
Abstract
Objective:
To describe attitudes towards acupuncture and expectations regarding potential treatment outcomes among women with self-reported primary dysmenorrhoea (PD) residing in Australia.
Methods:
A cross-sectional, descriptive online survey was conducted to assess attitudes and treatment expectancy using an adapted version of previously published complementary and alternative medicine (CAM) attitude scale and a validated acupuncture expectancy scale (AES). Data were analysed descriptively, with exploratory analysis conducted to support the interpretation of response patterns. Ethical approval was obtained from the Edith Cowan University Human Research Ethics Committee (2023-04471-LIU) and participants provided electronic informed consent.
Results:
A total of 247 responses were received. Participants were mainly aged 25–30 years and largely from Western Australia. Many reported having experienced PD for more than 6 months and a range of related symptoms. Item-level analysis suggested generally favourable attitudes towards acupuncture, with 81% expressing interest in acupuncture. Treatment expectancy was moderate overall. Sensitivity and exploratory stratified analyses showed broadly comparable descriptive patterns across demographic and clinical subgroups.
Conclusion:
Women with self-reported PD showed generally favourable attitudes towards acupuncture and moderate expectancy. Of note, this was found to be a self-selected sample with higher educational attainment that was predominantly interested in acupuncture. Findings reflect perceived acceptability rather than clinical effectiveness or population-level perspectives and should not be generalised. As attitudes were assessed using an adapted, non-validated instrument, results should be interpreted cautiously as indicative of response tendencies. Future research is needed among women not interested in acupuncture and those with a lower educational level to further explore the contextual and experiential factors that potentially shape how acupuncture is perceived and utilised.
Introduction
Primary dysmenorrhoea (PD) is a highly prevalent menstrual pain condition that substantially impairs physical functioning and quality of life. 1 Evidence suggests that non-steroidal anti-inflammatory drugs (NSAIDs) and hormonal contraceptives are first-line treatments; 2 however, many women report insufficient symptom relief, side effects or reluctance to use these options. These limitations have contributed to increasing interest in non-pharmacological and complementary approaches, including acupuncture. 3 Acupuncture—a widely used component of complementary and alternative medicine (CAM)—involves the insertion of fine needles into the body to support health and wellbeing. It is internationally utilised for pain management and has been proposed as a therapeutic option for pain-related conditions.4,5
Complex therapeutic interventions achieve their outcomes through a combination of specific and non-specific mechanisms. For instance, a study by Lewith et al. 6 showed that the specific physiological effects of acupuncture, such as the selection of needling location(s), appear to account for a relatively small proportion of its overall therapeutic impact (estimated at around 10%). Conversely, expectancy has emerged as a pivotal factor in non-specific effects, as evidenced by extensive psychological research.7,8 Expectation, which is defined as individuals’ cognitive anticipation of treatment-related health outcomes following a specific intervention, 9 plays a significant role in driving changes in symptoms and other health-related parameters. Clinical investigations have consistently indicated that patients’ positive expectations correlate with improved health outcomes, and patients exhibiting a positive attitude towards acupuncture and anticipating favourable treatment responses are more likely to benefit from acupuncture interventions.10 –12
Attitudes towards acupuncture may also influence treatment engagement by shaping perceived credibility, openness to complementary therapies and willingness to initiate or continue treatment. Evidence from broader CAM utilisation studies indicates that positive attitudes are linked to increased likelihood of trying complementary treatments, particularly among individuals who are dissatisfied with conventional care. 13
Despite an increasing amount of research into acupuncture for PD, little is known about how women in Australia perceive this treatment. Existing research has largely focused on clinical efficacy trials, with minimal attention to patient attitudes, expectancy or decision-making processes. A previous review identified a clear gap in understanding how women evaluate acupuncture as a potential management option for PD. 14 Similar attitude-oriented studies, such as research exploring perceptions, barriers and drivers of medicinal cannabis use among Australian women with PD, have demonstrated the value of capturing patient viewpoints to inform clinical practice and guide treatment communication. 15
Therefore, the aim of this study was to investigate how women with self-reported PD residing in Australia perceive acupuncture as a potential treatment option, focusing specifically on their attitudes towards acupuncture and their expectations of its likely benefits. In the present study, attitude refers to individuals’ general evaluations or beliefs about acupuncture, and expectancy refers to treatment-related expectations as operationalised, whereas the term “expectations” is used in a general descriptive sense. We anticipated that understanding these patient perspectives may support more informed communication and guide appropriate clinical integration of acupuncture in women’s health care.
Methods
Study design and recruitment
This study employed a descriptive, cross-sectional, anonymous online survey using a voluntary convenience sampling approach. Data were collected between August 2023 and January 2024. Participants were recruited via online dissemination of study advertisements, including digital flyers shared via social media and community networks, with limited distribution of printed materials in community settings. Participation was voluntary, and the survey was administered in English.
Sample size calculation and inclusion criteria
The sample size was estimated using Daniel’s formula for cross-sectional studies. 16 Based on a conservative estimated prevalence of dysmenorrhoea, informed by Australian studies in adolescents and young women,17,18 with a 95% confidence level (Z = 1.96) and 4% precision, the minimum required sample size was calculated to be 216. Allowing for an anticipated 20% rate of incomplete responses, a target sample size of 260 was set. The achieved sample size (n = 247) exceeded the minimum requirement and is believed to provide reasonably precise estimates of key proportions, with a margin of error of approximately ±6% at the 95% confidence level under the most conservative assumption (p≈0.5). The sample size calculation was based on the estimation of proportions in the overall sample and was not designed to ensure statistical power for detecting differences between subgroups.
In order to meet our inclusion criteria, participants needed to be aged 18 years or older, reside in Australia, be able to provide informed consent, and be able to read and understand English sufficiently enough to complete the questionnaire. Participants were eligible if they reported symptoms consistent with the widely accepted clinical definition of PD, defined as painful menstruation in the absence of pelvic pathology, which is typically characterised by recurrent and crampy lower abdominal pain during menstruation and is sometimes accompanied by symptoms such as nausea or diarrhoea. 1 Eligibility was irrespective of formal medical diagnosis, provided participants reported no pelvic pathology or other gynaecological conditions.
Data collection and instruments
A self-report online survey was developed using the cloud-based software Qualtrics (https://www.qualtrics.com). All survey questions were designed as mandatory, ensuring complete responses and consistent denominators across survey items. The survey consisted of three sections: demographic and clinical characteristics; attitudes towards acupuncture; and expectancy regarding acupuncture treatment outcomes.
Section A collected demographic data (including age, race, ethnicity, state, educational level, employment status and health insurance coverage), as well as information related to dysmenorrhea (such as symptoms, duration and severity of pain). Pain severity in section A was evaluated using a numerical rating scale (NRS). 19
Section B assessed participants’ attitudes towards acupuncture using an adapted version of a previously published CAM attitude scale, 20 in which the term “CAM” was replaced with “acupuncture” to align with the study’s focus. No other substantive wording or structural changes were applied. All items were reviewed by a multidisciplinary expert panel to ensure clarity and content relevance. The scale comprises 13 items covering multiple conceptual domains, including interest, safety, regulation and perceived legitimacy of acupuncture. Each item was rated on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree).
Section C assessed expectancy regarding acupuncture treatment outcomes using a validated acupuncture expectancy scale (AES). 21 The AES consists of four items measuring expectancy of symptom relief, improved overall health and increased energy levels. All original items were used without modification and were rated on the same 5-point Likert-type scale as described above. Permission to reproduce the full AES item set was obtained from Elsevier via RightsLink (license no. 6165750944975; Supplemental Appendix 1) and all instrument items are provided in the Supplemental Material (Supplemental Appendix 2).
Data analysis
Data quality and verification procedures
To minimise the risk of duplicate or inauthentic responses, several data quality and verification procedures were implemented before analysis. Qualtrics settings restricted multiple submissions from the same device or Internet protocol (IP) address. Responses were screened for geographic eligibility, and entries originating outside of Australia were excluded. Completion times were reviewed to identify and remove implausibly rapid responses. In addition, internal consistency checks were applied across eligibility, symptom and health condition items to exclude responses that were not consistent with the symptom profile and eligibility criteria for PD.
Descriptive statistics
A descriptive analysis was conducted to summarise participants’ demographic and clinical characteristics, attitudes towards acupuncture and treatment expectancy. Item-level responses to the adapted CAM attitude items and the AES were summarised using frequency distributions and percentages. Analysis focused on characterising response patterns in line with the descriptive objectives of the study.
Exploratory and sensitivity analysis
Survey data were exported from Qualtrics and analysed using the Statistical Package for the Social Sciences (SPSS) version 28 (SPSS Inc., Chicago, IL, USA). For the adapted CAM attitude scale, negatively worded items (Q2, Q4, Q5, Q6, Q13) were reverse-coded before analysis. Mean attitude scores and mean expectancy scores were calculated by averaging responses across the respective items (range 1–5), with higher scores suggesting more favourable attitudes and greater expectancy. Internal consistency for both scales was assessed using Cronbach’s alpha to inform interpretation of aggregated scores rather than to establish psychometric validity. Sensitivity analysis was conducted by repeating descriptive analysis after excluding participants without a formal clinical diagnosis of PD, to assess the robustness of observed response patterns. Exploratory stratified analysis examined descriptive response patterns across selected participant characteristics, including pain severity (NRS score), educational level, age group and race/ethnicity.
Ethical considerations
This study received approval from the Edith Cowan University Human Research Ethics Committee (no. 2023-04471-LIU), including an approved amendment that broadened the inclusion criteria to women with self-reported symptoms of PD, regardless of formal diagnosis. Electronic informed consent was obtained, with participants required to actively indicate consent on the information page prior to accessing the survey. Only women aged 18 years or older were eligible to participate; therefore, parental consent was not required. The study employed an anonymous online survey, and no personally identifying information was collected as part of the survey responses.
Results
Results are presented in parallel with the structure of the survey instrument, including demographic and menstrual characteristics, attitudes towards acupuncture and expectancy measured using the AES.
Demographic characteristics
A total of 298 responses were received, of which 247 were included in the data analysis. Fifty-one were removed due to incomplete information (n = 28), self-reported pelvic pathology or gynaecological conditions inconsistent with PD (n = 11) and participants residing outside of Australia (n = 12). The demographic characteristics are presented in Table 1. The majority of participants fell within the age brackets of 25–30 years (37.3%, n = 92) and 18–24 years (32.4%, n = 80). Of the participants, 21.1% (n = 52) identified as Australian, while 25.1% (n = 62) identified as Asian. The majority of participants resided in Western Australia (33.2%, n = 82), followed by Victoria (14.2%, n = 35), Queensland (11.7%, n = 29) and New South Wales (11.3%, n = 28). The highest level of education attained by most participants was a bachelor’s degree (34.8%, n = 86), followed by a postgraduate degree (33.2%, n = 82). In terms of employment status, 55.9% (n = 138) of participants were employed full time, 25.5% (n = 63) part time and 16.6% (n = 41) casually, while 2.0% (n = 5) were not employed. The majority of respondents reported having private insurance coverage (84.6%, n = 209), with 38 individuals (15.4%) not having private insurance.
Demographic characteristics of participants (n = 247).
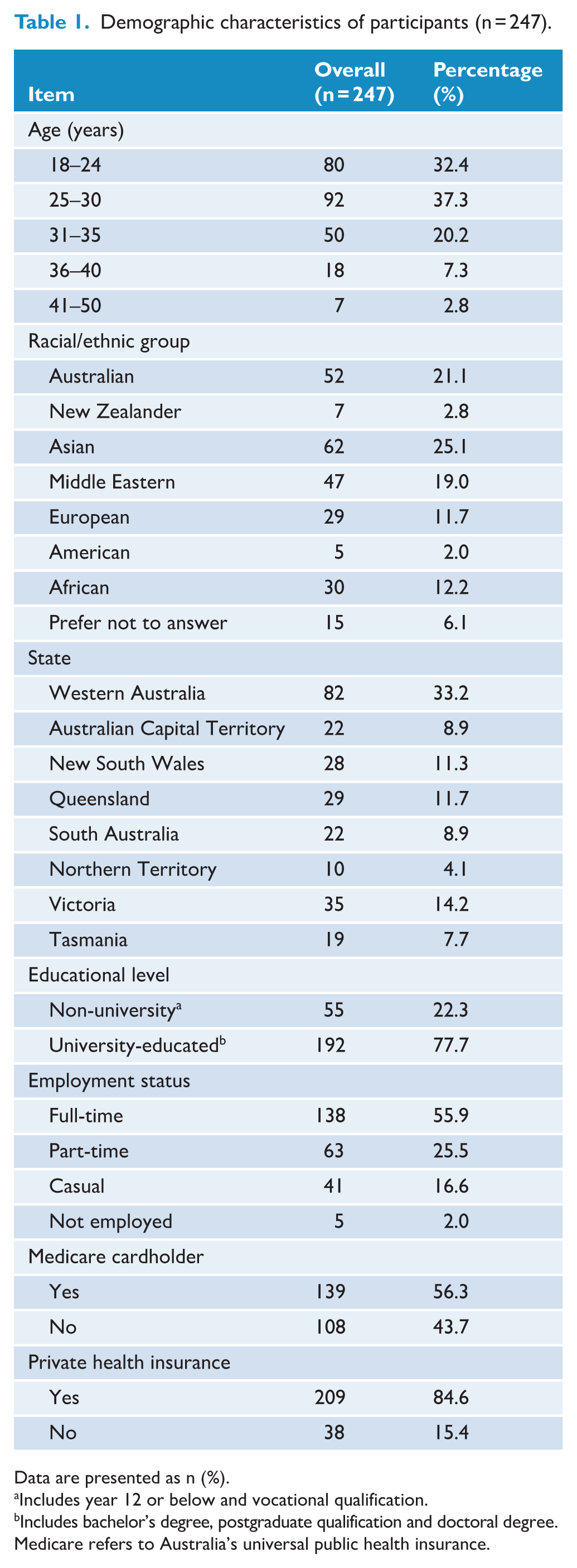
Data are presented as n (%).
Includes year 12 or below and vocational qualification.
Includes bachelor’s degree, postgraduate qualification and doctoral degree. Medicare refers to Australia’s universal public health insurance.
Menstrual characteristics
All participants reported symptoms consistent with PD. Of these, 56.7% (n = 140) reported a prior clinical diagnosis by a healthcare professional, while the remaining participants had no formal diagnosis. A total of 71.7% (n = 177) of participants reported having experienced pain for more than 6 months, and 28.3% (n = 70) reported having had pain for less than 6 months. Notably, two participants stated that they had been experiencing monthly pain since their first menstrual period. Dysmenorrhea symptoms varied among participants, with lower abdominal pain being the most common, followed by fatigue, diarrhoea, lower back pain or backache, headache, poor sleeping, muscle cramps, hip pain, dizziness, nausea and vomiting (Figure 1). Other symptoms included pain radiating to the leg, chills, impaired concentration and reduced appetite. PD symptoms were commonly reported as moderate to severe, with a median pain severity score of 6 on an 11-point NRS score (Figure 2).
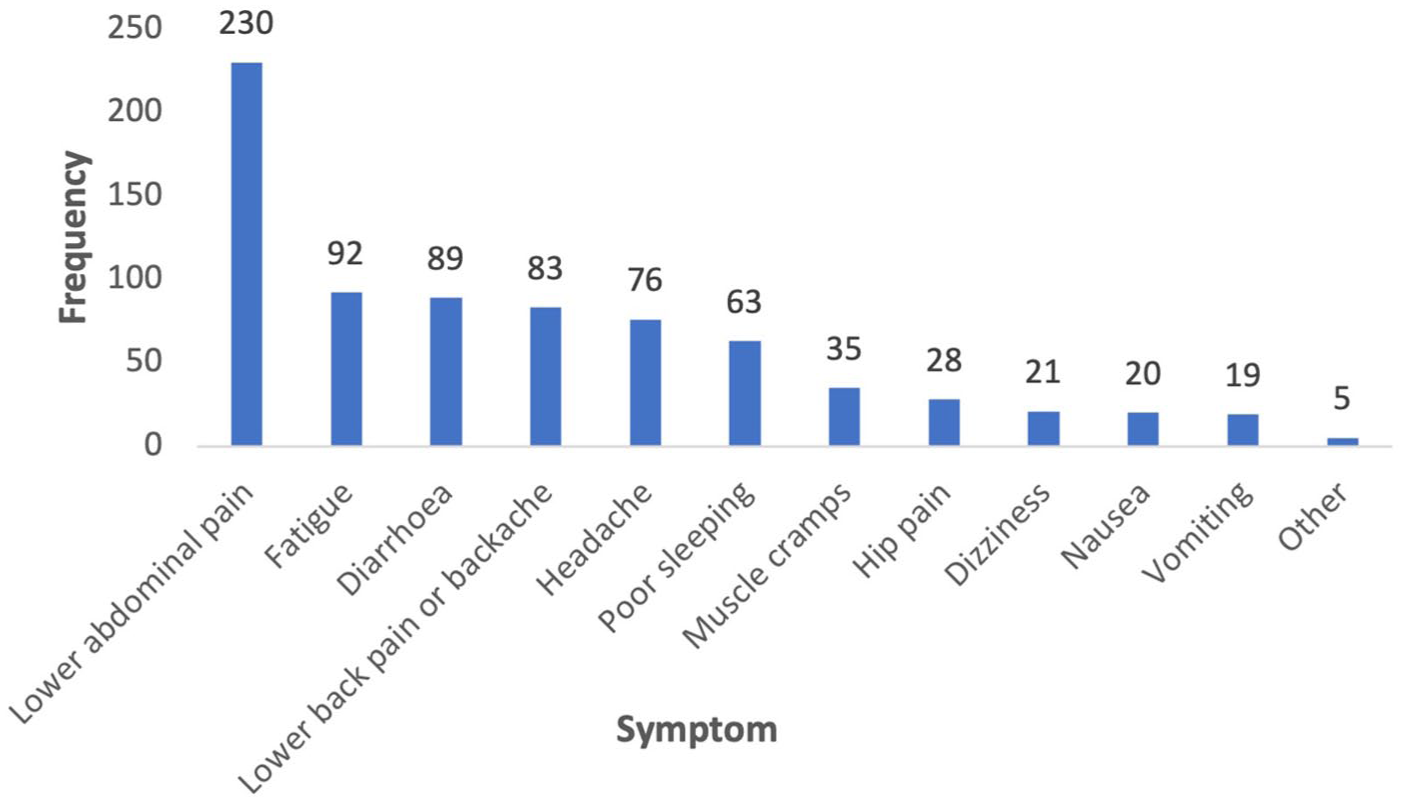
Frequency of primary dysmenorrhea symptoms reported by participants (multiple responses allowed).
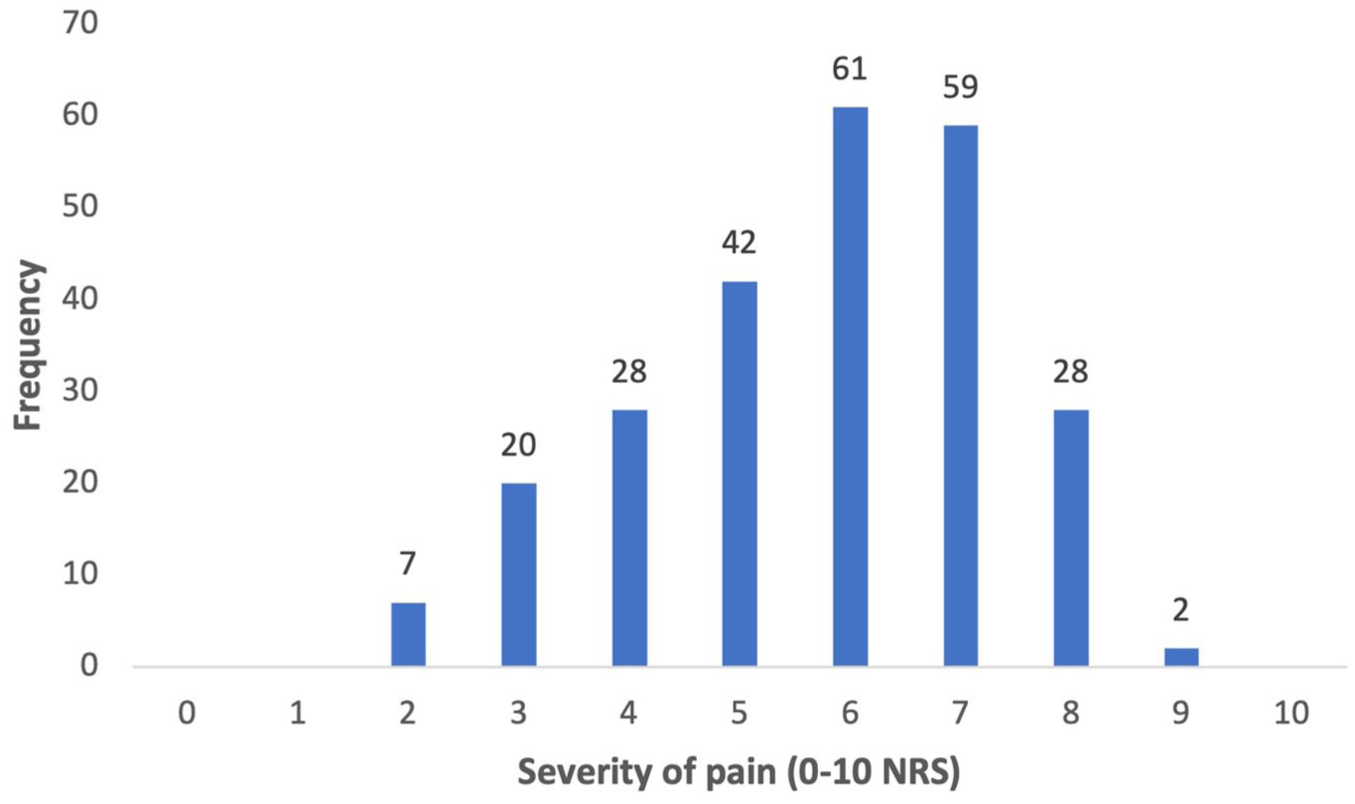
Severity of primary dysmenorrhoea pain assessed using a 0–10 numerical rating scale (NRS).
Attitudes towards acupuncture
Overall, item-level responses suggested generally favourable attitudes towards acupuncture. A substantial proportion of participants (81.0%, n = 200) agreed or strongly agreed that they were interested in exploring acupuncture and related treatments. Nearly half of the participants (45.3%, n = 112) strongly agreed on the importance of having a basic understanding of acupuncture before using it, followed by agreement with statements indicating that acupuncture warrants further research (40.1%, n = 99) and that it is important to consult a health professional before using acupuncture (31.6%, n = 78). Over half of the participants disagreed with several negatively framed statements about acupuncture, including it being unsafe and ineffective (Q2) or being effective only for minor complaints (Q4), as well as statements about placebo effects (Q5), threats to public health (Q6) and the presence of unqualified practitioners (Q13). Neutral responses were most common for the item on acupuncture being cost-effective (47.8%, n = 118) (Table 2).
Participant attitudes towards acupuncture (adapted CAM attitude scale; n = 247).
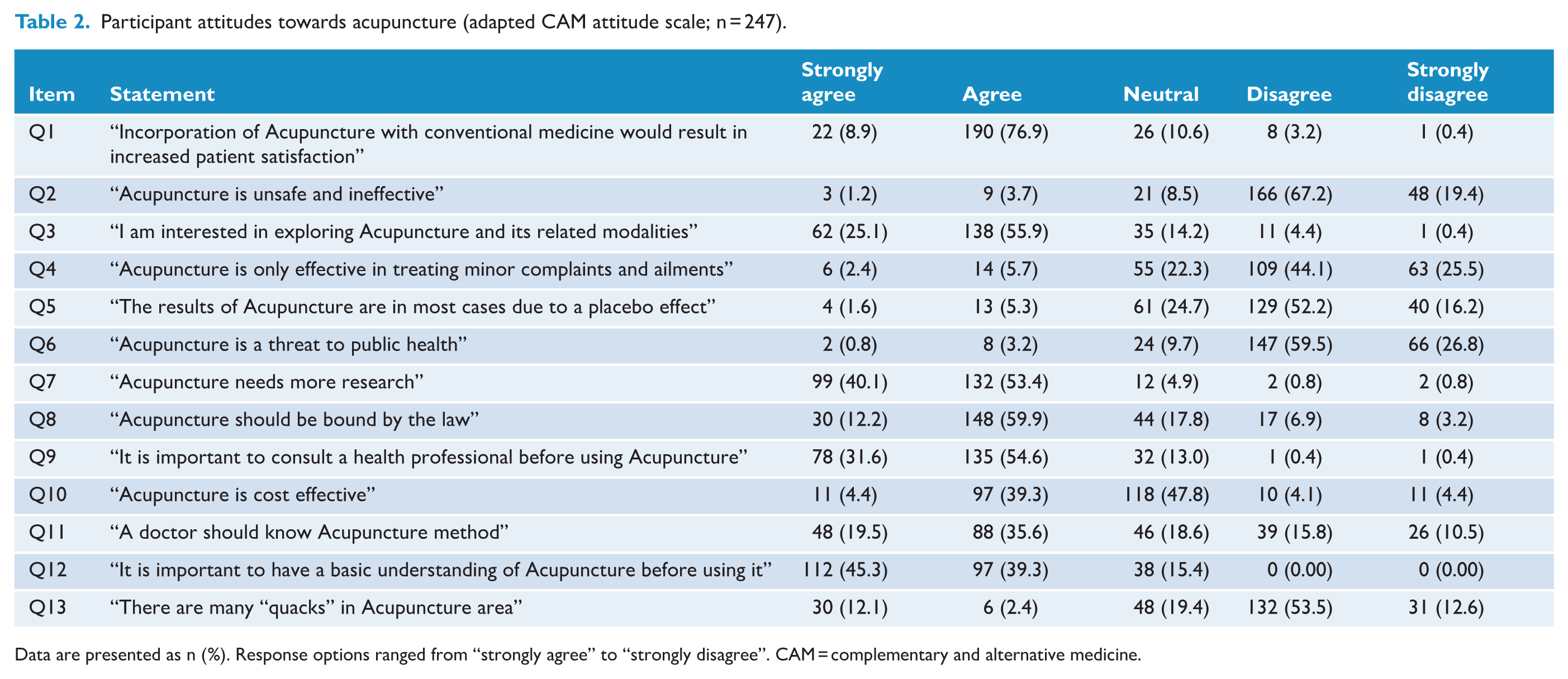
Data are presented as n (%). Response options ranged from “strongly agree” to “strongly disagree”. CAM = complementary and alternative medicine.
Expectancy towards acupuncture
Responses to the AES suggested a moderate level of treatment expectancy among this sample. At the item level, 47.0% of participants (n = 116) expressed moderate agreement that acupuncture could improve their symptoms, and 38.9% (n = 96) mostly agreed that acupuncture could help them cope better with their condition. In contrast, over half of the participants (52.2%, n = 129) did not agree that their symptoms would completely disappear following acupuncture treatment. Expectations regarding increased energy levels were mixed, with 34.4% (n = 85) reporting slight agreement, followed by moderate agreement (24.7%, n = 61) and disagreement (22.3%, n = 55) (Table 3).
Participant expectancy towards acupuncture (acupuncture expectancy scale; n = 247).
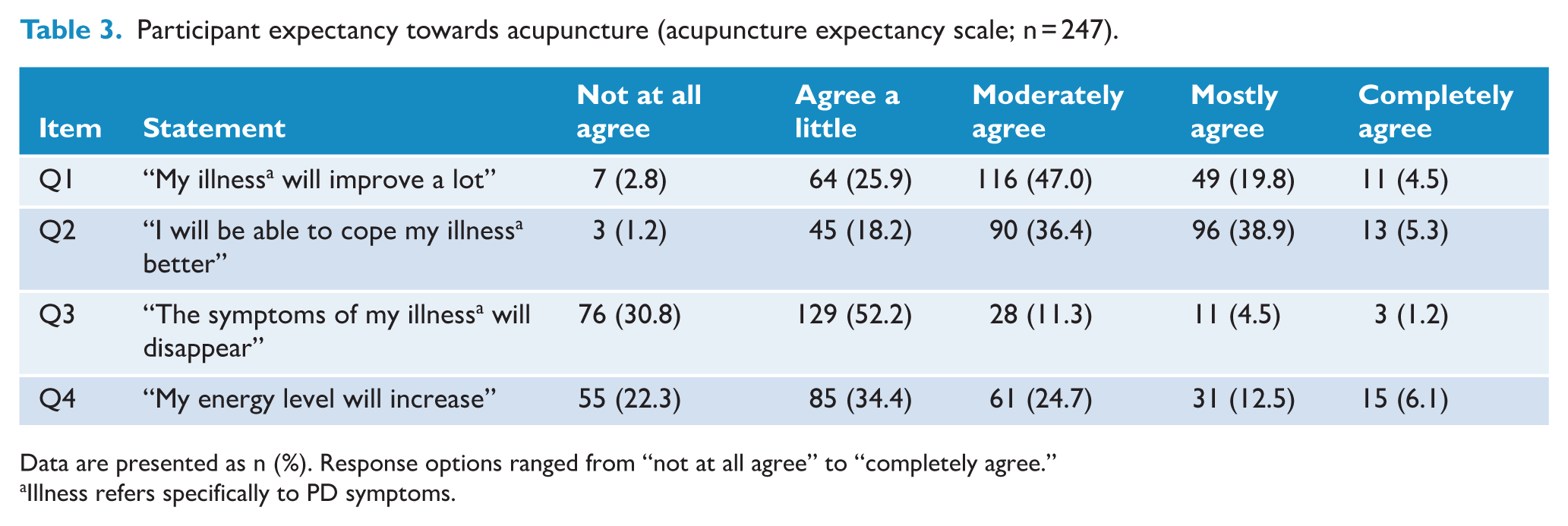
Data are presented as n (%). Response options ranged from “not at all agree” to “completely agree.”
Illness refers specifically to PD symptoms.
Robustness and supplementary analysis
Internal consistency of the adapted CAM attitude scale (Cronbach’s α = 0.789) and AES (Cronbach’s α = 0.758) was acceptable, supporting aggregation of item-level scores for descriptive analysis. Sensitivity analysis comparing the full sample with participants who reported a formal clinical diagnosis of PD showed highly similar item-level response distributions for both attitude and expectancy measures, with consistent dominant response categories across all items (Supplemental Appendix 3: Supplemental Tables S1 and S2).
Exploratory analysis using mean attitude and expectancy scores yielded patterns consistent with the item-level findings. Stratified analysis across demographic and clinical characteristics showed broadly comparable mean scores with overlapping standard deviations; however, these findings should be interpreted with caution given the relatively small size of the non-university subgroup (Supplemental Appendix 3: Supplemental Table S3).
Discussion
Main findings
In this study, item-level responses were consistent with generally favourable attitudes across multiple attitude items; however, the observed attitudes should be interpreted as descriptive response patterns rather than precise measurements of a validated construct, as the instrument was adapted without formal psychometric validation. Treatment expectancy was moderate overall, with participants expressing conditional expectations of symptom improvement and coping benefits. Taken together, these findings suggest that participants tended to view acupuncture favourably while maintaining cautious, differentiated expectations, as captured through a cross-sectional survey of perceptions.
Understanding attitudes and expectations
Favourable attitudes observed in this multicultural Australian sample can be contextualised within broader healthcare and regulatory developments. Substantial support of legal regulation and consultation with health professionals aligns with Australia’s established regulatory framework and may contribute to the high confidence among respondents. Over the past two decades, acupuncture has become increasingly embedded in the Australian healthcare landscape, 22 supported by mandatory practitioner registration introduced in July 2012 and ongoing professional oversight. As of June 2025, there were more than 4000 registered acupuncturists practising in Australia, 23 and the legally protected title of “acupuncturist” may further reinforce public perceptions of safety and trust.
Participants’ support for integrating acupuncture with conventional medicine provides further insights into the dimensions of these favourable perceptions. The belief that integration may enhance patient satisfaction suggests that acupuncture is viewed primarily as a complementary rather than a substitutive therapy. This perspective aligns with clinical guidance supporting the inclusion of CAM therapies, including acupuncture, within integrative approaches to pain management. 24 Evidence from integrative care studies across a range of clinical contexts supports the view that acupuncture may complement standard treatments and enhance overall care experiences.25 –27 At the same time, acknowledged challenges to integration, including institutional constraints, funding limitations and the need for consistent training and evidence standards, highlight that favourable attitudes towards acupuncture coexist with pragmatic awareness of systemic and professional considerations.28,29
Consistent with this balanced perspective, participants reported moderate rather than extreme expectancy regarding acupuncture outcomes. Such levels are clinically relevant, as expectancy is a recognised contributor to non-specific treatment effects and has been linked to pain-related outcomes through contextual and placebo mechanisms, including in acupuncture research. 30 Cross-cultural comparisons show relatively low expectancy in some US samples, 31 and higher expectancy in Chinese populations, 21 while moderate levels comparable to those in the present study have been reported in Korean participants. 32 In this study, a predominantly acupuncture-interested and university-educated sample with self-reported PD exhibited realistic yet moderate expectations towards acupuncture, balancing favourable attitudes against cautious appraisal in a regulated, evidence-oriented healthcare environment. Across the three aforementioned AES studies, expectancy was lower among individuals without prior acupuncture experience;21,31,32 however, in the present study, prior acupuncture use was reported by only a small number of participants, precluding meaningful comparison between users and non-users. Within this context, the observed expectancy levels are best interpreted as descriptive and situated within the broader literature.
Using the health belief model (HBM) 33 as an explanatory framework, the findings reflect conditional receptivity rather than uncritical endorsement. Approximately 81% of participants expressed interest in exploring acupuncture, reflecting perceived benefits and general receptivity shaped by views of safety, legitimacy and compatibility with conventional care. Within the HBM, these favourable attitudes can be understood as conditional and evaluative, indicating openness to considering acupuncture rather than assumptions of assured or universal effectiveness.
At the same time, expectancy regarding treatment outcomes—conceptualised as anticipated benefit rather than experienced effect—was moderate rather than uniformly high. Responses to the AES suggested greater expectation of functional improvement and symptom coping than of complete symptom resolution. While some participants anticipated meaningful improvement, expectations that symptoms would fully disappear or that energy levels would markedly increase were generally restrained. Within the HBM, this differentiated expectancy profile is consistent with anticipated benefits being framed selectively and tempered by pragmatic appraisal of likely outcomes, potentially helping to explain why favourable attitudes and interest did not translate into elevated expectations of efficacy.
Participants’ emphasis on consulting healthcare professionals and acquiring basic knowledge prior to treatment can be conceptualised as cues to action within the HBM. Rather than implying uncritical uptake, these cues appear to orient decision-making towards informed and selective consideration of acupuncture, particularly within a regulated healthcare context.
Taken together, the combination of high interest, generally favourable attitudes and moderate expectancy reflects a structured appraisal process rather than unquestioning endorsement. These views towards acupuncture signal openness to consideration under appropriate conditions, but do not imply assumptions of therapeutic effectiveness or guaranteed clinical benefit, particularly given the low-certainty and methodologically limited evidence reported in both a 2016 Cochrane review, 34 and a more recent systematic review. 35 However, these patterns should be interpreted cautiously, as the use of an adapted, non-validated instrument limits the extent to which these findings can be understood as representing a precisely measured attitudinal construct.
Implications for clinical practice and research
In clinical settings, the findings suggest that acupuncture may be perceived as a treatment option of interest rather than a guaranteed solution. This highlights the importance of open, patient-centred discussions that acknowledge interest in acupuncture, while clearly communicating the current evidence base and the range of possible outcomes. Such discussions may help support informed decision-making and align treatment expectations with individual preferences and clinical considerations.
For research, item-level differentiation in expectancy underscores the value of exploring nuanced perceptions regarding symptom management versus complete resolution. Qualitative or mixed-methods approaches could further explore how attitudes and expectations are formed, how they influence treatment engagement, and how women interpret perceived benefits in the context of PD. Longitudinal designs may also help clarify how expectations evolve over time and in response to treatment experiences. Importantly, the current findings should be interpreted in light of the sample composition, as women who were not interested in acupuncture and those with lower educational attainment were underrepresented. This is particularly relevant because the predominance of acupuncture-interested and university-educated participants is likely to have contributed to the generally favourable attitudes observed. Future studies should therefore specifically examine attitudes and expectations in these underrepresented groups to better understand the broader applicability of the findings.
Strengths and limitations
This study has several strengths. First, the item-level analysis in this study allowed a more detailed assessment of response distributions beyond aggregated mean scores. Second, the inclusion of sensitivity analysis comparing participants with and without a formal clinical diagnosis of PD provided additional descriptive insight, with broadly similar response distributions observed across these groups. Third, the use of a validated AES supports the measurement’s validity and enhances comparability with prior research. Finally, mandatory survey items, screening procedures and multiple data-quality checks were implemented to reduce the likelihood of incomplete, duplicate or geographically ineligible responses.
Several limitations should be considered when interpreting these findings. Attitudes towards acupuncture were assessed using an adapted version of a CAM scale that has not undergone psychometric validation in its modified form. Replacing “CAM” with “acupuncture” is likely to have altered item interpretation and introduced response bias, as acupuncture arguably represents a more specific and familiar treatment. Participants may therefore have drawn on prior experiences or beliefs when responding. Consequently, responses may not be directly comparable to those obtained using the original validated instrument, and findings might differ if the unmodified scale were applied. Although internal consistency was acceptable, the items likely capture multiple related dimensions of attitudes rather than a single unified construct. Therefore, findings regarding favourable attitudes should be interpreted as descriptive response patterns, reflecting a general tendency towards favourable endorsement of item content rather than as precise estimates derived from a fully validated composite scale.
The cross-sectional design and the descriptive, exploratory nature of the analysis limit the ability to explain underlying mechanisms or temporal relationships, as the data were collected at a single time point. 36 Although stratified and sensitivity analyses were conducted, the relatively small size of the non-university-level education subgroup (n = 55) limits the robustness of subgroup comparisons and precludes meaningful inferential conclusions. In addition, multivariable modelling was not performed, so independent associations or causal relationships cannot be inferred. The findings should be interpreted as reflecting observed patterns within this sample rather than explanatory relationships.
The sample was not fully representative of the broader population. There was a predominance of university-educated participants and a relatively higher representation of individuals identifying as African. These patterns are likely attributable to the study setting and the recruitment strategy. As the study investigators were affiliated with a university in Western Australia, recruitment through academic and professional networks may have preferentially reached individuals with higher educational attainment, contributing to geographic clustering. In addition, participation in an online, self-selected health-related survey may have further contributed to this pattern, as such surveys tend to attract individuals with higher levels of education.
The relatively higher representation of participants identifying as African may be explained by social network clustering inherent in online recruitment, whereby study information circulates within interconnected social and community networks. Such network-based diffusion may have amplified participation from specific groups, including African communities, and should be considered when interpreting the findings, as it may limit the generalisability.
A substantial degree of self-selection bias appeared to be present, with 81% of participants reporting an interest in exploring acupuncture. This suggests that the sample largely comprised individuals with an existing interest in acupuncture, which likely inflated the overall favourability of attitudes observed. Consequently, the findings should not be generalised beyond this acupuncture-interested sample. In addition, the English-speaking context of the study may further limit transferability to other populations and healthcare settings.
All data were self-reported and could not be independently verified, introducing potential misclassification, particularly in distinguishing primary from secondary dysmenorrhoea. As with any Internet-based survey, the possibility of inauthentic responses cannot be entirely excluded despite the implementation of quality-control procedures. Although restrictions based on IP addresses were implemented, these measures could potentially be bypassed through the use of different devices or networks, and no formal identity verification was undertaken. This may be particularly relevant given that 43.3% of participants reported no formal clinical diagnosis of PD, increasing the likelihood of inclusion of off-target respondents. While the anonymous and non-incentivised design may have reduced the incentive for intentional misrepresentation, it does not eliminate this risk.
Conclusion
This study identified generally favourable attitudes towards acupuncture across item-level measures, alongside moderate treatment expectancy, within a self-selected sample predominantly comprising university-educated individuals with an interest in acupuncture. These findings reflect perceived acceptability and interest in this voluntary, online sample, rather than population-level perspectives or evidence of clinical effectiveness. As the attitudes were assessed using an adapted instrument without formal psychometric validation, they should be interpreted as indicative of response tendencies rather than precise measurement of a validated construct. Future research should examine attitudes and expectations towards acupuncture among women without a prior interest in acupuncture and those with lower educational attainment and explore the contextual and experiential factors that influence how acupuncture is evaluated and integrated into women’s health care.
Supplemental Material
sj-pdf-1-aim-10.1177_09645284261458839 – Supplemental material for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia
Supplemental material, sj-pdf-1-aim-10.1177_09645284261458839 for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia by Weiting Liu, Amanda Towell-Barnard, Khui Hung Lee and Timothy Leen Kang in Acupuncture in Medicine
Supplemental Material
sj-pdf-2-aim-10.1177_09645284261458839 – Supplemental material for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia
Supplemental material, sj-pdf-2-aim-10.1177_09645284261458839 for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia by Weiting Liu, Amanda Towell-Barnard, Khui Hung Lee and Timothy Leen Kang in Acupuncture in Medicine
Supplemental Material
sj-pdf-3-aim-10.1177_09645284261458839 – Supplemental material for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia
Supplemental material, sj-pdf-3-aim-10.1177_09645284261458839 for Attitudes and expectations towards acupuncture for primary dysmenorrhoea: Findings from a cross-sectional survey in Australia by Weiting Liu, Amanda Towell-Barnard, Khui Hung Lee and Timothy Leen Kang in Acupuncture in Medicine
Footnotes
Acknowledgements
We would like to extend our gratitude to the administrators and staff at Edith Cowan University for their assistance in survey distribution, as well as to the individuals who contributed their support. Our sincere appreciation also goes to the participants who responded to our survey.
Ethical statement
This research obtained approval from the Edith Cowan University (ECU) Human Research Ethics Committee (REMS NO.2023-04471-LIU).
Author contributions
Conceptualisation: Weiting Liu, Amanda Towell-Barnard. Methodology: Weiting Liu, Amanda Towell-Barnard, Khui Hung Lee. Data curation: Weiting Liu, Khui Hung Lee. Writing – original draft preparation: Weiting Liu. Writing – review and editing: Amanda Towell-Barnard, Khui Hung Lee, Timothy Leen Kang. Supervision: Weiting Liu. All authors read and approved the final version of the manuscript accepted for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the project on Edith Cowan University Higher Degree by Research (S0059).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.