
Abstract
With increasing life expectancies in most Western populations, the number of people experiencing age-associated cognitive impairment is increasing. Research is needed to identify factors that may help the elderly maintain or even improve cognitive function in the face of advancing age. This review evaluates whether dietary supplementation with natural pharmaceuticals can be used as a means to improve cognitive function or limit cognitive decline. The evidence surrounding popular supplements such as Ginkgo biloba, fish oils, Bacopa monnieri, polyphenol extracts, and vitamins is reviewed briefly. Potential mechanisms of action are also highlighted. This review also discusses challenges surrounding cognitive testing in psychopharmacological research, highlighting discrepancies between the domains of human cognition as described by contemporary models and as measured in clinical trials.
Life expectancies are increasing rapidly throughout the developed world. Over 30 countries have current life expectancies of at least 80 years of age (World Health Organization, 2014). This increase in life expectancies, coupled with the maturation of baby boomers, has led to an ongoing and marked shift in the proportion of elderly individuals.
With old age comes new challenges for science, health care, and the well-being of our older citizens. Increasing age is a major risk factor for dementia (Corrada, Brookmeyer, Paganini-Hill, Berlau, & Kawas, 2010), associated with a progressive loss of cognitive ability that eventually leads to loss of independence and death. Even those who do not go on to develop dementia are likely to experience some decline in cognitive ability (Singh-Manoux et al., 2012). This is because the aging brain undergoes a host of structural and biological changes to key neurons and neuronal circuits involved in cognitive processing (Morrison & Hof, 1997).
Helping individuals improve or maintain their cognitive function in the face of advancing age is thus an important area of research. Targeted treatments for brain aging will require an in-depth understanding of the mechanisms linking aging to a functional decline in cognitive ability. Importantly, some of the risk factors underpinning brain aging are modifiable and may be amenable to intervention. Our approach described in this article is to explore pharmacological means of improving cognitive performance in the healthy elderly. Ultimately, however, combining different interventions, such as pharmacology, diet, exercise, and cognitive training, will most likely lead to the best strategies in the future. The aim of this review is to provide a current snapshot of research into pharmacological means of improving cognitive performance, with a focus on dietary and herbal supplementation, emphasizing data from our own laboratories.
What Is Cognitive Aging?
Numerous cognitive abilities have been shown to decline with advancing age, although different cognitive abilities are differentially affected by the aging process. The Whitehall II study showed that reasoning, memory, and fluency all declined over a 10-year follow-up period in adults aged 45 years and older (Singh-Manoux et al., 2012). Among these abilities, the temporal profiles of decline were diverse. The largest decline was in the domain of reasoning, while vocabulary was resistant to cognitive decline until very old age. Wilson et al. (2002) showed that there are large individual differences in the rate of cognitive decline, meaning that cognitive decline is driven by person-specific factors. That is to say that some people “age well,” experiencing little cognitive decline, while others are not so fortunate.
Biological Mechanisms Underpinning Cognitive Aging
The biological mechanisms responsible for cognitive decline are complex and incompletely understood. Many different biological systems have been implicated in brain aging. It was once thought that the insidious death of neurons caused cognitive abilities to slowly diminish with age. However, neuronal cell loss alone is not sufficient to explain cognitive aging. This is because age-related declines in neurons throughout the neocortex and hippocampus are not necessarily a significant feature of normal aging (Morrison & Hof, 1997). Age-related changes to brain structure may include shrinkage of neurons, decreases in the number of synapses and synaptic spines, and changes to the brain’s connections in the form of shorter white-matter axons (Fjell & Walhovd, 2010). The mechanisms underpinning these changes to brain structure are thought to be subtle and complex. Genetic factors and environmental influences—including changes in vascular health, hormone and neurotransmitter production and function, immune function, glucose metabolism, oxidative stress, and inflammation, as well as exposure to toxins, disease, and head trauma—are just some of the many mechanisms that may contribute to age-related cognitive decline (Lindenberger, 2014; Pase, 2012).
Natural Pharmacological Strategies
Many risk factors for cognitive decline appear to be modifiable (Lindenberger, 2014; Pase, 2012). This implies that individuals’ risk of cognitive decline may either increase or decrease depending on environmental factors, including those relating to diet and lifestyle. Of interest to our research group, certain pharmacological interventions have the ability to target multiple mechanisms implicated in cognitive decline. Many psychoactive pharmaceutical drugs have been designed to target single mechanisms and exert effects on the brain quickly. In contrast, many natural supplements contain multiple active ingredients, target multiple mechanisms implicated in cognitive aging, and produce behavioral effects only after weeks or even months of daily use. Here, we review some of the more popular natural supplements that have been suggested to improve cognitive performance or limit cognitive decline. Our aim is not to provide an exhaustive review but to highlight some of the more interesting and important findings.
Natural Supplements and Cognitive Aging—What Is the Evidence?
Ginkgo biloba
Ginkgo biloba extracts are derived from the leaves of the Ginkgo biloba tree. Ginkgo is perhaps the most extensively studied natural supplement with purported cognition-enhancing effects. The most common extract of ginkgo, EGb 761, has been very well characterized in terms of its chemical profile. Considerable interest surrounds the cognition-enhancing effects of EGb 761 because it appears to have multiple modes of action relevant to brain aging. Its mechanisms span antioxidant, anti-inflammatory, and anti-ischemic activity as well as beneficial effects on blood flow, glucose metabolism, and synaptic remodeling (DeFeudis & Drieu, 2000).
A Cochrane review examined the efficacy of Ginkgo biloba for dementia and cognitive decline across 36 randomized controlled trials (Birks & Evans, 2009). The review found no consistent evidence to suggest a cognitive benefit of ginkgo in those with dementia or cognitive impairment. However, most of the reviewed trials were less than 12 weeks in duration. The review has also been criticized for failing to differentially evaluate the effects of ginkgo on cognition in those without dementia as well as in the different types of dementia. A more recent meta-analysis investigated the effects of EGb 761 on Alzheimer’s disease, vascular dementia, and mixed dementia (Weinmann, Roll, Schwarzbach, Vauth, & Willich, 2010). Nine trials were included in this review, with trial durations ranging from 12 to 52 weeks. Across all studies, a favorable and moderately large effect of ginkgo was found on cognitive performance (standard mean difference [SMD] = −0.58). Subanalysis revealed a larger effect of ginkgo on cognition in Alzheimer’s disease as opposed to other types of dementia.
Bacopa monnieri
Bacopa monnieri is an Indian herb that has been used as a traditional medicine for centuries. Bacopa has been shown to act on a myriad of mechanisms associated with cognitive function, reducing inflammation and oxidative stress as well as modifying levels of acetylcholine (Russo & Borrelli, 2005), a key neurotransmitter involved in learning and memory. In animal models, bacopa has been shown to scavenge (i.e., remove) beta-amyloid (Holcomb et al., 2006), a protein abundant in the brains of those with Alzheimer’s disease. In 2001, our group conducted the first rigorous scientific study to examine the cognition-enhancing effects of a standardized extract of bacopa (CDRI08) in humans (Stough et al., 2001). After 12 weeks of daily supplementation, bacopa CDRI08 significantly improved processing speed, with a moderate effect size (d = 0.54), as well as learning and memory, with small to large effects depending on the specific measure (d = 0.27–1.01). There have been many randomized controlled studies of bacopa’s effects in humans since this early study. Our recent systematic review of six clinical trials revealed evidence to suggest that extracts of bacopa enhance free recall (Pase et al., 2012), defined as the recall of items from a sequentially presented list, in any order, either immediately or following a short delay. The magnitude of this effect varied across studies (d = 0.27–0.95). Studies on bacopa and cognition have generally been of short (e.g., 3 months) duration. Longer trials are needed to substantiate the effects of bacopa on cognitive decline.
Vitamins
One third of the U.S. population report taking multivitamins (Bailey et al., 2011). We performed a meta-analysis to quantify the effects of multivitamins on cognitive performance in adults. Across studies, multivitamins improved verbal immediate free-recall memory (SMD = 0.32), without evidence of enhancement in any other cognitive domains (Grima, Pase, MacPherson, & Pipingas, 2012). Many other cognitive abilities were found to be under-researched, and most included studies were of short duration. Congruent with our meta-analysis, a large randomized controlled trial (N = 4,447) reported that multivitamins maintained cued-recall memory (the verbal recall of a list of items belonging to numerous categories) over 6 years of supplementation (Kesse-Guyot et al., 2011). Although the effect was moderately large (SMD = 0.61), baseline cognitive function was not examined in this study, and the analysis of cognitive outcomes was carried out post hoc. In contrast, the Physicians Health Study II reported that supplementation with a daily multivitamin, relative to a placebo, did not slow the rate of cognitive decline over 12 years in 5,947 male physicians (Grodstein et al., 2013).
B vitamins have also received considerable attention with respect to cognitive aging. B vitamins are known to lower homocysteine, an amino acid linked to dementia (Seshadri et al., 2002). The VITACOG study demonstrated that supplementation with homocycteine-lowering B vitamins slowed the rate of brain atrophy by 27.1% and slowed cognitive decline (d = 0.2–0.58) in adults with mild cognitive impairment and high levels of homocysteine (De Jager, Oulhaj, Jacoby, Refsum, & Smith, 2012; Smith et al., 2010). However, in adults without cognitive impairment, a recent meta-analysis of 11 trials involving 22,000 participants found no effect of homocysteine-lowering B vitamins on cognitive function (Clarke et al., 2014).
Polyphenol-derived extracts
Polyphenols and related flavonoids are a group of compounds commonly consumed from many different food sources, including onions, apples, berries, cocoa, tea, and coffee. Many types of polyphenols are considered to be healthy because they appear to scavenge free radicals (i.e., they have powerful antioxidant effects), improve vascular health, and reduce inflammation (Nijveldt et al., 2001).
Certain pine-bark extracts are high in polyphenols, including Pycnogenol, a patent extract of the French maritime pine tree. Using a randomized placebo-controlled design, Ryan et al. (2008) reported that 3 months of daily Pycnogenol supplementation improved working memory (d = 0.44) and a decreased a biochemical measure of oxidative stress (d = 0.43). A further randomized controlled study reported that a similar pine-bark extract called Enzogenol improved spatial working memory (d = 0.47) and immediate picture-recognition memory (d = 0.54) after 5 weeks of supplementation (Pipingas et al., 2008).
Although mixed findings have been reported (Pase et al., 2013), some studies have shown that supplementation with dark chocolate, high in polyphenols derived from cocoa, improves cognition and brain function (Scholey & Owen, 2013).
Fish oil
Fish oils and oily fish, such as mackerel and salmon, are high in long-chain omega-3 polyunsaturated fatty acids known as docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). Such fatty acids play an important role in regulating cellular function and inflammation. They can also have beneficial effects on heart health, including via effects on blood pressure and triglycerides (Kris-Etherton, Harris, & Appel, 2002). With respect to the brain, some observational studies have shown that consumption of omega-3s can slow the rate of cognitive decline (Fotuhi, Mohassel, & Yaffe, 2009). However, randomized controlled trials have not universally supported the cognition-enhancing effects of fish oils. A recent meta-analysis reported that omega-3 supplementation had no effect on cognition in healthy people, although supplementation was found to have small benefits for attention and processing speed (d = 0.32) in people with cognitive impairment but no dementia (Mazereeuw, Lanctôt, Chau, Swardfager, & Herrmann, 2012). In contrast, a more recent trial reported that supplementation with DHA had small benefits for memory function (d = 0.19–0.34) in healthy young to middle-aged adults following 6 months of supplementation (Stonehouse et al., 2013). The subjects in this study all had low DHA levels at baseline, suggesting that the cognitive benefits of fish oils may be limited to those who are deficient in omega-3s.
Other natural interventions
Our review focuses on the natural cognitive enhancers with the most evidence and popularity. Many other natural pharmacological interventions have been examined with respect to cognitive aging that we cannot cover in this brief review. There are also many interesting plant-based molecules with mechanisms of action that are likely to improve brain function that have not yet been examined with respect to human cognition.
Current Challenges and Future Directions
There are numerous challenges associated with investigating the effects of natural supplements on cognitive function. For all the reviewed interventions, longer clinical trials are needed to establish whether supplementation can limit the progression of age-associated cognitive decline as well as the conversion from healthy cognitive aging to cognitive impairment. Short-term benefits to cognitive function following supplementation do not necessarily imply long-term protection against cognitive decline or cognitive impairment.
It is often hard to compare and contrast the results of individual trials given the differences in the cognitive tests, sample demographics, and products used across studies. The validity and sensitivity of cognitive outcomes in clinical trials is one issue of particular concern. As we recently highlighted (Pase & Stough, 2013), there is little consensus in the field about how to select, analyze, and report on cognitive outcomes. Cognitive composite scores are often created by combining tenuously related cognitive tasks without adequate justification. We recently suggested that the Cattell-Horn-Carroll (CHC) cognitive framework could be applied to help organize cognitive outcomes in clinical trials according to validated latent cognitive factors (Pase & Stough, 2013,2014). By outlining the structure of human cognitive function (Fig. 1), the CHC model can help researchers measure and categorize the effects of a specific intervention against the full spectrum of human cognitive abilities. Although the utility of the CHC is in helping individuals categorize cognitive tests into broad and narrow abilities, one could also use the CHC to examine the effects of a pharmacological intervention on general intelligence (g).
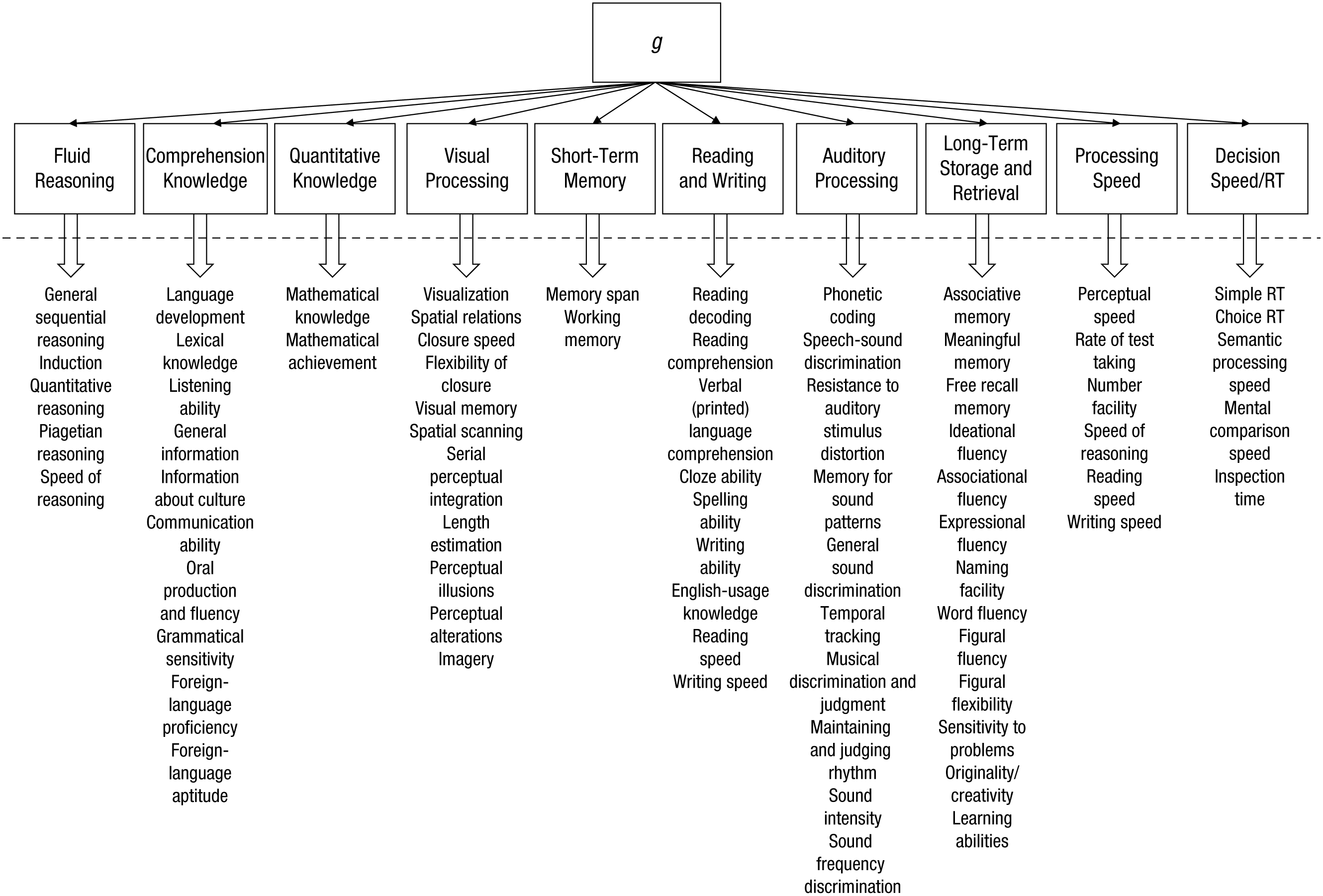
The broad and narrow abilities of the Cattell-Horn-Carroll model, based on the writing of McGrew (2009). Three additional narrow abilities of the auditory-processing factor and the newly identified and broad tactile, kinesthetic, olfactory, and psychomotor abilities, as well as domain-specific knowledge, are omitted owing to space constraints. RT = reaction time; g = general intelligence. Adapted from “An Evidence-Based Method for Examining and Reporting Cognitive Processes in Nutrition Research,” by M. P. Pase and C. Stough, 2014, Nutrition Research Reviews, 27(2), p. 235. Copyright 2014 by the American Society for Nutrition. Adapted with permission.
Standardized computerized cognitive-test batteries have become popular as a means to capture the effects of different natural supplements. Such batteries have many strengths, including the availability of parallel forms (i.e., differing versions of tests that contain the same items in a different order), which are important for minimizing the effects of practice following repeated assessments. However, many computerized cognitive-test batteries may provide an incomplete picture of cognitive performance. When the tasks from some standardized batteries are measured against the broad cognitive domains of the CHC, it becomes evident that many clinical trials are not examining the full range of cognitive functions (Pase & Stough, 2014).
To better assess the full spectrum of cognitive abilities in clinical trials, we propose the development of a computerized cognitive-test battery with individual tasks that map onto the different components of the CHC model. This could be achieved through our recently initiated international collaboration, whereby we hope to create a set of cognitive tasks with parallel forms that are made freely available on the Internet. This would allow those working in the area of clinical nutrition to measure and express outcomes within a validated psychological framework, improving communication, standardization, and validity. This would also provide a free alternative to the major computerized cognitive-test batteries, which are generally very costly. More information about this collaboration can be found at www.thecognitioncollaboration.com.
Conclusions
The results of the clinical trials reviewed here are an admixture of hopeful findings, often leavened by studies of small duration and sample size. Although difficult and costly to conduct, trials of longer duration are needed to ascertain which dietary supplements, if any, afford protection against cognitive decline and cognitive impairment. Differences between existing studies also make it hard to draw overall conclusions about any particular supplement. In our own work, standardized herbal extracts of bacopa and pine bark have shown promise in terms of their ability to improve cognitive function, with a larger trial of longer duration currently underway to validate these preliminary findings (Stough et al., 2012). Meta-analyses have shown that multivitamins, fish oils, and ginkgo can all enhance specific aspects of cognitive function. To minimize differences in cognitive outcomes between studies, we suggest cooperation between different groups working in the area to develop a set of freely available cognitive tasks validated against the CHC model.
Footnotes
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Funding
C. Stough has received funding from the Australian Research Council, Horphag (Switzerland), Soho Flordis International (Australia), Blackmores (Australia), and Barry Callebaut (Belgium) to study plant-based extracts and cognition. M. P. Pase is supported by an Australian National Health and Medical Research Council Early Career Fellowship (APP1089698).