
Abstract
The origins of modern psychology are deeply rooted in the notion that stressful early-life experiences negatively impact people’s mental health. Emerging work in the field of health psychology suggests that early-life stress also impacts physical well-being. Indeed, those who experienced severe early-life stress as children are more at risk for cardiovascular disease, type 2 diabetes, and cancer compared with those who did not have those early-life experiences. Recent work in the field of psychoneuroimmunology suggests that inflammation may be one mechanism underlying these associations. In this article, we provide a brief overview of the literature on early-life stress and inflammation and how psychological, autonomic, neuroendocrine, and epigenetic responses to the early environment lead to potentiated inflammation in adulthood. We conclude by highlighting the need for health-promotion and disease-prevention programs that are designed to reduce the frequency and severity of early-life stress.
The origins of modern psychology are rooted in the notion that stressful early-life experiences—events that exceed a child’s ability to cope (Cohen, Tyrrell, & Smith, 1991)—negatively impact mental health. Emerging work in both the behavioral and biological sciences has shown that early-life stress also negatively impacts physical well-being (Fagundes, Glaser, & Kiecolt-Glaser, 2013; Miller, Chen, & Parker, 2011; Perroud et al., 2011). Recent research in the field of psychoneuroimmunology suggests that inflammation may be a key biological mechanism explaining the associations between early-life stress and physical health (Miller et al., 2011). 1
Inflammation, Stress, and Health
When the immune system identifies a foreign virus or bacteria, an inflammatory response is mounted, causing white blood cells to accumulate and kill these invaders. This local inflammatory response is vital for maintaining good physical health. However, when inflammation persists and becomes chronic, it causes declines in physical functioning and promotes disease. Higher levels of inflammation, as indicated by inflammatory markers such as C-reactive protein (CRP), fibrinogen (an inflammatory protein), and proinflammatory cytokines (e.g., interleukin 6, or IL-6, and tumor necrosis factor alpha, or TNF-α), are reliable predictors of quality of life, morbidity, and many causes of mortality in older adults (Ershler & Keller, 2000; Kiecolt-Glaser, Gouin, & Hantsoo, 2009; Mills, Parker, Dimsdale, Sadler, & Ancoli-Israel, 2005). Importantly, elevated chronic inflammation is associated with cardiovascular disease, type 2 diabetes, Alzheimer’s disease, osteoporosis, rheumatoid arthritis, periodontal disease, and some cancers (Ershler & Keller, 2000). Chronic systemic inflammation is also an important biological mechanism underlying fatigue, frailty, and disability (Ershler & Keller, 2000; see Fig. 1). Future research will be important for delineating the differential tissue sources of these elevated levels of systemic inflammation.
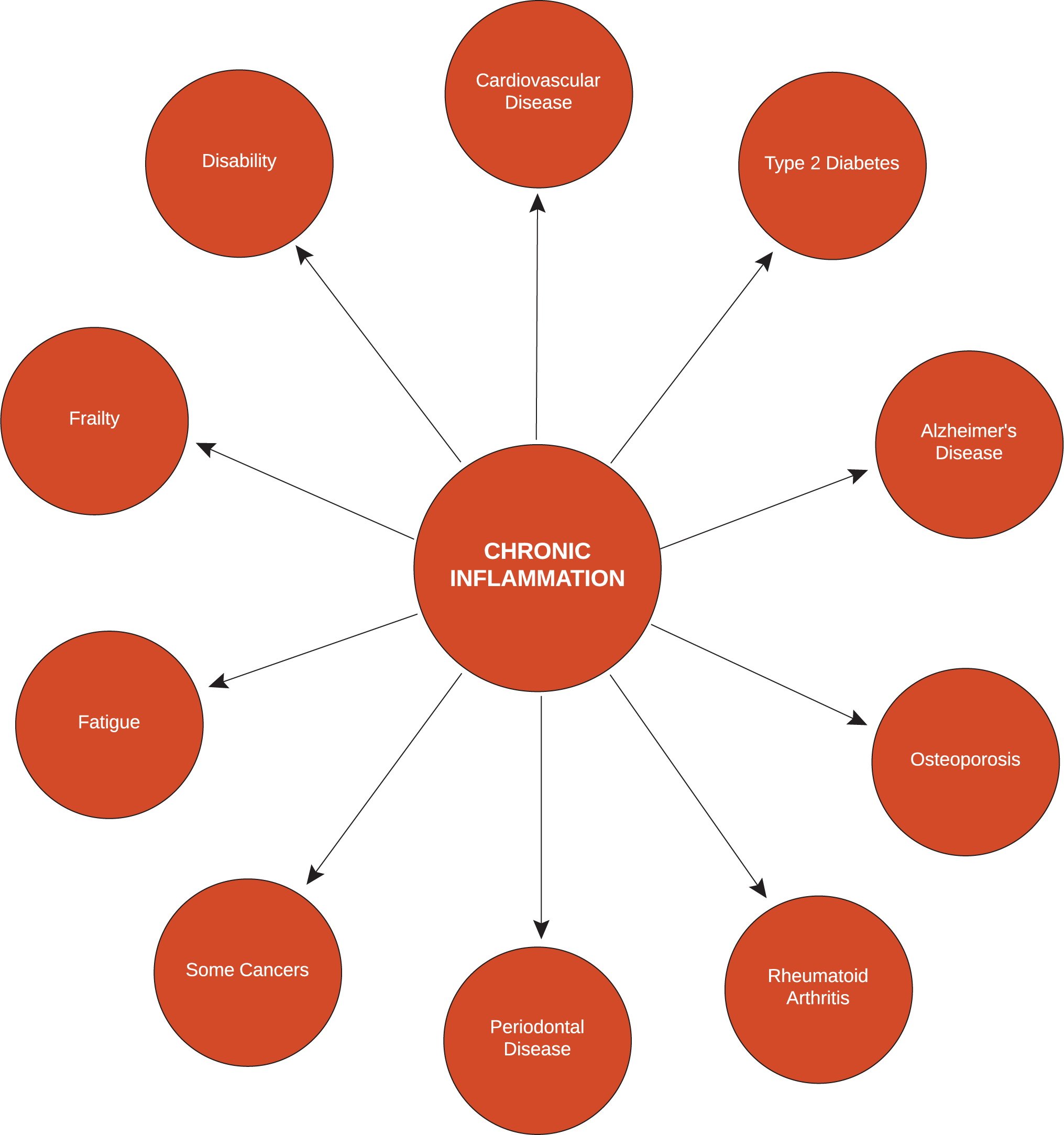
A diagram showing the conditions linked to inflammation.
There is considerable evidence that early-life stress enhances inflammation across the life span. When linking early-life stress to inflammation, psychologists have focused on childhood stressors that are both severe and chronic, because those are the type of stressors that are most likely to have a lasting impact on the immune system (Segerstrom & Miller, 2004). Up to this point, the vast majority of work linking early stress to inflammation has focused on parental maltreatment and socioeconomic status (SES).
Socioeconomic status
Children of lower socioeconomic position are confronted with a number of important social and environmental conditions that contribute to chronic stress (Cohen, Janicki-Deverts, Chen, & Matthews, 2010). They are also more likely to be exposed to malnutrition, high-fat diets, substance abuse, and poor health practices than their higher-SES counterparts (Lynch, Kaplan, & Salonen, 1997). All of these factors likely contribute to elevated circulating levels of inflammatory markers. There are a number of ways to evaluate SES. The most popular method is to assess education or income level. The association between SES and health generally shows a gradient increase (Adler et al., 1994; Gallo, Bogart, Vranceanu, & Matthews, 2005). Most studies model the adopted SES index as a continuous variable; accordingly, the terms “lower” and “higher” are relative terms across the SES continuum.
British women aged 60 to 79 who were raised in lower-SES environments as children had higher levels of CRP than those raised in higher-SES environments (Lawlor, Smith, Rumley, Lowe, & Ebrahim, 2005). Middle-aged women who had less educated parents had higher levels of CRP compared with those whose parents were more educated (Phillips et al., 2009). Likewise, in a sample of over 3,000 adults aged 32 to 47, those raised by less educated parents had higher levels of CRP than those raised by more educated parents (Taylor, Lehman, Kiefe, & Seeman, 2006). Participants who reported living in poorer neighborhoods as children or had parents who were less educated had higher levels of CRP and fibrinogen than those who reported living in more affluent neighborhoods as children or had more educated parents (Pollitt et al., 2007). Importantly, the associations between early-life SES and inflammation were independent of current SES status in each of these studies.
In addition to assessing inflammatory levels in serum, researchers often measure immune reactivity by exposing the white blood cells to a bacterial pathogen. The magnitude of the proinflammatory cytokines produced in response to this stimulus serves as a measure of the degree to which early adversity programmed the immune cells to react to challenge. Those who live in lower-SES households as children are more reactive to immune challenges well into adulthood than those from higher-SES households, regardless of their SES status as adults. Indeed, those who were raised in lower-SES environments as children also displayed larger cytokine responses to microbial challenges as adults (Evans & English, 2002).
Child maltreatment
Child maltreatment is a common experience; approximately 30% to 50% of adults report having experienced some type of abuse or neglect as children (Walker et al., 1999). This includes physical, emotional, and sexual abuse, as well as physical and emotional neglect. Teenagers who were raised in harsh family environments as children had progressively larger inflammatory-cytokine production in response to an immune challenge compared with those who were raised in supportive family environments (Dale et al., 2009). In a longitudinal prospective study, those who were neglected during the first decade of their lives had higher levels of CRP at age 32 compared with those who were not neglected (Danese, Pariante, Caspi, Taylor, & Poulton, 2007). Prospective longitudinal studies such as this are important for alleviating the concerns about retrospective bias inherent in most studies linking early adversity to inflammation (in the vast majority of studies, adult participants are asked to recall their early-life experiences). This association between child maltreatment and elevated circulating markers of inflammation persists into older age. In a study of healthy older adults caring for family members with dementia, those who had experienced emotional, physical, or sexual abuse as children were more likely to have higher IL-6 and TNF-α levels compared with those who were not abused (Kiecolt-Glaser et al., 2011). This is particularly interesting because these effects were apparent over and above the normal increases in inflammation that occur when people age (Walston et al., 2006).
In sum, childhood adversity leads to potentiated inflammatory activity. This is likely a mechanism underlying the higher levels of disease seen in those who were raised in adverse environments. Indeed, those who experience severe early-life stress as children are at greater risk for cardiovascular disease, type 2 diabetes, and cancer compared with those who do not have those early-life experiences (Fagundes et al., 2013; Fagundes, Lindgren, Shapiro, & Kiecolt-Glaser, 2012; Miller et al., 2011; Tyrka et al., 2012). However, up to this point, most studies have treated different types of abuse equally; it will be important for future work to disentangle the type of abuse that has the most profound impact on inflammation and adult health. Likewise, little is known about the severity of abuse necessary to produce a heightened proinflammatory state. It would also be helpful for researchers to identify the specific aspects of SES that have the greatest impact on inflammation. Finally, we do not know if children are most vulnerable to the deleterious effects of toxic stress during certain critical periods in development and to individual differences in risk and resilience to abuse.
Mechanisms
As it is clear that severe early-life stress is associated with elevated levels of adult inflammation, a critical question for researchers is how early experiences have such lasting consequences. We argue that these adverse experiences potentiate reactivity to challenges at multiple levels (see Fig. 2). Although we discuss these levels as independent in the interest of clarity, they are clearly integrative.
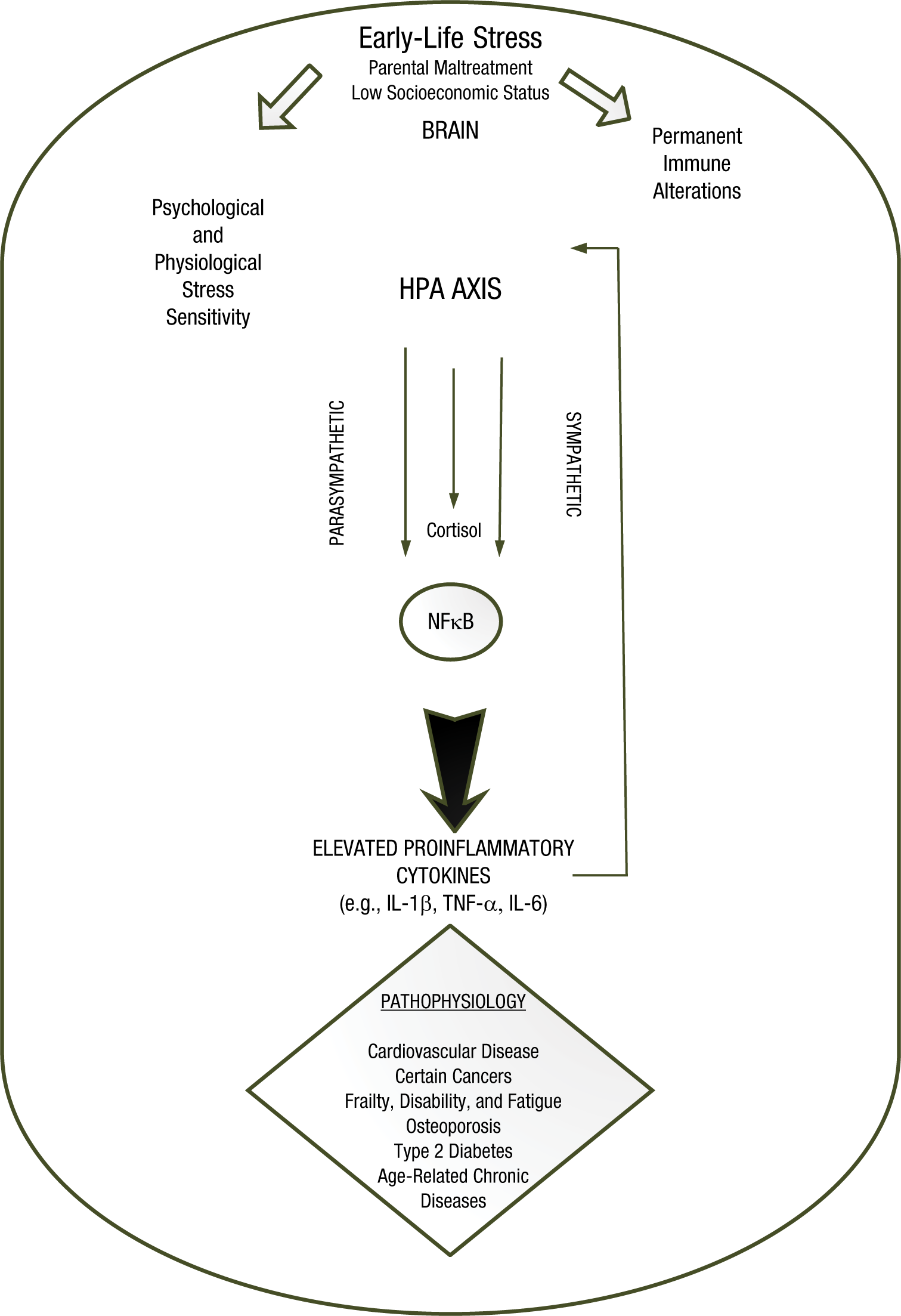
A diagram illustrating how stress impacts inflammation. HPA axis = hypothalamic-pituitary-adrenal axis; NFκB = nuclear factor kappa-light-chain-enhancer of activated B cells; IL-1β = interleukin-1 beta; TNF-α = tumor necrosis factor alpha; IL-6 = interleukin 6.
Psychological pathways potentiating inflammation
Psychological stress and depression can enhance inflammation by upregulating the transcription of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB), an intracellular signaling molecule that regulates proinflammatory-cytokine gene expression (Straub & Härle, 2005). Both the frequency with which life events are experienced as stressful as well as the intensity of reactivity to those life events can lead to elevated inflammation (Fagundes, Glaser, Hwang, Malarkey, & Kiecolt-Glaser, 2012).
Intensity of response to stressors
Adults who reported a history of childhood abuse showed significantly greater emotional reactivity to daily-life stress compared with those who did not report a history of abuse (Glaser, van Os, Portegijs, & Myin-Germeys, 2006). These reactions to daily-life stressors are more likely to trigger an inflammatory response that could lead to greater levels of inflammation. In the laboratory, plasma IL-6 levels were higher in response to an experimental laboratory stressor among those who reported childhood trauma compared with those who did not report such trauma (Carpenter et al., 2010). Similarly, among a sample of males with major depression, those who experienced early-life stress produced a more pronounced IL-6 response to a psychological-stress task in the laboratory than nondepressed males (Pace et al., 2006).
Frequency of psychological stress
In addition to more intense reactivity to stress, individuals coming from adverse early environments may experience more frequent psychological stress. Those who were abused as children or came from low-SES backgrounds were more likely to perceive ambiguous situations as threatening (Chen & Matthews, 2003). As a result, these individuals experienced more daily events as stressful than did those from more stable and loving homes.
Potentiated autonomic-nervous-system reactivity and elevated inflammation
Childhood abuse has generally been linked to autonomic activity (Heim et al., 2000). The autonomic stress response enhances sympathetic activity, which drives the “fight-or-flight” response. It also typically dampens parasympathetic activity. Because the autonomic nervous system can directly innervate immune organs, this autonomic profile of higher sympathetic and lower parasympathetic activity can raise inflammation (Thayer & Sternberg, 2006). Compared with nonmaltreated children, those with a background of neglect or abuse have generally been found to have lower heart-rate variability, reflecting lower parasympathetic activity (Dale et al., 2009; Oosterman, De Schipper, Fisher, Dozier, & Schuengel, 2010). Children who were raised in low-SES families also showed greater levels of sympathetic activity, as indexed by increases in the catecholamine epinephrine (Evans & English, 2002). Interestingly, adults who were raised in low-SES environments showed greater expression of genes upregulated by catecholamines (Miller et al., 2009). Thus, the increase in sympathetic activity and decrease in parasympathetic activity elicited by early adversity is another route by which children exposed to maltreatment or low SES can develop elevated inflammation in adulthood.
Neuroendocrine pathways to elevated inflammation
Childhood abuse has been linked to altered cortisol output in response to stressors in both experimental laboratory situations as well as daily life (Heim et al., 2000; van der Vegt, van der Ende, Kirschbaum, Verhulst, & Tiemeier, 2009). Although cortisol generally inhibits inflammation, the persistence of high cortisol levels can lead immune cells to decrease their response to cortisol. Once a cell has become insensitive to glucocorticoids like cortisol, proinflammatory cytokines are produced in an unregulated environment. In turn, this unregulated environment enhances inflammation.
Epigenetics
One important mechanism that Miller and colleagues (2011) have proposed underlies this potentiated immune response among those who experience early-life stress is epigenetic changes that occur as a result of the early environment. Epigenetic changes are modifications to DNA that persist across the life span and potentially into future generations. Therefore, they are an excellent candidate mechanism to explain how an early-life event can still affect immune reactivity in adulthood. The type of epigenetic change that is most studied in the social health literature is a process called methylation. This refers to the addition of a chemical group (specifically, a methyl group) to the DNA that typically impairs expression of the gene. Many genes throughout the genome, including genes in the immune system, have sites that can be methylated.
The study of epigenetic contributions to inflammation is in its infancy; however, there is suggestive evidence that epigenetic changes can affect later immune reactivity. For example, early-life adversity was related to genome-wide methylation in adulthood, which was related to the production of IL-6 after immune cells had been challenged with pathogens (Lam et al., 2012). When social status was experimentally altered in nonhuman primates, there was a similar relationship between immune-related gene expression and the amount of genome-wide methylation. This strongly suggests that social status is indeed a driver of epigenetic differences (Tung & Gilad, 2013). Recent work suggests that the majority of DNA-methylation changes are reversible (Tompkins et al., 2012). An important consideration for future studies will be to identify whether there are critical periods in development when these epigenetic changes occur, what role inflammatory molecules play in these methylation events, and how to reverse modifications that are deleterious (Gasche, Hoffmann, Boland, & Goel, 2011; Tompkins et al., 2012).
Policy Recommendations
Advances in the field of psychoneuroimmunology regarding early-life stress and inflammation provide a compelling rationale for designing policies and interventions that reduce toxic childhood stress in order to improve lifelong health. Because the epigenetic changes resulting from early-life adverse events can be perpetuated to future generations, these interventions can have truly long-lasting salubrious effects. Considerable national investments in programs that prevent childhood abuse and neglect and ameliorate childhood poverty are clearly warranted. Importantly, these primary prevention efforts could substantially reduce the onset of later diseases and their associated health care costs (Kaplan, 2000).
Basic research will be critical for identifying the most responsive time periods and biological pathways so that interventions can be most appropriately targeted. Interventions that help children who are abused or seriously neglected should be a high priority to improve not only mental health but adult physical health as well. For those who experienced early-life stress, anti-inflammatory medications and supplements (e.g., fish-oil supplements containing omega-3 fatty acids) may be warranted. Psychological interventions such as cognitive behavioral therapy and relaxation training may also prove beneficial. Inflammatory biomarkers offer a promising source of information for assessing the short- and long-term effects of these interventions.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.