
Abstract
Objectives
To explore barriers to cervical and colorectal cancer screening and attitudes to promotion of self-sampling kits upon attendance for breast cancer screening.
Methods
Interview study with women who had not responded to one or more invitations to cervical or colorectal cancer screening. A semi-structured interview guide was used and interviews were audio recorded and transcribed verbatim. Concepts from Temporal Motivation Theory were used to structure and analyse the data.
Results
Twenty-two women were interviewed. Screening was highly valued but the women perceived screening for cervical cancer and colorectal cancer as more troublesome to participate in, compared with participation in breast cancer screening. The lack of a pre-booked appointment or a suggested deadline attenuated the perceived value of cervical and colorectal cancer screening and this further increased procrastination. Promotion of self-sampling kits for cervical and colorectal cancer screening upon attendance for breast cancer screening was considered a feasible way to increase salience of both types of screening.
Conclusion
A high number of micro steps and absence of a deadline in cervical and colorectal cancer screening diverted attention away from screening participation in cervical and colorectal cancer screening. The main facilitator could be reduction of micro actions, proposing a suggested deadline, and promotion of self-sampling kits when attending breast cancer screening to increase salience and a renewed attention to all three screening programmes.
Introduction
Population-based screening programmes for breast cancer (BC), cervical cancer (CC) and colorectal cancer (CRC) have the potential to reduce morbidity and disease-specific mortality significantly, but non-participation reduces the effectiveness of the programmes.1–3 Across countries, participation in screening for CRC and CC is usually lagging behind screening for BC. 4 Fear, embarrassment, discomfort, and logistical challenges are generic reasons for non-participation in all three programmes, but fear of pain and embarrassment are more commonly found in CC and BC screening, while disgust and lack of awareness are common barriers to CRC, especially CRC using fecal occult blood test (FOBT).5–10 An Australian study comparing participation in BC and CRC showed that 16.2% of women participated in both screening programmes. 11 Similarly, a French study comparing screening for BC, CRC, and CC showed that only 11.5% of women participated in all three programmes (‘joint participation’). 12 An English study found a joint participation rate of 35%, 13 while a study from Scotland showed a joint participation rate of 52.1%. 4 To support awareness about all cancer screening programs and increase the joint participation rate among eligible women, it has been suggested that attendance for one kind of screening could be used as leverage for promotion of other screening offers.14–16 In particular, BC screening attendance offers a unique opportunity to provide self-sampling kits to eliminate embarrassment and pain, which is particularly relevant in CC screening, and to increase awareness, which may be particularly relevant in CRC screening as suggested above.
In order to target an intervention to increase joint participation, the reasons for non-participation in CC and CRC screening among BC screening participants need to be understood. The aim of this study was to identify reasons for non-participation particular to CC and CRC among women attending screening for BC, and to explore attitudes to promotion of self-sampling kits for CC and CRC screening when attending BC screening.
Methods
Setting
The study took place in Randers, a city with approximately 63,000 inhabitants in the Central Denmark Region, which is the second largest region in Denmark with 1.3 million residents, covering 23% of the total Danish population. Women aged 50–69 years are invited for BC screening every second year by secure email including a pre-booked appointment for a screening mammography. Women are invited by secure email to book an appointment with their general practitioner for CC screening every third (23–49 years) or fifth year (50–64 years). Men and women aged 50–74 are invited by postal mail to participate in CRC screening using a fecal immunochemical test (FIT) self-sampling kit for detection of occult blood in the stool. All screening and follow-up are free of charge. Screening for BC has an 84% participation rate, 17 the CC screening programme has a 61% participation rate, 18 and screening for CRC has a 60% participation rate. 19
Design, participants and recruitment
This was an interview study with women defined as non-participants if they had not responded to CC and/or CRC screening invitations at least once within recent previous screening rounds. The women were recruited consecutively when they attended BC screening in November 2020. A secretary informed the woman about the interview study and asked permission to check her screening status in an in-house patient record system with data about invitations and participation. If the women had not participated regularly according to the in-house database, they were eligible for inclusion and invited to an interview in a meeting room close to the screening unit right after their appointment for BC screening or within a week. Due to the COVID-19 situation, 20 women were also provided the option to be interviewed by telephone or online. The level of information power was continuously assessed during the research process to determine the sample size. 21 A high level of information power requires a narrow aim, dense specificity of the sample, application of theory, high quality of dialogue in the interviews, and an analysis strategy that is appropriate to meet the aim. In our study, the aim was to explore barriers and attitudes of a specific population, using an appropriate analysis strategy involving an established theory. The quality of the dialogue of the interviews was deemed high as the interviewer was experienced and able to challenge the views of the participants in an empathetic way without causing resentment in the situation. Thus the sample size was determined as appropriate when information power was high.
Data collection
Inspired by the components of the Health Belief Model (perceived severity, perceived susceptibility, perceived benefits, perceived barriers, cues to action, and self-efficacy), a semi-structured interview guide was developed (Table 1).22,23 All participants were asked about attitudes to cancer screening and reasons for participation and non-participation. They were asked to imagine if any structural changes could make them want to choose to participate on a regular basis, and subsequently presented with the possibility to receive a self-sampling kit for human papillomavirus (HPV) testing for CC screening and/or delivery of a self-sampling kit for collection of stool for CRC screening after attending BC screening.
Semi-structured interview guide.

BC: breast cancer; CC: cervical cancer; HPV: human papillomavirus; CRC: colorectal cancer; FIT: fecal immunochemical test.
The participants filled out a small questionnaire about socio-demographic data before the interview. The interviews were undertaken by the first author as the interviewer was experienced. The interviews were audio-recorded and transcribed verbatim by a secretary, supervised by the first author. The data were managed and documented using a text editor featuring tracked changes and comments to support a continuous dialogue between the authors.
Data analysis
The approach was inspired by the interpretive tradition of ethnography, adopting a funnel-structured research cycle process to undertake an inductive thematic analysis.24,25 The interviews were read carefully to perform an open coding of content and meaning, and to inform discussions about patterns and themes among all authors.26,27 Differences and similarities across the transcripts were discussed to challenge analytical insights and narrow down the focus of the themes. Theories about experiences, barriers, intentions, and attitudes from social and cognitive psychology were compared with the themes to discuss the interpretation.22,28–30 To achieve trustworthiness, quotes reflecting strong patterns as well as discrepant quotes were selected to illustrate the findings below. 31
Ethics
In accordance with the EU's General Data Protection Regulation article 30, the project was listed in a register for research projects in the Central Denmark Region (journal number 1-16-02-575-20). According to Danish legislation, the study did not require ethical approval. 32 Oral and written consent was obtained on the day of recruitment. The women were informed that their interview data would be pseudonymised before publishing and they were allowed to withdraw the data before publishing.
Results
In the recruitment period, 162 women were approached, of whom 89 declined to have their screening status checked (mean age 59). Seventy-three women accepted to have it checked (mean age 58) and among these 22 were non-participants in screening for CC and/or CRC according to our definition and thus eligible for interview (mean age 57) (Table 2).
Participant characteristics.
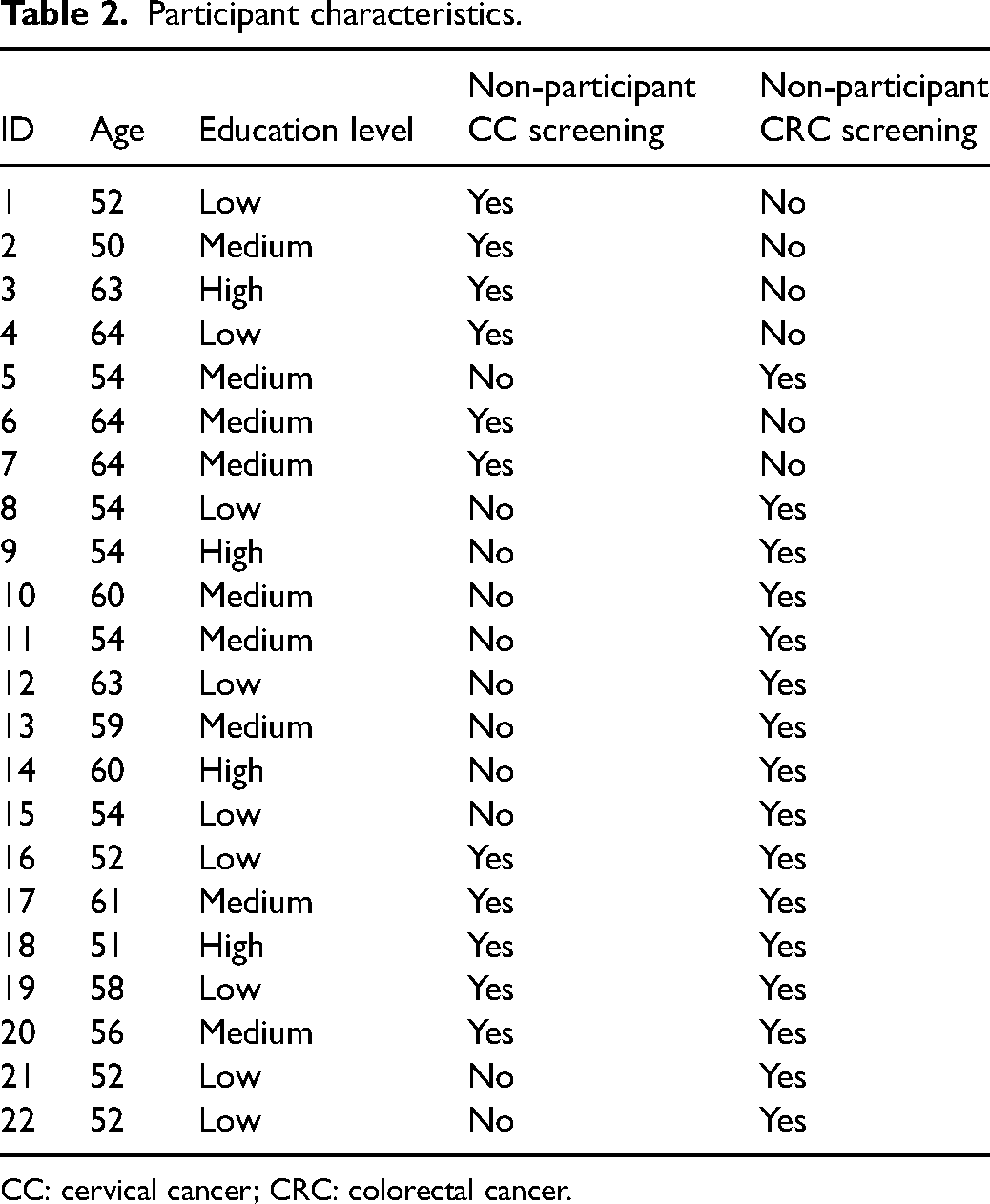
CC: cervical cancer; CRC: colorectal cancer.
Barriers to participation in CC screening
Out of 22 study participants, 11 were non-participants in screening for CC. Feelings of exposure and transgression during the gynaecological examination made CC screening only episodically doable for some: Interview 22: Getting my breast scanned is okay but the other thing… it is really unpleasant. It is for me. You expose yourself when you undergo that examination and it is so uncomfortable. It is so transgressive to get in there and it is cold and brutal in some way. It takes 30 seconds and then it is over and done with, but I feel like my pelvis remains in there. I think it is so dreadful.
Being cued or reminded by their general practitioner (in addition to the invitation letter) to get a gynaecological examination for CC screening was a motivating factor for women who did not express excessive discomfort related to the gynaecological examination. They explained that the invitation by secure email was easily forgotten but the general practitioner reminded them when they showed up with other health issues: Interview 19: I haven't participated on a regular basis. When I visit my general practitioner he says ‘oops we forgot to do it last time you were here’. Then I do it. I simply forgot it, I think.
Interview 17: I haven't participated regularly but I did it one year ago, and why did I do it…? Maybe because my general practitioner encouraged me to do it. I think that's why.
In many cases the additional task of booking an appointment was a barrier to participation because the invitation became inconspicuous after a short while: Interview 1: When I have to book an appointment myself and things like that, I just don't get it done. For my part, I keep putting it off and then time passes and I don't go.
Interview 9: I think it‘s the daily grind, house and dog and work and the humdrum of everyday life. You don‘t take the time to deal with it because you have to do it yourself [book an appointment]. You have to take the time to do it.
Barriers to regular participation in screening for CRC
Out of the 22 study participants, 16 were non-participants in CRC screening.
Some women found BC screening less troublesome than screening for CRC because BC screening requires less mental energy, even though it requires taking time off to attend BC screening at a predefined screening unit: Interview 18: In breast cancer screening you get a pre-booked appointment and you know you can show up and get it done. It‘s a no-brainer. You don‘t have time to get worried, you just go in and get it over with.
Interview 11: It‘s just because it (FIT) is a bit more troublesome than the other thing [breast cancer screening].
A few expressed a reluctance to taking the FIT sample because they were afraid of doing it wrong. Confusion about the instruction was common, and information overload, especially about the pros and cons of participation, was mentioned as a barrier to getting it done: Interview 18: You get a load of material. You open it and think ‘My God, how am I supposed to…?’ You read about the risks before you actually see the instruction. If you read how easy it is at first, and afterwards we could talk about the risks, then I’d probably get it done.
Interview 21: I think I just need to overcome myself and do it. It‘s the procedure of taking the sample… I think it‘s because you have to do it right. That‘s what I’m thinking about every time I take a look at it. How do I do it? Then I haven‘t come any further.
The most common explanation for non-participation in both CC and CRC screening was a sense of ‘non-urgency’. The women simply forgot about it, although they had the intention to participate: Interview 21: I’ve opened it (FIT self-sampling kit) and now it‘s placed on the shelf at home and I have been thinking ‘I’m going to send it soon’. I know for a fact that I haven‘t done that. I just put it on the shelf and it‘s just there and it‘s actually a bit strange that I haven‘t done it yet. I believe it‘s just easier to leave it there on the shelf.
Invitations to CRC screening with FIT do not include an explicit deadline except a pre-stamped expiry date on the kit and thus, in the daily humdrum, the invitation became inconspicuous and increased the tendency to procrastination.
The FIT self-sampling kit also required too many steps or micro actions that need planning and a large amount of mental energy: Interview 17: It‘s just a bit more troublesome to collect faeces, I think. It comes in a package and I’ve peeked into it. Well, I don‘t know, it‘s just a bit more troublesome. I also think that you have to send it in rather quickly, so you have to plan in advance when you do it, consider how to submit it et cetera. So it‘s more pervasive.
Interview 16: I haven‘t opened it yet. Last time I got an invitation, I didn‘t open it. It‘s all about how to get it done when there is no one there to tell you to do it right now. You are busy in the morning and first you didn‘t get round to doing it and then you didn‘t do it and after that you didn‘t do it either. I need someone to tell me to do it and someone to tell me to do it right now. That‘s me. When someone tells me to show up, I show up.
Attitudes to promotion of CC and CRC screening when attending BC screening
During the interviews, the women were asked to imagine that a secretary or screening assistant would ask permission to check their status on screening for CC and CRC the next time they showed up for BC screening, and possibly hand out self-sampling kits (FIT and HPV) if screening was due. When the women were asked whether they would prefer taking the HPV sample immediately after the BC screening or at home in this scenario, some women said they liked the idea of getting it done in a suitable room at the screening unit: Interview 17: That‘s clever. I think it‘s clever. It would suit me. I believe you could do it in a restroom in the unit? I could do that quite easily. I’d have no problems doing that.
Interview 18: I would think it was fine. I would think it was fine to get it done right away and if you get good enough counselling to do it yourself that would be fine. Then I could ask [a screening assistant] if I had any questions about it. I think it would be fine. Then the screening examinations are done and that‘s it.
Interview 15: I think it would be fine to get everything done at once so you have to show up only one time instead of booking an appointment at the doctor and waiting in a queue. You spend time doing that. It would be better if you could do it in a more rational manner like that.
A few women rejected the idea of taking an HPV sample with a self-sampling kit and preferred to go to their general practitioner to get a standard CC screening:
Interview 11: I think I would prefer that a professional takes the sample. I mean, if you don't do it properly yourself…. I would think to myself ‘have I done it correctly?’
Interview 9: I would worry that the (HPV) sample was not taken properly. Would I be able to do it myself? I don't know if I could collect enough. When I get a smear it hurts a bit sometimes. I think I would worry that I didn't get enough out for someone to check it. I’d be worried that I was not able to do it properly myself.
Many women said that being reminded about screening for CRC and possibly receiving a FIT self-sampling kit when showing up for screening for BC would be feasible and meaningful, because cancer is the common denominator: Interview 8: I think it‘s okay because it is part of the same thing. I think of my body as a whole so it makes sense that I receive it there [when showing up for breast cancer screening]. If they wanted to perform an eye test on me, I would find it strange, but it‘s screening for cancer after all, no matter where the cancer is.
Interview 16: I think that would be really good because I could kill two birds with one stone.
Discussion
Overall, barriers to participation in CC screening included anticipated discomfort and inconspicuousness of the invitation, and for CRC screening, barriers to regular participation included fear of failure and too many micro actions. Women delayed the task they had intended to perform, until someone would cue them and make the CC and CRC screening salient. According to the women, the cuing of CC and CRC screening when attending BC screening and delivery of an HPV or FIT self-sampling kit might bridge the gap between intention and action.
Strengths and limitations
The study participants had a wide range of education levels and age which is a strength to the study. The interviews took place immediately after the BC screening, either as interviews on location or as online interviews. During the COVID-19 pandemic, online meetings have been more common and the study participants were familiar with the online format.
The study participants were informed that the interviewer (first author) comes from a research department involved in cancer screening. The interviewer was careful to be explicit about her role as a researcher who is not judgemental about participation or non-participation. Although courtesy bias cannot be ruled out, the study participants were keen to explain why they sometimes did not respond to the invitation. A limitation to the interpretation of the findings is the fact that we interviewed the women about their intentions to be screened in case scenarios where a self-sampling kit was made available. It is well-established, as also shown in the quotes, that intention does not always lead to action, and research about actual participation using the suggested interventions should be undertaken.
Comparison with theory and existing literature
Procrastination is a psychological barrier which has been defined as ‘the voluntary delay of an intention despite the expectation of being worse off for the delay’; in daily terms, ‘not getting round to doing it’.33,34 As described in the Methods section, the components of the Health Belief Model: perceived severity, perceived susceptibility, perceived benefits, perceived barriers, cues to action, and self-efficacy, inspired the interview guide and thus guided the thematic analysis. However, the Health Belief Model and other related theories did not help in understanding the procrastination aspect which was prominent in the data.22,28–30
Instead, the insights and concepts from the Temporal Motivation Theory were helpful to unfold the significant yet underexplored challenge of time and procrastination. 35 This theory explains how people make individual decisions with consequences that play out over time (intertemporal decisions), which involves trade-offs between sooner and later outcomes. According to the Temporal Motivation Theory, any person will always prioritise activities that promise the highest utility, and the subjective evaluation of utility may change over time. Decision-making about any type of screening for a disease could be considered an intertemporal decision because it requires choosing between an activity in the present with an increased chance of an attractive outcome in the future, or a ‘non-activity’ in the present with increased risk of an adverse consequence in the future. The theory indicates that motivation to complete a task may be understood by four features. 35 The first is the value of the task and satisfaction associated with outcomes of completion of the task. In our study, the women attached high value to cancer screening in general but found more obstacles associated with CC and CRC than with BC. The second is expectancy which includes self-efficacy and task difficulty. In our study many women expected and had experienced that both CRC screening and screening for CC were ‘troublesome’ with too many micro actions and discomfort. The third features in the theory is delay (time) which implies that the closer temporally an event becomes, the greater its influence on value and expectancy will be. The fourth feature is impulsiveness (or ‘sensitivity to delay’) which implies a distraction away from the task, particularly if the task is inconspicuous or ‘out of sight’. For instance, when a task is far in the future or has no suggested deadline, people may discount its value and postpone the task, sometimes indefinitely. We found both time and sensitivity to delay to be prominent in the women's accounts of non-participation.
A Danish register study showed that one in four cervical cytologies were collected opportunistically, defined as a sample taken more than nine months after latest invitation. 36 This supports the finding in our study suggesting that convenience and cuing by a general practitioner may be important facilitators for screening. A Swedish qualitative study showed that women who actively declined participation in CC screening attached low value and low expectancy to CC screening. 37 They lacked confidence in the benefits of screening and had previous negative health-care experiences. This was not found in our study. A qualitative Scottish study examined non-participation in FOBT-based CRC screening among women who participated in screening for BC and CC. 14 A FOBT-based self-sampling procedure requires more micro-actions compared with a FIT-based self-sampling procedure (three samples compared to one), 38 and the study showed a low perceived value of CRC screening, a low expectancy due to disgust, and confusion about how to complete the FOBT self-sampling procedure correctly. In our study, disgust was not mentioned as a reason to delay or avoid CRC screening, but some of the participants had low expectancy regarding self-efficacy to perform the sampling properly. A US randomised controlled trial showed that specifying a deadline significantly increased FIT-based CRC screening participation. 39 The findings in our study showed that participation in screening for CC and especially CRC was sometimes delayed because there was no deadline to it, which made it seem less important. This is also supported by two studies showing evidence of a positive effect of a scheduled appointment (or a deadline) and emphasised the importance of reducing micro actions.40,41 These studies suggested that people invited to CRC could be encouraged to leave the material near or in the bathroom within view as a cue.
It has been suggested that attending BC screening could be ‘a teachable moment’ where participants are more easily motivated to also receive advice about other screening programmes.16,42 The findings in our study, however, do not explicitly support the underlying notion of advice-driven motivation. Our participants already attached high value to screening, but rather asked for a cue to make the offer salient again, e.g. if a self-sampling kit for CC or CRC screening was delivered when attending BC screening.
The question remains whether the passive non-participation can be reduced by using the concepts from Temporal Motivation Theory, i.e. by reducing delay and distraction away from the task, thereby also closing the intention-action gap for procrastinators. 34 Based on concepts from the theory, a ‘MADS’ model featuring attention to Micro Actions (MA), suggested Deadline (D), and Salience (S), could be proposed to inform future interventions as important cues and bridge the gap between intention and action among women who wish to participate in screening according to official guidelines but fail to do so due to procrastination.
Conclusion
The study showed that non-participation was often a passive decision. Participation in screening for CC and CRC was delayed because there was no deadline to it, and it quickly became inconspicuous. Non-participation increased with a higher number of micro actions that require conscious attention and mental effort, which was more prominent in CC screening and particularly CRC screening compared with BC screening. Promotion of CC and CRC screening when attending BC screening was perceived as meaningful by the women in our study because it would make the screening offers salient again. Interventions to reduce non-participation should aim to critically revise the nature and number of micro actions, provide a suggested deadline, and increase salience. Understanding non-participation in the light of value, expectancy, delay, and impulsiveness may be a way to reduce the intention-action gap among women who attach value to screening for CC and CRC but procrastinate. Understanding the root causes of procrastination may hold the key to support the link between motivation and action in regular screening participation. Further research is needed to test the effect of a MADS model.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.