
Abstract
Suicidal and nonsuicidal self-injurious behaviors represent perplexing yet highly prevalent public health problems. Though the behaviors are differentiable, they frequently co-occur. The nature of the association between them, however, remains poorly understood. The interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010) offers one viable framework for enhancing our understanding in this domain. In this review, we provide an overview of the literature on nonsuicidal self-injury, its relation to suicidal behavior, and how the interpersonal theory of suicide conceptualizes this relationship. Alternative perspectives and future directions are also discussed.
Keywords
Introduction
Suicidal and nonsuicidal self-injurious behaviors 1 affect millions of individuals worldwide, representing important public health problems. In the United States, suicide is the 10th leading cause of death, with nearly 100 Americans dying by suicide every day (National Center for Injury Prevention and Control, 2009). Among young adults and adolescents, it is the second and third leading cause of death, respectively (National Center for Injury Prevention and Control, 2009). As for nonsuicidal self-injury (NSSI; i.e., direct, self-inflicted damage of one’s own body tissue without the intent to die and for purposes that are not socially sanctioned; Nock, 2009), prevalence estimates suggest that the behavior occurs among about 4% of adults (Klonsky, Oltmanns, & Turkheimer, 2003), 17% of undergraduates (Whitlock, Eckenrode, & Silverman, 2006), and 14% of adolescents (Ross & Heath, 2002).
Though both involve self-inflicted injury, suicidal behavior and NSSI are differentiable. Distinctions exist with respect to intent, chronicity, methods, cognitions, prevalence, and demographics, among others (Muehlenkamp, 2005; Nock, 2010). Suicidal behavior and NSSI do frequently co-occur, however. Research has consistently indicated elevated rates of suicidal ideation and behavior among individuals who engage in NSSI (Whitlock et al., 2006), placing them at greater risk of death by suicide.
Although the link between suicidal behavior and NSSI is well documented, the nature of the association remains poorly understood. The interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010) offers one viable framework for enhancing the understanding of this issue. Our focus in this review is to provide an overview of the literature on NSSI, its relation to suicidal behavior, and how the interpersonal theory of suicide conceptualizes the relationship. We begin with a short summary of leading models of NSSI, followed by an overview of the interpersonal theory of suicide. We then focus on the relationship between NSSI and suicidal behavior as conceptualized by the theory and discuss alternative perspectives.
Nonsuicidal Self-Injury
Clinicians and researchers have struggled to understand NSSI, and various theories have been proposed to this end. Among these, a functional perspective has emerged as a leading conceptualization, suggesting that NSSI is maintained via reinforcement―intrapersonal or interpersonal, negative or positive (Nock & Prinstein, 2004).
Intrapersonal functions most frequently underlie NSSI (Nock & Prinstein, 2004). NSSI may be negatively reinforced by alleviating negative affect (Chapman, Gratz, & Brown, 2006) or aversive self-perceptions (Heatherton & Baumeister, 1991). NSSI may also be positively reinforced by generating desired feelings or sensations, such as sensations that counteract emotional numbing or dissociation (Klonsky, 2007). For some, NSSI has interpersonal functions: It may facilitate escape from undesired situations and thus be maintained through negative reinforcement, or elicit desired responses from others and thus be positively reinforcing (Nock & Prinstein, 2004).
Despite its emotional and social regulatory functions, NSSI increases risk of suicidal behavior. Although both behaviors involve self-inflicted injury and commonly co-occur, differences between them are well documented. In addition to being characterized by an absence of suicidal intent, NSSI is often associated with thoughts of relief that do not involve perceptions of death. NSSI is also more frequent and chronic, often involving multiple low-lethality methods, whereas serious suicidal behavior often consists of a discrete occurrence using more lethal methods. NSSI is most common in adolescents, with equal rates between genders, whereas women have higher rates of suicide attempts and men have higher suicide death rates (Muehlenkamp, 2005; Nock, 2010).
So, the question remains: If NSSI functions for many individuals as a means of alleviating aversive states or enhancing positive ones, why is it that the behavior is associated with suicide attempts and death? Moreover, why do some individuals engage in NSSI and do so repeatedly, despite its daunting and painful nature? The interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010) is one theory that offers a grounding framework that may be useful in answering these questions.
The Interpersonal Theory of Suicide
The interpersonal theory of suicide (Joiner, 2005; Van Orden et al., 2010) holds that individuals die by suicide because they have both the desire to die and the capability to attempt to do so. The theory includes four main hypotheses concerning the underlying causal processes resulting in suicidal behavior (Fig. 1).
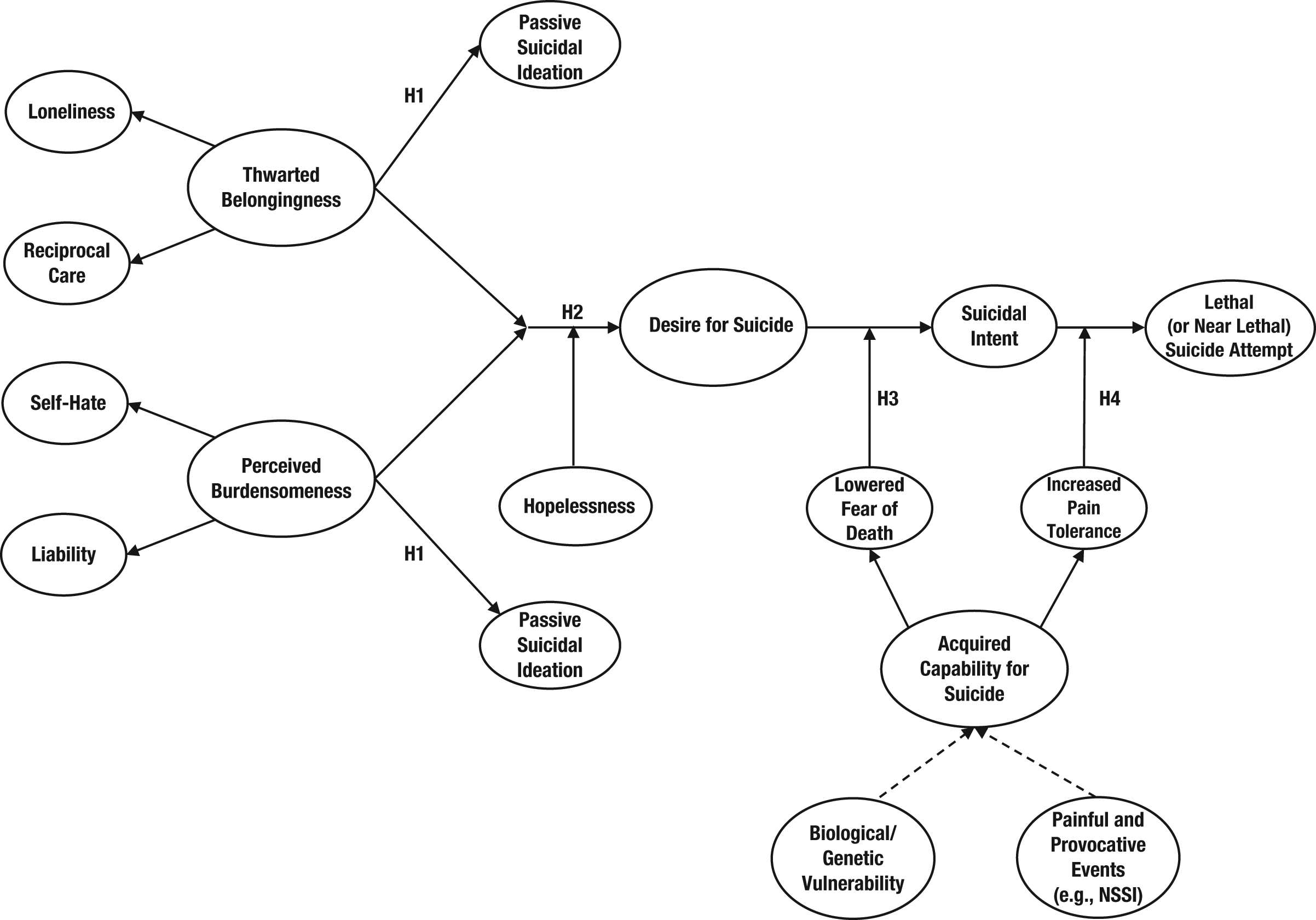
Causal pathway to suicidal behavior, as conceptualized by the interpersonal theory of suicide. NSSI = nonsuicidal self-injury; H1 = Hypothesis 1; H2 = Hypothesis 2; H3 = Hypothesis 3; H4 = Hypothesis 4. Adapted from “The Interpersonal Theory of Suicide,” by K. A. Van Orden, T. K. Witte, K. C. Cukrowicz, S. R. Braithwaite, E. A. Selby, and T. E. Joiner Jr., 2010, Psychological Review, 117, p. 588. Copyright 2010, American Psychological Association. Adapted with permission.
According to the theory’s first hypothesis, experiencing either complete perceived burdensomeness or thwarted belongingness elicits passive suicidal ideation. Thwarted belongingness is defined by loneliness and a lack of reciprocally positive relationships. Perceived burdensomeness refers to misperceptions of being a burden on close others and is characterized by self-hatred as well as a belief that one is a liability for others. Both states are dynamic, responding to both interpersonal and intrapersonal (e.g., mood, schemas) factors (Joiner, 2005; Van Orden et al., 2010). Consistent with the theory, associations of suicidal ideation with perceived burdensomeness (Joiner et al., 2002; Van Orden, Lynam, Hollar, & Joiner, 2006) and thwarted belongingness (Conner, Britton, Sworts, & Joiner, 2007) are well documented.
The joint experience of these states confers greater risk for suicidal ideation than the experience of either one alone, according to the theory. This effect holds even after controlling for strong covariates, including severity of depressive symptoms (Joiner et al., 2009; Van Orden, Witte, Gordon, Bender, & Joiner, 2008). When these combined states are perceived as stable and unchanging (i.e., hopeless), an active desire for suicide will develop—this idea forms the basis for the theory’s second hypothesis. This hypothesis draws from the literature on the relationship between feelings of hopelessness and suicide; however, the effect of specific hopeless cognitions regarding belongingness and burdensomeness on suicidal behavior has yet to be directly researched.
Recognizing that engaging in suicidal behavior is difficult because it requires people to stare down basic self-preservation instincts, the theory proposes that the ability to engage in suicidal behavior must be developed, which happens with repeated exposure to stimuli that are fearsome and painful. Once developed, the acquired capability engenders a sense of fearlessness about pain, injury, and death, as well as an increased pain tolerance necessary for suicidal behavior.
According to the theory’s third hypothesis, suicidal desire will escalate to suicidal intent only if an individual has the requisite levels of fearlessness about the pain, injury, and death associated with suicidal behavior. In addition. because suicidal behavior is physically painful, 2 translating intent into behavior requires the ability to withstand the physical pain involved in suicide. Therefore, the theory’s fourth hypothesis holds that serious suicidal behavior will occur only when the desire to die by suicide is accompanied by the capability to do so.
Though it has yet to be tested fully, initial support for the fourth hypothesis exists. Van Orden and her colleagues (2008) found that the highest levels of clinician-rated suicide risk were associated with high levels of acquired capability for suicide and perceived burdensomeness. Further, Joiner and his colleagues (2009) demonstrated that thwarted belongingness, perceived burdensomeness, and the acquired capability for suicide (as indexed by past suicide attempts) predicted current suicide-attempt status. There were notable limitations of both studies, however. Despite using direct assessments of the constructs, the first study failed to use prospective suicidal behavior as an outcome variable. Although the second study improved on this, its use of proxy measures to index theory constructs raises concerns. Therefore, longitudinal studies predicting suicidal behavior using direct assessments of the constructs are needed.
The Interpersonal Theory on the Co-occurrence of NSSI and Suicide
Resting on the tenets of opponent-process theory (Solomon, 1980), the interpersonal theory of suicide proposes that repeated exposure to a painful and provocative stimulus will result in a decrement in the original response (e.g., fear and pain) and an increase in the response of the opposite valence (e.g., relief and analgesia)–this is viewed as the process underlying the development of the capability for suicide. Over time, behaviors that were once frightening and painful (e.g., self-injury) become less so. NSSI, therefore, can be conceptualized as one highly salient risk factor for developing the capability for suicide.
Consistent with this perspective, indirect evidence has indicated that attenuated perceptions of pain and increased pain tolerance are associated with self-injury. This pattern is observed when past suicide attempters are compared with nonsuicidal controls, psychiatric inpatients, and victims of accidental injuries (Orbach, Mikulincer, King, Cohen, & Stein, 1997; Orbach, Palgi, et al., 1996; Orbach, Stein, et al., 1996). Similarly, individuals who engage in NSSI often report experiencing little or no pain while doing so (Schmahl et al., 2006) and evidence greater tolerance for pain. For instance, women diagnosed with borderline personality disorder (BPD) who engage in NSSI have been shown to have higher pain thresholds and greater pain tolerance than BPD patients without a history of NSSI (Kemperman, Russ, & Shearin, 1997), depressed inpatients (Russ, Campbell, Kakuma, Harrison, & Zanine, 1999), and noninjuring controls (Bohus et al., 2000). Even in the absence of a BPD diagnosis, individuals with histories of NSSI have been found to have aberrant perceptions of pain (Bresin & Gordon, 2011; Bresin, Gordon, Bender, Gordon, & Joiner, 2010).
When examined directly, results have indicated that pain tolerance mediates the relationship between the frequency of self-reported painful and provocative experiences (PPEs) and acquired capability for suicide (Bender, Gordon, Bresin, & Joiner, 2011; Franklin, Hessel, & Prinstein, 2011). Further, NSSI in particular has been shown to be an important PPE that directly contributes to the development of the acquired capability via elevated pain tolerance (Franklin et al., 2011).
Opponent-process theory may also explain why individuals repeatedly engage in NSSI despite its being initially painful and frightening. Consistent with this idea are findings of a “rebound” effect, whereby individuals reportedly feel calmer, more relieved, and soothed after NSSI (Gordon et al., 2010). Further, in a study by Franklin and his colleagues (2010), exposure to an NSSI-proxy procedure (i.e., a cold-pressor task) resulted in a shift away from negative affect. Psychophysiological results indicated the shift represented increased positive affect among individuals who did not have a history of NSSI and reduced negative affect among individuals who did. Franklin and his colleagues (2010) speculated that this pattern may reflect an opponent-process mechanism, given that NSSI is initially positively reinforcing and later becomes negatively reinforcing.
It is important to emphasize that although NSSI is a highly salient risk factor for acquired capability for suicide, a history of nonlethal suicidal behavior is a more potent risk factor and arguably the most direct means of developing the capability. According to the interpersonal theory of suicide, escalation from NSSI to nonfatal suicidal behavior is contingent on the intensity of suicidal desire. Although the processes underlying suicidal desire are distinct from those that increase the acquired capability for suicide, the problems that may exacerbate the perceived need for and severity of NSSI (e.g., difficulties coping with feelings of isolation and/or burdensomeness) may also increase suicidal desire, thereby increasing the likelihood of a nonfatal suicide attempt.
Alternative Perspectives on the Co-occurrence of NSSI and Suicide
Alternative perspectives that may explain the relationship between NSSI and suicide are important to consider. Among individuals with emotion dysregulation, for example, NSSI and suicide attempts can both serve to provide relief or an escape from intolerable emotions or aversive mental states. Baumeister (1990) proposed that a marked sense of inferiority triggers the desire to escape from self-awareness and related aversive emotions. As the wish to escape escalates, NSSI or suicide may emerge as means of distraction or ending awareness, respectively. Indeed, escape from aversive states is the primary reason given for engaging in NSSI (Nock & Prinstein, 2004), and escape from intolerable experiences is a leading reason for suicide reported by those who have survived a suicide attempt (Boergers, Spirito, & Donaldson, 1998).
More recently, Franklin, Aaron, Arthur, Shorkey, and Prinstein (2012) found that emotion dysregulation is generally associated with diminished pain perception and accounts for significant variance in the relationship between NSSI and pain tolerance. 3 It is plausible that emotion dysregulation (as opposed to fearlessness, natural diminished pain perception, or PPEs) also makes individuals more willing to engage in a range of self-injurious behaviors (via diminished pain perception), as well as more prone to suicidal ideation (e.g., via feelings of hopelessness, need for escape, or beliefs that one deserves pain or punishment).
Future Directions
Despite the enigmatic nature of suicidal and nonsuicidal self-injurious behaviors, they represent tremendous public health concerns—unfortunately prevalent and associated with high levels of morbidity and mortality. In this review, we have briefly summarized the literature on leading conceptual perspectives of NSSI, as well as one prominent theory of suicidal behavior. We have further discussed how the relationship between NSSI and suicidal behavior is conceptualized by the interpersonal theory of suicide and offered alternative perspectives. We close now with recommendations to guide future research.
Moving forward, more research is needed to test the predictions of the interpersonal theory with regard to how NSSI might confer risk of suicidal behavior. The development of prospective designs for conducting such tests would be particularly useful. Studies aiming to identify moderating factors that either accelerate or delay the development of the acquired capability for suicide are also needed. Continued research integrating psychophysiological and other biological techniques (e.g., Franklin et al., 2010) into experimental designs will likely prove fruitful as well. Research testing competing perspectives on the mechanisms underlying the relationship between NSSI and suicide will be crucial in furthering our understanding of it.
Although in this review we have focused on how NSSI relates to eventual death by suicide, another interesting direction would be an examination of how the predictions of the interpersonal theory and NSSI might relate to more acute risk factors. A growing body of literature suggests that, in addition to direct communications of intent, extreme social withdrawal and three indicators of overarousal—insomnia, nightmares, and agitation—are important indicators of imminent suicide (Fawcett et al., 1990; Ribeiro et al., 2012). Understanding how NSSI might relate to these risk factors may inform treatment and prevention. Furthermore, although the interpersonal theory’s conceptualization of acute risk for suicide is currently underdeveloped, its tenets may generalize to acute risk factors. For instance, marked social withdrawal may be indicative of increased suicidal desire. Acute overarousal may be related to acquired capability for suicide, given that overcoming the fear associated with suicidal behavior likely requires energy, arousal, and resolve.
In short, though recent advances in the understanding of suicidal self-injury and NSSI are beginning to clarify the natures of these behaviors independently and outline the relationship between them, important questions still remain. Continued research is crucial for furthering our understanding of self-injurious behaviors, their treatment, and their prevention.
Recommended Reading
Joiner, T. E., Jr. (2005). (See References). A seminal book introducing the interpersonal theory of suicide.
Van Orden, K. A., Witte, T. K., Cukrowicz, K. C., Braithwaite, S. R., Selby, E. A., & Joiner, T. E., Jr. (2010). (See References). A comprehensive review on the interpersonal theory of suicide and its empirical evidence to date.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.