
Abstract
Objective
Attendance as well as re-attendance is important for an effective screening program for breast cancer. We aimed to evaluate re-attendance among women with a false positive versus negative screening result in BreastScreen Norway.
Methods
The study sample included 3,990,388 screening examinations performed between 1996 and 2021 among women with an invitation to the subsequent screening examination available, that is, women eligible for re-attendance in the period 1998–2023. Mixed logistic regression was used to analyze the association between screening results, including negative versus any false positive, and negative versus false positive with or without a needle biopsy, and attendance in the subsequent screening round. We adjusted for screening history and age.
Results
Crude attendance rates in the subsequent screening round were 90.8% for those with a negative result and 88.3% for those with a false positive result. The adjusted odds ratio (OR) for re-attendance after a false positive result was 0.91 (95% CI: 0.87–0.93) using a negative screening result as the reference. Also using negative screening result as the reference, adjusted OR for re-attendance among those with a false positive screening result without a needle biopsy was 0.93 (95% CI: 0.91–0.96) while it was 0.85 (95% CI: 0.82–0.87) for those with a false positive result including a biopsy.
Conclusions
Women invited to BreastScreen Norway re-attended screening less often after a false positive compared to a negative result. The benefits of regular attendance should be communicated to women targeted for breast cancer screening.
Introduction
In 2022, breast cancer was the most common cancer and the most common cause of cancer death among women worldwide. 1 Organized mammographic screening is shown to reduce mortality from the disease and is thus recommended by international health authorities.2,3 The success of a screening program depends on a consistently high uptake in the eligible population and regularity of screening attendance is important for early detection of breast cancer.4,5
Factors associated with attendance are reported to be immigration status,6,7 invitation methods including reminders,8–10 costs of participation, income, access to health insurance, marital status and employment status.7,11,12 Information about cancer screening influences attendance less than the aforementioned factors.9,13
In mammographic screening, a false positive screening result is defined as a recall for further assessment due to abnormal findings on the screening mammogram, but ultimately no breast cancer is detected. Screening result is also reported to be associated with attendance, and women with a false positive screening result are reported to have lower re-attendance compared to those with a negative screening outcome.14–16 A recent meta-analysis based on six studies showed 23% lower odds for re-attendance for women with a false positive compared to a negative result. 7 Studies conducted more than a decade ago showed comparable re-attendance rates for the two groups.17–19 This may be due to small study samples and/or short follow-up periods, as well as regional differences in screening practices.
Regularity of screening attendance is important for women with a false positive result as these women have a higher risk of breast cancer.20–22 Studies have shown that false positive screening results cause short-term and long-term psychological distress,16,23,24 and the long-term psychological consequences might influence women's decision to re-attend screening. 24
BreastScreen Norway started in 1996 and offers biennial mammographic screening to all women aged 50–69 who have a Norwegian social security number. 25 In 2025, the program targets 680,000 women, who are invited to a screening at 16 stationary and four mobile units. The Cancer Registry at the Norwegian Institute of Public Health administers the screening program, which includes monitoring and quality assurance of the program. A study on re-attendance in BreastScreen Norway was published in 2003, reporting a rate of 91.8% among women screened negative and 83.9% among those with a false positive screening result. 26 The rate has been monitored continuously since the start-up of the program, and in 2019, a study using data from BreastScreen Norway showed a higher risk of interval cancer and screen-detected cancer in the consecutive screening rounds for women with a false positive versus a negative screening result. 22 The results led to a discussion about the necessity of making an intervention to increase attendance after a false positive screening result and/or offer these women an extra screening examination. As part of this work, it was decided to update the results on attendance in the relevant groups. The aim of this study was therefore to update the evidence on re-attendance among women with a false positive versus negative screening result in BreastScreen. We hypothesized that re-attendance would be lower for women with a false positive versus negative screening result.
Methods
This study has a legal basis in accordance with Articles 6 (1) (e) and 9 (2) (j) of the General Data Protection Regulation. The data was disclosed with a legal basis in the Cancer Registry Regulations section 3-1 and the Health Register Act section 19 a to 19 h. 27
We received individual pseudonymized data on invitations and attendance among all women targeted by BreastScreen Norway since its start-up in 1996 and up to 2023 from the Cancer Registry of Norway. The Cancer Registry administers the screening program, which includes collection and storage of information related to screening invitations, attendance, and outcome, in dedicated databases. 28 BreastScreen Norway invites women aged 50–69 to biennial mammographic screening. The women are invited either by a postal or digital invitation letter with stated time and place for the examination. Together with the invitation, women receive an information leaflet explaining benefits and harms of screening, including links to further information. 28 Digital invitations were implemented in 2014 and in 2022, 59% of the target group used the digital invitation service. A reminder is sent to women who do not attend their scheduled appointment, 4 weeks after the missed appointment. The reminder is an open invitation encouraging the recipient to contact their local breast center to schedule a new appointment within 6 months after the scheduled appointment. Results of a negative screening examination are sent by post (physical or digital letter). Women with a positive screening result are called back for further assessment via a summons letter or a phone call from their respective breast center. Recall assessments usually take place within 3 weeks of screening. The outcome of the assessment is communicated to the woman immediately after the assessment, by phone or at an appointment.
During the first 25 years of the screening program, the average annual attendance rate was 75% and 86% of the invited women had attended once or more.25,28 For the same period, the average recall rate was 3.3%, with an invasive procedure (needle biopsy) performed in about 50% of the recall assessments, while the rate of screen-detected cancers was 0.59%. The cumulative risk of a false positive screening result is heavily depending on the recall rate.29,30 In a review from 2013 including European breast cancer screening programs, the cumulative risk of a false positive result ranged from 8% to 21%. 30 The cumulative risk of a false positive result including a needle biopsy was substantially lower. In BreastScreen Norway, the cumulative risk of a first false positive result has been reported to be 18% over 10 biennial screening rounds, while the risk was 5% for a false positive result with needle biopsy. 31
Study sample
The primary sample included information from all women with at least one attendance in the period from 1996 to 2021 and an invitation to the subsequent screening round in BreastScreen Norway during the period from January 1998 to 2023 (eligible for re-attendance). Screening results from 2023 or the last attendance from a woman aged 69 years were, for example, not included, as solely information on attendance/non-attendance to link it to the prior screening result was required for analyses. The screening interval in BreastScreen Norway is 2 years ± 6 months, and the median number of days between two consecutive examinations is 731 days. 25 Attendance after a reminder was also included in our study sample. We excluded examinations of women with a prior breast cancer diagnosis and screening examinations that resulted in a recall due to clinical symptoms or technically inadequate images (Figure 1).
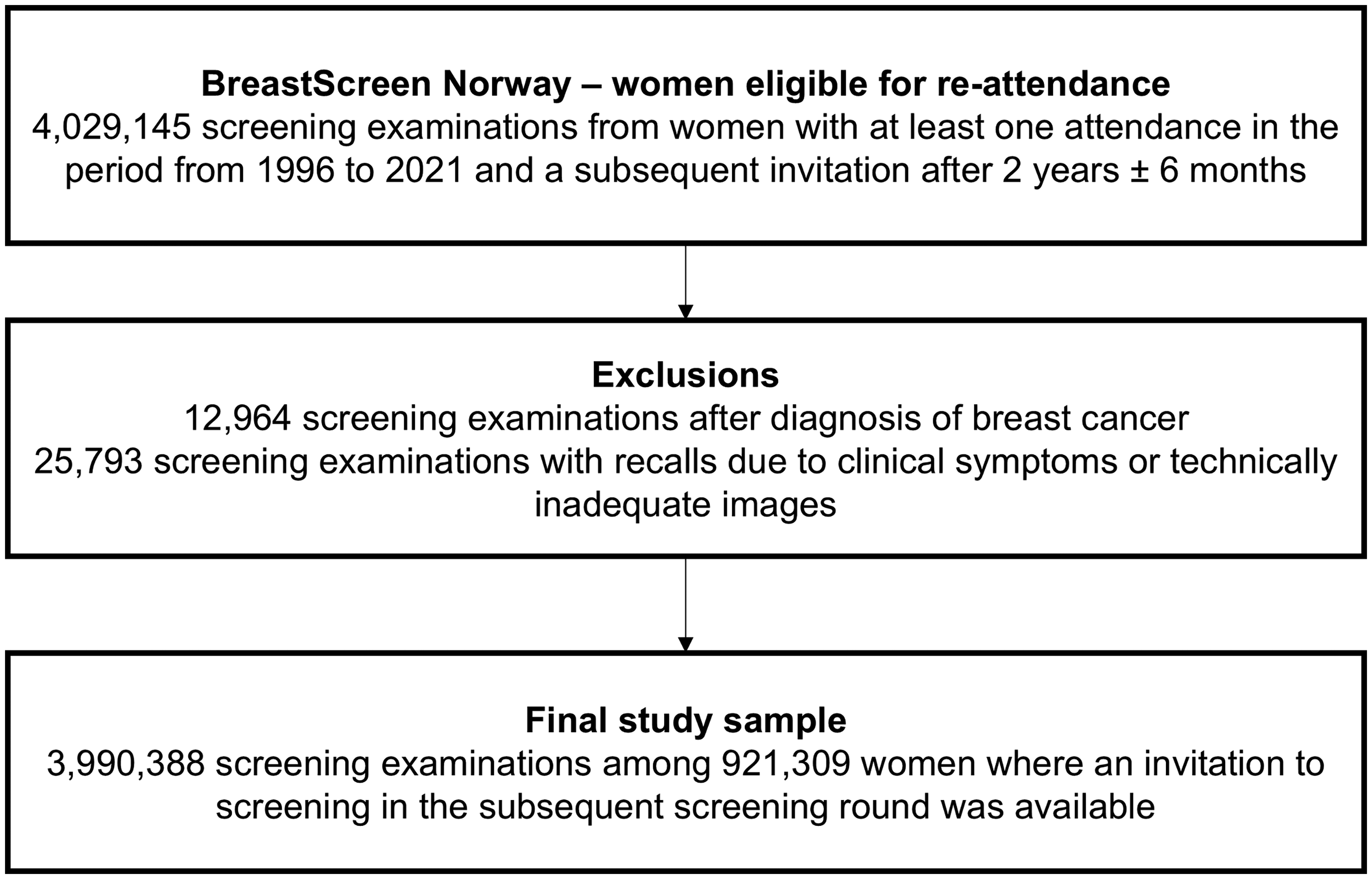
The flowchart of the study sample.
Variables of interest
A false positive screening result was defined as a recall for further assessment due to mammographic findings without breast cancer being diagnosed. A recall assessment usually includes additional mammographic imaging, ultrasound and/or an invasive procedure. 25 In this study, results were presented for any false positive and for those with or without a needle biopsy. If no needle biopsy was performed, the women had their result before they left the hospital. The waiting time for results of a needle biopsy usually varies between 3 and 15 days, whereafter the women were informed by phone or at an appointment with a radiologist, surgeon or oncologist. A negative screening result was defined as a screening examination interpreted negative at initial screen-reading or after a consensus meeting, consisting of two to three radiologists deciding if a woman should be recalled for further assessment or not. The woman was informed of this within 2–4 weeks of the screening examination. The primary outcome in this study was re-attendance to the subsequent screening round in BreastScreen Norway. Other variables included in analyses were age at invitation (years) and screening history (prevalent, subsequent regular, and subsequent irregular). A prevalent examination was defined as a woman's first attendance. Subsequent regular was a subsequent examination registered within 24 ± 6 months of the last attendance, while subsequent irregular was a subsequent examination registered more than 24 ± 6 months since the last attendance. 25 For women with a false positive screening result, number of days between the screening examination and the follow-up examination was included.
Statistical analysis
Mixed logistic regression models with a random intercept were used to analyze the association between screening results and re-attendance in the subsequent screening round. The intercepts in the regression models were used to account for repeated measures (examinations). For the overall study sample, odds ratios (ORs) with 95% confidence intervals (CIs) for re-attendance were presented for two models. The first model included any false positive versus negative as the exposure variable, while the second model included a false positive with a needle biopsy, false positive without a needle biopsy, and negative result as the exposure variable. Both models used negative screening results as the reference category. Adjustment variables were age and screening history as these were considered potential confounders. Secondary analysis only included women with a false positive screening result. Re-attendance was analyzed by including days between screening and follow-up assessment and first, second or third/fourth/fifth false positive in addition to age and screening history. Age and days from screening to further assessment were presented categorically in the descriptive table but used as continuous variables in the regression analyses. Differences in probabilities of re-attendance for negative and false positive results were estimated from the regression coefficients using marginal average effects. We used STATA Version 18.5 (StataCorp, TX, USA) for all statistical analyses.
Results
The study sample included 3,990,388 screening examinations performed during the period 1996 to 2021 with information about re-attendance in the subsequent screening round, 1998–2023, among 921,309 women (Figure 1). In the study sample, 2.7% (108,551/3,990,388) of the examinations had a false positive screening result (Table 1). Unadjusted for dependency between observations and other variables, the crude re-attendance rate after a negative screening result was 90.8% (3,523,000/3,881,837). For women with a false positive result, re-attendance was 88.3% (95,838/108,551). The lowest re-attendance was observed for the youngest women in the target group regardless of the result of the prior examination. The percentage of re-attendance among women with a false positive versus a negative screening result was lower for all age groups and for prevalent as well as subsequent regular attendance. For subsequent irregular screening history (did not attend the examination prior to the examination with a false positive result), 77.4% attended the subsequent screening round after a false positive result compared to 75.3% for those with a negative result.
Re-attendance rates in the subsequent screening round for 3,990,388 screening examinations based on screening outcome in BreastScreen Norway.
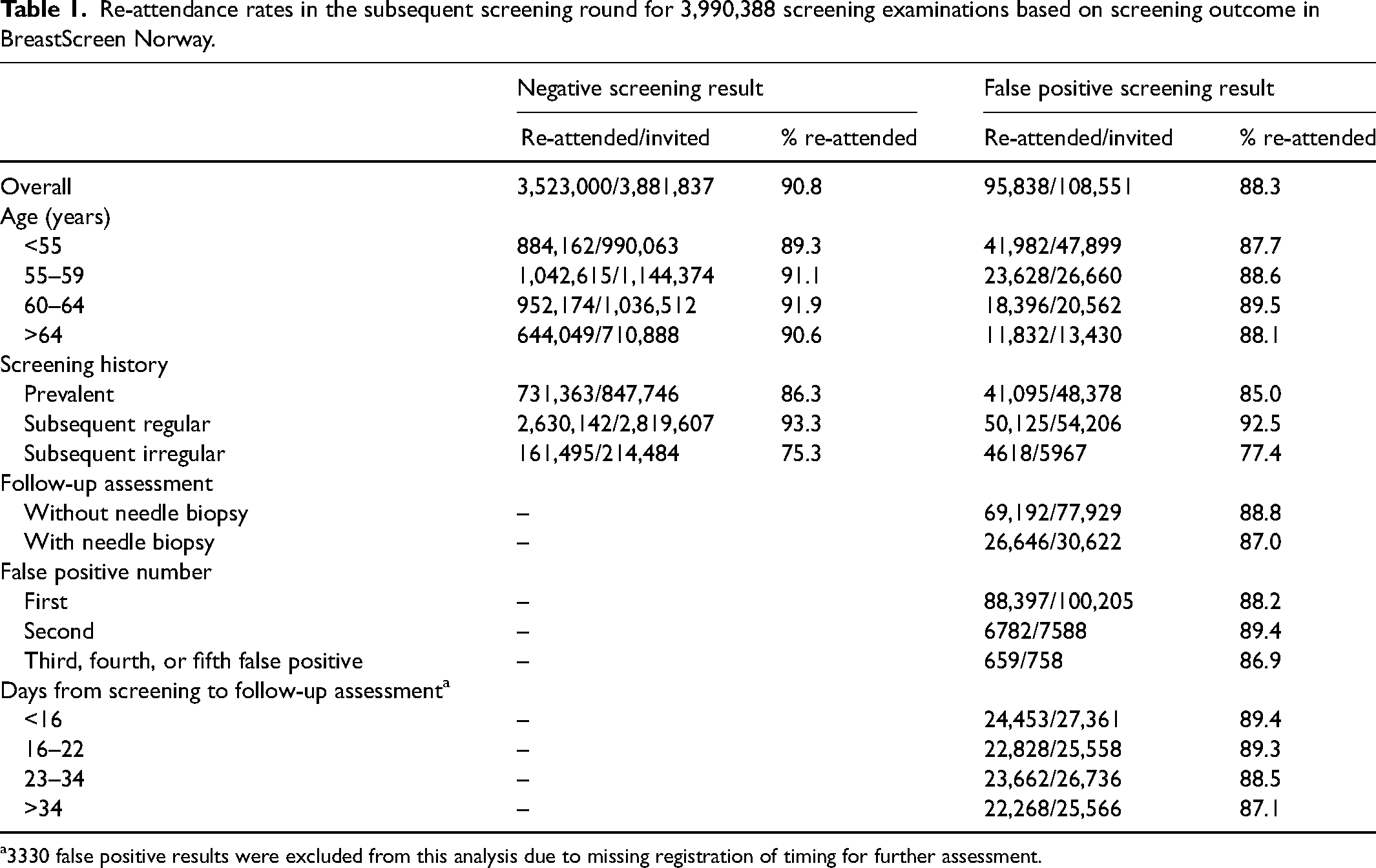
3330 false positive results were excluded from this analysis due to missing registration of timing for further assessment.
Re-attendance after a false positive or negative screening result was stable during the period 1996–2021 (Figure 2). Re-attendance stratified by screening round and screening result is presented in Supplemental Table 1.
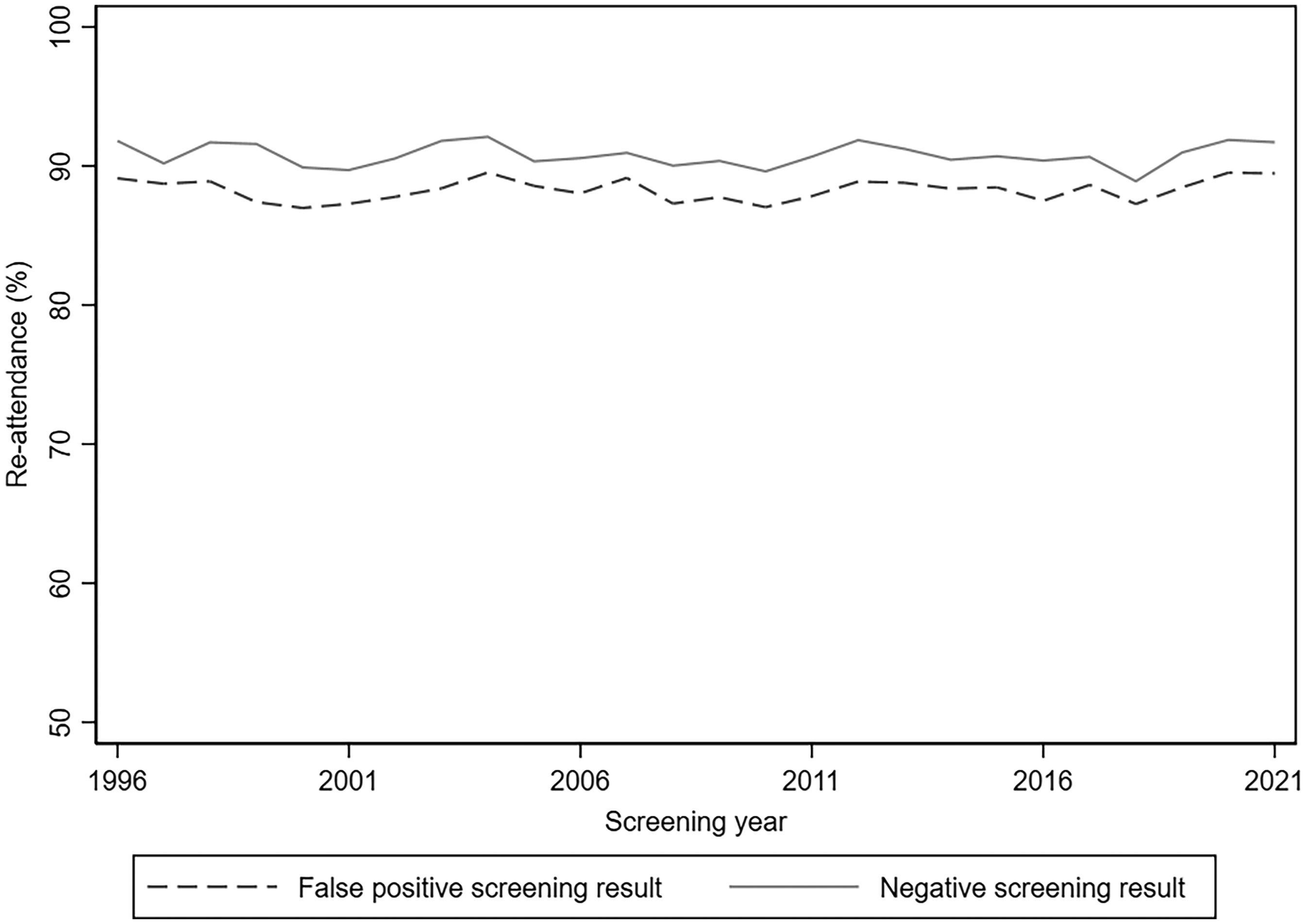
Re-attendance in the subsequent screening round after a false positive or negative screening result among 3,990,388 examinations performed in 1996–2021.
Among women with a false positive screening result, re-attendance was 87.0% (26,646/30,622) for those who underwent a needle biopsy and 88.8% (69,192/77,929) for those who did not undergo biopsy (Table 1). Re-attendance after a first false positive result was 88.2% (88,397/100,205), while it was 89.4% (6782/7588) after a second false positive result. For women with a false positive result, re-attendance was 89.4% (24,453/27,361) when time from screening to follow-up assessment was < 16 days and 87.1% (22,268/25,566) when time from screening to follow-up assessment was >34 days.
Adjusted for age at screening and screening history, the odds of re-attendance were lower for women with a false positive screening result compared to women with a negative result (OR = 0.91, 95% CI: 0.87–0.93) (Table 2). Using a negative result as reference, adjusted OR for women with a false positive result with versus without a needle biopsy was 0.85 (95% CI: 0.82–0.87) versus 0.93 (0.91–0.96), respectively. Adjusted predicted difference in re-attendance was 0.7 percentage points (95% CI: 0.6–1.0) for a negative versus false positive result (88.9%, 95% CI: 88.9–89.0 vs. 88.2%, 95% CI 88.0–88.3).
Unadjusted and adjusted odds ratio (OR) with 95% confidence intervals (CIs) for re-attendance calculated using mixed logistic regression. Adjusted results included screening result, age at screening and screening history as covariates.
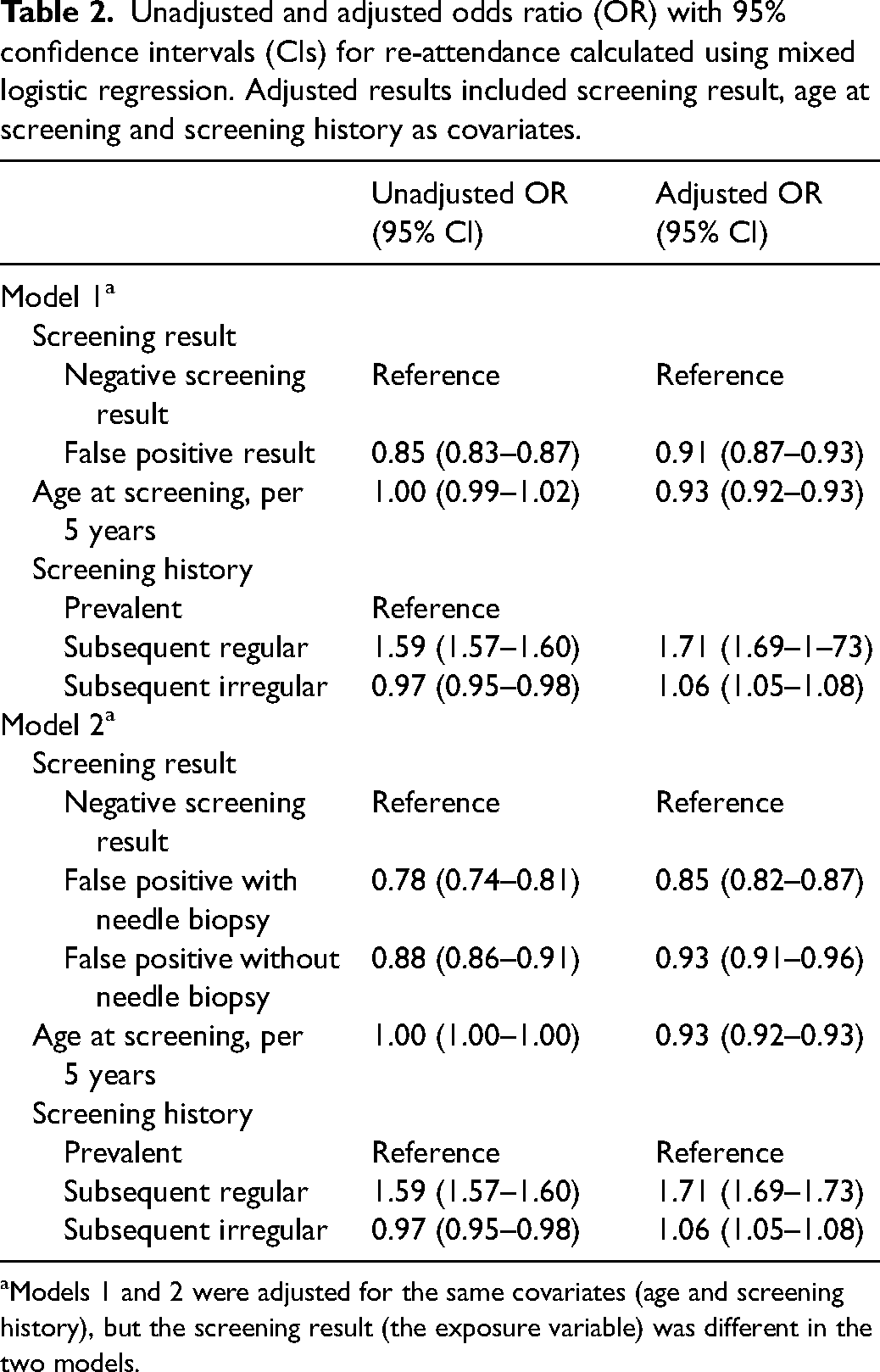
Models 1 and 2 were adjusted for the same covariates (age and screening history), but the screening result (the exposure variable) was different in the two models.
When including only false positive screening results in the regression analyses, adjusted OR for re-attendance was 0.89 (95% CI: 0.85–0.92) for false positives with a needle biopsy compared to those without a needle biopsy (Table 3).
Unadjusted and adjusted odds ratio (OR) of re-attendance with 95% confidence interval (CI) in the subsequent screening round after a false positive screening result. a
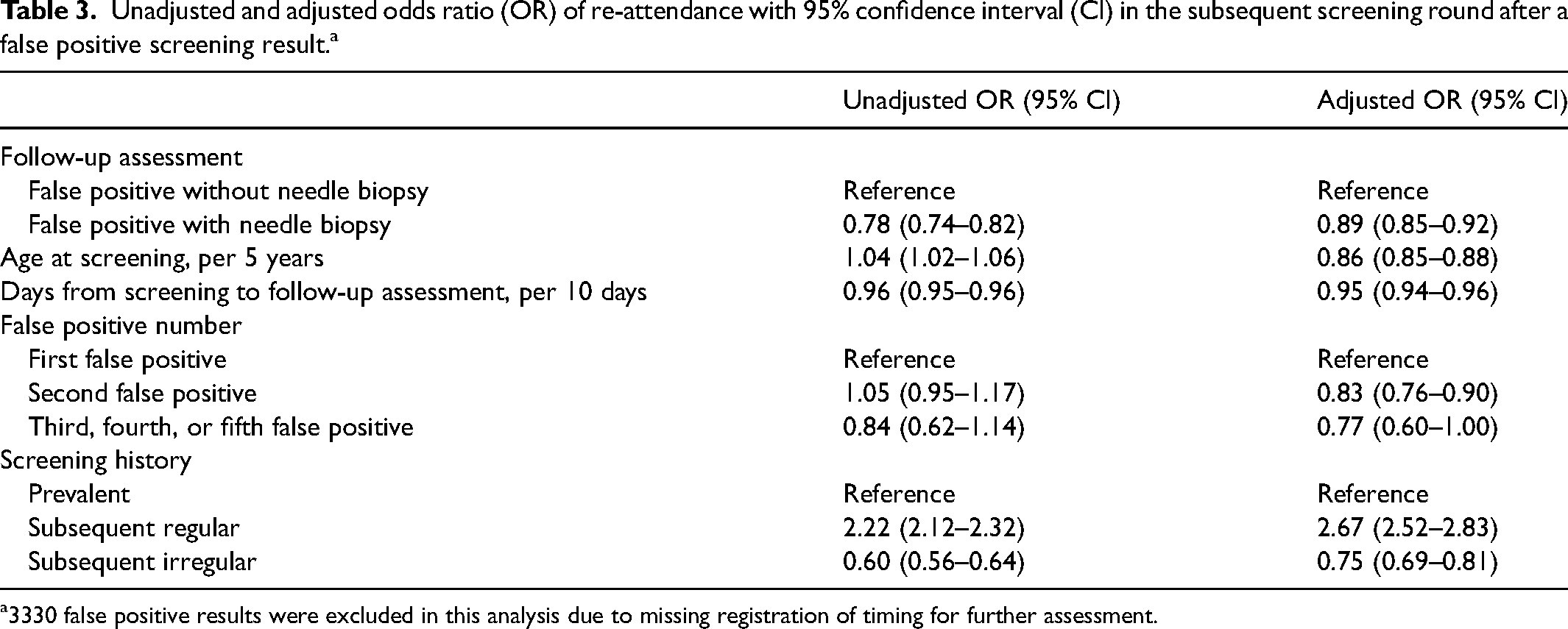
3330 false positive results were excluded in this analysis due to missing registration of timing for further assessment.
Discussion
Based on 25 years of screening data available from BreastScreen Norway, re-attendance in the screening program was lower after any false positive screening result, and specifically after a false positive with a needle biopsy, compared to a negative screening result.
Our findings are in line with our hypothesis and results from previous studies.7,14,21 However, the difference in re-attendance between a false positive and negative result was smaller in our study compared to other studies. In a systematic review and meta-analysis, 23% lower odds were reported based on six studies for women with a false positive result compared to women with a negative result. 7 In our study, we found 10% lower odds, but estimates cannot be directly compared. A study with 3,529,825 screening mammograms found that women were more likely to return after a negative result and estimated the adjusted absolute difference to be 1.9 percentage points lower for those with a false positive screening result. 14 In our study, the predicted difference was 0.7 percentage points. With data from the Stockholm Mammography Screening program, it has been reported that screening attendance in the subsequent screening round was statistically significantly lower for women with a false positive screening result compared to those without a false positive result (84.6% vs. 86.5%). 21 A recent study from the Netherlands reported a screening re-attendance rate of 81% after a false positive result, but re-attendance after negative results was not included, 32 while an older study from the Netherlands showed no significant differences in re-attendance by screening results. 19
In our study, the odds of subsequent re-attendance were lower for women who underwent a needle biopsy as part of their follow-up assessment compared to those without a needle biopsy. In the recent study from the Netherlands, similar findings were reported. 32 In that study, the OR of re-attendance was 0.48 (95% CI: 0.36–0.64) for women with a false positive referral who underwent invasive examinations (needle biopsy) after referral compared to those who only received additional imaging. In our study, the OR was 0.89 (95% CI: 0.85–0.92). Further assessment with versus without a needle biopsy might be associated with more anxiety and discomfort, in addition to waiting time for the results of the biopsy. Our findings highlight the importance of minimizing the use of invasive follow-up techniques to reduce the psychological burden and improve attendance rates in a subsequent screening round. This emphasizes the need for methods with higher sensitivity than mammography alone, which could reduce the use of invasive procedures with a benign outcome. Rates of invasive procedures are generally high in Norway, 2.1% for prevalent and 1.1% for subsequent screening examinations, compared to other European countries offering organized breast cancer screening, where the rates are 0.8%–1.7% for prevalent and 0.3%–0.9% for subsequent screening examinations. 30
The odds of re-attendance among those with a false positive result decreased with increasing time between screening and further assessment. Long waiting periods between screening and further assessment might be associated with increasing anxiety about the result and could therefore lead to unwillingness to attend the subsequent screening round. It is also possible that some women experiencing a long gap between screening examination and further assessment decide to skip the next screening examination due to a short gap between follow-up examination and the next screening invitation. However, this is less likely since 3/4 of women have a waiting time of < 35 days.
A recent study from BreastScreen Norway showed that 84% of women in the target group considered the information received along with the invitation to screening, on benefits and harms of attending the screening program, as largely sufficient. 33 However, despite good knowledge of benefits and harms, importance of regular attendance might not be communicated well enough to the women in the target group of the screening program and might thus be reflected in the results of this study. As regular attenders are at a lower risk of breast cancer death compared to irregular attenders or non-attenders, 34 and false positive results are associated with an increased risk of interval and next round screen-detected breast cancer, 22 women with false positive screening results should be informed about the importance of re-attendance. Preventive measures for these women could be a separate letter attached to their next invitation to screening, encouraging them to attend, or an extra examination after one year, as they are at increased risk of breast cancer.21,22 Personalized screening schemes for women with a false positive result might be considered in the future.
Psychological distress and anxiety caused by the recall assessment and false positive screening result are suggested as reasons for lower re-attendance rates.16,23,24 Negative psychosocial consequences of false positive screening results have been shown to diminish after 3 years. 24 This might indicate that skipping one round could give enough time to stabilize levels of negative psychological consequences and attend the next round. In this study, we only looked at re-attending the subsequent screening round. On the other hand, studies have shown that the levels of anxiety and distress caused by false positive screening results might be transient and might not explain lower re-attendance at the subsequent screening round.24,35,36
A major strength of our study was the large sample in which screening attendance could be linked with the screening history for each individual woman. The study also had limitations. The women's background information such as general health or socioeconomic, employment and marital status was not collected, but could have been helpful for better understanding the groups of women who did not re-attend.
Conclusion
Overall, the findings in our study emphasize the importance of addressing the psychological consequences of false positive screening results to increase attendance rates in the subsequent screening round. This could be achieved by providing appropriate information, support, and counseling to the women affected. Women with a false positive screening result should also be informed about the increased risk of breast cancer, and thereby the importance of attending regularly. Finally, efforts to minimize the use of biopsies could also help reduce the psychological burden and harm of screening and thereby increase re-attendance rates and compliance in mammographic screening.
Supplemental Material
sj-docx-1-msc-10.1177_09691413251329671 - Supplemental material for Re-attendance to mammographic screening after a false positive screening result
Supplemental material, sj-docx-1-msc-10.1177_09691413251329671 for Re-attendance to mammographic screening after a false positive screening result by Marthe Larsen, Nataliia Moshina, Åsne Sørlien Holen, Marie Burns Bergan and Solveig Hofvind in Journal of Medical Screening
Footnotes
Data availability statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.