
Abstract
Edward S. Miller was born into slavery in 1858. After navigating the racist educational system in Kentucky, he moved north to seek greater opportunities. In Chicago, he obtained medical training, built a practice in the Black community, and participated in the growth of Provident Hospital. He earned broad respect and expanded his networks, serving in the Spanish American War as a field surgeon for a unique Black volunteer regiment. He prospered as an entrepreneur and civic leader, using the power of community networks to help found the first Black cemetery and a federally chartered bank in Chicago, both of which supported the Black community. Miller was a respected civic leader and physician whose story illustrates the complexity and challenges of the medical system in the north at the turn of the 20th century and the resourcefulness needed by a Black leader to succeed in a segregated society.
Keywords
Introduction
Black American physicians have contributed to the health of their communities both directly and indirectly by improving access to healthcare. 1 However, their contributions to the social cohesion and economic stability of the Black community have received little attention. This biography focuses on Edward S. Miller, M.D., grandfather of Paul Miller and Vivian Lewis. He was an African-American physician who went to Chicago to train in medicine and practiced from 1893 to 1938. Beyond the medical benefits of his work, his civic involvement and entrepreneurial spirit helped create job opportunities and improve the quality of life for his community. 2 His accomplishments required intellect, dedication, persistence, selflessness, and a deep-seated desire to alleviate suffering. They also required an empowered Black community. This biography will explore the challenges he faced from a racist system and economic obstacles in his path toward career success. How did family, community, and professional networks in Miller's community enable him to succeed despite these challenges?
To answer this question, we sought out and studied newspapers, magazines, government reports, and other documents published during Miller's lifetime. Many of the newspapers and images were available only through special collections: the Vivian Harsh Research Collection of the Chicago Public Library, the Abakanowicz Research Center at the Chicago History Museum, and the archives of the Abraham Lincoln Presidential Library and Museum. We used US Census reports and property inventories of slaveholders to help confirm timelines. These sources were supplemented by books and medical journals. Finally, we used selected interviews with Miller's family.
Born into slavery in Garrard County, Kentucky, in 1858, Edward S. Miller became a physician in 1893 by seeking and exploiting every opportunity for formal education. Starting in poverty, he became a successful practitioner, property owner, and community leader. Persistence and hard work helped him grow a critical social network that included family and church members, fellow war veterans, civic organizations, and businesspeople. With their support, he built a large private practice, served in the nation's first Black-owned hospital, earned honors as a field surgeon to a first-of-its-kind army regiment of Black volunteers, and helped to found a Black cemetery and the first African-American-owned national bank.3,4
Preparation for a medical career in the 19th century
Childhood and family influences
For newly emancipated enslaved persons, securing food and shelter were vital priorities, but Miller moved far beyond subsistence living. His biological father was probably John Miller, a free Black man. However, his mother, Susan Penman, along with Edward and his siblings, were enslaved in Garrard County and owned by Ormond Beatty (Beatty Family Papers, Centre College Archives), a former president of Centre College. 5 Susan was often “rented out to the family of a Presbyterian minister, who though harsh and cruel in many ways, did not want to be surrounded by ignorance, so had his slaves taught to read and write.” 6 After the Civil War, Susan worked in Kentucky as a domestic and seamstress and married Samuel Davis, a Union Army veteran who achieved emancipation through his military service. 7 Reading was a regular practice in the home. Susan Penman's granddaughter, Susie Jones, recalled in a 1978 oral history: “My mother's mother had great influence on my life. … When my two oldest children were three or four, I took them to see her, and she recited for us, sitting in her rocking chair on the front porch, all of Byron's Prisoner of Chillon.” 8
Miller and his siblings were able to attend the local school, until it was destroyed by the Ku Klux Klan. 9 The nearest town, Danville, Kentucky, had a single sabbath school that started in a local church in 1868 and enrolled 104 students, both adults and children. Sabbath schools began before the Civil War, enabling Whites and free Blacks to attain basic literacy by studying Biblical texts. 10 During Reconstruction, these schools were sometimes supplemented by the Freedmen's Bureau, but it lacked the resources to build and staff all of the schools needed as the South began to rebuild. Before establishment of Freedmen Schools, access to primary education for Blacks was limited to a handful of subscription-funded private schools (35 for all of Kentucky, serving over 4000 students). In Danville, the only school open to Black children was established by the American Missionary Association. It depended on tuition fees collected from students to cover extra expenses, such as schoolhouse upkeep and salary supplements. 10
Two hundred Freedmen schools convened in Kentucky churches and rented spaces to serve adults and children.
11
These greatly expanded the educational resources available to African Americans, but local pressure, harassment, and arson forced many to close. In his 1869 survey of Freedmen schools, the superintendent commented: I believe Kentucky is now the only portion of the habitable world where men are beaten and stoned for instructing the inner ignorant. … This bitter hostility to the education of the Negro … has made it impossible to secure much aid from the benevolent associations. The Bureau and freedmen must meet the main expense.
10
Advanced education
When Reconstruction ended in 1876, federal troops were removed from the South. The Jim Crow era brought systematic segregation, lynchings, and racist legislation; advanced education for Blacks became even more scarce. Centre College, located in Edward's home city of Danville, would not accept African-American students until 1958. 13 Knowing the local threat posed by vigilantes 9 and seeking better educational and career prospects, Edward decided to move north.
In Danville, Miller was already working as a barber. 14 He moved to Meadville, Pennsylvania, where his uncle Russell Penman had a barber shop on Main Street. Penman hired his nephew and mentored him in business. Since the early 18th century, barbering was a common occupation for African-American entrepreneurs, who often exercised skills now associated with the healthcare profession, such as “pulling teeth and lancing boils.” 15 Miller barbered to pay tuition at Allegheny College, which accepted women and a few Blacks, completing a 2-year college-level curriculum before moving to Chicago in the late 1880s to pursue a medical career. 3
Medical education at the turn of the 20th century
In the late 1800s, medical education offered new options for Blacks, despite widespread segregation. Medical schools were proliferating, although many were more entrepreneurial than educational. No national standards existed for coursework, faculty numbers, or graduation requirements. Chicago needed more physicians, as rapid population growth and poor sanitation contributed to a heavy disease burden, especially in Black neighborhoods. 16
Edward Miller graduated with honors from the Chicago Homeopathic Medical College in 1893 and obtained his Illinois medical license. This college was founded by a group of Hahnemann Medical College faculty, who left the Hahnemann in 1876 to create higher standards and broader training in basic medical studies (Figure 1). Using Cook County Hospital as a training site, both schools had adequate resources for clinical coursework. The Chicago Homeopathic Medical College thrived for two decades, but by the turn of the century, it rejoined Hahnemann Medical College because both faced uncertain economic prospects and stiff competition for students from over 10 area medical schools. 16
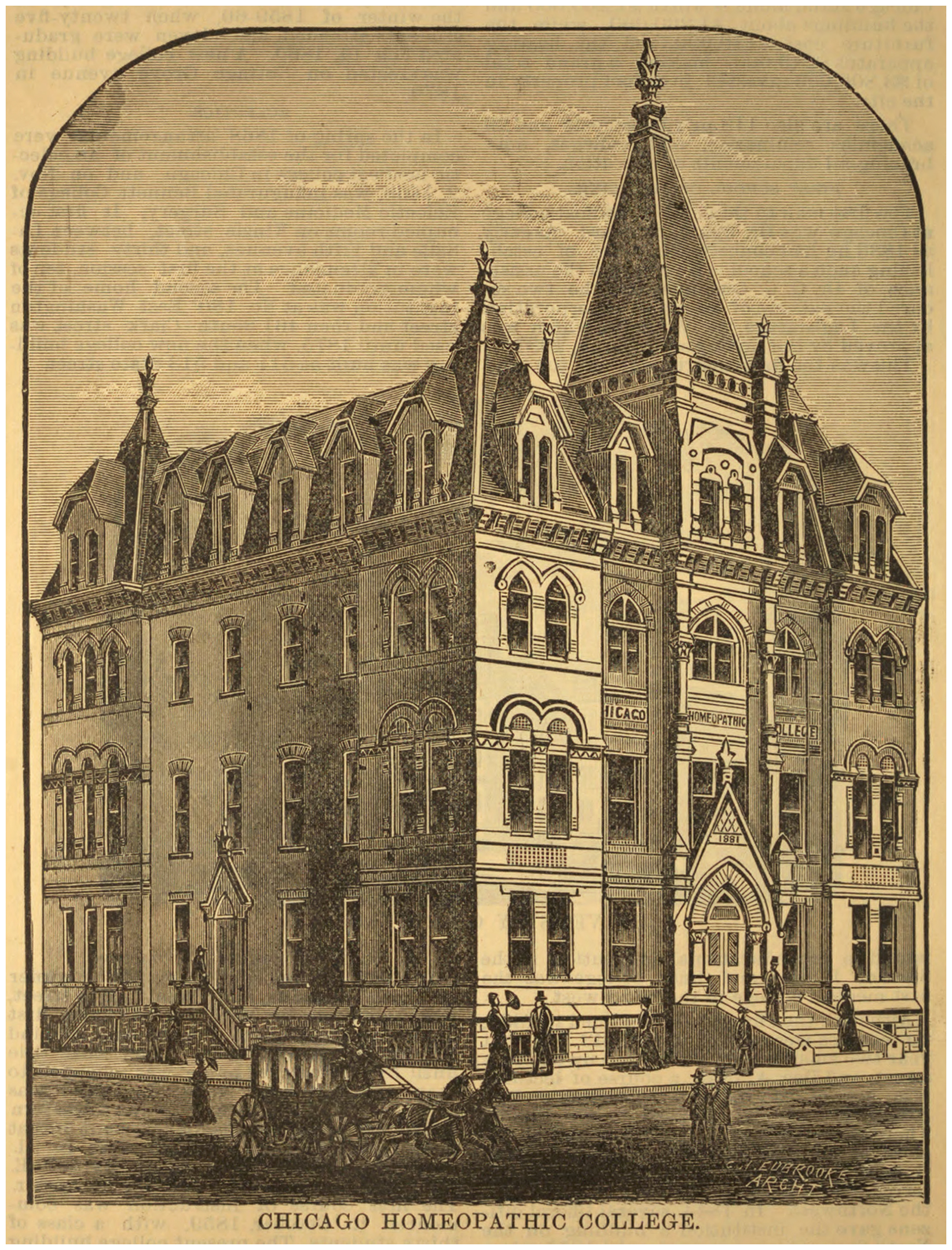
Chicago Homeopathic Medical College 1882. Photo from the University of Illinois Digital Library (cited 20 June 2025), https://digital.library.Illinois.edu/items/f20e87a0-1a05-0134-1d6d-0050569601ca-8.
Standards for medical education developed gradually in the 1880s. New requirements for college-level preparation and postgraduate medical education increased medical schools’ competition for students. 16 Some Chicago schools responded by offering evening classes, despite the opposition of several prominent physicians.16,17 However, students who could not afford to attend a full-time school, like Edward Miller, welcomed this change. Already in practice in 1893, he sought to expand his knowledge and skills, completing a postgraduate course at Harvey Medical College by 1898. In fact, most surgeons, regardless of race (including the Mayo Brothers), learned their specialty through part-time study as interns or physician assistants, plus taking a short postgraduate course. 18
Racism in medical education and Black self-help in the United States
Before the Civil War, “a handful of Northern medical schools” were admitting Blacks. 19 After the war, a movement emerged to establish medical schools for Blacks. They had little money and few resources, but White missionary associations and former abolitionists helped create some schools, including two of today's Historically Black Colleges. Savitt wrote case studies of six African-American medical schools established in that era. 19 All were in the South, except for Pennsylvania's Lincoln University Medical Department, and only Howard and Meharry have survived. Savitt argued that finances underlay the story of each school's success or failure. Independent Black-owned proprietary institutions lacked sufficient capital for long-term success, whereas those founded by northern White missionary groups endured with the blessing of medical schools organized by Whites and by philanthropic organizations. 20
Some scholars attribute the demise of these African-American schools to the impact of the Flexner report. 21 Commissioned by the Carnegie Foundation and the American Medical Association (AMA), Flexner surveyed all US and Canadian medical schools in 1908 and recommended closure of at least half, based on low quality and an assumption that physicians were overabundant. This assumption did not apply to the Black population, most of whom lived in the Jim Crow South. Flexner recommended closure of five of the seven Black medical schools and all three of the women's medical schools. He recommended that money used toward medical education of women would best be spent on coeducation, 22 but for the education of Black physicians, he did not suggest integration. Instead, he recommended that the remaining Black medical schools, Howard and Meharry, focus on teaching Black physicians “hygiene rather than surgery.” 22
Nationally, in 1890, only 0.9% of all physicians were Black, most practicing in the South. 20 Blacks wishing to practice medicine faced a segregated system that enrolled few African-American students and prevented those in practice from admitting patients to area hospitals. They were often barred from established medical societies, such as the AMA, 1 typically a prerequisite for gaining hospital privileges. 23
To address these challenges, a national Black self-help movement emerged. While the AMA had been established in 1847, 24 the National Medical Association (NMA) was founded in 1895 to address the healthcare needs of the Black population and increase the number of minority physicians. “Conceived in no spirit of racial exclusiveness, fostering no ethnic antagonisms, but born out of the exigency of the American environment…,” the NMA was open to all physicians but focused primarily on issues confronting the Black population. 1 By creating a national infrastructure, local chapters, and a medical journal, the NMA served as a counterpoint to the AMA. As an advocacy group, it was allied with organizations such as the National Association for the Advancement of Colored People. 1
Medicine and the Black self-help movement in Chicago
Although only 11 African Americans practiced medicine in Chicago in the 1890s, the city was a place of great opportunity for Blacks. It had jobs available, and Illinois had a history of progressive (although inconsistently enforced) legislation that protected the civil rights: Blacks had the right to vote, serve on juries, and receive equal treatment under the law.26,25 Nonetheless, the only Chicago hospital that admitted Black patients was Cook County Hospital, which employed no Black physicians until 1896. Blacks were excluded from segregated medical societies and journals and had limited opportunities for the information exchange and continuing education necessary for physicians to maintain currency in practice. 23
In this setting, Daniel Hale Williams was a force for change. He was a graduate of Chicago Medical College, had an exceptional reputation among White and Black Chicagoans, and founded Provident Hospital, the nation's first Black-controlled hospital, in 1891. 26 Provident was founded when Emma Reynolds, the college-educated sister of a local Black pastor, was denied admission to Chicago nursing schools. Reverend Reynolds teamed with Williams to start a nursing school for Black women. It expanded to include a 12-bed hospital within its first year to meet the clinical needs of the community and the educational needs of area medical schools. Later, it also supported the continuing medical education needs of practicing Black physicians.26,27
Williams himself faced significant racial constraints. He could perform only minor operations at a local infirmary and for employees of the Chicago Railroad Company because no local hospitals would grant him admitting privileges. 27 Williams envisioned Provident as an integrated institution for patient care and education that would equal any White hospital. It was initially funded by a biracial association of Black civic and community groups and the prominent White businessmen, Phillip Armour and George Pullman, who recognized the importance of healthcare for their Black employees. 27 Many in the Black community viewed Provident with racial pride and enthusiastically gave monetary support.
In the 1890s, Chicago's growing Black community had 200 Black-owned businesses and three newspapers. 26 Williams worked tirelessly to solicit their support; community networks funded 90% of Provident's endowment by the year 1912. The hospital initially served a biracial population and house staff: patients were ∼18% White in its first year. 27 This changed, however, as Chicago became increasingly segregated after the influx of Black migrants from the South. While the Black community continued to financially support Provident, the need to provide increasingly complex care for an overwhelmingly indigent population led to continuing financial challenges (Annual Bulletins of the Provident Hospital and Training School and Abakanowicz Research Center at the Chicago History Museum). During the Depression, Provident affiliated with the University of Chicago, which enabled it to upgrade its facilities. This connection was troubled, however, partly because the Black community perceived that Whites had usurped control of their institution, and some felt that the arrangement perpetuated segregation. Hence, the affiliation was severed in 1944, 28 and Provident officially closed as a private entity in 1987. 29 In 1990, it was acquired by Cook County and now operates as Provident Hospital of Cook County.27,29
Edward Miller contributed to the growth of Provident and learned from the strategies that facilitated its early success. He was an attending physician there and joined the teaching staff of Northwestern Medical School in 1896. 30 He helped to train interns who moved into leadership positions at other institutions. His trainee, Dr Austin Curtis, a mentee of Daniel Hale Williams, became the first Black staff physician at Cook County Hospital. 31
The politics of Cook County has been highly competitive since the late 19th century. In 1896, Theodore Jones, one of the first Black County commissioners, made good on a campaign promise by asking Chicago's Black physicians to recommend which physician should be appointed to serve at Cook County Hospital.
31
Miller was one of Chicago's 15 African-American physicians who met to suggest that Dr Curtis effectively represent the race as the hospital's first Black physician. When Curtis later moved to Washington DC to succeed Daniel Hale Williams as surgeon-in-chief at Freedmen's Hospital, Miller offered this recommendation: … Dr. Curtis has successfully performed more delicate operations than any colored surgeon in this city. And as surgeon-in-chief of the Freedman's Hospital he will not only do credit to himself but to the entire race. Dr. Curtis is one of the progressive men of this age and therefore is the sort of man we want in the foreground of every scene.
31
Building success in the army, the community and in business
Edward Miller's military service at a pivotal time
At age 40, Miller volunteered to serve in the Spanish American War as part of the 8th Illinois Volunteer Regiment, the only all African-American infantry regiment led by African Americans (Figure 2).
32
The decision to appoint Blacks as officers was controversial; it was considered a test case for African-American capabilities.
33
When large numbers of the all-White First Illinois Regiment succumbed to yellow fever, the opportunity arose to deploy Black soldiers, who some believed possessed natural immunity to tropical diseases.
34
Responding to ongoing pressure from Chicago's growing Black population, who numbered 60,000 and had become a recognized voting block,
32
Governor Tanner decided to appoint Black officers to the regiment and prevailed upon President McKinley to deploy them in Cuba: …believing that this race should have the opportunity to show the country at large whether or not its members possessed the ability to govern themselves, and in a spirit of “fair play” determined, and carried into effect [his] idea that Negroes could, and in this case should, be commanded by Negroes.
35
…most of them raw recruits, all of them ignorant of the conditions of life in a tropical country, but whose hearts thrilled with patriotic pride in their country, their country's flag and their own unique organization, [and] were precipitated into a struggle with an enemy far more deadly than Spanish shot and shell [i.e., tropical diseases].
36
…characterized by a paroxysm of coma, a temperature of 105° F, full, soft, rapid pulse and stertorous breathing; the paroxysm lasted about 188 hours. Quinine hyperdermically and per rectum was exhibited and the case made a good recovery in eight days. Among other cerebral manifestations of the fever, acute mania developed in two cases, while delusions and hallucinations frequently accompanied the paroxysms … [Another] … attack was of an exceedingly aggravated character and terminated fatally in fourteen days. … The fever was remittent … running as high as 106 during an exacerbation. The urine was decreased in quantity, was of a dark brown color, which, after standing a while, showed a greenish tinge and deposited a thick grumous sediment. Diarrhea was present and vomiting of a dark greenish substance….
36
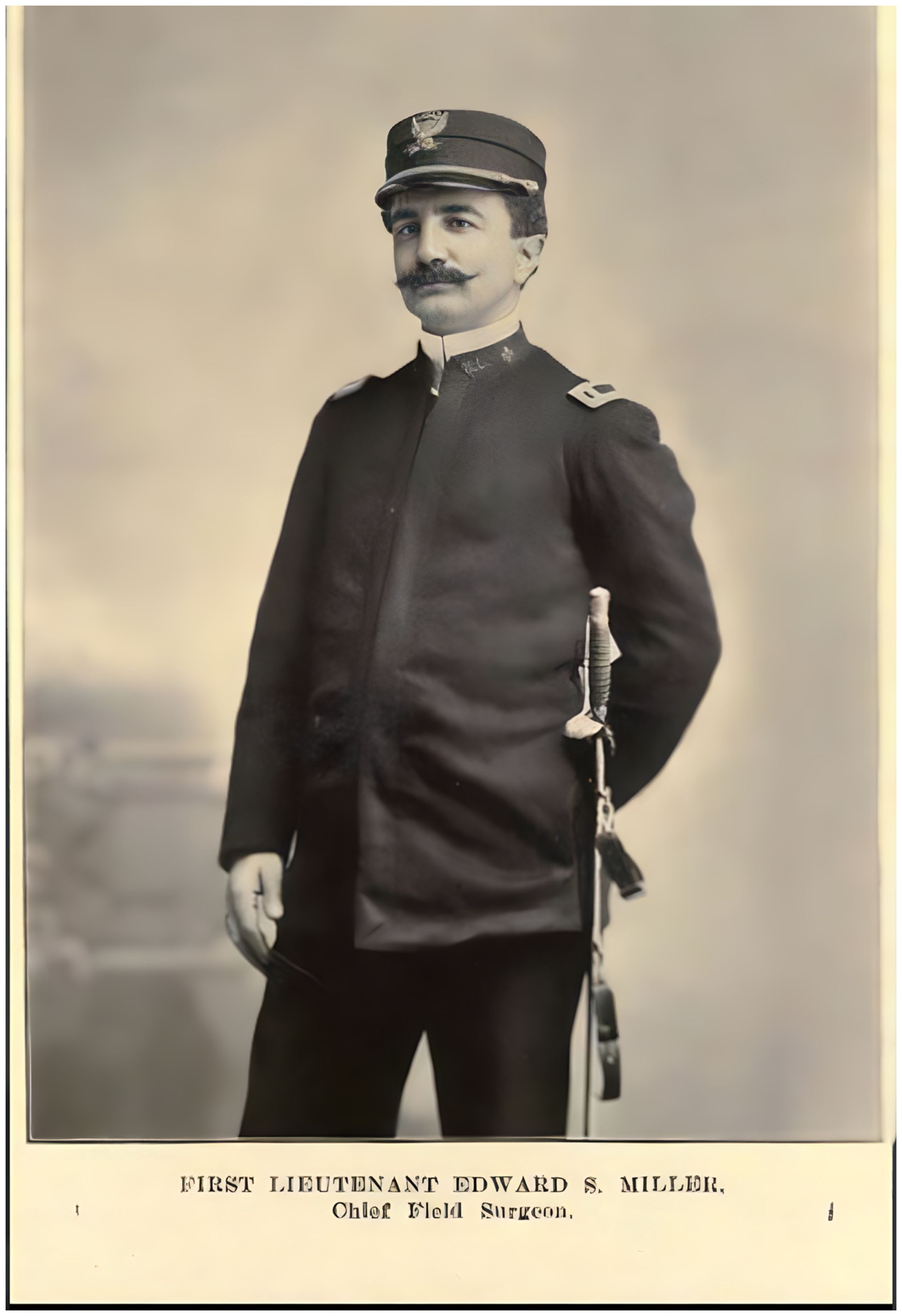
First Lieutenant Miller. Miller oversaw a field hospital for 10 companies in the Spanish-American War. Photo from The Eighth Illinois. 38
By the war's end, Miller “was held in esteem by all the officers of his regiment and every private spoke good words of him.”
38
Miller ended his reflections on the war by saying: April 3, 1899, the 8th Illinois U.S.V., the first of its kind, passed into the misty shadows of the past but its memory will long live in the hearts of those of us who served in it. … [Our] story will be a monument to the liberality and moral courage of Governor John R. Tanner.
36
After the war, Miller continued to serve as assistant surgeon with the 8th Illinois, which became part of the state national guard and remained a source of pride for Blacks 3 (Figure 3). Membership provided training opportunities and facilitated political and social connections. Through advocacy and political pressures, the 8th Illinois had its own armory built in 1915 in the heart of the Black community. It provided a community meeting site and was a visible symbol of the power and influence of Blacks in Chicago. “The armory represented many things to African Americans in Chicago, not the least of which was state commitment to their formal equality and full citizenship.” 39

Eighth Illinois regiment staff 1903. Miller (far left, top row) is shown here at Camp Lincoln in
Despite favorable reviews from federal inspectors, however, the regiment was not called into service for domestic disturbances. “[The] regiment is always spoken of as a political regiment in that it is believed that it would be criminal to order it out for local duty, … as it would be almost certain to precipitate a race war.” 40
Serving the Black community
After the war, Miller's medical career and social and financial influence blossomed. His office was in the heart of the growing commercial district of Chicago's Bronzeville neighborhood. His reputation in the medical community, secured by his long-standing position at Provident Hospital, grew with his wartime service and his membership in local medical and civic organizations. He acquired property and helped to found three businesses in Bronzeville,3,4,41 using the community networking process that had served Chicago's Black community so well in establishing Provident Hospital. Miller understood the value of community input in establishing and maintaining new businesses.
Mount Glenwood Cemetery
Miller was one of three founders of the Parkwood Cemetery Associates in 1906.
41
African Americans were denied access to a burial plot unless it was unmarked or registered under an assumed name. Miller wished to create a place without “discrimination on account of race or color on the price of graves….”
42
A Mr Patton spoke with deep feeling about “The unrest, and heavy heartedness of a washerwoman telling how she had to pay $50.00 for a grave, and white people $25.00….”
42
After slowly building investors, Parkwood joined forces with the African-American Mount Glenwood Cemetery Association. Glenwood advertisements tapped into the common experience of discrimination, such as this notice in the Broad Ax newspaper: Colored Men and Women of Chicago, do not let any undertakers “Jim Crow” you into a “Jim Crow” Cemetery. Mount Glenwood has no “Jim Crow” Section. It has One Section and One Entrance for all. Undertakers’ profits in Mount Glenwood go to the people.
43
Douglass National Bank
Miller's most ambitious business undertaking was the Douglass National Bank, founded in 1922 and named after Frederick Douglass (Figure 4). 45 In an era of expanding Black entrepreneurship and home ownership, acquiring capital was a common need. White-owned banks regularly denied loans to African Americans or charged exorbitant rates. 4 Two Chicago groups created alternatives: the Binga State Bank, founded by Black real estate mogul Jesse Binga in 1919, 46 and the Douglass National Bank in 1922. 45 Their combined assets represented over one third of all Black-owned bank assets in the country before the panic of 1929. 47
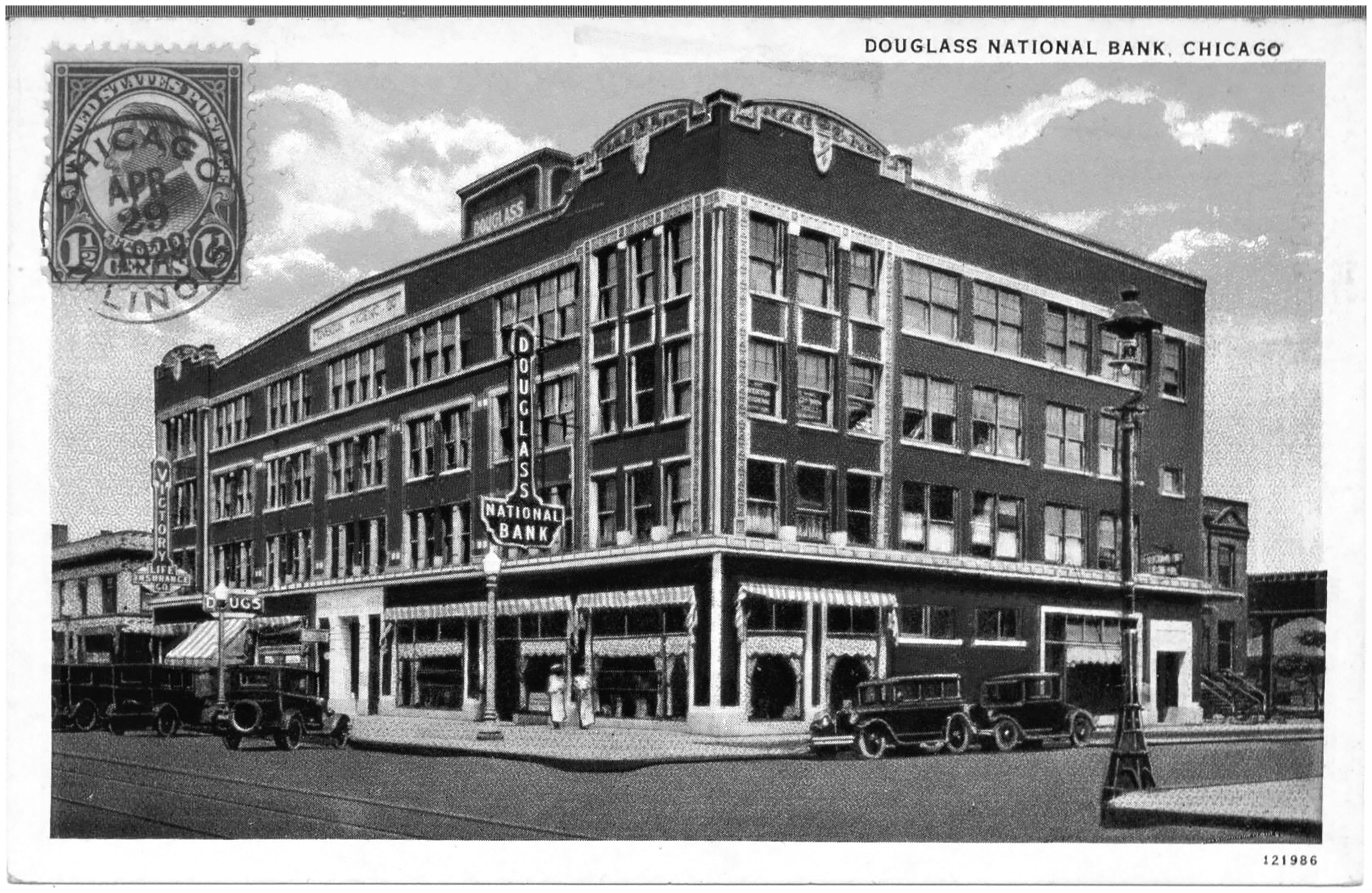
Douglass National Bank in Chicago, 1929. Photo from a private collection.
The Douglass Bank was generally thought to be the brainchild of Anthony Overton, a well-connected Black entrepreneur with a reputation for social consciousness. 4 The board of directors was a small group of initial investors that included Miller and other prominent Black businessmen, attorneys, clergy, and politicians, none of whom had banking experience. 4 One founder, PW Chavers, managed to get Douglass a federal charter, giving it the stature to attract investors beyond the Black community. The Chavers model required a grassroots effort to engage a large number of small investors, employing the community networking techniques used to build Mount Glenwood Cemetery. 4 Meetings were held in Black churches and the 8th Illinois Armory, and the bank opening was greeted by a parade of 5000 stockholders through Bronzeville. 48 Prominent speakers championed the importance of financial independence, and the movement to “trade with your own” helped fuel the growth of the bank. 49
In 1922, the board of directors sought to accelerate the capitalization by attracting larger investors, and they appointed Overton as president. He owned a newspaper, a manufacturing business, and multiple real estate holdings, and his influence and connections helped the bank gain national visibility. 4 Black newspapers in other cities regularly published articles about the progress of the bank; advertisements and meetings in other cities touted the ability to bank by mail.45,50
By 1926, there were 45,000 depositors from 29 states. 51 However, with the onset of the Great Depression in 1929, many of these loans defaulted. The bank's assets were a complicated mix of stock in other cash-strapped businesses and the real estate holdings of its officers, and these problems eventually led to the bank's demise. As a national bank, the Douglass Bank was able to secure a small federal loan, which helped for a time. 4 Miller was one officer who lost everything except his home, which he maintained only by deeding the property to a family member and taking in boarders. When the bank finally closed in 1932 and all of the assets were accounted for, depositors received almost all of their original savings. 52
The Great Depression
The Depression was especially hard on Black-owned businesses, like the Douglass Bank. Loss of real estate value and soaring unemployment proved disastrous for businesses, and the practices of Black physicians were no exception. 52 Miller often accepted favors or home-grown produce as remuneration for medical care. Like many Black physicians, he could no longer afford an office in Bronzeville, and he was forced to use his home for his practice, as well as a boarding house. Provident Hospital survived only with the support of the University of Chicago (Leonidas Berry Papers, 1891–1995; Vivian Harsh Collection of the Chicago Public Library; interview with Miller's daughter, Vivian Miller Lewis).
Miller's health declined significantly during the Depression and he was forced to give up medicine entirely by 1938 at the age of 80. Veteran’s benefits and rental income from boarders provided his only income (Miller's personal correspondence with US Veterans Administration). He ultimately required full-time care from a Veterans Administration nursing home until his death at 84 years old.
Conclusion
Edward S. Miller was born into slavery in 1858. After navigating the racist educational system in Kentucky, he moved north to seek better opportunities. In Chicago, he obtained medical training, built a successful practice in the Black community, and participated in the growth of Provident Hospital. He expanded his networks when serving in the Spanish-American War as a field surgeon for a unique Black volunteer regiment. Thereafter, Miller prospered as an entrepreneur and civic leader, using the power of community networks to help found the first Black cemetery and a large bank in Chicago. Both organizations employed and supported the Black community.
Edward Miller was a respected civic leader and physician whose story illustrates the complexity and challenges posed by the social and medical system in the north at the turn of the 20th century. His life also demonstrates the resourcefulness a Black leader needed to succeed in a segregated society.
Footnotes
Acknowledgments
The authors wish to acknowledge the contributions of Professor Martha S. Jones of Johns Hopkins University and Stephanie D. Smith, Ph.D., Research Assistant in the Department of History at University of Illinois at Chicago for their help in obtaining primary resource material and for their invaluable critical advice.
Ethical considerations
Not applicable.
Author contributions
Vivian Lewis conceived of this work along with Paul Miller. All authors participated in the acquisition and analysis of background material, drafting and critical review of the work for intellectual content, and final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of the work are appropriately investigated and resolved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.