
Abstract
As brain-computer interfaces are promoted as assistive devices, some researchers worry that this promise to “restore” individuals worsens stigma toward disabled people and fosters unrealistic expectations. In three web-based survey experiments with vignettes, we tested how refusing a brain-computer interface in the context of disability affects cognitive (blame), emotional (anger), and behavioral (coercion) stigmatizing attitudes (Experiment 1, N = 222) and whether the effect of a refusal is affected by the level of brain-computer interface functioning (Experiment 2, N = 620) or the risk of malfunctioning (Experiment 3, N = 620). We found that refusing a brain-computer interface increased blame and anger, while brain-computer interface functioning did change the effect of a refusal. Higher risks of device malfunctioning partially reduced stigmatizing attitudes and moderated the effect of refusal. This suggests that information about disabled people who refuse a technology can increase stigma toward them. This finding has serious implications for brain-computer interface regulation, media coverage, and the prevention of ableism.
1. Introduction
Brain-computer interface development, societal responsibilities, and the problem of stigma
Brain-computer interfaces (BCIs) convert brain activity into output signals to help users control external devices in real time. This new capability has inspired a range of applications, including controlling one’s movement via a wheelchair or smart prostheses (e.g. grabbing something with a prosthetic hand) and communicating by moving a computer cursor or typing on a digital keyboard, all by using one’s thoughts. Although they are represented symbolically in transhuman imaginaries (Jasanoff, 2016), BCIs are already being developed in experimental laboratory and clinical contexts. Researchers in a range of fields, from biomedical engineering to neuroethics, have promoted these devices as helping persons with motor or communicative impairments regain some autonomy (Glannon, 2014) and participate in social life. For instance, BCI developers have justified their work as a response to “personal, social, and economic burdens of [user] disabilities” (Wolpaw et al., 2002: 768), or as “restorative” and “assistive” (Soekadar et al., 2011). Such effects may be seen as ways to reduce the stigma of disability; by making the user appear less burdened, more independent, or “restored” to some previous state, the BCI may thus reduce factors previously associated with stigmatizing attitudes.
This narrative of restoration has significant public support, especially as compared with support for the idea of enhancement. One tri-national survey suggests that healthcare and assistive applications are the most exciting use of the technology (Sample et al., 2019b), a sentiment also present among rehabilitation professionals, who would be responsible for assistive BCI implementation (Boehlen and Sample, 2020; Sample et al., 2022). Disabled people, 1 too, have expressed hopes for increased mobility, interaction, and communication through BCI technology (Kögel et al., 2019, 2020). Studies of an analogous technology, brain stimulation devices, suggest that the public judges such applications more favorably compared with those that might enhance cognitive function (Medaglia et al., 2019; Sattler and Pietralla, 2022). Still, other studies indicate that the use of certain performance enhancing biotechnologies (such as pharmaceuticals) is sometimes seen as legitimate for particular high-stakes professions, like physicians or military personnel (Franke et al., 2012a, 2012b), despite raising questions about autonomy (Annas and Annas, 2009; Sattler et al., 2022). These examples demonstrate the complex narratives and concerns surrounding the purpose and use of neuro- and biotechnologies.
Despite ostensibly positive framing, assistive BCIs are not always met with enthusiasm. Researchers in bioethics, (dis)ability studies, and science and technology studies (STS) have expressed serious worry that the devices, when promoted as “restorative,” will actually worsen stigmatization and undermine personhood (Sample et al., 2019a). Aas and Wasserman (2016: 40), for example, suggest that the rhetoric used to promote BCIs will further stigmatize disabled users as “trapped in their own bodies” and in need of augmentation. This link between identity and device has been discussed with reference to cochlear implants and their rejection by some Deaf communities as a threat to their way of life (Sparrow, 2005). Wolbring and Diep (2016), similarly, note that “patients” are the most frequently cited beneficiaries of neural technology, implying the need for treatment; they observe that, problematically, this rhetoric may conflict with the way some disabled people understand themselves (i.e. as healthy and not at all ill), creating unfair “ability expectations.” This possibility motivates the present study, as the stigma linked to expectations is associated with harmful effects on individuals, setting the terms of their participation in society (Puumalainen, 2011) and restricting or excluding individuals who fail to meet that standard.
In this way, the impact of BCI discourse in society may corroborate a high-level theoretical finding from STS; technological objects and their associated discourses have political implications (Jasanoff, 2004; Winner, 1980), shaping the rights and responsibilities of individuals. Assistive technologies are likely no exception, having been both promoted as enabling disabled people to work (e.g. Strobel and McDonough, 2003) and recognized as the center of legal conflicts over ableism in the workplace (e.g. Sussman, 2007). In general, the STS literature already establishes that the growth of research in neuroscience and biomedicine has been influential in shaping the individual’s role in society, creating new means and obligations for individuals to remain independent and productive (Pitts-Taylor, 2010; Rose, 2007; Vidal and Ortega, 2017). But this critical scholarship has seldom been applied to BCI technology or the communication of its societal promise, and never in terms of the underlying social psychological mechanisms.
Investigating stigma toward BCI refusal through attribution theory
Theoretical statements in STS are rarely examined experimentally, in part because few of the contributing disciplines rely on causal or correlational models to report their findings. In this case, however, the central ethical concern that promoting assistive BCIs will exacerbate disability stigma and ableism constitutes a significant opportunity to integrate disconnected qualitative and quantitative perspectives. Here, the common element across these literatures is the importance of responsibility judgments. The historical, conceptual, and qualitative research cited above posits that, as the idea of an assistive BCI spreads, individuals and especially disabled people will be subjected to new responsibilities—“ability expectations” in the words of Wolbring and Diep (2016)—and thus new forms of ableist stigma when those responsibilities are not fulfilled. This argument implicates an extensive literature on the social psychology of stigma (Corrigan and Wassel, 2008; Goffman, 1963; Link and Phelan, 2001; Major and O’Brien, 2005), which has not been applied to the specific case of BCIs. While several causal factors have been identified for stigmatization (Jones et al., 1984), Attribution Theory is well-suited for investigating the above concerns about BCIs, as it emphasizes the role of responsibility judgments (Weiner et al., 1988).
Quantitative studies drawing on Attribution Theory typically measure judgments of responsibility for a negative achievement or event (e.g. failing a test) and examine their effects on stigmatizing attitudes (see, for example, Weiner et al., 1988). Notably, based on Attribution Theory, Corrigan et al. (2003) have proposed an informative social psychological model of the stigma of mental illness by focusing on two factors: controllability and dangerousness. This model explains the causes of stigmatization in terms of signals and signaling events that affect stereotyping cognitions (such as dangerousness or responsibility) that are followed by negative emotions (such as anger) and discriminating behavior (such as coercion) (e.g. Corrigan, 2006; Weiner, 1993). These signals and signaling events can be obvious or hidden marks of the person (Corrigan and Wassel, 2008). They include (1) causes of being in a certain condition (here disability) and the control a person has over those causes (e.g. negligent behavior), (2) causes for remaining in the current state in terms of perceptions of a lack of effort or ability of the person to “overcome” this state (e.g. refusing assistive technology), and (3) outcomes of the condition (e.g. perceptions about being dangerous to others).
With this model in mind, it can be hypothesized that refusing a technology that counteracts limitations associated with disability will increase stigma. This stigmatization would consist of blaming the disabled person for not improving their own condition. Thus, the use and refusal of a BCI can be also perceived as an indicator of the willingness (or lack thereof) to gain control over the disability and take responsibility for its effects. However, it remains an open question whether the use or refusal of a BCI is indeed associated with stigmatization. Neither is it known how stigmatizing attitudes would be affected by the level of functioning afforded by BCIs or their documented limitations, such as high error rate (Fenton and Alpert, 2008) and inability of some people to use them effectively (inappropriately labeled as “BCI illiteracy”) (Thompson, 2019). These different conditions can be seen as signals for the control the person might gain or lose over their current state when using a BCI or not. Given how much hope and enthusiasm is associated with BCIs—as evidenced in unrealistic public discourse about them (Gilbert et al., 2019; Purcell-Davis, 2013)—this is an important and timely issue.
The present study
Using a factorial vignette method (see below), we examine the effect of BCI technology refusal on the endorsement of stigmatizing attitudes toward disabled people when interacting with others (customers) in a work context. Experiment 1 explores whether refusing to use a BCI evokes stigma. Experiment 2 tests whether such stigmatization is modulated if the BCI technology has limited, moderate, or high device functionality. Finally, Experiment 3 examines whether such stigma is lower if the BCI has a higher malfunctioning risk and therefore its refusal would be seen as justified, while on the contrary, its use could be attributed to reckless behavior. This third experiment also extends the test to another context, that is, a higher stakes situation with more severe practical consequences for the customer. In this way, the present study reports the ways in which being informed about the use or nonuse of an assistive BCI technology and its usefulness (i.e. the level of functioning and malfunctioning risk) causes respondents to stigmatize (or not) BCI refusers who are disabled, either in the form of negative cognitive (e.g. blaming them for their refusal), emotional (e.g. feeling anger toward them), or behavioral (e.g. being willing to coerce them to use BCIs) responses toward the (non)users. By examining these processes, this study provides a social psychological perspective on both ableism and the STS insight that technology and social order are interdependent.
2. Experiment 1
To date, no experimental research has examined how decisions of disabled people are judged if they use or refuse a BCI. Concurrently, more assistive and human enhancement technology (including prosthetics, BCIs, and others) enters the workplace with the hope that it improves interactions between and within the group of customers and employees, while its influence on customer–employee interactions has been hardly researched (Grewal et al., 2020). In this study, a fictitious cashier is presented in a hypothetical work scenario centering on an inaccessible workspace. In the scenario, the cashier cannot use the register touchscreen because of his partial paralysis and considers the use of an assistive BCI as an alternative control mode, potentially improving his workplace performance and interactions with customers (see Figure 1 for full scenario text). Given this additional function gained by the user, we expect that the cashier deciding to use the BCI signals effort to offset the effects of disability. The cashier might also be perceived as having greater control over the disability and creating benefits for others. Refusing the BCI, accordingly, is predicted to trigger greater stigma (H1Resigning benefits). This experiment thus tests whether individuals view disability as something that can be controlled with a BCI and, consequently, will blame the disabled person for their decision to refuse an assistive device and react with anger and endorse coercive responses.

Cashier vignettes of Experiments 1–3 with the respective outcome measures.
Method
Participants
We recruited 336 participants in the United States through Amazon Mechanical Turk (AMT). AMT is a web-based platform with a large pool of possible participants who are paid for completing small tasks. AMT provides more demographically diverse samples than standard Internet samples and American college samples (Buhrmester et al., 2011; Clifford et al., 2015). Respondents were asked to provide their consent after being informed about the study purpose, duration, voluntariness, anonymity, and data usage. Consent was provided by 324 (96.4%) respondents. To increase data quality, we used an attention check as an ex-ante detection method to exclude possible bots and speeders, as well as to provide a motivational influence (Shamon and Berning, 2020). Therefore, a question ostensibly asked if the respondent was using a desktop computer, the detailed instructions directed the respondent to ignore the question and instead type the word “serious” (Sample et al., 2019b). A total of 267 (82.4%) passed this check. We used the data of 222 (83.1%) respondents, who consented, passed the check, completed the survey, and had no missing responses. Completers received a small cash compensation depending on current AMT provider rates. Of the analytical sample, 66.7% identified as men, and the average age was 36.77 years (standard deviation (SD), 10.58). This and the following two experiments were approved by the research ethics committee of the Institut de recherches cliniques de Montréal (Approval No. 2018-904).
Experimental design
To test our hypothesis, we used a factorial survey experiment. Such experiments bring together the advantages of experiments (as they provide high internal validity and non-multicollinearity due to the orthogonal design of the manipulated factors) and traditional surveys (which aim for external validity by using a heterogeneous sample of participants) (Atzmüller and Steiner, 2010; Auspurg and Hinz, 2015). In such experiments, respondents are provided with short hypothetical scenarios, so-called vignettes that are experimentally varied. Vignette designs are useful when it is difficult to directly observe the investigated behavior or attitude and when it is impossible or ethically challenging to create experimental conditions in the real world (Graeff et al., 2014). They have the further advantages of offering high levels of response consistency in acceptable survey time (Sauer et al., 2011) and examining sensitive topics (such as stigmatizing attitudes) in a controlled way (Aguinis and Bradley, 2014).
Respondents read a narrative that was designed to familiarize them with the idea of using a BCI in a social context, written not for maximum technical accuracy but in a form they might encounter in actual social discourse, including some of the simplifications, imprecise language, and frequently unfair framing used therein (Figure 1 for the full vignette wording). Using simple language emulating real-world cases and representations of BCI devices in popular media, the vignette describes a disabled person who sometimes has difficulty at an inaccessible workplace and is offered “a new assistive technology” in response. The story continues with an explanation that the BCI would improve functioning toward the speed of an average person at low malfunctioning risk, as well as the vignette person’s decision to use or not use it. Respondents were randomly assigned to a version in which the vignette person decided either to not use or to use the BCI (between-subject design).
Dependent variable
After the vignette was presented for a minimum of 45 seconds, we assessed three dimensions of stigmatization using measures adapted from the Attribution Questionnaire (Corrigan, 2012; Pinto et al., 2012): stigmatizing cognition (i.e. blaming the vignette person), negative affect (i.e. anger felt), and a coercive behavioral response (i.e. requiring BCI use irrespective of the person’s will). The wording is provided in Figure 1. Response options ranged from “not at all” (value 1) to “very much” (10).
Cognitive pretesting
To increase instrument effectiveness, think-aloud cognitive pretests with additional probing questions (Van Someren et al., 1994) were conducted with undergraduates and local researchers unfamiliar with our project (N = 5). This led to changes of the vignettes and the questions to increase clarity and uniformity in respondent interpretation of the scenario, the vignette person’s characteristics, and the survey questions.
Results
Based on a linear regression model (for descriptive details and for the regression tables, see Tables S1a and b in the Supplemental Material), we found that respondents expressed statistically significantly (t = 5.47; p < .001) more blame toward the vignette person’s decision regarding the BCI if he refused a BCI (as opposed to choosing to use it). Figure 2 shows that blame increased by B = 2.069 (95% CI = 1.323 to 2.814) on the 10-point scale. Further models reveal that such a decline evoked more anger (B = 1.361; 95% CI = 0.649 to 2.072; t = 3.77; p < .001), but it did not cause a coercive behavioral response (B = −0.067; 95% CI = −0.872 to 0.738; t = −0.16; p = .870).
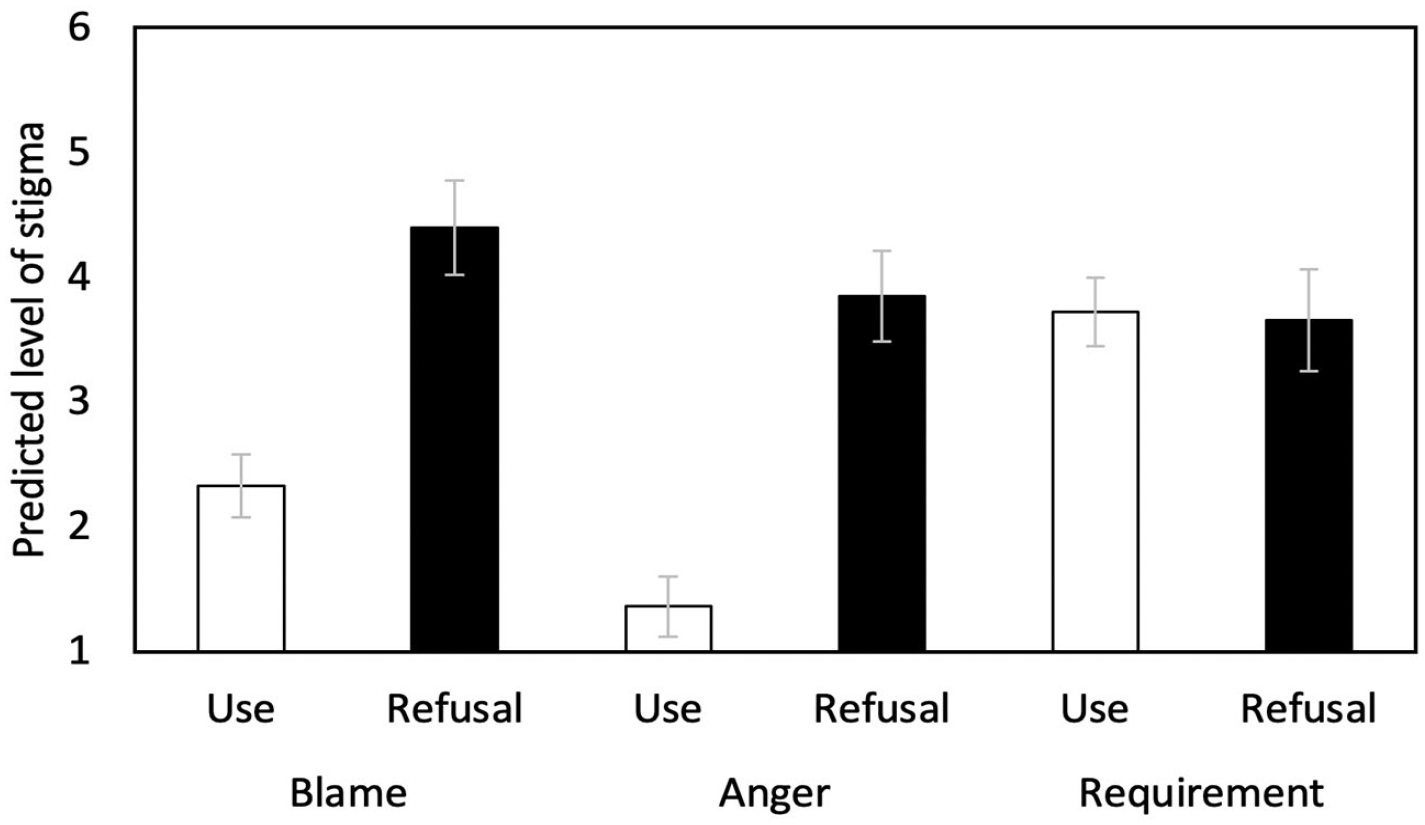
Predicted values (with standard errors) regarding three stigma dimensions depending on the experimental treatment (use-decision), based on the linear regression models—Experiment 1 (N = 222).
Discussion
Experiment 1 provides initial evidence that the active refusal of technology described as modestly improving the work situation of a disabled person causes stigmatizing cognitions and affects. However, irrespective of the decision, participants moderately endorsed making BCI use mandatory for the vignette person even if he does not want it. Thus, our first hypothesis (H1Resigning benefits) was supported for two out of three stigma dimensions. Still, the moderately high level of endorsement of the coercive behavioral response (i.e. making BCI use mandatory) suggests a serious form of stigma, even if it is not causally affected by the experimental variable tested here.
It is important to emphasize that in this experiment the BCI was described as helping the vignette person serve customers as fast as “the average person,” representing an improvement to the associated level of human function. However, current BCIs may not always be this effective, while other depictions of the technology in popular media promise performance beyond “normal.” The latter form of rhetoric is exemplified by the private start-up Neuralink and associated hype (Fourneret, 2020). Therefore, it would be important to also observe if the stigma associated with refusing BCI technology is altered by the technology’s level of function.
3. Experiment 2
Experiment 2 examined whether stigmatization concerning the decision to use or refuse a BCI was affected by the level of BCI functioning. It can be assumed that better functioning BCIs create higher benefits to the interaction partner (i.e. the customer) and offer more control to the user over their disability, which makes the use judged more positively and the refusal more negatively. Accordingly, Experiment 2 tested the basic assumption that a refusal is more strongly stigmatized the more functionality is forgone by nonuse, because missing benefits for bystanders is judged negatively, that is, functioning plays a moderating role concerning the decision. In other words, the higher the functioning (and thereby its promised controllability and positive outcomes for others), the more the stigma. Thus, we assumed that average (H2aFunctioning level) and high (H2bFunctioning level) functioning compared with low functioning, as well as high compared with average (H2cFunctioning level) increase stigma. It is reasonable that especially high (vs low) functioning increases stigma, since the forgone benefit is comparatively large. However, above-average functioning could create fears of societal competition and “super humans” (Sandel, 2007) and due to partially negative views and low acceptability of enhancement (Medaglia et al., 2019; Sattler and Pietralla, 2022), refusing high-functioning BCIs might be seen as a justified rejection of unnatural human features and therefore judged less negatively than refusing BCI devices allowing only for “restoration.”
Methods
Participants
As in Experiment 1, participants were recruited via AMT. Of 998 prospective respondents, 984 (98.6%) consented to participate and 695 (70.6%) passed the attention check. We used the data of 620 (89.2%) respondents who completed the survey and had no missing responses. Of these, 59.2% identified as men and the average age was 36.32 (SD 11.10). Those who completed the survey also received a small cash compensation.
Experimental design
The basis of the vignette was identical to Experiment 1, but in addition to varying the decision of the vignette person to not use versus use a BCI device, we experimentally varied the functionality of the BCI along three levels: faster than he currently does, but slower than the average person, versus as fast as the average person, versus much faster than the average person (Figure 1). This resulted in a 2 × 3 between-subjects design.
Dependent variable
We again asked questions about blame, anger, and coercive behavioral response toward the cashier after the vignette was displayed for at least 45 seconds.
Cognitive pretesting
The vignettes were pretested as described in Experiment 1 (N = 5).
Results
A main effects linear regression model supports the findings of Experiment 1 by showing that statistically significantly more blame was expressed toward vignette persons refusing BCIs as compared with using them (B = 1.543; 95% CI = 1.050 to 2.035; t = 6.15; p < .001, Tables S2a and b). Blame was not substantially affected if the BCI improved the functioning lower than versus the same as that of the average person (B = 0.287; 95% CI = −0.307 to 0.880; t = 0.95; p = .343). But functioning much faster than the average person (compared with below) increased blame statistically significantly (B = 0.711; 95% CI = 0.649 to 2.072; t = 3.77; p < .001). Post-estimation Wald tests found no statistically significant difference between the average and higher functioning conditions (F = 1.94; p = .165). In a subsequent model, an interaction term between the use-decision and functionality was added to test our hypotheses (H2a-cFunctioning level). However, we found no differential effects of refusal on stigma depending on functioning, that is, if the functioning was lower versus the same as that of the average person (B = 0.498; 95% CI = −0.689 to 1.685; t = 0.82; p = .411) or if the functioning was lower than versus much higher than that of the average person (B = −0.269; 95% CI = −1.523 to 0.975; t = −0.42; p = .672) (Figure 3).
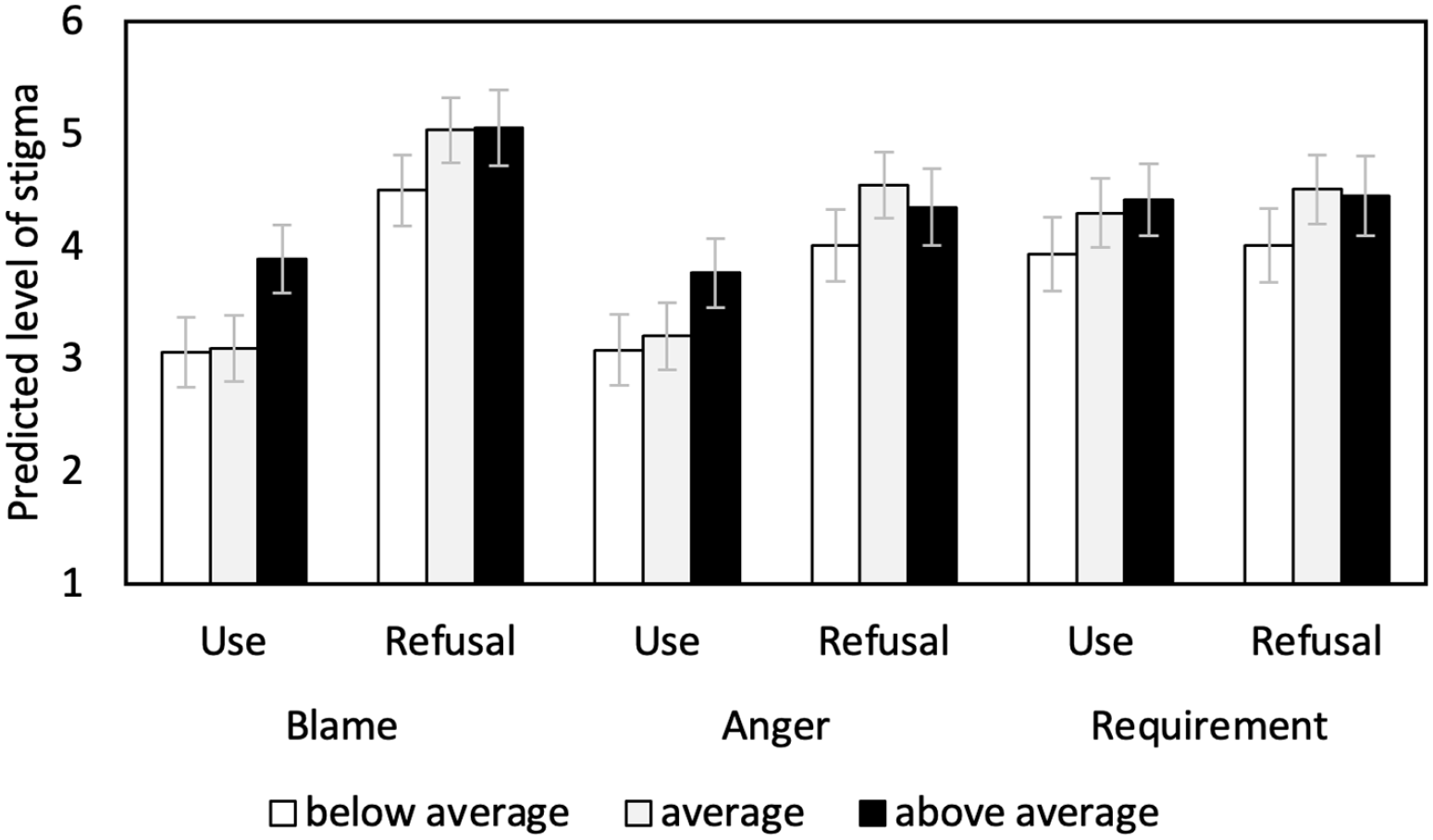
Predicted values (with standard errors) regarding three stigma dimensions depending on the experimental treatments (use-decision and functionality of the BCI) and their interaction, based on the linear regression models—Experiment 2 (N = 620).
Similar to Experiment 1, anger was higher toward vignette persons refusing rather than using BCIs (B = 0.977; 95% CI = 0.477 to 1.477; t = 3.84; p < .001). Anger was, however, not affected by the functionality, neither when comparing lower functioning with average functioning (B = 0.329; 95% CI = −0.274 to 0.931; t = 1.07; p < .284) or higher functioning (B = 0.531; 95% CI = −0.098 to 1.161; t = 1.66; p < .098) nor average functioning with higher functioning (F = 0.43; p = .513). Again, no interaction effects between the use-decision and functionality were found if the functioning was lower than versus the same as that of the average person (B = 0.411; 95% CI = −0.794 to 1.616; t = 0.67; p = .503) or lower than versus much higher than that of the average person (B = −0.346; 95% CI = −1.608 to 0.917; t = −0.54; p = .591).
Opinions about requiring BCI use were independent of the decision to use or not use a BCI (B = 0.116; 95% CI = −0.403 to 0.635; t = 0.44; p = .661). Functioning did not affect views concerning coercion to use a BCI, neither when comparing lower functioning with average functioning (B = 0.434; 95% CI = −0.192 to 1.059; t = 1.36; p = .174) or higher functioning (B = 0.468; 95% CI = −0.185 to 1.122; t = 1.41; p = .160) nor average functioning with higher functioning (F = 0.43; p = .513). No interaction effects were found between the decision and the functionality (low vs average: B = 0.130; 95% CI = −1.122 to 1.382; t = 0.20; p = .838; low vs high: B = −0.042; 95% CI = −1.354 to 1.270; t = −0.06; p = .950).
Discussion
Experiment 2 found that, in line with H1Resigning benefits and consistent with Experiment 1, stigmatizing attitudes in the form of blame and anger were on average higher if the vignette person refused a BCI. Coercive behavioral responses were again not affected by the decision but were on average moderately high. These effects were independent of the functioning level of the BCI, not supporting H2a–cFunctioning level. However, we found a tendency toward more blame when the BCI was able to make its user “much faster” than the average person (as compared with low functioning, independent of the decision). Yet, the concern here that people fear the creation of “super humans” might not be as substantial as sometimes voiced in the literature. This is supported by the finding that the level of coercive behavioral response was unaffected by this high functionality. However, this could be different if the person would have no disability because benevolence-minded stigma might have buffered potential negative stigmatization. While the functioning seems of little relevance, it is an open question as to whether the risk of device malfunctioning lowers the stigma of refusing a BCI. A recent survey indicated that the seriousness of device failure was the second most concerning factor for respondents (Sample et al., 2019b), pointing toward this being a relevant factor for judging BCIs and their use(rs).
4. Experiment 3
As highlighted above, many BCI devices are prone to errors and low reliability for some users (Fenton and Alpert, 2008; Thompson, 2019). A high malfunctioning risk indicates that the user has little control over the device and that the device might be of limited value for the user and interaction partners. Refusing it might be seen as more justified than refusing a device with low malfunctioning risk. We therefore predict a moderating role of the level of malfunctioning, namely, that less stigma is associated with refusal if the malfunctioning risk is average (H3aMalfunctioning) and high (H3bMalfunctioning) compared with low, as well as high compared with average (H3cMalfunctioning). After Experiments 1 and 2 found consistent stigma effects of BCI refusal in one context (BCI use by a cashier), we wanted to test whether these effects also hold in another context. Given that the first context described a low-stakes situation, that is, in which the (non)use of the BCI has limited practical consequences for co-workers, customers, and the user in the form of perceived inconvenience, we wanted to increase the practical and ethical stakes and test the expected effects in a higher-stakes situation: driving a vehicle.
Methods
Participants
For Experiment 3, we again recruited participants via AMT. Of 959 prospective respondents, 945 (98.5%) consented to participate, and 701 (74.2%) passed the check. We used the data of 622 (89.50%) respondents who completed the survey and had no missing responses. Of the analytical sample, 58.0% identify as men, and the average age was 38.37 years (SD 12.18). Completers received a small cash compensation.
Experimental design
While using the same basis for the low-stakes vignette as before, the decision to not use versus use a BCI varied along three levels of risk of device malfunctioning: low versus moderate versus high, resulting in a 2 × 3 between-subjects design (Figure 1). The high-stakes vignette was composed to follow the basic structure of the low-stakes vignette, but the workplace difficulty was framed to be much more salient. A taxi driver’s driving was described as too slow to save an ill passenger’s life, making the potential benefit of a BCI more pressing (Figure 4). This vignette was shown after respondents provided their answers for the low-stakes vignette. Respondents received one vignette randomly drawn from this 2 × 3 between-subjects design with the same two vignette dimensions (usage and risk of device malfunctioning), but with a randomization of vignette levels that was independent of the given low-stakes vignette.
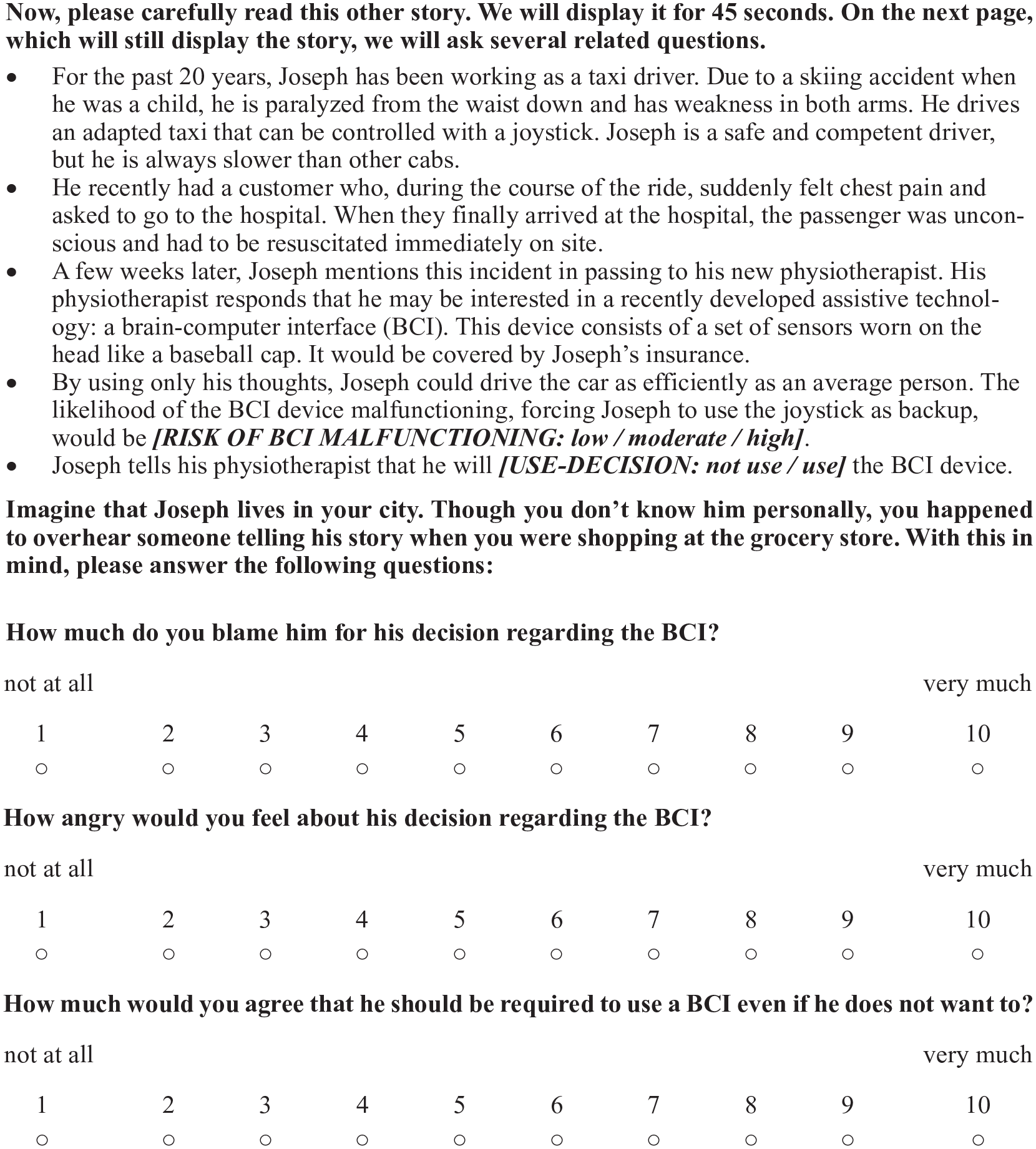
Taxi vignettes of Experiment 3 with the respective outcome measures.
Dependent variable
For both vignettes, the levels of blame, anger, and coercive response were assessed.
Cognitive pretesting
Both the low-stakes and high-stakes vignettes underwent cognitive pretesting (N = 5) as described in Experiment 1.
Results
Low-stakes situation
As in both prior experiments, a multivariate linear regression model testing the main effects revealed more blame for BCI refusal than use (B = 0.588; 95% CI = 0.083 to 1.093; t = 2.29; p = .022; Tables S3a and b). No statistically significant differences were found between low versus moderate malfunctioning risk (B = −0.497; 95% CI = −1.113 to 0.119; t = −1.58; p = .114) and between moderate versus high risk (F = 2.16; p = .143). However, high risks evoked less blame than low risk (B = −0.961; 95% CI = −1.575 to −0.346; t = −3.07; p = .002). When adding an interaction term between use-decision and malfunctioning risk to the model, blame associated with refusing BCIs was not statistically significantly reduced if the risk was only moderate compared with low (B = −0.619; 95% CI = −1.838 to 0.600; t = −1.00; p = .319, Figure 5). However, we found an interaction effect between the use-decision at high versus low malfunctioning risk (B = −2.416; 95% CI = −3.634 to −1.197; t = −3.89; p < .001). A follow-up simple slopes test showed that at the level of low malfunctioning risk, the refusal of a BCI resulted in more blame than the use of the BCI (B = 1.588; 95% CI = 0.734 to 2.441; t = 3.65; p < .001). At the level of moderate malfunctioning risk, a refusal still led to more blame than a use decision (B = 0.969; 95% CI = 0.098 to 1.840; t = 2.18; p = .029). When the risk level was high, a refusal was not statistically significantly blamed further compared with a use decision (B = −0.828; 95% CI = −1.697 to 0.041; t = −1.87; p = .062). While this effect sharply misses conventional levels of significance in this condition, it shows the tendency for users to be blamed more than refusers. Moreover, in the case of refusal, a high risk resulted in statistically significantly less blame compared with a low risk (B = −2.081; 95% CI = −2.913 to −1.249; t = −4.91; p < .001).
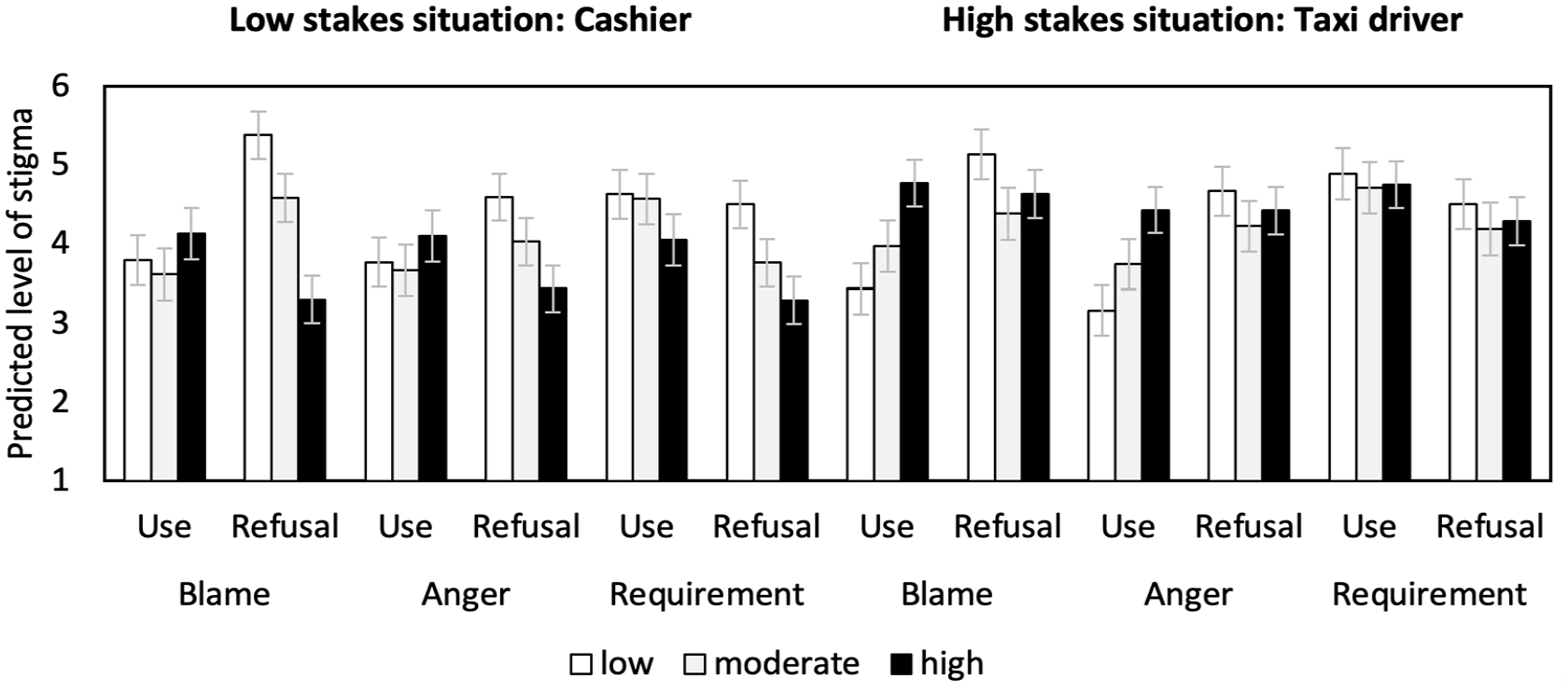
Predicted values (with standard errors) regarding three stigma dimensions depending on the experimental treatments (use-decision and risk of BCI malfunctioning) and their interaction for low-stakes and high-stakes situations, based on the linear regression models—Experiment 3 (N = 622).
A main effects model showed main effects neither of BCI refusal on anger (B = 0.183; 95% CI = −0.313 to 0.678; t = 0.72; p = .470) nor of the malfunctioning risk (low vs moderate: B = −0.337; 95% CI = −0.942 to 0.267; t = −1.10; p = .274; low vs high: B = −0.466; 95% CI = −1.069 to 0.138; t = −1.52; p = .130; or moderate vs high: F = 0.17; p = .679). When testing for possible interaction effects between the use-decision and the malfunctioning risk, the anger evoked by refusing BCIs was not statistically significantly reduced if the risk was only moderate compared with low (B = −0.465; 95% CI = −1.672 to 0.742; t = −0.76; p = .449, Figure 5), but an interaction effect between the use-decision for high versus low malfunctioning risk was found (B = −1.489; 95% CI = −2.695 to −0.284; t = −2.43; p = .016). A follow-up simple slopes test showed that at the level of low malfunctioning risk, a refusal led to more anger than a use decision (B = 0.826; 95% CI = −0.018 to 1.671; t = 1.92; p = .055). At a moderate malfunctioning risk, a refusal did not result in more anger (B = 0.361; 95% CI = −0.501 to 1.223; t = 0.82; p = .411). At a high risk level, the sign of the effect turned negative for refusal (but failed conventional levels of significance), still indicating a tendency toward less anger for BCI refusal (B = −0.663; 95% CI = −1.523 to 1.223; t = −1.51; p = .131). In the case of refusal, anger was statistically significantly lower if the risk level is high as compared with low (B = −1.157; 95% CI = −1.980 to −0.334; t = −2.76; p = .006).
Respondents on average endorsed a coercive response less in the case of BCI refusal as compared with a use (B = −0.562; 95% CI = −1.058 to −0.658; t = −2.22; p = .026). The endorsement was also lower if the malfunctioning risk was high versus low (B = −0.909; 95% CI = −1.513 to −0.305; t = −2.95; p = .003), but no statistically significant differences were found between low versus moderate levels of risk (B = −0.413; 95% CI = −1.019 to 0.192; t = −1.34; p = .181) and moderate versus high malfunctioning risk (F = 2.55; p = .111). We did not find evidence for possible interaction effects between the use-decision and functionality if the malfunctioning risk was low versus moderate (B = −0.682; 95% CI = −1.899 to 0.526; t = −1.11; p = .267, Figure 5) or low versus high (B = −0.634; 95% CI = −1.846 to 0.577; t = −1.03; p = .304). However, an additional simple slope test indicated that only in the case of refusal, low versus high malfunction had a statistically significantly effect on the level of endorsement, namely, that this endorsement was lower when the risk was high rather than low (B = −1.208; 95% CI = −2.035 to −0.381; t = −2.87; p = .004). No such effect existed in the other conditions, that is, the slope was always statistically insignificant (in case of use when comparing low with moderate risk: B = −0.055; 95% CI = −0.932 to 0.823; t = −0.12; p = .903 or low with high risk: B = −0.574; 95% CI = −1.459 to 0.312; t = −1.27; p = .204 and in case of refusal when comparing low with moderate risk: B = −0.741; 95% CI = −1.577 to 0.096; t = −1.74; p = .082).
High-stakes situation
In the high-stakes situation, BCI refusal also resulted in higher blame compared with BCI use when testing for main effects (B = 0.630; 95% CI = 0.120 to 1.140; t = 2.42; p = .016; Tables S4a and b). No statistically significant differences were found between low versus moderate (B = −0.118; 95% CI = −0.760 to 0.524; t = −0.36; p = .718), low versus high (B = 0.414; 95% CI = −0.200 to 1.028; t = 1.32; p = .186), and moderate versus high malfunctioning risk (F = 2.81; p = .094). We found statistically significant interaction effects of the use-decision and moderate versus low risk level (B = −1.288; 95% CI = −2.565 to −0.011; t = −1.98; p = .048), as well as high versus low risk level (B = −1.837; 95% CI = −3.058 to −0.615; t = −2.95; p = .003). This was also shown by a simple slopes analysis: at a low level of malfunctioning risk, refusal as compared with use resulted in more blame (B = 1.702; 95% CI = 0.811 to 2.592; t = 3.75; p < .001, Figure 5). The refusal effect became statistically insignificant at the moderate level (B = 0.414; 95% CI = −0.502 to 1.323; t = 0.89; p = .375), while the sign of the statistically insignificant effect turned negative at the high level (B = −0.135; 95% CI = −0.972 to 0.701; t = −0.32; p = .751). In addition, blame increased if a high versus a low risk BCI was used (B = 1.335; 95% CI = 0.471 to 2.199; t = 3.03; p = .003).
Refusing instead of using a BCI led on average to more anger (B = 0.635; 95% CI = −0.137 to 1.133; t = 2.50; p = .013). No main effect existed regarding different levels of malfunctioning risk (low vs moderate: B = 0.060; 95% CI = −0.567 to 0.682; t = 0.19; p = .852; low vs high: B = 0.506; 95% CI = −0.093 to 1.105; t = 1.66; p = .098; or moderate vs high: F = 2.08; p = .150). When adding the interaction term between use-decision and malfunctioning risk, we found no interaction for moderate versus low risk (B = −1.027; 95% CI = −2.276 to 0.222; t = −1.62; p = .107, Figure 5), but for high versus low risk there was an interaction effect (B = −1.516; 95% CI = −2.276 to −0.321; t =−2.49; p = .013). A simple slopes test showed that a refusal (vs use) only statistically significantly increased anger at low risk levels (B = 1.508; 95% CI = 0.638 to 2.379; t = 3.40; p = .001, Figure 5). At moderate (B = 0.481; 95% CI = −0.414 to 1.377; t = 1.06; p = .292) and high (B = −0.008; 95% CI = −0.826 to 0.810; t = −0.02; p = .985) risk levels, refusal had no statistically significant effect on anger. Moreover, anger was only increased if a high versus a low risk BCI was used (B = 1.266; 95% CI = 0.421 to 2.111; t = 2.94; p = .003). In the other conditions, the slopes were always statistically insignificant (in case of use when comparing low with moderate risk: B = 0.581; 95% CI = −0.303 to 1.464; t = 1.29; p = .197 and in case of refusal when comparing low with moderate risk: B = −0.446; 95% CI = −1.329 to 0.436; t = −0.99; p = .321 and low with high risk: B = −0.250; 95% CI = −1.095 to 0.594; t = −0.58; p = .561).
The endorsement of requiring BCI use was not affected by the use-decision (B = −0.456; 95% CI = −0.967 to 0.055; t = −1.75; p = .080) or the malfunctioning risk (low vs moderate: B = −0.246; 95% CI = −0.889 to 0.397; t = −0.75; p = .453; low vs high: B = −0.179; 95% CI = −0.793 to 0.436; t = −0.57; p = .569; or moderate vs high: F = 0.04; p = .833). We found no evidence of an interaction between the use-decision and functionality if the malfunctioning risk was low versus moderate (B = −0.136; 95% CI = −1.424 to 1.152; t = −0.21; p = .836, Figure 5) or low versus high (B = −0.082; 95% CI = −1.314 to 1.149; t = −0.13; p = .896).
Discussion
Experiment 3 generally verified the findings of Experiments 1 and 2 on the refusal effect of BCI technology in two settings (low-stakes and high-stakes), in line with H1Resigning benefits. More blame, anger (only in the high-stakes vignette), and coercion to use a BCI (only in the low-stakes vignette) were observed in the case of refusal (vs use) in the main effects analyses in Experiment 3. However, when taking the risk of malfunctioning into account (i.e. in the interaction effect analyses), refusal (vs use) did not always result in such an increase in stigmatizing tendencies. There was mainly a significant tendency toward this when the risk level was low (in the low-stakes situation, there was also more blame when the risk was moderate). This partially supports the assumption in H3a, bMalfunctioning that the stigma-increasing effect of BCI refusal disappeared when the BCI had higher risks of malfunctioning. In the low-stakes vignette, respondents generally voiced less coercive responses to use of BCIs if the vignette person refused the BCI and if the malfunctioning risk was high. Both effects were independent of each other.
5. General discussion
Summary and interpretation of the findings
In this study, we conducted three survey experiments to examine whether the refusal of assistive technology in the form of BCIs elicits stigma. We consistently found—across all experiments and in two contexts—that refusing as compared with using an assistive BCI in the workplace by a person with motor impairments evoked more blame and anger (on average), which supports our first hypothesis (H1Resigning benefits). The only exception was anger in the low-stakes situation in Experiment 3. Respondents’ judgment on whether someone should be required to use a BCI irrespective of their desires was not affected by the use-decision or the conditioning factors functionality and malfunctioning risk. Only in the low-stakes vignette in Experiment 3, a refusal evoked lower levels of coercive response. Against our second hypothesis (H2Functioning level), the functioning level of the BCI did not moderate the effect of refusal on stigmatization. In support of our third hypothesis (H3Malfunctioning), we found evidence that a high malfunctioning risk can offset stigma of refusing a BCI, that is, the refusal was blamed less and anger was less voiced if the BCI malfunctioning risk was high. Moreover, we found in the low-stakes vignette that in the case of refusal, the endorsement of a coercive response was lower when the risk was high rather than low. Another general observation is that the mean values for blame, anger, and views on requiring a BCI are below the theoretical scale mean (besides few exceptions in few experimental conditions), also in case of refusal. Based on this, one could conclude that stigmatizing attitudes are not extensively prevalent. However, in all three experiments, the full range of response options was always used (i.e. a share of respondents also used the highest response category implying very strong stigmatizing attitudes).
Overall, these results seem to reinforce the seriousness of worries expressed by scholarly critics of BCIs in STS, (dis)ability studies, and bioethics, particularly Wolbring and Diep (2016) regarding “ability expectations” and Aas and Wasserman (2016) regarding stigma. Reading about a new assistive technology that potential users do not adopt can evoke unfair “ability expectations” toward disabled people. Refusing the offer of a new technology, even if the benefits for the disabled person and others are only moderate, may be seen as rejecting widely shared hopes for a technological solution (Sample et al., 2019b). Thus, in line with the predictions of Attribution Theory, the expected responsibility to “overcome” the current state of disability evokes stigmatizing attitudes since respondents may have attributed a lack of effort and taking this responsibility if the vignette person decided against a BCI (Corrigan, 2006; Weiner, 1993). These results are consistent with critiques of widespread ableist rhetoric in society (Cherney, 2011), and reveal one possible mechanism underpinning a core tenet of STS, which holds that the rights and responsibilities of individuals and technological systems are interdependent (Jasanoff, 2004; Winner, 1980). As new neural technologies enter collective awareness through the media and unrealistic narratives, our expectations toward one another shift.
The specific finding that more blame was voiced if the BCI enabled enhanced abilities—independent of the use decision—may correspond to previously observed fears of “cyborgization” which may lead to dehumanization or concerns about the effects of enhancement on fairness (Grewal et al., 2020; Sample et al., 2019b). However, our results suggest that fear of enhancement might not be the major driver in the evaluation of disabled individuals’ refusal as operationalized in our study. Malfunctioning, in contrast, is a noted risk of BCI technology (Sample et al., 2019b; Thompson, 2019), and we expected to find that higher risk can offset the stigma attached to its refusal since their users would not gain the expected higher control over their situation, and because their use could even be seen as dangerous, while stigma attached to refusal is especially high in the absence of such risks. We found evidence for both, that is, reduced stigma attached to the refusal in the case of high malfunctioning risk (i.e. the refusal of gaining unreliable control) and higher stigma attached to BCI use in the case of high malfunctioning risk (i.e. engaging in unreliable technology that could evoke the fear of dangerous consequences).
Finally, our results also have urgent practical and ethical implications. First, service research and consumers should critically reassess the use of BCIs in retail, sales, and service settings (e.g. Grewal et al., 2020) concerning the possible burden resulting from expectations to use assistive technology by disabled employees. Besides the psychological discomfort of the employees using or refusing such technologies, simply promoting the idea of BCIs as removing the effects of disability may cause customers and co-workers to harbor unfair expectations and negative assessments of disabled employees who still experience difficulty, adding to pre-existing workplace ableism and associated injustices. Likewise, our findings provide further reason to worry about the many unrealistic depictions of BCI devices in the research literature and in the media (Gilbert et al., 2019; Purcell-Davis, 2013). By promising life-changing solutions to the challenges faced by disabled people, the vague communication of technological hope may cause harm. It may perpetuate a restorative narrative for people living with disabilities and reinforce unfair ability expectations. Familiarizing workplace staff and customers, as well as the general public, with the real-world limitations of new technologies could allay possible stigmatization, but ultimately a holistic institutional and regulatory response may be required.
Strengths, limitations, and directions for future research
In comparison to previous methods of BCI research (Kögel et al., 2019; Burwell et al., 2017), our study is perhaps the first to causally test high-level hypotheses about the social effect of BCIs in society. Because of the methodological necessity to limit the number of experimental variables in the vignette (e.g. depicting someone implied to be a man and choosing to focus a work context), our study lends clarity on some important factors in stigma linked to BCIs but leaves many uninvestigated, including gender, aesthetics, context of use, class and economic environment, racialization, and able-bodied use. A comprehensive understanding of how these factors impact stigma requires further quantitative experimental research (e.g. outside the work context) and, if BCIs become more widely used in society, validation through qualitative studies of the lived experience of BCI users.
It also a strength of our study that we collected samples from a platform with more demographically diverse samples as compared with standard Internet and American college samples (Buhrmester et al., 2011; Clifford et al., 2015). Still, such samples are not representative of the population and, as a technology, AMT may pose its own ethical challenges and potential for inequity (Gleibs and Albayrak-Aydemir, 2022; Heen et al., 2014; Ipeirotis, 2010). For example, we found a larger number of men participating in our experiments. Such gender disparities can depend on the type of task and survey platform (Al-Ani and Stumpp, 2016). Moreover, we found that the proportion of respondents failing the attention check ranged between approximately 20% and 30% across our experiments. However, these high rates also indicate a strong selection for participants who paid sufficient attention to continue with the survey. This ex ante screen out of inattentive respondents is therefore a means to increase data quality and it can also be seen as a motivational trigger (Shamon and Berning, 2020). Both are important for vignette studies that require a careful reading. Future research should test our findings with nationally representative samples and also target different countries, as views toward BCIs vary geographically (Sample et al., 2019b).
Expressing stigmatizing attitudes can be seen as a sensitive topic that can result in socially desirable responses and item nonresponse. All our experiments were self-administered online using hypothetical situations (vignettes). Both design features have been found to increase the accuracy of providing sensitive information (Choong et al., 2002; Crutzen and Göritz, 2010; Kreuter et al., 2008). When including a measure of anonymity perception (concerning our survey) to the models (Patrzek et al., 2015), we found the same pattern in the results (available upon request). This suggests that respondents who have stigmatizing attitudes and ableist beliefs are comfortable expressing them, which itself deserves further consideration in study design. Future studies could, for example, include a debriefing session to counteract these attitudes, based on design feedback and testimony from disabled people.
6. Conclusion
In this study, we set out to empirically investigate a serious concern in BCI ethics and, in a more abstract way, in the STS literature: the idea that the promotion of BCIs as an assistive technology could exacerbate the stigmatization of disability. We used Attribution Theory and survey experiments to examine the effect of technology refusal on the endorsement of stigmatizing cognitive, emotional, and behavioral reactions toward disabled people when interacting with others in the work context. Overall, our results support academic critiques; hearing about a refusal of an assistive technology evoked blame and anger. It is possible that the social reinforcement of beliefs and attitudes toward technology and disability (e.g. by the media or biomedical experts) would further amplify stigmatization. We showed that the level of BCI functioning did not change reactions toward BCI refusal, while the likelihood of malfunction, which is a common occurrence for most BCIs, did. In terms of theoretical significance, our study suggests there is value in connecting STS theory and social psychology of stigma; STS, thanks to its high-level theses about technological discourses and social order, provides a domain of inquiry, to which social psychology can contribute experimental methods, interpersonal models, and quantitative measures. Finally, and perhaps more importantly, our findings pose an urgent practical and ethical challenge. As BCI technology is popularized as the solution to many forms of disability, false hopes and unrealistic depictions of reliability could exacerbate ableism in society with very concrete and harmful implications. BCI developers and proponents in the media, in addition to government and regulatory agencies, will need to adapt their practices and respond accordingly.
Supplemental Material
sj-pdf-1-pus-10.1177_09636625221141663 – Supplemental material for Brain-computer interfaces, disability, and the stigma of refusal: A factorial vignette study
Supplemental material, sj-pdf-1-pus-10.1177_09636625221141663 for Brain-computer interfaces, disability, and the stigma of refusal: A factorial vignette study by Matthew Sample, Sebastian Sattler, Wren Boehlen and Eric Racine in Public Understanding of Science
Footnotes
Acknowledgements
The authors thank the members of the Pragmatic Health Ethics Research Unit for assistance in cognitive pretesting, Floris van Veen for programming the survey, and Stefanie Blain-Moraes for input on the survey instrument.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
The questionnaire and methodology for this study was approved by the research ethics committee of the Institut de recherches cliniques de Montréal (Approval No. 2018-904).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the Canadian Institutes of Health Research and the Fonds de recherche du Québec—Santé (European Research Projects on Ethical, Legal, and Social Aspects (ELSA) of Neurosciences).
Informed consent
Informed consent was obtained from all study participants.
Supplemental material
Supplemental material for this article is available online.
Notes
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.