
Abstract
Operative nerve-stretching was first described in 1872 to relieve incurable pain from sciatica and tabes dorsalis. It became popular for 20 years and numerous articles were published on the subject. It had many complications but relief was only transient and, consequently, it fell into disuse. This paper analyses the literature, contemporary views on the benefits of nerve stretching and its influence on more recent neurological practice.
Introduction
In the second half of the 19th century, neurology was emerging as a separate discipline. The understanding of the anatomy and the pathophysiology of the central nervous system was well advanced with contemporary descriptions of diseases clearly recognisable today yet treatment for neurological disorders was limited. Doctors did not operate on the brain or the spinal cord. Treatment consisted of electrical stimulation, massage, hypnosis, anaesthesia and the administration of morphine. Operative nerve-stretching, sometimes known as neurectasy, was first described in 1872 to relieve incurable pain or neuralgia. 1 This unorthodox procedure became popular for more than 20 years with variants of the initial concept in the form of massage and friction of the nerves, non-operative stretching and percussion/irritation of the nerves. After the initial enthusiasm, patients suffered frequent relapses and the practice was discredited. This article reviews the history and the contemporaneous literature on nerve-stretching, describes the methodology and resulting physiological investigations and analyses the influence of nerve-stretching on neurological practices in the 20th century and beyond.
Historical background
In 1872 Theodor Billroth (1829–1894), a Prussian-born Austrian surgeon (see Figure 1), operated on a woman suffering from sciatica. She experienced total relief of pain despite the fact that he merely exposed and examined the sciatic nerve. A German surgeon, Johan Nepomuk Von Nussbaum (1829–1890), attributed the result to surgical manipulation and stretching of the nerve and during that same year he operated on a soldier suffering from brachial neuralgia following a blow to the neck with a rifle. He intentionally stretched the nerves, which form the brachial plexus and the soldier was cured.
2
These successes generated enthusiasm within the medical profession and the procedure became popular. Most accessible peripheral and cranial nerves were subjected to the procedure and, while pain relief was the main objective, this new therapy was applied to many incurable neurological conditions. It is virtually forgotten today but for a time it was widely endorsed.
Christian Albert Theodor Billroth. Photograph by F Luckhardt.
Anthony Bowlby (1855–1929), John Marshall (1818–1891), William Gowers (1845–1915) and Henry Charlton Bastian (1837-1915) gave detailed accounts of the procedure.1,3–5 In his textbook devoted exclusively to nerves, Bowlby dedicated two chapters (60 pages) to the technique and made reference to more than 60 British and International publications on the subject, indicating the procedure was widely practised in Western Europe and in the United States. In 1872 Weir Mitchell, the foremost neurologist in the United States, described traumatising the nerves for the treatment of causalgia. 6 On 15 May 1878, J Symington addressed the Medico-Chirurgical Society of Edinburgh on ‘The Physics of Nerve-Stretching’ and on 6 December 1883 Marshall, then President of the Royal College of Surgeons, delivered the Bradshaw Lecture at the Royal College of Surgeons of England on ‘Nerve-stretching for the relief or cure of pain’, evidence that the treatment was endorsed by his peers and sufficiently important to be worthy of a lecture.7,8 The following year, Marshall reviewed 252 cases of nerve-stretching described in the literature. Jean-Martin Charcot (1825–1893), the doyen of experimental neurology, did not write about nerve-stretching. 8 William Hammond (1828–1900), Adolf Strumpell (1853–1899) and later Hermann Oppenheim (1858–1919) and Samuel Kinnier-Wilson (1878–1937) (as late as 1940), all described the role of nerve-stretching.9–12
Methodology
Marshall (see Figure 2) observed that nerves could be stretched through open operation or by non-surgical mechanical stretching but, since both procedures required the use of anaesthesia with chloroform or ether, the latter did not bring an undue advantage.
13
Practitioners used broadly similar techniques.
John Marshall photograph by J Jerrard.
Operative nerve-stretching
This technique (see Figure 3) was employed most commonly upon the sciatic nerve. Doctors carrying out the incision applied antiseptic precautions as directed by Joseph Lister (1827–1912). Hammond used anaesthesia although French doctors thought an anaesthetic was contra-indicated. Hammond described the procedure:
9
I make an incision four or five inches in length through the skin and aponeurosis, and expose the nerve. I then pass an ivory paper-knife, and gradually lift the nerve from the bottom of the wound, stretching it to the extent of three or four inches, while making the traction as far as possible in a downward direction. In the last case, I put my index finger under the nerve and lifted it out of the thigh with much more ease and with less risk of injury than before, and this is certainly the preferable procedure. The object being to carry the extension to the point of producing very decided numbness … for several days subsequently there have been numbness and paresis but these phenomena have gradually disappeared and without being followed by a return of pain.
Stitched wound resulting from operation for stretching the sciatic nerve, 1882, taken from Antiseptic Surgery by Cheyne W Watson.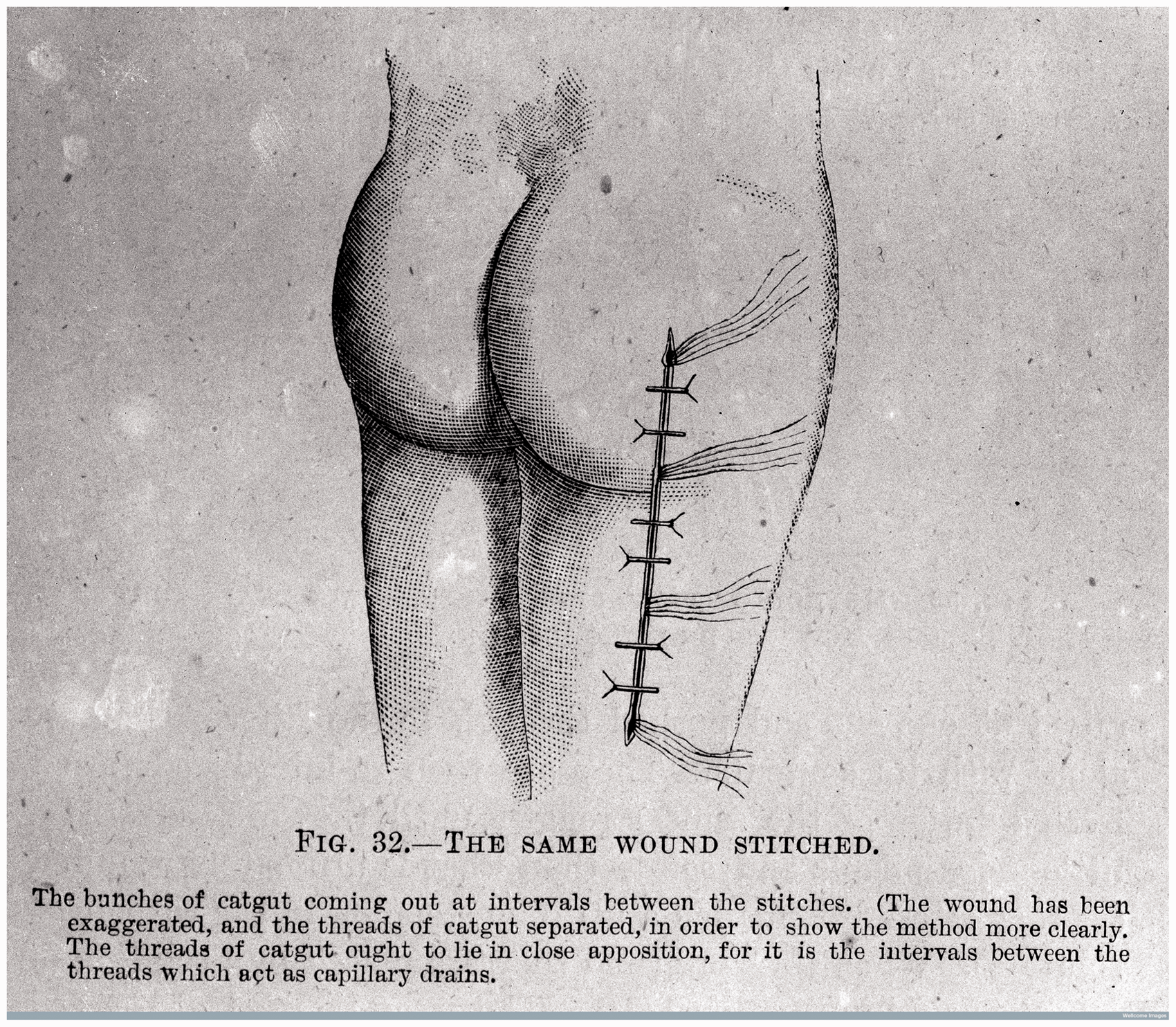
Bastian modified the technique by pulling the nerve in both directions with the fingers rather than a hard object so as not to injure the nerve fibres. 5
Bowlby (see Figure 4) suggested it was advisable to render the limb bloodless by the application of Esmarch's bandage before undertaking the procedure. He also recommended using a weight of 30 lbs to stretch the nerve using a hook and, in the case of a small nerve such as the trigeminal nerve, an aneurysm needle.
1
Sir Anthony Alfred Bowlby. Photograph by Doris V Jaeger.
Non-operative nerve-stretching
The open operation was not the only way to ‘distress the nerve’. Stretching of the sciatic nerve could be achieved by flexing the thigh upon the body so that the knee comes up to the chin and the leg is straightened upon the thigh. Flexing the foot upon the leg to stretch the ankle joint caused maximum tension upon the sciatic nerve. This non-operative procedure was applied successfully to the treatment of tabes dorsalis before the use of suspension became popular. Non-surgical procedures were used mostly when the nerve was inaccessible. Marshall described how he used compression for the treatment of two cases of neuralgia of the testis. With an apparatus similar to a lemon-squeezer, he subjected the spermatic cord to pressure strong enough to break up the axis cylinder of the spermatic nerve with complete relief in both instances. 9
Indications
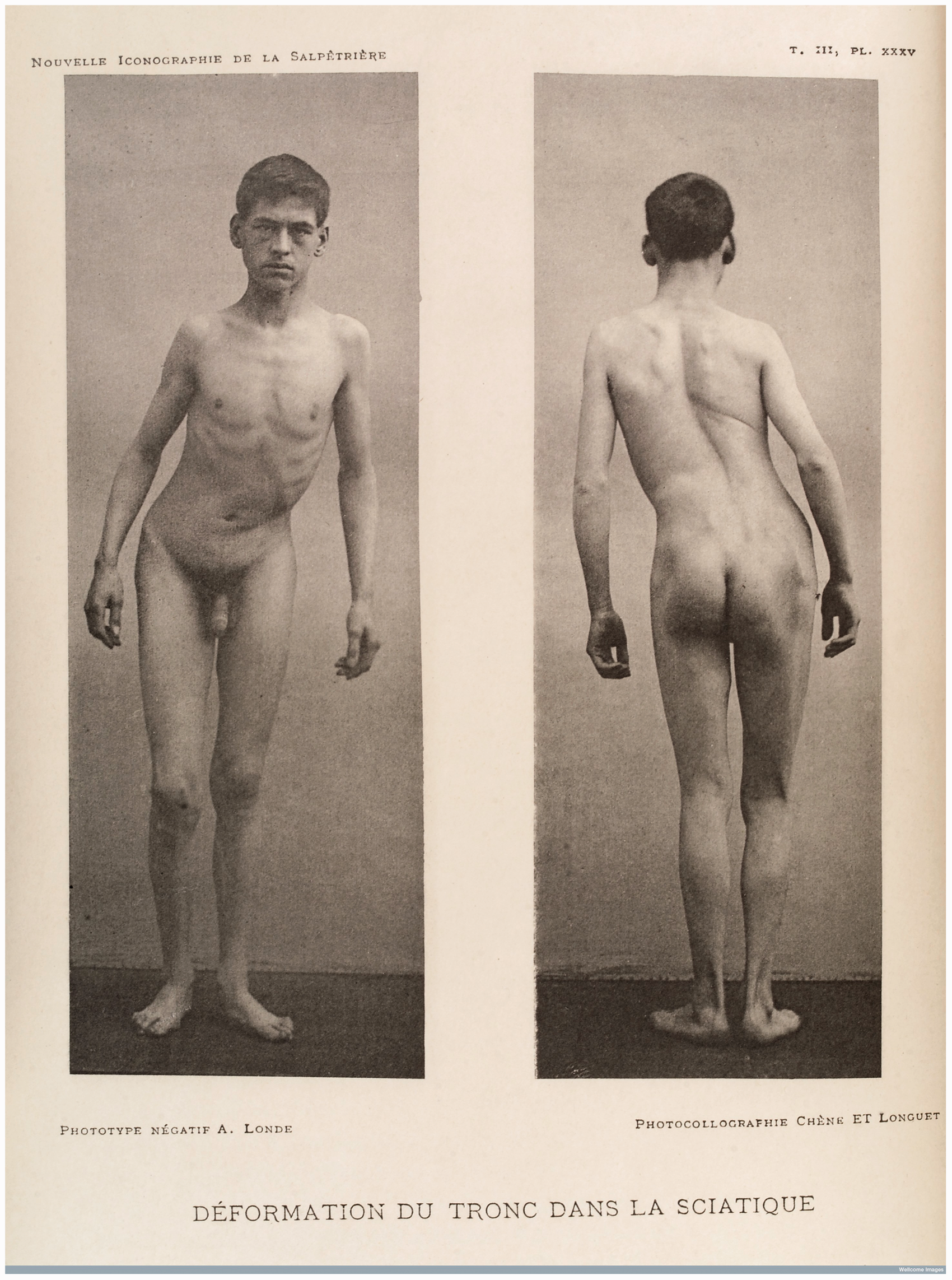
Frequently nerve-stretching (see Table 1) was used to treat the pain associated with sciatica (see Figure 5), possibly either because the sciatic nerve was easily accessible or because the condition was so intractable. James Paton Bramwell (1824–1890) justified the operation thus:
14
The operation is a very simple one and not for a moment to be compared with the suffering of some sciatic cases.
Front and back views of a young man whose body trunk has been deformed through sciatica. Bears the caption: ‘Deformation du tronc dans la sciatique’, c. 1890 taken from ‘Nouvelle Iconographie de la Salpêtrière; Clinique des Maladies du Système Nerveux’. Results of 252 cases of nerve-stretching in disease.
8

Results and complications
I would not feel justified holding out any prospect of a complete and permanent cure of tabes using nerve-stretching. … failure is more probable than success … relief is more likely to be transient than permanent.
Nocht's results of nerve-stretching.
8

By contrast Marshall presented a statistical analysis of all 252 cases reported in the literature. The only conditions which responded to treatment were neuralgia and to a lesser extent tabes dorsalis: ‘ … enormous success for neuralgia but less success for tabes’, ‘temporary sensation of pain’. 8 Marshall interpreted the results with caution as failures went unrecorded, pain was subjective, patients were over-hopeful and wanted to please the doctors, surgeons wanted to achieve good results, there was insufficient follow up and recurrences passed unnoticed. He still favoured nerve-stretching for the treatment of neuralgia, stating: ‘you will not dispute the fact that it often does and will cure that disease’. 8
He presented another 70 cases treated by Albrecht Nocht (1857–1945) (see Figure 6); 10 suffered from tabes dorsalis and 7 of these improved.
Albrecht Eduard Bernhard Nocht, photograph.
Despite the use of antiseptic techniques, a significant number of patients died from complications brought on by general anaesthesia or following an infection of the incision wound or through thrombosis. Some practitioners used only local anaesthesia.
Bowlby recorded nine deaths as a result of myelitis, meningitis, infected bed sores, epilepsy, injury to the sacral nerve, haemorrhage of the spinal cord and membranes leading to meningitis, suppuration of the wound followed by incontinence and acute pyelonephritis. 1 He commented that nerve-stretching showed the usual complications associated with any surgical incision including lacerations leading to suppuration that travelled along the nerve from the seat of the wound. He reported abscesses extending from the sciatic notch to form an abscess half way down the thigh. He suggested that this was particularly dangerous as the nerves are in continuity with the spinal cord. Not all cases with cord involvement were fatal and Bowlby reported cases of paralysis of the opposite leg, of the bladder and the bowels, with severe cystitis and incontinence. He also recorded cases following non-operative stretching where post-mortems showed haemorrhage along the sciatic nerve and involvement of the dura matter. Remarking that several of the deaths occurred in cases where several nerves were stretched in one operation, Bowlby recommended a time interval between stretching two large nerves.
Marshall was less critical in his review of the cases and considered that:
8
With regard to the dangers of nerve-stretching in tabes, if you read the cases you find there are comparatively few. One patient died from chloroform, another from thrombosis in the veins, another from pyaemia due to inattention to antiseptic, a fourth from a similar cause. We may record three or four cases in which undoubtedly the death may be attributed to disease of the spinal cord set up by nerve-stretching but one of these was a case of spasmodic disease. These mishaps have taken place in other operations. A boy had his hips and knees contracted, he had these stretched and collapsed and died two or three days later.
Discussion
Nerve-stretching was a dramatic, dangerous and bizarre form of treatment with a high morbidity and mortality yet it achieved great popularity. Its main indication was for the treatment of intractable pain, particularly neuralgia (in sciatica) and tabes. Pain, a subjective experience, is ill-understood and poorly treated today. At the end of the 19th century, doctors were still influenced by Hippocrates' theory of humours and believed that in order to effect a cure conditions had to reach a point of crisis in order to disperse, and pain was an inherent and necessary part of the process. 15 Further influence came from the church and the biblical belief that brought a fatalistic view of pain: ‘In pain you will bring forth children’. 16 Doctors thought pain was a necessary element of a successful operation and attempting to remove pain could delay the healing process and so they were reluctant to eliminate it altogether. They would also inflict greater pain through the administration of moxas (poisonous substances that would cause an infection or ulcer which was very painful) to ‘distract’ from the original lesser pain. 15
Experimental medicine was fundamental in the elucidation of organic disease including stroke but the mechanics of pain did not yield to experimentation. The anatomical basis for the transmission of pain was in its infancy and ill-understood. In 1852, Johannes Purkinje (1787–1869) and Rudolf Kölliker (1817–1905) demonstrated that nerve cells had a main body (the nucleus) and a fibrous ‘tail’ extending from the main body. The long tails were actual nerve fibres and every such fibre had a parent body several feet distant from the nerves, as with the nerves of the toes. In his histological studies Kölliker showed how ‘Nerve fibres were secondary to nerve cells and at least some of them were the processes of nerve cells’. 17 In 1852, Charles Edouard Brown-Séquard (1817–1894) demonstrated that the spino-thalamic tract was responsible for the transmission of pain impulses from the periphery. 18 The causes of two diseases treated with nerve-stretching, sciatica and tabes were not understood. The relationship of sciatica to a prolapsed disc in the lumbar region was not established until 1934, by Mixter and Barr. 19 Since there was tenderness over the sciatic notch and muscle tenderness, sciatica was attributed to inflammation of the nerve. 20 While the lightning pains of tabes dorsalis were recognised as a late manifestation of syphilis, their relationship to the spinal cord or posterior nerve roots was not established. Doctors treated the pain locally and nerve-stretching became popular for the treatment of the intractable pain associated with sciatica and tabes dorsalis.
Experiments showed that traction upon the peripheral nerves was not transmitted to the spinal column or the spinal cord. Post-mortem studies showed the amount of elongation of the nerves and the forces exerted before the nerve fractures. The nerves of the upper limb are more extensible than those of the lower limb and the sciatic nerve could sustain traction equal to half the body weight before breaking. Victor Horsley (1857–1916) (Figure 7) demonstrated that nerve-stretching led to a decrease in the diameter of the nerve and damage to the nervi nervorum, the small nerve fibres in the sheaths of the peripheral nerves. It also affected the perineurium which in the un-stretched nerve seemed to be wavy and loose within the sheath but in the stretched nerve perfectly straight.
Portrait of Victor Horsley, 1916.
There was speculation about the effect of nerve-stretching. Marshall attributed the benefits of nerve-stretching in sciatica to the interference with the nervi nervorum. These nerves were more susceptible to stretching than the major trunks of the nerve inside:
8
… the nerve tubuli, the extremities of which are fastened into the sheath must be stretched so as to be paralysed completely … Nerves, whilst very elastic, are only capable of a small amount of stretching.
Leaders of the profession Bowlby, Gowers, Silas Weir-Mitchell (1829–1914), Hammond, Strumpell, Oppenheim, Kinnier-Wilson and Samuel Wilks (1824–1911) did not write specific papers on nerve-stretching but their textbooks of neurology reflect the contemporary accepted views.1,4,6,9,10–12,21 They evaluated the role of nerve-stretching in various diseases and thought it could play a role in the treatment of sciatica. Hammond and Kinnier-Wilson found it offered immediate relief but Gowers and Strumpell were less enthusiastic:
10
… Experience however has taught us that nerve-stretching in spite of some initial successes, scarcely ever exerts a permanent favourable action and is also not wholly without danger.
Influence of nerve-stretching on the treatment of neuralgia
Nerve-stretching did not address the fundamental cause of a disease and therefore failed to cure the majority of conditions and the frequent relapses after the initial improvement led to an abandonment of this treatment although Hammond persisted in its use for the treatment of athetosis until 1920. While nerve-stretching both operatively and non-operatively fell into disuse, it drew doctors’ attention to the function of the nerves and variants of the procedure persisted for 50 years. Otfrid Foerster (1873–1941) divided the posterior nerve roots to treat gastric crisis in tabes but this was abandoned due to unpredictable results.22,23 He pursued the transmission of pain proximally in the spinal cord and carried out a spino-thalamic cordotomy by cutting the lateral column.
Adams in 1959 made an attempt to revive the procedure some 80 years after it was abandoned. 13 By this time, the source of sciatica in many cases had been identified as being a prolapsed disc and as a result surgeons were slavishly operating upon the discs and carrying out spinal fusions to treat all forms of sciatica. Adams used this procedure when dealing with a ‘failed back’ after disc surgery had failed due to adhesions and incomplete removal of the disc; he treated 40 patients with this procedure, 30 of whom had had previous removal of the disc. He only achieved success in two of the patients and he stated that it was only when there were dense adhesions around the nerve that stretching it resulted in any benefit. No other surgeon repeated this procedure.
Perhaps the most interesting application of an attack on the peripheral nerves in pain therapy was first demonstrated by Weir Mitchell who observed that in causalgia the nerve stump was painful and he massaged and traumatised the nerve to treat this difficult condition. 15 This work was followed up in 1949 by Ritchie Russell (1903–1980) who pursued the treatment successfully in painful amputation stumps by hammering the neuromas. 24
Nerve-stretching is no longer used as a formal therapy but it is experienced iatrogenically. Initially mentioned by Marshall, limb lengthening is carried out and nerves can be traumatised. The nerves are able to sustain up to 25% lengthening but, beyond this, severe damage occurs with serious and intractable injury with paralysis of motor, sensory and sympathetic function with a poor prognosis for spontaneous recovery and poor results from surgical repair since there is considerable longitudinal damage to the nerves.
Physiotherapists will use hands on techniques which can help reduce neural tension and tethering called ‘neural glides’. 25
Today the practice of nerve-stretching, either operatively or by closed traction as a therapeutic measure, has been abandoned but it is a product of other measures practised until 60 years ago. When John Silver was a medical student and a registrar in orthopaedics, manipulation under an anaesthetic was commonly practised to treat back pain. This would involve flexion of the hip thereby stretching the sciatic nerve although this was not the prime object of the treatment. Occasionally surgeons carry out manipulation but it is not practised regularly by orthopaedic surgeons.
Chiropractors do manipulate the spine by thrusting down and applying pressure upon the vertebrae beyond the normal range but this does not generally involve flexion of the hip and stretching of the sciatic nerve. These procedures have given rise to ruptures of the disc, causing nerve palsies and even paraplegia and for this reason have been abandoned.
Conclusion
At the zenith of its popularity, there were numerous papers presenting the results of nerve-stretching particularly for the treatment of sciatica. Authoritative textbooks reviewed its place in treatment but, after it was abandoned, the subject has been forgotten and is barely mentioned. In the last 30 years, three papers allude to it.
JR Keane (1990) presents a short history of therapeutic nerve-stretching and suspension and critically evaluates its use in the treatment of sciatica and tabes and the complications. 26 O Sugar (1990), in a meticulous paper describes the pathological basis of nerve-stretching by Horsley. 27 DJ Lanska (2013) reviews the role of nerve-stretching for the treatment of athesosis. 2 Walker's textbook on the history of neurosurgery gives a brief mention of nerve-stretching by Bowlby for the treatment of peripheral nerve injuries. 19 McHenry, Clifford-Rose, Bogousslavsky and Finger do not mention it.
Doctors, desperate for a cure, believed it offered relief from the intractable pain of neuralgia and tabes dorsalis. It was not without danger and more so since doctors did not understand the physiological relationship of the central nervous system to the peripheral nerves and they attacked the nerves locally where the pain manifested itself. The technique was soon abandoned but a legacy remains in the form of traumatising the nerve in amputation stumps as practised by Weir Mitchell and later Ritchie Russell.
Footnotes
Acknowledgements
We are grateful to Rolfe Birch, Trevor Hughes, Eric Nieman and Kit Wynn Parry for their valuable input. We would like to thank the Wellcome Library, London for permission to reproduce the illustrations.