of obtaining information about the N0PCP was “city newsletters” (79.5%), followed sequentially by “leaflets to every household” (38.0%) and “word of mouth” (29.5%). Females acquired information by “city newsletters” and “word of mouth” significantly more than males (p = .002, p = .001, respectively). More elderly people than younger people took advantage of “leaflets to every household” and “personalized notice letter.”
In group Y, 24.6% had already participated in the N0PCP, 55.6% wanted to participate, and 18.7% did not want to participate. In group N, 68.6% wanted to participate, and 31.4% did not want to participate. No significant differences were observed between males and females. Older males had a more positive attitude than younger males (p = .035), while females showed no age differences. Those in group Y had more a positive attitude toward participating in the N0PCP than those in group N (p < .001). Both males and females who had already participated and wanted to participate in the N0PCP were more health conscious than those who did not want to participate. Females who participated in two or more community activities were more positive about participating in the N0PCP.
As for self-rated health, no significant difference was revealed between those who had positive attitudes toward the N0PCP and their counterparts.
Attitudes toward the N0PCP
Regarding attitudes toward the project, the most common positive aspect in group Y was “free and extensive health check-up program,” including 71.9% of those who had positive attitudes toward the N0PCP (i.e. those who had already participated and wanted to participate in the project) and 29.7% who did not want to participate in the N0PCP, and in group N, 49.9% of those who wanted to participate in the N0PCP and 18.4% of their counterparts (followed by same sequence in parentheses). These results were followed sequentially by “long-term follow-up” (62.2%, 31.5%, 39.8%, 17.9%, respectively) and “helpful for medical development” (47.0%, 18.4%, 24.7%, 15.3%, respectively). Of the group Y males who did not want to participate in the N0PCP, 36.6% responded “nothing”; in group N, 27.3% responded “I don’t know.”
The most common negative aspect was “nothing,” followed sequentially by “privacy concerns are raised” (13.9%, 19.1%, 11.3%, 10.3%, respectively) and “unexpected negative effects might arise” (9.2%, 9.5%, 8.1%, 5.4%, respectively). The three most common positive aspects were significantly associated with both males’ and females’ positive willingness to participate in the N0PCP, whereas for both males and females, “privacy concerns are raised” and “unexpected negative effects might arise” were not significantly associated with willingness to participate in the N0PCP.
Logistic regression analyses were performed to investigate factors associated with willingness to participate. Those who had positive willingness to participate in the N0PCP (i.e. those who had already participated and wanted to participate) and those who did not to want to participate were dichotomized. According to the results presented in Table 2, significant differences between males who had positive attitudes about participating in the N0PCP and their counterparts were observed regarding “health consciousness” and “free and extensive health check-up.” Significant differences between females who had positive attitudes about participating in the N0PCP and their counterparts were observed regarding “participating in two or more community activities,” “free and extensive health check-up,” “questionnaire about lifestyle,” and “awareness of the N0PCP.”
Relationship between the willingness to participate to the N0PCP and the background factors.
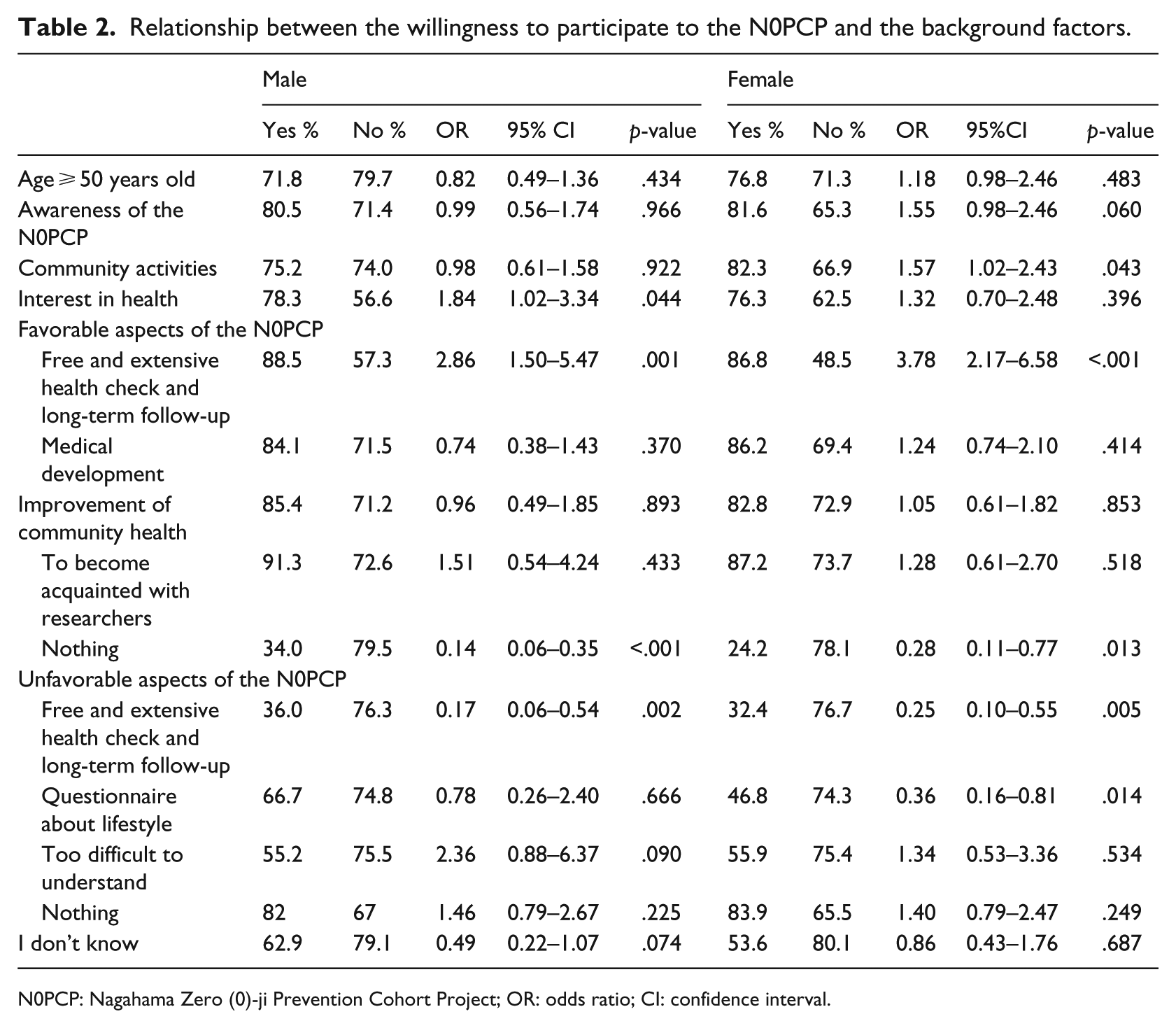
N0PCP: Nagahama Zero (0)-ji Prevention Cohort Project; OR: odds ratio; CI: confidence interval.
Willingness to participate in the N0PCP and reasons for positive or negative attitudes toward such participation
In group Y, the most common reason for positive willingness to participate in the N0PCP was “extensive health check-up” (71.5%), followed sequentially by “health consciousness” (59.4%), and “free” (55.7%) (Table 3). Significant differences between those who had already participated and those who wanted to participate in the N0PCP were observed in regard to “health consciousness,” “inducement from family members and acquaintances,” and “no other health check-up opportunity.”
Reasons of positive willingness toward participating to the N0PCP.
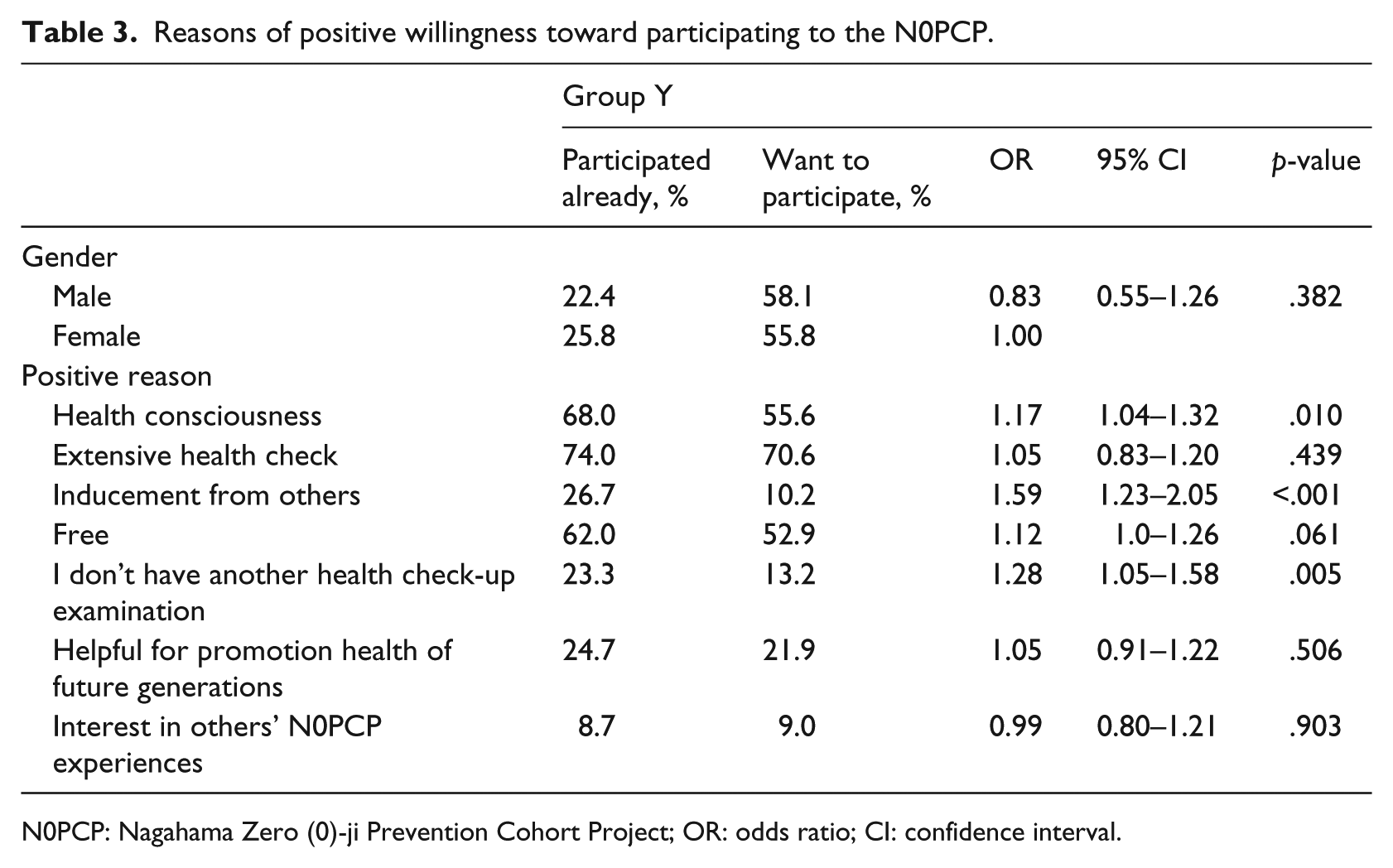
N0PCP: Nagahama Zero (0)-ji Prevention Cohort Project; OR: odds ratio; CI: confidence interval.
The most common reason for group Y’s unwillingness to participate in the project was “other” (36.9%); this might reflect the free descriptions saying that most respondents had other health check-up programs, followed sequentially by “busy” (29.8%), and “fear of negative results of the check-up” (19.0%). In group N, the most common reason for unwillingness to participate was “unawareness of the N0PCP” (28.5%), followed sequentially by “busy” (24.3%), and “I don’t know how to participate in the project” (22.2%).
Understanding the N0PCP
When we asked respondents whether they knew about the five aspects of the N0PCP (the extensive health check-up, the questionnaire survey about lifestyle, the 10-year follow-up study, genetic tests, and the terminology “genome cohort study”) among subjects who had already participated in the N0PCP, 34.7% knew about all five items, and 8.8% knew nothing. Of those who wanted to participate, 10.5% knew about all five items, and 10.2% knew nothing. For subjects who did not want to participate, 7.5% knew about all five items, and 16.8% knew nothing. The most common answer was given for “extensive health check-up.” The rates for knowledge about the item concerning genetic tests were 51.7% in those who had already participated in the N0PCP, 26.5% in those who wanted to participate, and 15.9% in those who did not want to participate.
4. Discussion
The survey of Nagahama residents reported here was administered during performance of a genome cohort study in the area. These results provide insight into approaches for future recruitment and informational activities. The response rate of 54.5% was approximately the same as that in the nationwide survey on attitudes toward genome studies (Ishiyama et al., 2008), but there were fewer answers from males in their 30s and 40s.
For half of the 3-year N0PCP period, the local government and researchers disseminated information through leaflets and citizen-information papers to every household in Nagahama, sent notices by personalized letter, and held symposia and other meetings. However, 65.7% of males and 47.2% of females became aware of the N0PCP only after receiving the present survey. Actually, many more people might not have known about the N0PCP since the rate of participation in the N0PCP, as reported in this survey, was higher than the actual rate of participation in the N0PCP at the end of December 2009 (the same period as this survey). In group Y, 80.5% of males and 81.6% of females had positive willingness to participate in the project, whereas in group N, 71.4% of males and 65.3% of females had positive willingness to participate. In the nationwide hypothetical survey in Japan (Ishiyama et al., 2008), 73.8% of males and 65.6% of females approved the promotion of genomic studies. Males had more positive attitudes toward genetic studies; this supported our result from those who first became aware of the N0PCP through this study. In Singapore (Wong et al., 2004) and in Sweden (Kettis-Lindblad et al., 2006), in investigations about willingness to participate in genetic tests, the most common reason for a positive attitude was “I want to help a future patient.” Background factors associated with a positive attitude toward participation were having a family member or close friend with a hereditary disease (Kettis-Lindblad et al., 2006; Wang et al., 2001) or having accurate knowledge about heredity (Ishiyama et al., 2008). From these results, the researchers tended to appeal to the necessity of educational dissemination. Clearly, however, notification about the genome cohort study is key for participation in a real community-based study. That should be the first consideration for researchers finding channels to reach even residents who are not aware of leaflets to every household and personalized mail from local sources and researchers, especially for males in their 30s and 40s. Inducement from others might lower females’ barriers for participating in genome studies. Researchers should also find channels to reach females who are not involved in community activities.
Several reports show that medical study participants do not read manuals and consent forms (Matsui et al., 2007; Nakayama et al., 1999; Wise, 1996). This tendency was monitored in the N0PCP. Generally, the public knew that the N0PCP was a free, extensive health check-up, rather than a medical study. This might be why people interested in health were more likely to participate, whereas those who were too busy or had access to other health check-ups were reluctant to participate. In a preliminary survey (Tomoda, 2008), 78.9% of subjects gained knowledge of the N0PCP’s contents for the first time by using the survey manual. The most common reason for willingness to participate was to contribute to future generations’ health. Unwillingness to participate was mainly based on concerns about unforeseen disadvantages. However, in the current survey, more people who had participated in the N0PCP indicated that information from a family member, friend, or acquaintance was a decisive factor in participation. This might imply that the N0PCP being an advantageous health check-up, not a medical study, spread through word of mouth. In contrast, a genetic test becoming a topic of everyday conversation is unlikely.
Regarding understanding of the N0PCP’s contents, more people knew about the health check-up and lifestyle questionnaire, but fewer knew about the medical study component with genetic tests. In the pilot N0PCP study, all applicants were required to participate in a briefing session ahead of time. However, applicants were negative about this time-consuming process. Participation in the briefing session became arbitrary, and most applicants read eight pages of a manual at home before participation and received individual explanations from researchers on the health check-up day if they had questions. According to the qualitative study by McCarty et al. (2008), residents who were eligible, but did not participate in the community-based biobank, thought that too much information had been provided to understand and enroll in the study. Sturgis et al. (2010) investigated the effect on public attitudes of providing information about genome science through short films. They found no significant difference in knowledge and interest in genomics between respondents who viewed the films and those with no information. They also found that providing information caused study dropout among less-educated subjects. Matsui et al. (2007) examined effects on participant understanding and participation rate of obtaining informed consent in different ways (i.e. a routine approach and a more intense approach) in a genetic cohort. They clarified that those in the routine group who obtained less information rated their understanding of research higher than those in the intense group. A high level of self-rated understanding caused a high participation rate. A complicated process can reduce consent to participate and undermine a study’s power (Murphy et al., 2009). As McCarty et al. (2008) suggested, researchers and policy-makers should make the process easy to understand and less time-consuming for participants. Our study clarified that there would be considerable difficulty in doing so.
The inducement of a health check-up may be advantageous for encouraging participation. Wong et al. (2004) found that the absence of benefits for donors obstructs recruitment into a genome study and suggested the offer of a free medical examination as an incentive. Our results supported this finding. Some investigations using hypothetical situations have been performed on the basis of monetary compensation for medical study participation (Bentley and Thacker, 2004; Cryder et al., 2010); however, we were unable to find a study linking an extensive health check-up with medical study participation. Grady (2005) suggested that increased participation of low-income people owing to monetary compensation has not been proven. Participants in the N0PCP were more interested in health than others and participated more in community activities. One goal of the N0PCP is promotion of all Nagahama residents’ health, not just that of N0PCP subjects. Thus, exploration of ways to reduce health status disparity between health-conscious participants and nonparticipants is required.
This survey clarified three issues. First, there were several large groups of people not reached by messages from local sources and researchers. The obstacles to information transfer might arise not only from time (e.g. busy) or place (e.g. far) but might also be psychological (National Cancer Institute, 1989). Some citizens might discard a notice from the Nagahama City Health Promotion section without examining it. We are exploring settings in which such people might be more attentive and open-minded (National Cancer Institute). Miyamoto et al. (2014) investigated the social network of the nonprofit organization (NPO) driven by the N0PCP. Results suggested that health communication through individual connections is more effective than through community associations. Arranging grassroots networks might enhance both citizens’ health and project quality, which are the N0PCP’s goals.
Second, in a community study, once the general public accepts information, that information takes on a life of its own. In other words, the information does not have to come from an official source, but it does require public acceptance. Bates et al. (2005) suggested, “There is not a direct relationship among having information, understanding, and accepting genetic science.” Our findings suggest that “genome cohort study” is difficult to grasp, but that an “advantageous health check-up program” is easy to grasp. A hypothetical investigation in Japan concluded that people with high genome literacy were positive about participation in a genome study. This indicates a path from public understanding to public acceptance and emphasizes the importance of genome education to promote study participation. For a study in progress, reversing the pattern from acceptance to understanding might be possible. Moreover, for people to create a culture of talking to each other, according to their contexts, about genome and medical research is desirable.
In the case of the N0PCP, researchers organized science cafés, workshops, and lectures to try to improve knowledge and interest. Furthermore, an NPO executed the Health Festival and, there, attempted to deliver the Genome Map (Kano, 2008). Researchers, residents, and policy-makers should explore the process of communicating that which is difficult to communicate.
Finally, in a community-based study, notices not to exclude nonparticipants are necessary. Subjects with an interest in health were positive about the N0PCP, but the effect of the N0PCP causing health disparities and division between participants and nonparticipants would be negative. To obtain support from participants and nonparticipants, it is important that the N0PCP takes root in the community and continues for a prolonged period.
Our study has several limitations. First, Nagahama is an ancestral town for many citizens, and their strong social bonds might have impacted outcomes. Specifically, information from familiar persons could stimulate participation in a genome cohort study. This might not be directly applicable to communities with poor interpersonal relations or those with high respect for self-reliance. Second, this study in itself might have become a N0PCP public relations tool and influenced respondents’ intention to participate. Third, our data indicated that Nagahama residents recognized the N0PCP more as a reasonable health check-up program than as a medical study involving genome-wide analyses; therefore, public awareness and willingness to participate in a genome cohort study might not have been entirely clear.
5. Conclusion
Our results showed that researchers might have difficulty sharing information with the public in order for them to accept a community-based genome cohort study. This suggests that activities of citizen volunteers are important (Lasker and Weiss, 2003). We believe that the N0PCP will advance community-based medical projects in Japan not only by contributing to medical developments but also by promoting public health in a community of cooperation among the public, local government, and academia. During a long cohort study period, monitoring public awareness and attitudes at the community level and maintaining open channels of communication are both vital.
Footnotes
Acknowledgements
We would like to thank the citizens of Nagahama and the Nagahama City Health Promotion section for their cooperation in this research. We are very grateful to anonymous reviewers for detailed comments on the original manuscript.
Funding
This project was supported in part by the “Nagahama Regional Open Genome Epidemiology Study” of Research Institute of Science and Technology for Society (RISTEX) in the Japan Science and Technology Agency.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.