
Abstract
Mesenchymal stromal cell (MSC)–based therapies have demonstrated broad therapeutic potential across inflammatory, degenerative, and neurological disorders; however, clinical outcomes remain highly variable, largely due to heterogeneity in cell source, dosing strategies, routes of administration, treatment timing, and patient-specific factors. This review evaluates how MSC dose and delivery route influence clinical efficacy and safety, and whether specific administration routes require tailored dosing strategies. A systematic literature search of PubMed, Scopus, Web of Science, and the Cochrane Library (2015–2025) identified 29 eligible clinical trials employing intravenous (n = 13), intrathecal (n = 10), intramuscular (n = 4), intranasal (n = 1), and multi-route (n = 1) administration, with doses ranging from 2 × 105 cells/kg body weight to fixed doses exceeding 1 × 108 cells. Intravenous delivery was predominantly used for systemic indications but was limited by pulmonary first-pass sequestration, whereas intrathecal and intranasal routes enhanced central nervous system targeting and intramuscular administration supported prolonged local persistence and paracrine activity. Although MSC therapy was generally well tolerated across studies, substantial outcome variability underscores the need for harmonized frameworks for dose selection, route optimization, and manufacturing consistency. This review highlights critical gaps in dose–route optimization and supports the development of standardized clinical guidelines and advanced strategies, including MSC priming and engineering, to improve therapeutic predictability and translational success.

Keywords
1. Introduction
Regenerative medicine, particularly therapies based on mesenchymal stromal cells (MSCs) and their derivatives, has demonstrated substantial therapeutic potential across a wide range of clinical indications. Accumulating preclinical and clinical evidence indicates that MSC-based interventions may promote tissue repair and modulate immune responses, largely through mechanisms involving cell homing, paracrine signaling and microenvironmental (niche) modulation.1–7 Despite these advances, many clinical conditions remain inadequately managed, and the translation of MSC-based therapies into consistent clinical benefit remains challenging. Nevertheless, selected clinical studies have reported meaningful improvements in patient outcomes, underscoring the therapeutic promise of MSC-based approaches.5,8,9
However, therapeutic responses to MSC-based therapies remain highly variable across patients and disease contexts. While some patients experience substantial clinical benefit, others demonstrate limited or no response. This variability represents a critical barrier to clinical translation and highlights the need to better understand the determinants of therapeutic efficacy.1,6 Multiple factors have been implicated in contributing to this heterogeneity, including the route of administration, dosing regimen, treatment interval, patient-specific characteristics, and product-related variables such as cell source, manufacturing processes, and phenotypic attributes.10–13
In addition, variability in administration strategies, dosing approaches, and manufacturing practices further complicates the standardization of MSC-based therapies and limits cross-study comparability. At present, there is no universally accepted framework for defining optimal MSC product characteristics, including donor selection, potency, and quality attributes. Furthermore, inconsistencies in patient preparation, treatment protocols, and post-administration management contribute to the difficulty in achieving reproducible therapeutic outcomes. 14
Despite encouraging clinical signals, the overall performance of MSC-based interventions remains inconsistent across trials. Variability in dosing strategies, routes of administration, treatment timing, and product quality continues to limit reproducibility and comparability across studies. Moreover, the absence of consensus guidelines for dose optimization and route selection further complicates clinical decision-making and translational implementation. Therefore, this review focuses on clinical trials of MSC-based therapies to systematically evaluate how dose, route of administration, and treatment timing interact as key determinants of efficacy and safety. By integrating evidence across diverse clinical settings, this study aims to identify emerging patterns that may inform more rational and standardized approaches to MSC therapy optimization.
2. Methods
2.1. Literature screening
The protocol used to conduct this review was organized according to the Preferred Reporting Items for Reviews and Meta Analysis (PRISMA) guidelines 15 (see supplementary file 1). Original studies published in English between 2015 and 2025 were searched using PubMed, Scopus, Web of Science, and Cochrane Library with the keywords of “stem cell therapy”, “mesenchymal stem cells”, “mesenchymal stromal cells”, “stem cell doses”, “stem cell route of administration”, “clinical trial”. Studies were further screened to include human clinical trials with clearly defined outcomes and sample sizes. To ensure comprehensive literature coverage and account for variations in terminology, both the terms “mesenchymal stem cells” and “mesenchymal stromal cells” were included in the search strategy. These terms were combined using “AND”, “OR” and adapted for each database. The last literature search was conducted on December 18, 2025.
2.2. Literature analysis
A systematic literature search followed by narrative synthesis was conducted in accordance with the PRISMA 2020 guidelines, as illustrated in Figure 1. A total of 34,694 records were identified through database searching. After the removal of non-English articles (n = 923), 33,771 records remained for screening. Following duplicate removal (if applicable), 33,771 records were screened based on titles and abstracts. Of these, 33,421 records were excluded for not meeting the predefined inclusion criteria. The inclusion criteria consisted of clinical trials, including randomized controlled trials (RCTs), non-randomized trials, and single-arm studies, involving human participants with medical conditions requiring treatment, interventions administered via intramuscular, intranasal, intrathecal, or intravenous routes, and reporting outcomes related to therapeutic effectiveness, clinical improvement, adverse effects, safety, and efficacy. Due to the limited number of randomized controlled trials in this field, broader clinical study designs were included to provide a more comprehensive overview of current clinical evidence. PRISMA flow diagram of the study selection process. Records were identified through database searching and screened according to predefined inclusion and exclusion criteria. Full-text articles were assessed for eligibility, and studies meeting the criteria were included in the final qualitative review.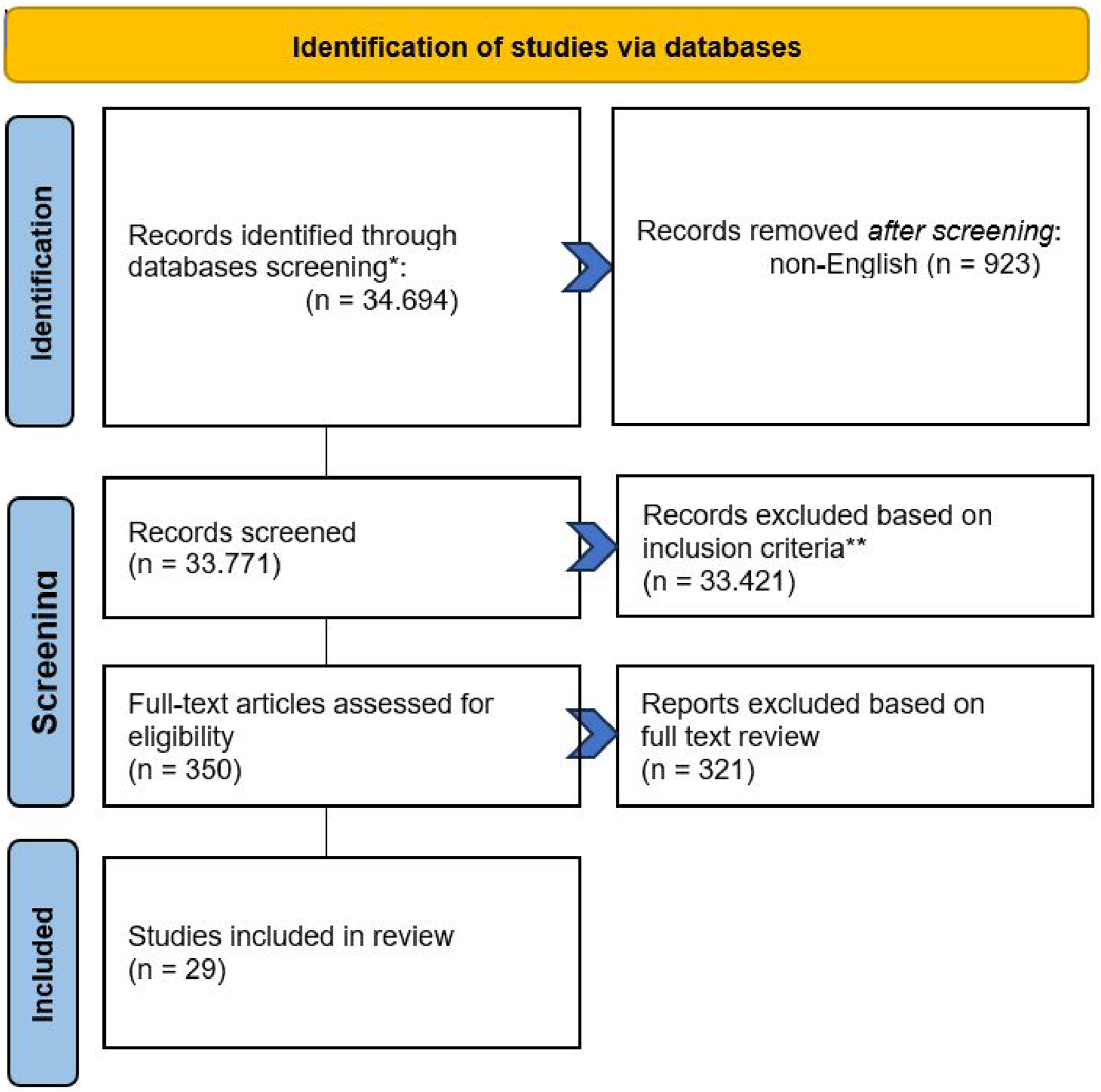
A total of 350 full-text articles were assessed for eligibility. Among these, 323 articles were excluded after full-text evaluation due to non-clinical study design (e.g., preclinical or in vitro studies), non-human subjects, absence of relevant outcome data, lack of dosage or administration details, or interventions not aligned with the specified routes of administration details. Extracted data were summarized in tabular form using Microsoft Excel and presented descriptively to facilitate comparison across studies. Studies then were grouped according to the route of administration (intravenous, intrathecal, intramuscular, and intranasal) and further analyzed descriptively based on dosing strategies and reported clinical outcomes. The primary outcomes of interest included clinical efficacy and safety. Efficacy outcomes were defined based on disease-specific clinical improvements, functional scores, or biomarker changes as reported in individual studies. Safety outcomes included the incidence of adverse events and serious adverse events.
Potential sources of bias and methodological limitations were considered narratively during the full-text assessment and interpretation of findings. A formal risk of bias assessment using standardized tools was not performed due to the heterogeneity in study designs, interventions, and outcome measures across the included studies, which also represents a limitation of this review. Ultimately, 29 studies were included in the qualitative synthesis of this systematic literature search followed by narrative synthesis.
Because of substantial heterogeneity in study design, dosing regimens, and outcome measures, a formal quantitative meta-analysis and standardized risk-of-bias assessment were not performed. In addition, due to the limited number of randomized controlled trials in this field, broader clinical study designs were included to provide a more comprehensive overview of current clinical evidence.
2.3. Data extraction and synthesis
Data extraction was conducted using a standardized form to capture study characteristics including author, publication year, study design, and treatment period, as well as population details such as demographic characteristics and baseline clinical conditions. Intervention-related information was extracted, including stromal cell source, dosage, administration frequency, and route of delivery, along with reported outcome measures related to effectiveness, safety indicators, and statistical significance. Data extraction was performed independently by two reviewers (CRS, AC), with any discrepancies resolved through discussion and consensus. The extracted data were synthesized using a structured narrative synthesis approach, in which studies were grouped according to intervention characteristics, routes of administration, and reported clinical outcomes. Comparative analysis was applied descriptively to explore patterns of effectiveness and safety across different dosing strategies and delivery routes. When data were missing or not clearly reported, the available information was used as presented in the original publications, and no additional assumptions or imputations were applied. This synthesis aimed to provide an integrated overview of current evidence on mesenchymal stromal cells therapy, with particular emphasis on identifying considerations for optimizing dosage and administration routes while maintaining safety in regenerative medicine applications.
3. Results
3.1. Study characteristics and selection
Of the 34,694 literatures identified, 29 met our criteria. Studies were excluded based on the predefined exclusion criteria described in the Methods section. Based on route of administration, the included studies were categorized as intravenous (n = 13), intrathecal (n = 10), intramuscular (n = 4), intranasal (n = 1), and multi-route (n = 1). Reported MSC doses ranged from 2 × 105 cells/kg body weight to fixed doses exceeding 1 × 108 cells.
3.2. Description of included studies
Literature review of clinical trials of MSCs’ dose and route.

Abbreviations: AD-MSC, Adipose Derived–Mesenchymal Stromal Cells; ALS, Amyotrophic Lateral Sclerosis; ASD, Autism Spectrum Disorder; BM-MSC, Bone Marrow–Mesenchymal Stromal Cells; BPD, Bronchopulmonary Dysplasia; CLI, Critical Limb Ischemia; DFU, Diabetic Foot Ulcer; DPN, Diabetic Peripheral Neuropathy; hcMSC, Human bone marrow–derived clonal Mesenchymal Stromal Cells; IM, Intramuscular; IN, Intranasal; ITH, Intrathecal; IV, Intravenous; MS, Multiple Sclerosis; MSC-NPs, Mesenchymal Stromal Cells–Non Progenitor; nRCT, Non-randomized Controlled Trial; PAD, Peripheral Artery Disease; P-MSCs, Placenta Derived–Mesenchymal Stromal Cells; RA, Rheumatoid Arthritis; RCT, Randomized Controlled Trial; RP, Retinitis Pigmentosa; SAE, Serious Adverse Event; SCI, Spinal Cord Injury; UC-MSC, Umbilical Cord–Mesenchymal Stromal Cells; WJ-MSCs, Wharton’s Jelly–Mesenchymal Stromal Cells.
Across the included studies, most clinical trials demonstrated favorable safety profiles, with minimal reports of serious adverse events. Clinical improvements were more frequently observed in studies utilizing localized (intramuscular) or central nervous system-targeted (intrathecal) delivery routes compared to systemic intravenous administration. However, the magnitude and consistency of therapeutic outcomes varied substantially across disease indications, dosing strategies, and study designs.
In addition, the majority of studies did not report quantitative data on MSC survival, engraftment, or persistence following administration, representing a critical limitation in interpreting therapeutic mechanisms. This heterogeneity, combined with inconsistent reporting standards, limits direct comparison across studies and underscores the need for more standardized clinical and reporting frameworks in MSC-based therapy.
4. Discussion
4.1. Dosing strategies and treatment schedules in MSC therapy
The dosage of MSCs therapy varies substantially across clinical indications, as summarized in Table 1. This variability reflects differences in disease pathology, route of administration, therapeutic objectives, and trial design. Such heterogeneity underscores the ongoing challenge of defining optimal dosing strategies in cell-based therapy and highlights the importance of tailoring treatment to disease context and patient characteristics.
MSC doses are typically reported either as a fixed total number of cells or adjusted to body weight in cells per kilogram. Intravenous administration demonstrates the widest dosing range, from 2 × 105 cells per kilogram 27 to fixed total doses of 2 × 108 cells, 26 with some protocols administering up to 4 × 108 cells per infusion. 16 Weight-based dosing, such as 2.05 ± 0.20 × 106 cells per kilogram, 19 is often adopted to account for inter-patient variability in systemic exposure. In contrast, intrathecal administration generally employs doses between 1 × 106 and 1 × 107 cells per kilogram, although fixed-dose regimens, such as 30 million cells per injection in amyotrophic lateral sclerosis (ALS) patients, 32 are also reported. For intramuscular delivery, clinical data remain limited. Most studies have used fixed doses ranging from 3 to 60 million cells,40–42 while only one trial implemented weight-adjusted dosing in Buerger’s disease. 45
The choice between fixed and weight-adjusted dosing reflects both practical and biological considerations. Weight-based strategies may improve dose precision in systemic delivery, whereas fixed dosing offers logistical simplicity and manufacturing feasibility, particularly for localized or intrathecal administration. Regulatory requirements, product scalability, and predefined safety thresholds further influence dosing decisions. However, the absence of standardized dose-ranging frameworks limits cross-trial comparability and hampers the identification of disease-specific dose-response relationships.
Beyond absolute dose, treatment timing and administration schedules represent critical yet inconsistently reported variables. Among the included studies, the onset of MSC administration ranged from 12 days to several months after injury. In spinal cord injury, delivery occurred between 12 and 16 days, 18 between 43 and 189 days, 17 or broadly within 14 days to 6 months post-injury. 29 In ischemic stroke, MSCs were administered approximately 61 days after onset, 19 whereas treatment for diabetic peripheral neuropathy was initiated an average of 6.4 ± 6.41 years after diagnosis. 42 Incomplete reporting of treatment timing in several studies further complicates interpretation of efficacy outcomes. Because host inflammatory status and tissue remodeling dynamics evolve over time, such variability may significantly influence therapeutic responsiveness.
The interval between administrations also varies widely, particularly in multidose regimens. Short intervals, including weekly infusions, have been applied in inflammatory and dermatological conditions requiring sustained immunomodulation.22,24 In neurodegenerative diseases, longer intervals are more common. For example, intrathecal MSC injections were administered every two months in patients with ALS. 32 Chronic conditions such as recessive dystrophic epidermolysis bullosa have involved extended treatment courses spanning months to years to maintain clinical benefit. 20 These patterns suggest that dosing frequency should align with disease chronicity and the expected duration of MSC-mediated effects.
Single-dose administration is typically employed in acute conditions or early-phase safety trials, where risk mitigation is prioritized. For example, a single intravenous dose of 2 × 108 adipose-derived MSCs was used in rheumatoid arthritis, 26 and 1 × 108 umbilical cord-derived MSCs were administered in retinitis pigmentosa. 28 In contrast, chronic or progressive diseases more frequently utilize repeated dosing to sustain therapeutic effects over time.
Despite encouraging clinical signals, no consensus currently exists regarding the optimal MSC dose or treatment schedule across indications. Weight-adjusted dosing may enhance systemic precision but increase logistical complexity, whereas fixed-dose approaches offer practicality but may not fully account for inter-patient variability. Furthermore, heterogeneity in cell sources, manufacturing processes, potency characteristics, and delivery protocols complicate direct comparison across studies. Collectively, these factors emphasize the need for mechanistically informed dose-ranging trials and standardized reporting frameworks to enable rational optimization of MSC therapy.
4.2. Route of administration and target tissue engagement
Multiple routes of MSC administration have been reported, with intravenous, intramuscular, intrathecal, and intranasal delivery representing the most frequently studied approaches. These routes differ substantially in terms of invasiveness, anatomical targeting, biodistribution, and dominant mechanism of action. Consequently, route selection represents a critical biological determinant of therapeutic outcome rather than a purely technical consideration.
Intravenous administration is the most applied route in clinical trials, particularly for systemic inflammatory and vascular conditions. Clinical studies have reported therapeutic effects in COVID-19, ischemic stroke, recessive dystrophic epidermolysis bullosa, atopic dermatitis, diabetic foot ulcer, and peripheral arterial disease.16,19,20,22,24,26 These disorders often involve systemic immune dysregulation or widespread tissue injury, making systemic delivery biologically plausible. However, intravenously infused MSCs undergo substantial pulmonary sequestration shortly after administration, a phenomenon often described as the first-pass effect, which may limit direct homing to distal organs. This suggests that clinical benefit may primarily result from systemic immunomodulation rather than durable engraftment at the site of injury.
Intramuscular administration is generally selected when localized or regional effects are desired, such as in Buerger’s disease, 45 diabetic foot ulcer, 40 and critical limb ischemia. 41 In diabetic peripheral neuropathy, intramuscular injection has also been applied to support neurotrophic effects within affected tissues. 42 Experimental evidence indicates that intramuscularly injected umbilical cord-derived MSCs can persist for several months while remaining functionally active and secreting therapeutic factors, as demonstrated by bioluminescence imaging. 46 Such prolonged local activity may enhance paracrine-mediated tissue repair.
Intrathecal administration is primarily used for disorders involving the central nervous system, including spinal cord injury,29,30,33 cerebral palsy,
31
multiple sclerosis,34,35 and ALS.32,36,38 By delivering cells directly into the cerebrospinal fluid as illustrated in Figure 2, this approach increases the likelihood of interaction with neural and glial compartments and avoids the limitations imposed by the blood brain barrier. However, intrathecal injections require lumbar puncture and carry procedural risks,47,48 which may limit its broader applicability. Schematic illustration of intrathecal administration of mesenchymal stromal cells. MSCs are delivered via lumbar puncture into the cerebrospinal fluid within the subarachnoid space, enabling direct access to the central nervous system and bypassing the blood–brain barrier. This figure was created by the authors using CanvaPro (Canva Pty Ltd., Australia).
Compared with other delivery routes, intranasal administration remains relatively novel and has not yet been widely adopted in clinical practice. Although it has been extensively investigated in neurodegenerative disorders, particularly Alzheimer disease, most of the available evidence remains at the preclinical level.
49
Clinical application has been limited, with reported use primarily in perinatal arterial ischemic stroke.
43
Intranasal delivery is of interest because it may enable access to the central nervous system through olfactory and trigeminal pathways as shown in Figure 3, thereby partially circumventing the blood-brain barrier. This approach offers a non-invasive alternative to direct central nervous system administration and may reduce systemic exposure. Preclinical studies suggest that intranasal delivery can enhance central bioavailability while minimizing peripheral distribution.
49
However, variability in nasal anatomy, mucosal integrity, and underlying comorbidities may influence cell transport efficiency. In addition, current clinical evidence remains insufficient to establish standardized protocols or confirm long-term efficacy. Schematic illustration of intranasal delivery of mesenchymal stromal cells. MSCs access the central nervous system through olfactory and trigeminal pathways, partially circumventing the blood–brain barrier and reducing systemic exposure. This figure was created by the authors using CanvaPro (Canva Pty Ltd., Australia).
The route of MSC administration determines biodistribution patterns, target tissue exposure, and the dominant therapeutic mechanism. Systemic delivery may preferentially support immune modulation, whereas localized or central nervous system-directed approaches may enhance tissue-specific effects through increased local bioavailability. Route selection should therefore be aligned with disease pathophysiology, target accessibility, and intended mechanism of action. Strategic matching between delivery route and therapeutic objectives may improve treatment precision, optimize cell survival and distribution, and ultimately enhance clinical efficacy.
4.3. Dose-route interaction and therapeutic implications
MSC-based therapy has demonstrated therapeutic potential across multiple disease categories; however, clinical translation remains constrained by heterogeneity in dosing strategies and delivery routes. Dose and route should not be interpreted independently, as the administered cell number and anatomical delivery site together determine effective tissue exposure. Although clinical data remains limited, preclinical studies provide mechanistic insight into how dose, route, and timing interact to influence therapeutic efficacy.
In animal models of spinal cord injury, direct comparison of intrathecal and intravenous delivery of human umbilical cord-derived MSCs (hUC-MSCs) demonstrated superior functional recovery, reduced lesion volume, and greater suppression of inflammatory responses following high-dose intrathecal administration at 10 × 106 cells per kilogram, compared with intravenous delivery at 20 × 106 cells per kilogram. 50 These findings indicate that effective neuroprotection depends not only on total cell number but also on achieving sufficient local bioavailability at the injury site. A meta-analysis of spinal cord injury animal studies further supports this relationship, showing that higher-dose transplantation of at least 1 × 106 cells, local delivery strategies, and administration during the subacute phase were consistently associated with improved outcomes compared with lower doses, systemic infusion, or acute and chronic phase interventions. 50 Together, these data suggest that dose magnitude, route selection, and treatment timing act synergistically to determine therapeutic response.
Similar dose–route dependencies have been observed in liver injury models. In vivo bioluminescence tracking demonstrated that administration via the superior mesenteric vein at higher doses of 1.0 × 106 or 5.0 × 105 cells enhanced hepatic localization but resulted in portal vein embolization and treatment-related mortality. In contrast, a lower dose of 2.5 × 105 cells achieved effective liver targeting without adverse events, suggesting the presence of a therapeutic window defined by both dose and vascular delivery route. 51 Route comparison further revealed that systemic infusion through the inferior vena cava led predominantly to pulmonary entrapment, whereas superior mesenteric vein or intrahepatic delivery enhanced liver-specific distribution bypassing pulmonary sequestration. These findings demonstrate that excessive dose escalation cannot compensate for suboptimal biodistribution and may introduce safety risks.
Clinical studies in cardiovascular disease provide complementary translational evidence. Localized delivery approaches such as intracoronary administration have been associated with higher myocardial retention and improved cardiac function compared with systemic venous infusion, even when comparable numbers of viable cells were administered. 52 Although these studies primarily emphasize route-dependent differences, they reinforce the concept that effective dose at the target tissue may differ substantially from the total administered dose.
Additional clinical observations in acute myocardial infarction further illustrate this interaction. In a recent report evaluating umbilical cord-derived MSC therapy, intracoronary administration of a fixed dose of 50 million cells was associated with more consistent improvements in left ventricular ejection fraction compared with intravenous delivery using weight-adjusted dosing at 2 × 106 cells per kilogram. 52 Functional assessment using the six-minute walking test also demonstrated greater early improvement in patients receiving intracoronary therapy, particularly within the first six months following treatment. Despite higher total administered cell numbers in the intravenous group, functional recovery was less pronounced, especially in cases of extensive myocardial injury. Although derived from a limited and non-randomized dataset, these findings support the concept that therapeutic response depends not solely on nominal dose but on route-dependent myocardial targeting efficiency.
Functional assessment using the six-minute walking test indicated greater early improvements in patients receiving intracoronary UC-MSCs, especially within the first six months following treatment. While these observations are derived from a limited and non-randomized dataset, they suggest that the therapeutic response to UC-MSC therapy may be influenced not only by the administered dose but also by the route of delivery. These findings provide supportive clinical context indicating that intracoronary administration may facilitate more efficient myocardial targeting in acute myocardial infarction, although further validation in larger, controlled studies is required. 53
Collectively, available preclinical and emerging clinical evidence indicates that therapeutic efficacy depends on the integrated relationship between dose magnitude, delivery route, and disease context. Increasing total cell number alone does not guarantee improved outcomes if biodistribution limits effective tissue exposure. Rational optimization of MSC therapy therefore requires mechanistically informed dose-ranging strategies aligned with route-specific biodistribution patterns and target tissue accessibility.
Taken together, the findings of this review highlight that dose and delivery route should not be considered as independent variables, but rather as interdependent determinants of therapeutic efficacy. The interaction between dose magnitude and route-specific biodistribution appears to play a critical role in shaping clinical outcomes, with localized or targeted delivery approaches often requiring different dosing considerations compared to systemic administration.
In this context, the present review provides an integrative perspective by systematically linking dose, delivery route, and treatment timing as interconnected factors influencing therapeutic response. By synthesizing evidence across diverse clinical indications and study designs, this work extends beyond prior reviews that have typically evaluated these parameters in isolation. Importantly, this integrative framework highlights key translational gaps, including the lack of standardized dosing strategies, inconsistent outcome reporting, and limited data on MSC persistence and biodistribution, which remain major challenges for optimizing clinical efficacy and reproducibility. These insights may support the development of more rational and standardized strategies for MSC-based therapy optimization in future clinical practice.
4.4. Manufacturing and cost considerations in dose selection
Based on the review, several studies have implemented MSCs therapy using range-based dosing regimens. From a manufacturing perspective, this approach is justifiable, as producing products in a limited number of standardized dose batches (e.g., low, medium, and high doses) is more efficient than tailoring exact doses for each individual patient.
The manufacturing process for cell-based therapies is inherently expensive, as the cost is “embedded” within each cell produced. In addition, the complexity of these therapies further increases the manufacturing burden. A review by Ham et al. (2024) reported that a single production batch can yield between 1 and 88 doses, with costs ranging from €23,000 to €190,000 per batch. 54 Given these high production costs, partial use of cell products can substantially increase the effective cost per administered dose. Discarding unused cell fractions represents not only biological waste, but also a loss of embedded manufacturing, quality control, and facility-associated costs. 55
Consequently, strict weight-based dosing that requires highly precise cell numbers may necessitate partial use of a vial, with the remaining cells often discarded. This practice reduces overall manufacturing efficiency and further amplifies cost-related challenges. Therefore, the use of dose ranges, rather than fixed individualized doses, may represent a pragmatic strategy to improve manufacturing efficiency by enabling full utilization of prepared batches while reducing the overall cost per treatment.
4.5. Future directions and limitations
Future research in MSC therapy should prioritize mechanistic refinement of dose–route optimization rather than indiscriminate dose escalation. Strategies aimed at enhancing cell potency, including genetic modification and preconditioning approaches, may improve therapeutic consistency by augmenting paracrine signaling and immunomodulatory capacity. Genetic engineering has been explored to increase secretion of angiogenic, neurotrophic, or anti-inflammatory factors, whereas priming under hypoxic or inflammatory conditions may enhance responsiveness to specific disease microenvironments. While these approaches hold potential, their integration into clinical protocols requires careful evaluation of safety, scalability, and regulatory considerations.
Advances in delivery technologies may also improve effective tissue exposure. Sustained release systems, biomaterial scaffolds, or repeated administration strategies could enhance local retention and prolong biological activity. However, these innovations must be evaluated within structured dose ranging frameworks to determine whether enhanced persistence translates into meaningful clinical benefit.
Despite these advances, several limitations in the current body of evidence and in this review should be acknowledged. Many included studies were early-phase trials with small sample sizes, heterogeneous patient populations, and variable follow-up duration, which may limit generalizability of the findings. In addition, inconsistent reporting of dosing strategies, timing of administration, and outcome measures limited cross-study comparability and precluded formal quantitative meta-analysis. Emerging routes such as intranasal and scaffold-based delivery remain underrepresented in large-scale clinical trials, restricting definitive conclusions regarding their relative efficacy. Furthermore, substantial variability in cell source, manufacturing processes, potency characterization, and route-specific protocols further complicates interpretation. Standardized reporting of dose definitions, including total administered cells, weight-adjusted dosing, delivery route, timing relative to disease stage, and frequency of administration, will be essential to facilitate meaningful comparison across studies. Establishing harmonized methodological frameworks represents a critical step toward evidence-based optimization of MSC therapy.
From a methodological perspective, this review also has limitations, including the absence of a formal risk of bias assessment and the potential for selection bias due to database restrictions and predefined inclusion criteria.
4.6. Conclusion
MSC-based therapies continue to demonstrate a favorable safety profile and broad therapeutic potential across diverse clinical indications. However, their clinical efficacy remains inconsistent, largely due to substantial heterogeneity in dosing strategies, routes of administration, treatment timing, and product-related variables. The findings of this review highlight that dose and delivery route should not be considered as independent parameters, but rather as interdependent determinants that collectively influence biodistribution, target tissue exposure, and therapeutic outcomes.
Accordingly, despite encouraging clinical signals, the absence of standardized frameworks for dose optimization, route selection, and outcome reporting remains a major barrier to reproducibility and clinical translation. Furthermore, the limited availability of data on MSC persistence, engraftment, and in vivo behavior continues to constrain mechanistic understanding and cross-study comparability.
Overall, these challenges underscore the need for greater harmonization in clinical design, dosing strategies, and reporting standards to enable more reliable evaluation of MSC-based therapies in clinical settings.
Supplemental material
Supplemenal material - Optimizing dose and delivery route in mesenchymal stromal cells (MSCs)-based therapy: A systematic review of their implications for clinical efficacy
Supplemenal material for Optimizing dose and delivery route in mesenchymal stromal cells (MSCs)-based therapy: A systematic review of their implications for clinical efficacy by Cynthia Retna Sartika, Rima Haifa, Angliana Chouw, Atikah Anwar Hasibuan, Karina Kalasuba1 and Lestari Mahardika Urbaningrum in Cell Transplantation.
Footnotes
Acknowledgements
The authors would like to thank Prodia StemCell Indonesia (ProSTEM) Laboratory, Jakarta, Indonesia, for administrative and technical support during the preparation of this manuscript.
Ethical considerations
This study is a narrative review and does not involve any new studies with human participants or animals.
Authors Contributions
Conceptualization: CRS, RH, AAH; Methodology: CRS, AC, RH, LMU; Data Curation: AAH, RH, LMU, KK; Writing – Original Draft: CRS, AAH, RH, LMU, KK; Writing – Review & Editing: CRS, AC, RH, KK, LMU; Supervision: CRS, AC, RH; Supervision: CRS, AC; Visualization: LMU, KK: Project Administration: CRS, AAH, RH.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by PT. Prodia StemCell Indonesia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
AI policy statement
The authors declare that no artificial intelligence (AI) tools were used in the preparation, writing, or editing of this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.