
Abstract
This study aimed to define the incidence of Clostridioides difficile infection (CDI), identify its risk factors, and evaluate its association with early post-transplant complications and overall clinical outcomes. To characterize CDI in the allogeneic hematopoietic stem cell transplantation (allo-HSCT) setting, we retrospectively analyzed a cohort of 539 recipients who experienced diarrhea in the peri-transplant period (from conditioning to discharge from laminar flow). Among these diarrheic recipients, 64 patients developed CDI, the cumulative incidence of CDI was 12.1%, with a median onset of day -1 (range, -7 to +26) relative to HSCT. In a multivariate analysis, older age was independently associated with a lower risk of CDI (HR, 0.97; P = 0.008) among diarrheic recipients. The incidence of CDI stratified by the median onset time revealed that pre-transplant CDI was an independent risk factor for grade 1-4 lower gastrointestinal acute graft-versus-host disease (lower-GI aGVHD) (HR, 2.43; P=0.024). Furthermore, pre-transplant CDI was associated with a markedly increased risk of severe fungal infection (HR,6.97; P=0.026) and 100-day non-relapse mortality (NRM) (HR, 3.13; P=0.046). In conclusion, this study highlights a critical, timing-dependent distinction in CDI-associated severe complications and mortality in allo-HSCT recipients with diarrhea.

Keywords
Introduction
Clostridioides difficile (C. difficile), a spore-forming, anaerobic, Gram-positive bacterium, represents a significant pathogen implicated in healthcare-associated infections. 1 The clinical presentation of Clostridioides difficile infection (CDI) ranges from mild diarrhea to toxic megacolon and, in severe cases, can be fatal.2,3 The risk of CDI in hematopoietic stem cell transplantation (HSCT) recipients is up to nine times higher than that observed in the general population. 4 The incidence of CDI has been reported in allogeneic HSCT (allo-HSCT) recipients ranging from 9% to 31.2%.4–10
The relationship between CDI and acute graft-versus-host disease (aGVHD), a common complication following allo-HSCT, remains controversial. While a significant association between CDI and aGVHD, particularly gastrointestinal (GI) and severe forms of aGVHD, has been suggested by some studies,6,11–18 other studies have failed to identify such a link.4,8,19–24 Similarly, the impact of CDI on post-transplant prognosis is contested, with conflicting conclusions having been reported. For instance, several studies have found no significant effect of CDI on overall survival or mortality rates.6–9,13,21,24,25 In contrast, other studies suggest that CDI is associated with a poorer prognosis, with some reports indicating significantly shorter overall survival in CDI patients compared with non-CDI patients. 26 The relationship between CDI and other infectious complications has been less thoroughly investigated. One study reported that although CDI was not significantly associated with multidrug-resistant organism (MDRO) colonization or bloodstream infection (BSI), a higher rate of infection-related mortality was observed among CDI patients compared to non-CDI patients. In contrast, mortality among individuals without CDI was primarily attributed to disease relapse. 21 Additionally, an increased incidence of BSI has also been documented in patients with CDI compared to control groups. 17
In summary, the existing evidence on the role of CDI in allo-HSCT recipients is characterized by divergent findings. To elucidate this issue further, a retrospective analysis was conducted on allo-HSCT recipients who underwent diarrhea at our center. The objective of this study is therefore to investigate CDI in this population, including its incidence, risk factors, and effects on early post-transplant complications and clinical outcomes.
Methods
Design of the study
This was a single-center, retrospective cohort study conducted at the Bone Marrow Transplantation Center, the First Affiliated Hospital, Zhejiang University School of Medicine. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics review committee of the First Affiliated Hospital of Zhejiang University School of Medicine. Data were retrospectively collected from patient charts and electronic medical record systems.
The inclusion criteria were as follows: (1) underwent allo-HSCT at our center between January 2021 and December 2023; and (2) developed diarrhea (three or more unformed stools within a 24-hour period 27 ) during the peri-transplant period (from the initiation of the conditioning regimen until discharge from the laminar airflow unit). The exclusion criteria included: (1) a pre-existing history of CDI with ongoing treatment upon admission for HSCT; (2) resolution of diarrhea following treatment for another identified pathogen of diarrhea, which precluded the need for CDI testing; and (3) incomplete clinical records.
Definitions and endpoints
CDI was defined as the occurrence of diarrhea accompanied by a positive stool test result for C. difficile during the peri-transplant period. The stool samples were tested for glutamate dehydrogenase (GDH) and toxins A/B based on enzyme-linked immunosorbent assay (EIA) method. The test for C. difficile considered positive when both glutamate dehydrogenase (GDH) and toxins A/B were detected. The history of severe infection, antibiotic therapy and usage of steroids were evaluated within 100 days prior to the conditioning regimen. Only the administration of a cumulative dose ≥0.5mg/kg of methylprednisolone or equivalent other steroids for at least 7 consecutive days was considered steroid use. Patients who had used one of the following for at least 7 consecutive days: carbapenem, β-lactam/β-lactamase inhibitors, fluoroquinolone, and glycopeptide were considered to have a history of antibiotic therapy.
The primary endpoint of the study was the relationship of lower-GI aGVHD incidence with CDI, second endpoints were severe infection within 100 days after HSCT and 100-day non-relapse mortality (NRM). Lower-GI aGVHD was defined as GVHD targeting the lower gastrointestinal tract that occurred within 100 days after allo-HSCT. Lower-GI aGVHD was diagnosed based on clinical symptoms and/or biopsy and graded according to the MAGIC criteria. 28 The diagnosis of severe infection was followed by the criteria described previously. 29 According to 2016 IDSA and 2021 EORTC/MSG criteria, all proven or probable invasive fungal infection were defined as fungal severe infections. If multiple severe infections occurred, only the first episode was accounted for the purpose of the study. NRM was defined as death from any cause except relapse. Relapse was defined bone marrow (BM) blasts of ≥ 5%, recurrence of blasts in blood, development of extramedullary disease, or development of worsening cytopenias. 30
Transplant procedure
As previously described, conditioning regimens incorporated myeloablative conditioning (MAC) regimen of Busulfan/Cyclophosphamide (Bu/Cy) and reduced-intensity conditioning (RIC) regimen of either Fludarabine/Busulfan (Flu/Bu) or Fludarabine/Melphalan (Flu/Mel).31,32 Graft-versus-host disease (GVHD) prophylaxis consisting of cyclosporin A, methotrexate, and low-dose mycophenolate mofetil was administered to patients. Rabbit antithymocyte globulin (ATG; Thymoglobulin, Genzyme, Cambridge, MA, USA) was administered to patients receiving HID-HSCTs or URD-HSCTs. 31 Peripheral blood stem cells (PBSC) were mobilized with G-CSF without ex vivo T-cell depletion. BM grafts were collected by BM aspiration. Patients diagnosed with aplastic anemia received a combined graft of BM and PBSC, while other patients received PBSC alone. All grafts were unmanipulated. During the peri-transplant period, standard supportive care included the routine administration of proton pump inhibitors (PPIs) for gastric protection and trimethoprim-sulfamethoxazole (TMP-SMX) for prophylaxis against opportunistic pathogens. Additionally, patients presenting with fever or infection received broad-spectrum antibiotics, such as β-lactam/β-lactamase inhibitors and carbapenems.
Stool screening for C. difficile was routinely performed on all patients who developed diarrhea during the peri-transplant period. Patients diagnosed with CDI received oral vancomycin as the standard first-line therapy. In accordance with an institutional surveillance protocol, weekly rectal swabs were collected from all patients during the peri-transplant period, irrespective of diarrheal symptoms, to screen for carbapenem-resistant Enterobacteriaceae (CRE) colonization. The collected swabs were inoculated onto Columbia blood agar for microbial identification, followed by antibiotic susceptibility testing. Patients with a positive rectal swab for CRE were consequently defined as colonized.
Statistics analysis
Continuous variables are presented as median (range). Differences between cohorts were analyzed using Student’s t-test or Mann-Whitney U test. Categorical variables are expressed as frequencies (percentages) and were compared using Pearson χ 2 test, χ 2 test with continuity correction, or Fisher exact test. The cumulative incidence of CDI, GI aGVHD, severe infection, and NRM was estimated via competing risks analysis using Fine and Grey’s regression models. 33 A landmark analysis was performed at day +15. Variables with a p-value <0.2 in univariate analyses, along with clinically relevant variables, were included in the multivariate model. All analyses were performed using SPSS version 27.0 (SPSS, IBM Corp., Chicago, IL, USA) and R language statistical software (https://www.r-project.org/). All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant.
Results
Patient characteristics
Between January 2021 and December 2023, a total of 1,158 patients underwent allo-HSCT at the Bone Marrow Transplantation Unit of the First Affiliated Hospital, Zhejiang University School of Medicine. Of the 550 patients who experienced diarrhea during the peri-transplant period, 11 were excluded, including 2 patients who had a history of CDI prior to admission and were still receiving oral vancomycin for treatment after admission for HSCT, 5 patients who achieved resolution of diarrhea following antibiotic therapy initiated after the detection of other pathogens in fecal screening, thus obviating the need for CDI testing, and 4 patients who had incomplete medical records. Consequently, a total of 539 allo-HSCT recipients were retained in the final analysis. Data were retrospectively collected from patient charts and electronic medical record systems. The flowchart of patient selection and exclusion process is detailed in Figure 1. Flow diagram of patient enrollment.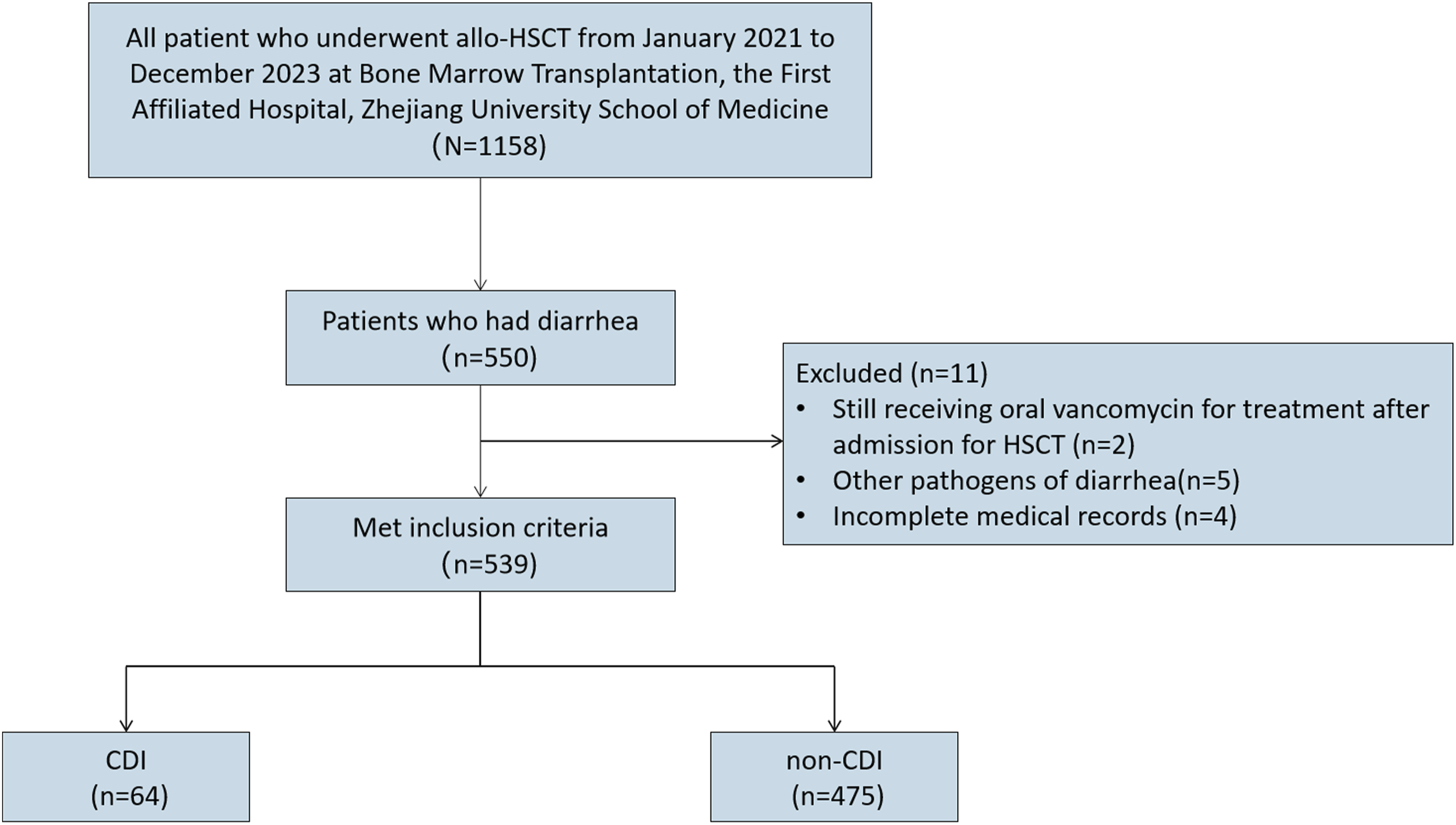
Characteristics of patients who underwent allo-HSCT.

Abbreviations: AML, acute myeloid leukemia; ALL, acute lymphoblastic leukemia; CR1, first complete remission; CR2, second complete remission; >CR2, than a second complete remission; CRE, carbapenem-resistant enterobacteriaceae; HID, haploidentical donor; MAC, myeloablative conditioning; MDS, myelodysplastic syndrome; MSD, matched sibling donor; NR, no remission; RIC, reduced-intensity conditioning; URD, unrelated donor.
Variable correlation
A correlation coefficient matrix was generated for all variables to assess for multicollinearity and reduce variable redundancy (Table S1). As detailed in Table S1, strong correlations were observed between several variable pairs, including: (a) patient sex and the female donor-to-male patient pairing, as well as between donor sex and this pairing; (b) history of steroid use and underlying disease, and between conditioning regimen and underlying disease; (c) history of antibiotic therapy and exposures to specific antibiotic classes (including β-lactam/β-lactamase inhibitors, fluoroquinolones, glycopeptides, and carbapenems); (d) carbapenem exposure and exposures to other antibiotic classes (including β-lactam/β-lactamase inhibitors, fluoroquinolones, and glycopeptides); and (e) donor type and GVHD prophylaxis. For each collinear set, the variable with the greatest clinical or biological plausibility was retained for subsequent analyses.
Incidence and risk factors for CDI
Univariate and multivariate analyses of factors associated CDI.

Abbreviations: CR1, first complete remission; CR2, second complete remission; >CR2, more than a second complete remission; HID, haploidentical donor; MAC, myeloablative conditioning; MSD, matched sibling donor; NR, no remission; RIC, reduced-intensity conditioning; URD, unrelated donor.
A multivariate analysis was performed to adjust for potential confounding variables and to isolate independent predictors of CDI. After this adjustment, only increasing patient age remained independently associated with a reduced risk of CDI (HR = 0.97, 95% CI: 0.95-0.99, P=0.008), corresponding to a 3% decrease in risk per additional year of age (Table 2).
Lower-GI aGVHD
Univariate and multivariate analysis of lower-GI aGVHD.

Abbreviations: CDI, Clostridioides difficile infection; CR1, first complete remission; CR2, second complete remission; >CR2, more than a second complete remission; CRE, carbapenem-resistant enterobacteriaceae; HID, haploidentical donor; MAC, myeloablative conditioning; MDS, myelodysplastic syndrome; MSD, matched sibling donor; NR, no remission; RIC, reduced-intensity conditioning; URD, unrelated donor.
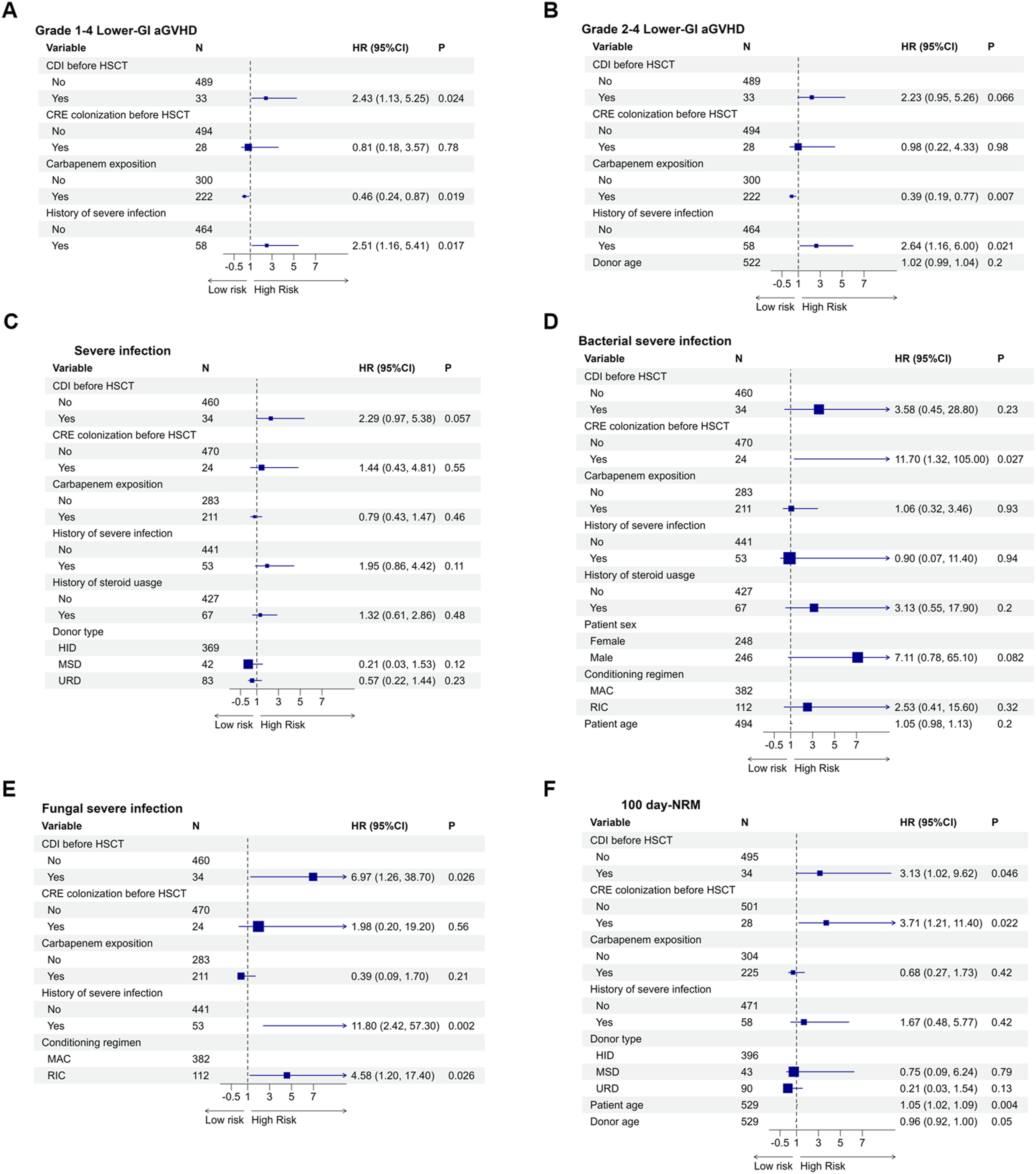
The 100-day cumulative incidence of grade 1-4 lower-GI aGVHD was significantly higher in patients with pre-HSCT CDI compared to those without CDI before HSCT (21.2% [95% CI, 9.2%-36.5%] vs. 9.4% [95% CI, 7.0%-12.2%]; P = 0.036) (Figure 2(a)). Univariate analysis indicated that pre-HSCT CDI was associated with an increased risk of subsequent grade 1-4 lower-GI aGVHD (HR = 2.29, 95% CI: 1.07-4.92, P = 0.033) (Table 4). This association remained statistically significant in the multivariate model after adjusting for pre-HSCT CRE colonization, carbapenem exposure and a history of severe infection (HR = 2.43, 95% CI: 1.13-5.25, P = 0.024) (Figure 3(a)). For grade 2-4 GI aGVHD, the 100-day cumulative incidence rates were 18.3% (95% CI, 7.3%-33.3%) and 8.6% (95% CI, 6.4%-11.3%) for patients with and without pre-HSCT CDI, respectively (Figure 2(b)).In the multivariate analysis, after adjusting for variables including pre-HSCT CRE colonization, history of severe infection, carbapenem exposure and donor age, pre-HSCT CDI was suggestive of a trend toward a greater than 2-fold increased risk of grade 2-4 lower-GI aGVHD (HR = 2.23, 95%CI: 0.95-5.26, P = 0.066) (Figure 3(b)). In contrast, CDI occurring post-HSCT showed no association with the development of either grade 1-4 or grade 2-4 GI aGVHD. The impact of CDI before HSCT on early complications and prognosis following allo-HSCT. Subgroup analysis of lower-GI aGVHD, severe infection and 100-day NRM. Abbreviations: CDI, Clostridioides difficile infection; GI aGVHD, gastrointestinal acute graft-versus-host disease; NRM, non-relapse mortality. Forest plot for multivariable analysis of outcomes.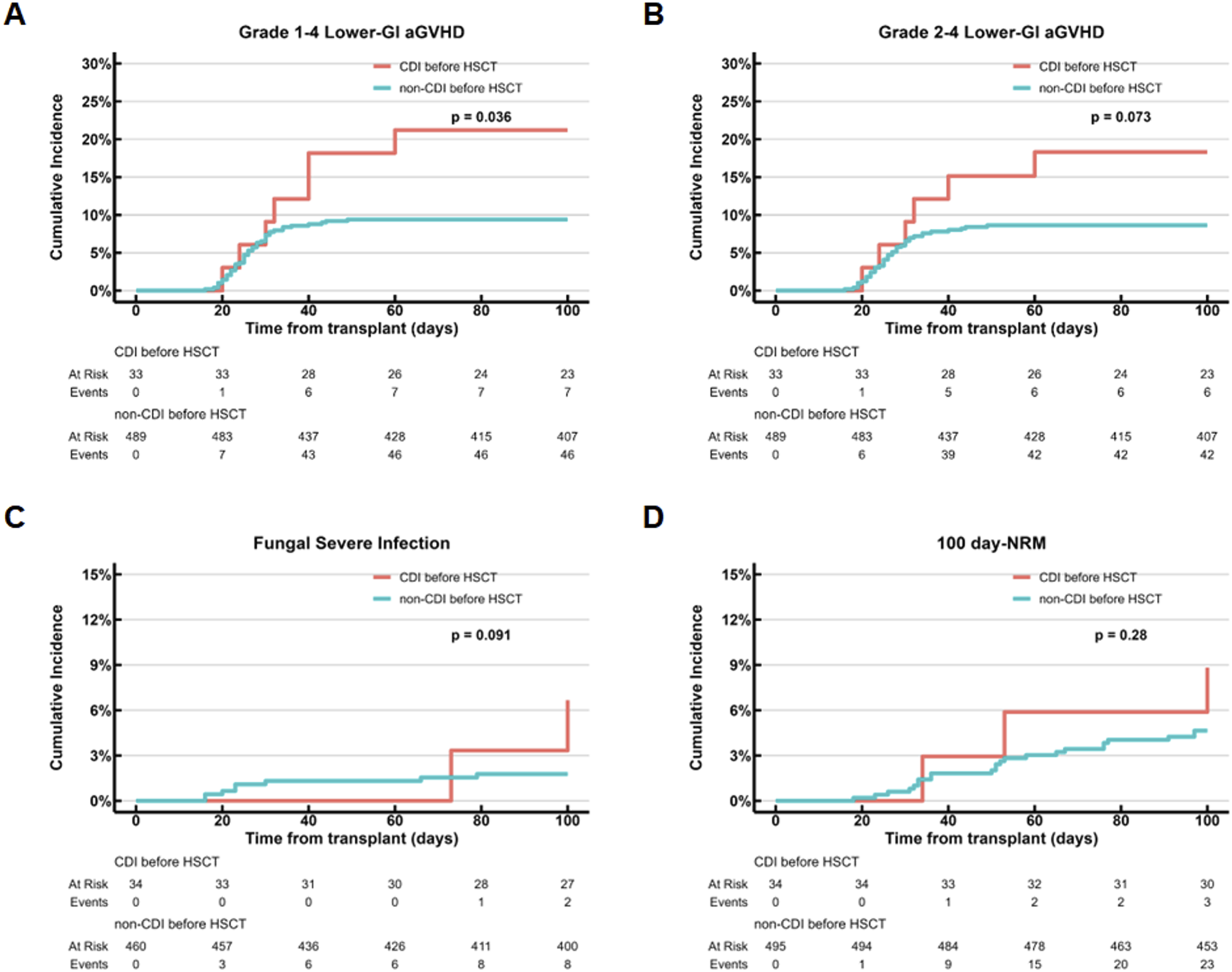

Severe infection
The results of the analyses for severe infection are presented in Table S2. Analyses of the overall cohort and the stratified subgroups revealed no significant associations between CDI and the overall risk of severe infection within 100 days post-HSCT (Figure 3(c)–(e)) (Table 4).
However, in a further analysis stratified by pathogen type among allo-HSCT recipients with diarrhea, pre-HSCT CDI was identified as an independent risk factor for severe fungal infection in the multivariate model following adjustment for pre-HSCT CRE colonization, history of severe infection, carbapenem exposition and the conditioning regimen (HR = 6.97, 95% CI: 1.26-38.7, P = 0.026) (Figure 3(e)). No significant associations were observed between pre-HSCT CDI and severe bacterial infection (Table 4). As no events of bacterial or fungal severe infection occurred in the post-HSCT CDI group, the impact of this subgroup could not be evaluated.
Additionally, while pre-HSCT CRE colonization was associated with an increased risk of severe bacterial infection in the univariate analysis (HR = 6.67, 95% CI: 1.34-33.2, P = 0.020), this association remained significant in the multivariate model (HR = 11.70, 95% CI: 1.32-105, P = 0.027) (Figure 3(d)).
100-Day NRM
The results of the analyses for 100-day NRM are presented in Table S3. Among patients experiencing diarrhea during the peri-transplant period, the multivariate model identified pre-HSCT CDI as a significant independent risk factor for this outcome (HR = 3.13, 95% CI: 1.02-9.62, P = 0.046) (Figure 3(f)). Other independent predictors of 100-day NRM included pre-HSCT CRE colonization (HR = 3.71, 95% CI: 1.21-11.4, P = 0.022) and increasing patient age (HR = 1.05, 95% CI: 1.02-1.09, P = 0.004) (Figure 3(f)). As no NRM events occurred in the post-HSCT CDI or post-HSCT CRE groups, their associations with 100-day NRM could not be evaluated.
Discussion
In this study, for allo-HSCT recipients with diarrhea, CDI occurring specifically during the pre-transplant conditioning period as an independent risk factor for the subsequent GI aGVHD, severe fungal infection and 100 days NRM.
In contrast to previously published reports, our study is distinguished by its stringent screening and diagnostic criteria. Specifically, our cohort was intentionally restricted to patients who developed diarrhea during the peri-transplant period. This approach aligns with clinical guidelines that recommend limiting C. difficile testing to symptomatic HSCT recipients. 34 The cumulative CDI incidence of 12.1% (95% CI: 9.5%–15.1%) observed specifically in our restricted cohort of patients with diarrhea suggests that the overall CDI incidence across our entire allo-HSCT population is likely substantially lower than the 10% to 12.1% rates reported in unselected cohorts.6,22,23 In our center, C. difficile detection is based on the EIA method for GDH and toxins, whereas other centers utilize the Nucleic Acid Amplification Test (NAAT) for toxin genes. The lower sensitivity of the EIA may account for this reduced incidence.
A further notable feature of this study is the composition of the patient population, which was characterized by a predominance of patients who received grafts from haploidentical donors (400/539, 74.2%). This proportion is substantially higher than the 2.9% to 35% reported in previous studies,4,6,12,13,20–22 making this the largest reported cohort of HID recipients in the context of CDI research to our knowledge.
We identified a novel and unexpected association, demonstrating that younger patients exhibited a higher susceptibility to peri-transplant CDI among allo-HSCT recipients with diarrhea. To further investigate the potential reasons for this observation, we stratified patients into two groups using 41 years as the cutoff. A comparative analysis of their primary diseases, pre-transplant infection-related factors, and conditioning regimens was conducted, with detailed data presented in Table S4. The results indicated that younger patients had a significantly higher likelihood of pre-transplant steroid and MAC regimens. Age in this context may not be a direct causal factor but rather a surrogate for other underlying variables that are the true determinants of CDI risk. In addition, our study found no significant link between CDI and carbapenem exposure, a history of severe infection, or the use of a MAC regimen, a finding that contrasts with several established studies.6,9,13,19,23 Given that diarrhea often serves as a clinical marker reflecting the cumulative effects of pre-transplant therapy, systemic health status, intestinal environment and the conditioning regimen, it is plausible that baseline differences between diarrheic and non-diarrheic patients could introduce bias into the analysis of CDI risk factors. The restriction of our cohort to only patients with diarrhea likely minimized such baseline heterogeneity, which may explain why no significant differences in the aforementioned variables were detected between the CDI and non-CDI groups.
The bidirectional relationship between GI aGVHD and CDI is underpinned by complex pathophysiological mechanisms that have been extensively investigated. mucosal barrier damage induced by CDI triggers a pro-inflammatory cascade14,35,36 that not only initiates or exacerbates GI aGVHD but also facilitates the translocation of bacteria across the gut epithelium, further intensifying the infection. 37 This intricate interplay constitutes a vicious cycle, rendering the determination of causality in multivariate analyses particularly challenging. 5 Our study was designed to address this question, and revealed that patients who developed CDI prior to HSCT—at a timepoint characterized by the absence of both engraftment and GVHD—had a significantly elevated risk of subsequent lower gastrointestinal acute GVHD in the cohort of patients experiencing diarrhea during the peri-transplant period.
In addition to pre-HSCT CDI, a history of severe infections within 100 days prior to the conditioning regimen was identified as an independent risk factor for lower-GI aGVHD in this study. The gut microbiota serves as the primary reservoir for pathogens in most cases of sepsis, and severe infections further compromise the intestinal mucosal barrier. 38 Patients with a history of severe infection possess a more profoundly impaired gut microenvironment than those without such a history, rendering them more susceptible to lower-GI aGVHD. These findings reinforce our findings regarding the critical role of gut dysbiosis in both infections and gastrointestinal aGVHD. Contrary to the widely accepted consensus, pre-HSCT carbapenem exposure emerged as a protective factor against gastrointestinal aGVHD among patients experiencing diarrhea within the peri-transplant period in the present study. Although these patients had a history of carbapenem exposure for at least 7 consecutive days, the administration of carbapenems rather than advanced antibiotics like tigecycline or polymyxin indicates that these infections were relatively manageable. Consequently, carbapenem exposure in this cohort may reflect a history of highly controllable infections rather than indicating a severely degraded state of intestinal homeostasis.
Furthermore, the analytical scope of our study was extended beyond the commonly investigated association between CDI and subsequent BSI to include severe infections from any anatomical site caused by all categories of pathogens. This broader approach revealed that pre-transplant CDI was also a significant independent risk factor for severe fungal infection in multivariate analysis (HR = 7.46, 95% CI: 1.08-51.7; p = 0.042). The observed associations between CDI and both gastrointestinal GVHD and severe fungal infections may be explained by the fact that CDI serves as a clinical marker of intestinal dysbiosis, which reflects greater pre-transplant comorbidity or underlying disease severity.6,19 This interpretation is further supported by our finding that both pre-transplant CDI and CRE colonization, a recognized consequence of gut dysbiosis, were associated with an increased risk of 100-day non-relapse mortality (NRM). Taken together, the observed associations between pre-transplant CDI and both subsequent severe complications and mortality suggest that the current paradigm of treating CDI reactively after diagnosis may be insufficient to fully abrogate its detrimental impact on transplant outcomes for diarrheic recipients. This finding provides a partial theoretical basis for considering a shift toward primary prevention of CDI in clinical practice.
This study has several limitations. First, restricting our population to patients experiencing diarrhea during the peri-transplant period implies that the observed incidence of CDI and its association with clinical outcomes may not fully represent the general allogeneic hematopoietic cell transplantation population. Second, due to the retrospective design and the reliance on data extracted from electronic medical records, the reported incidence of CDI in our cohort may be an underestimation of the true rate. Third the potential for surveillance bias exists, as the shared clinical manifestation of diarrhea may lead to more frequent evaluations in patients with CDI and consequently a higher detection rate of GI aGVHD.6,13 This bias could lead to spurious associations between CDI and aGVHD. Fourth, evaluating CDI that occurred after transplantation was restricted by the absence of severe events within that specific subgroup. Finally, the relatively small sample size and the limited number of outcome events may have limited the statistical power of our analyses and could constrain the generalizability of the findings.
Conclusions
In conclusion, our study demonstrates that for allogeneic HSCT recipients with diarrhea, particularly those receiving grafts from haploidentical donors, the development of CDI during the conditioning phase is an independent predictor of severe early post-transplant complications. Future prospective studies are warranted to validate whether prophylactic treatment of CDI can meaningfully improve transplant outcomes.
Supplemental material
Supplemental material - Pre-transplant Clostridioides difficile infection predicts subsequent gastrointestinal GVHD and non-relapse mortality after allogeneic hematopoietic stem cell transplantation
Supplemental material for Pre-transplant Clostridioides difficile infection predicts subsequent gastrointestinal GVHD and non-relapse mortality after allogeneic hematopoietic stem cell transplantation by Wenyi Wang, Yibo Wu, Yunbo Chen, Xiaoyu Lai, Lizhen Liu, Jimin Shi, Yanmin Zhao, Luxin Yang, Lin Li, Jian Yu, Huarui Fu, Panpan Zhu, He Huang, Yi Luo in Cell Transplantation
Footnotes
Acknowledgements
We would like to acknowledge the contributions of all members of the study group.
Ethical considerations
This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Zhejiang University School of Medicine in China ([2026B] IIT Ethics Approval No.0572; 14 May 2026).
Consent for participation
Informed consent was obtained from patients in accordance with the Declaration of Helsinki.
Consent for publication
Informed consent for publication was obtained from all patients.
Authors’ contributions
Study concept and design: L.Y. and H.H. Acquisition of the data: W.W.Y., W.Y.B., C.Y.B., L.X.Y., L.L.Z., S.J.M., Z.Y.M., Y.L.X., L.L., Y.J., F.H.R., Z.P.P., H.H., and L.Y. Analysis and interpretation of the data: W.W.Y., W.Y.B., C.Y.B., and L.Y. Writing original draft: W.W.Y. Writing and editing the final manuscript: All authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82300240) and the Zhejiang Provincial Natural Science Foundation of China (LQN25H080002, LMS25H080005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data and material are available upon reasonable request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.