
Abstract
Objectives
To evaluate the economic benefits of implementing an organized community-based screening program for oral, breast, and cervical cancers in rural Bangladesh.
Methods
A cost–benefit analysis was conducted over a one-year time horizon, with program costs estimated from the provider perspective and economic benefits assessed from the household perspective. Screening costs were estimated using primary data from a 2024 pilot implementation and extrapolated to all rural areas nationally. Economic benefits were defined as savings from averting late-stage cancer through early detection and included avoided direct medical and non-medical costs, income loss of patients and caregivers, and intangible benefits related to pain and distress. Benefit estimates were derived from a facility-based survey of 346 patients with oral, breast, or cervical cancer and extrapolated to the rural population using an incidence-based approach. Parameter uncertainty was assessed using one-way and probabilistic sensitivity analyses.
Results
The total annual cost of implementing the screening program in rural Bangladesh was estimated at US$69.02 million. Total annual economic benefits were estimated at US$106.77 million, yielding net benefits of US$37.76 million and a benefit–cost ratio of 1.55. Probabilistic sensitivity analysis indicated a high likelihood of cost–benefit, with 98.9% of simulations exceeding unity.
Conclusions
An organized community-based screening program for oral, breast, and cervical cancers in rural Bangladesh is economically favorable and robust to uncertainty, even under conservative benefit assumptions. The findings support a transition from opportunistic to organized screening in Bangladesh, and provide policy-relevant evidence for cancer control planning in other resource-constrained settings.
Keywords
Introduction
Cancer constitutes one of the most significant global public health challenges, accounting for approximately one in six deaths worldwide. 1 Low- and middle-income countries (LMICs) bear a disproportionate share of the global cancer burden, driven by demographic transitions, epidemiological shifts, and constrained health-system capacity.2–4 Projections indicate that cancer incidence will rise substantially faster in developing countries than in developed countries in the coming decades. 5 Bangladesh exemplifies this trend, where cancer has emerged as the third leading cause of death, accounting for approximately 7.7% of all fatalities. 6 Among all types of cancers, oral, breast, and cervical cancers are among the most prevalent in the country, which together constitute over 23.2% of all diagnosed cases. 7 Beyond their substantial contribution to morbidity and mortality, these three cancers impose considerable economic burdens on households and the health system. These burdens primarily arise from high out-of-pocket (OOP) expenditures, productivity losses, and psychological distress.8,9
Despite national policy initiatives, including the National Cancer Control Strategy and Action Plan (2009–2015) and the Multisectoral Action Plan for Prevention and Control of Non-communicable Diseases (2018–2025), cancer incidence and mortality in Bangladesh have continued to rise.10–12 This trend is closely linked to persistent limitations in access to timely diagnosis and appropriate cancer care. Cancer screening coverage in the country remains limited, contributing to a high proportion of late-stage diagnoses. 13 Moreover, cancer treatment is largely centralized in urban areas. 14 As a result, approximately two-thirds of the country's population residing in rural areas tend to experience poorer access to treatment and worse clinical outcomes than their urban counterparts.13,15–17 These disparities reflect structural weaknesses in cancer care delivery, screening coverage, and referral pathways.
At present, Bangladesh relies predominantly on an opportunistic approach to cancer screening, focusing entirely on breast and cervical cancers. A national cervical and breast cancer screening initiative, supported by Bangladesh Medical University (BMU), has been in operation since 2005. By 2020, 503 visual inspection with acetic acid (VIA) and clinical breast examination (CBE) centers had been established across primary, secondary, and tertiary levels, with 25 medical college hospitals and BMU serving as referral centers for screen-positive cases. 13 However, this approach remains limited in scale and opportunistic in nature, resulting in the systematic under-reach of at-risk populations. As a result, population coverage remains low, estimated at only 1.7% for breast cancer and 8.8% for cervical cancer screening. 18 Such limited reach constrains the potential of screening to reduce late-stage disease and the associated economic and health burdens.
In contrast, organized screening programs have demonstrated superior performance in multiple countries. These programs are defined by systematic population identification, proactive invitation, adherence to evidence-based screening guidelines, and clearly defined referral and follow-up pathways. International evidence indicates that organized screening is associated with earlier cancer detection, improved treatment outcomes, and more efficient use of health-system resources.19–22 In addition, studies evaluating the existing opportunistic screening program in Bangladesh have strongly recommended a transition to a population-based, systematic screening approach to achieve higher coverage.23,24 Despite this growing body of international and country-specific evidence, a community-based, organized cancer screening approach has yet to be implemented in Bangladesh. Notably, the existing opportunistic screening infrastructure for breast and cervical cancer provides a strong foundation for implementing an organized community-based screening approach. This includes a wide network of screening centers across levels of care, trained service providers, and established referral and follow-up mechanisms. Moreover, within this existing framework, the inclusion of oral cancer screening would require minimal additional resource commitment. 25 Oral visual examination (OVE) can be readily integrated into current service delivery and has the potential to substantially reduce the burden of oral cancer through earlier detection. 26
Although several studies have examined existing screening initiatives in Bangladesh and identified potential implementation challenges,13,23,24,26 a comprehensive economic evaluation capable of informing national policy decisions on the adoption of organized community-based screening remains lacking. In resource-constrained settings, such evidence is particularly critical, as governments must weigh the expected benefits of large-scale public health interventions against their financial and opportunity costs. Cost–benefit analysis (CBA) is particularly well suited to this decision context, as it enables a direct comparison of program costs against monetized economic returns.
Against this backdrop, this study aims to evaluate the net economic benefits of implementing an organized community-based screening program for oral, breast, and cervical cancers in rural Bangladesh using a CBA framework. The focus on rural areas is motivated by their higher cancer burden, poorer clinical outcomes, and the presence of an established community clinic (CC) network that provides a feasible platform for community-based organized screening delivery.27,28 By generating policy-relevant evidence, this study seeks to inform governmental decision-making and to offer a transferable model for other LMICs facing similar constraints.
Methods
Program design, eligible population, and screening modalities
The proposed screening program is anchored at CCs, which are the lowest-tier public health facilities in Bangladesh and the primary point of care for rural populations. Approximately 14,377 CCs provide primary healthcare services in rural areas, each covering three wards and serving a population of about 6000.28,29 Each union parishad, comprising nine wards, typically hosts three CCs, and there are approximately 4596 union parishads nationwide. The proposed program is designed to operate across all union parishads and their corresponding CCs to ensure broad and equitable coverage of the rural population. Screening activities are proposed to take place six days per week, with services delivered on two consecutive days at each CC in a rotating schedule to cover the three CCs within a union. For program implementation, one nurse and one nurse assistant would be appointed at the union level and would rotate across CCs, supported by two paid volunteers and a Community Health Care Provider at each CC for participant mobilization and registration.
Suspected cases from CCs would be referred to the nearest Upazila Health Complex (UHC) for sample collection and further evaluation. To support this referral pathway, at least one female medical officer in each of the 434 UHCs would receive training in relevant diagnostic procedures. Where additional confirmatory testing is indicated, samples would be referred onward to higher-level facilities. The program design was refined through consultations with clinicians and program implementers experienced in cancer screening and referral practices in Bangladesh. A schematic overview of the program design is presented in Figure 1.
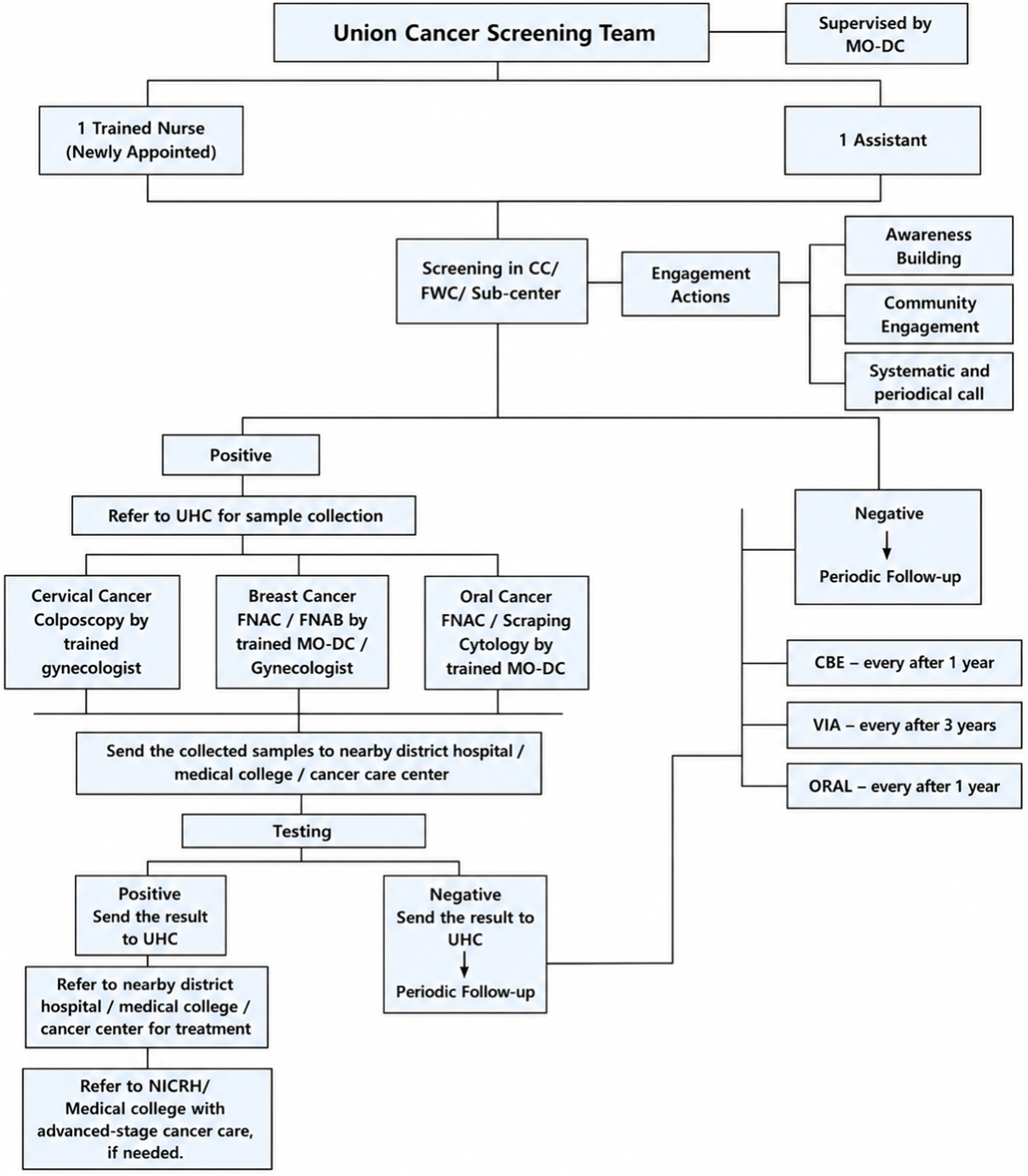
Screening program design.
The proposed program targets women aged 30–59 for breast, cervical, and oral cancer screening, while men in the same age group are eligible for oral cancer screening. Screening is intended to be delivered through organized invitations to attend designated CCs located near participants’ residences. The proposed screening modalities include VIA for cervical cancer, CBE for breast cancer, and OVE for oral cancer. The target population and screening modalities are consistent with scientific evidence and resource-appropriate practices currently implemented in Bangladesh.18,26,30,31
Data sources and parameters
Primary data
For union- and upazila-level cost estimation, primary cost data were derived from a 2024 pilot implementation of an organized community-based screening program for cervical, breast, and oral cancers conducted in Nawly village, Jashore. 30 This pilot was implemented under routine public sector conditions and was designed to reflect feasible service delivery using existing primary healthcare infrastructure. Cost estimation followed an ingredients-based (normative) costing approach, reflecting the full set of resources required for effective service delivery under a fully functional implementation scenario. Cost data from the pilot were shared with the study team through project collaboration and included detailed information on equipment, supplies, unit prices, operational expenditures, and information, education, and communication (IEC) and behavior change communication (BCC) activities. Data on personnel salaries, diagnostic test fees at higher-level facilities, and training-related expenditures were informed by consultations with practicing oncologists, while estimates of equipment life span were obtained from publicly available sources.
This study was conducted as part of the project titled “Introducing a National Cancer Screening Program with an Organized Community-based Approach.” In the absence of published evidence from Bangladesh on the economic benefits of cancer screening programs and given the lack of a national cancer registry, benefit estimation relied on a combination of primary survey data and secondary data sources. Primary data were obtained through a facility-based survey carried out between March and May 2024 in eight tertiary-level hospitals located in Dhaka, Chattogram, and Rajshahi. Together, these facilities encompass nearly all public and non-governmental tertiary institutions providing advanced cancer care in Bangladesh and were selected through expert consultation. The list of facilities included in the facility-based survey is provided in section 1 of the online Supplemental Material. Eligible participants were adult patients (≥18 years) with a confirmed diagnosis of oral, breast, or cervical cancer who were receiving or had recently completed treatment at the selected facilities. Two patient groups were included in the survey: (i) follow-up outpatients attending post-discharge visits and (ii) discharged patients immediately after completing brachytherapy or radiotherapy. Data were gathered using structured questionnaires administered through face-to-face interviews with 346 patients. The survey instrument included modules on facility characteristics, patient sociodemographic and household information, disease and treatment-related information, and detailed cost and financing components. A purposive consecutive sampling strategy was employed to ensure adequate representation of advanced-stage cases. The majority of patients were in stage III (217) or stage IV (47), while early-stage cases were limited (stage I: 1; stage II: 22), and a proportion had an unknown stage at diagnosis (59). The sample comprised 167 breast cancer cases, 113 cervical cancer cases, and 66 oral cancer cases. Patient-reported direct medical and non-medical costs were collected from the time of diagnosis, alongside income-related data and workdays lost for both patients and caregivers. In order to estimate the intangible costs related to psychological distress, we applied a contingent valuation approach, in which each respondent was asked to report their maximum willingness-to-pay (WTP) to avoid pain and suffering within their household's financial capacity. 8
Secondary data
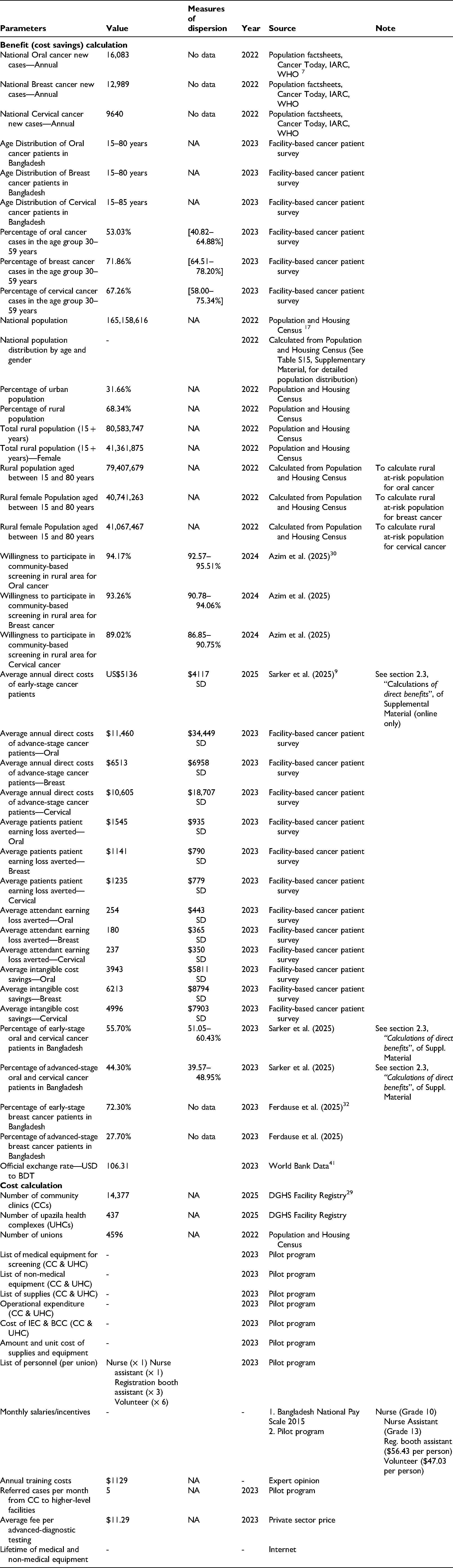
Secondary data were obtained from academic literature and government reports to inform cancer-specific national incidence, early-stage direct costs, population size and age–sex distribution, rural–urban population composition, screening participation rates, and the proportion of early- and late-stage disease by cancer type in Bangladesh.7,9,17,30,32 A comprehensive list of parameters, their corresponding values, and data sources is provided in Appendix 1.
Cost–benefit methodology
A CBA was conducted using a one-year analytical framework for both cost and benefit estimation. Costs represent the annual financial requirements of implementing the screening program, while benefits represent the annual economic gains associated with shifting cancer cases from late-stage to early-stage diagnosis in a given year. The analysis compared the direct costs of implementing the screening program with the economic benefits arising from earlier detection and treatment. All costs were identified from the provider perspective and evaluated using an ingredient-based approach. Only the direct costs of the screening were considered. Direct costs occurred at the union-level CCs and upazila-level UHCs, including costs of medical and non-medical equipment, supplies, salaries, training, operational expenses, IEC, and BCC expenses. Additional costs associated with suspected cases referred to nearby higher-level facilities were also incorporated. As this will be a new program, additional salaries for new staff, including a nurse, nurse assistant, and volunteers, as well as training costs for existing female medical officers, were included in the cost estimates. Capital costs were annuitized over the expected useful life of each item using a 3% discount rate. 33 Screening costs were calculated at three service delivery levels, namely per CC (union), per UHC (upazila), and per referred case at higher-level facilities. These unit costs were subsequently extrapolated using the total number of unions and UHCs in Bangladesh, along with the projected number of referred cases, to estimate the total screening cost in rural areas (Figure 2).
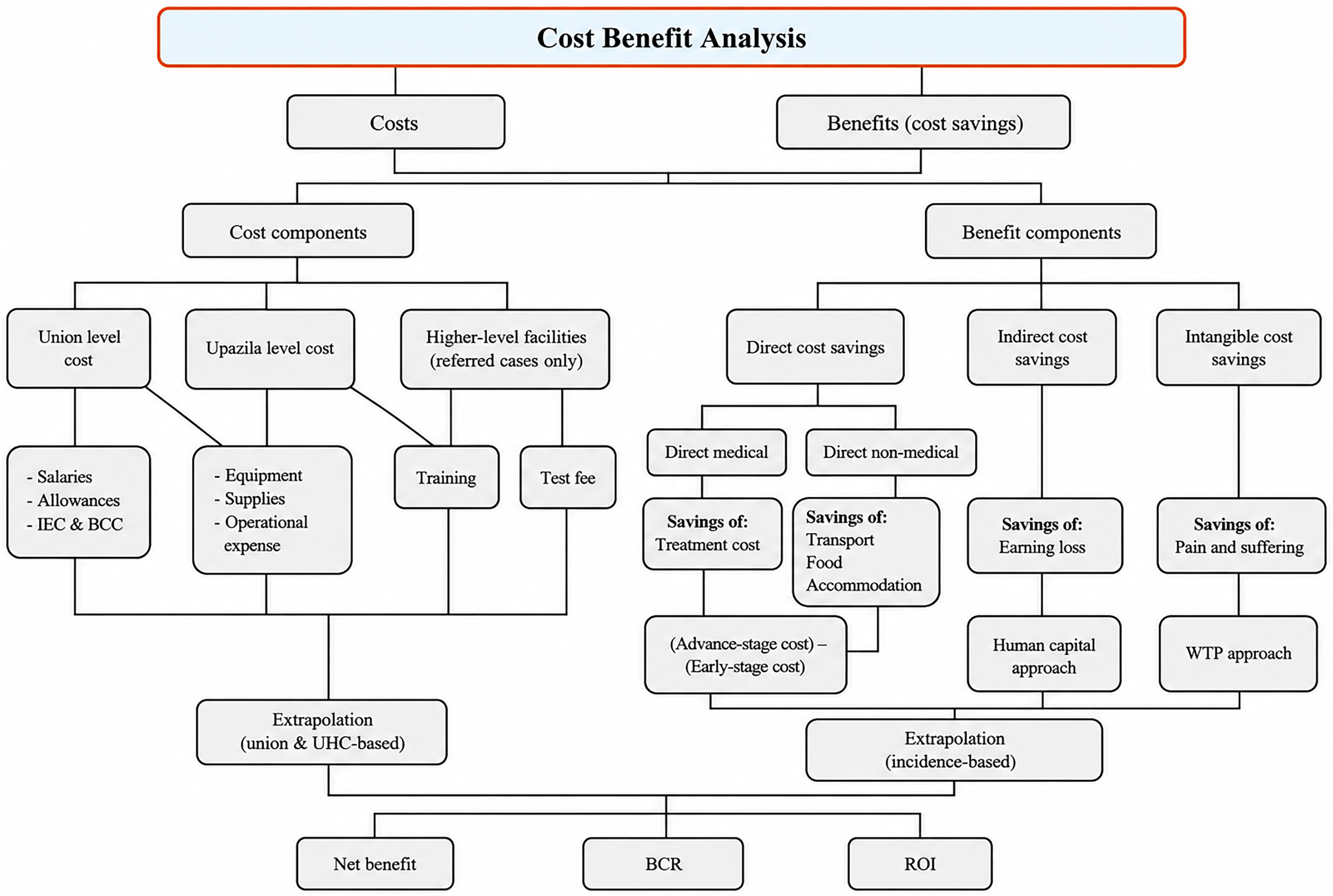
Analytical framework of cost–benefit analysis of an organized community-based cancer screening program.
In this study, benefits were defined as the cost savings associated with averting late-stage cancer cases through early detection. Following Drummond et al., three categories of benefits arising from the screening program were identified from household perspective: (i) future health care costs avoided, (ii) increased productive output (hereafter referred to as indirect benefits), and (iii) intangible benefits, defined as the value of improved health to cancer patients. 34 Future health care costs avoided were calculated as the difference between treatment costs for advanced-stage and early-stage cancer, incorporating both direct medical and direct non-medical costs. Direct medical costs comprised OOP expenditures related to health care resource use during treatment, including costs for medicines, diagnostic procedures, and other medical services. Direct non-medical costs included OOP expenditures incurred by patients and caregivers for transportation, food, accommodation, and other related expenses during care-seeking. Indirect benefits included income loss avoided for both patients and their caregivers. Intangible benefits, a dimension often overlooked in economic evaluations of screening programs, captured the monetized value of pain and suffering avoided through early detection, estimated using a contingent valuation approach based on individuals’ WTP. 8 We adopted an open-ended contingent valuation format in this study. While more structured formats, such as bidding games or discrete choice experiments, are available, we selected the open-ended approach to facilitate straightforward data collection and to capture respondents’ valuations of intangible costs with minimal respondent burden. Although this approach has limitations, it provides a useful foundation for incorporating intangible costs into health economic evaluations in the Bangladesh context. To implement this, we presented respondents with a hypothetical scenario and asked, “If there were a way to completely eliminate this suffering and difficulty, how much money would you or your family, based on your ability to pay, be willing to pay to obtain that solution?” We used the elicited WTP values as a proxy for the monetary value of psychological distress and quality-of-life losses associated with cancer.
All benefits, except intangible benefits, were annualized and adjusted for inflation. Average annual benefits per early-detected case were subsequently extrapolated using an incidence-based approach for rural areas, incorporating expected screening participation rates and the proportion of late-stage cancer cases in the rural population (Figure 2).
The result was calculated and presented using formulas for benefit–cost ratio (BCR):
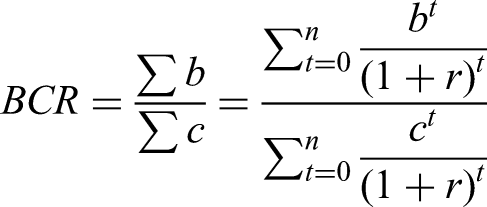
where b represents the total quantified benefits of the screening program (e.g. avoided treatment costs, absence from work, and pain and distress), and c denotes the total costs incurred to implement the screening (e.g. diagnostic equipment, operational expense, etc.). For the purposes of the current study, no discounting was applied because the costs were calculated for a period of 1 year (discount rate in the formula above is 0%). All the costs and benefits were referenced to the 2023 year standard and converted to US$ 2023 values. We used the CHEERS checklist when writing our report. 35
Sensitivity analysis
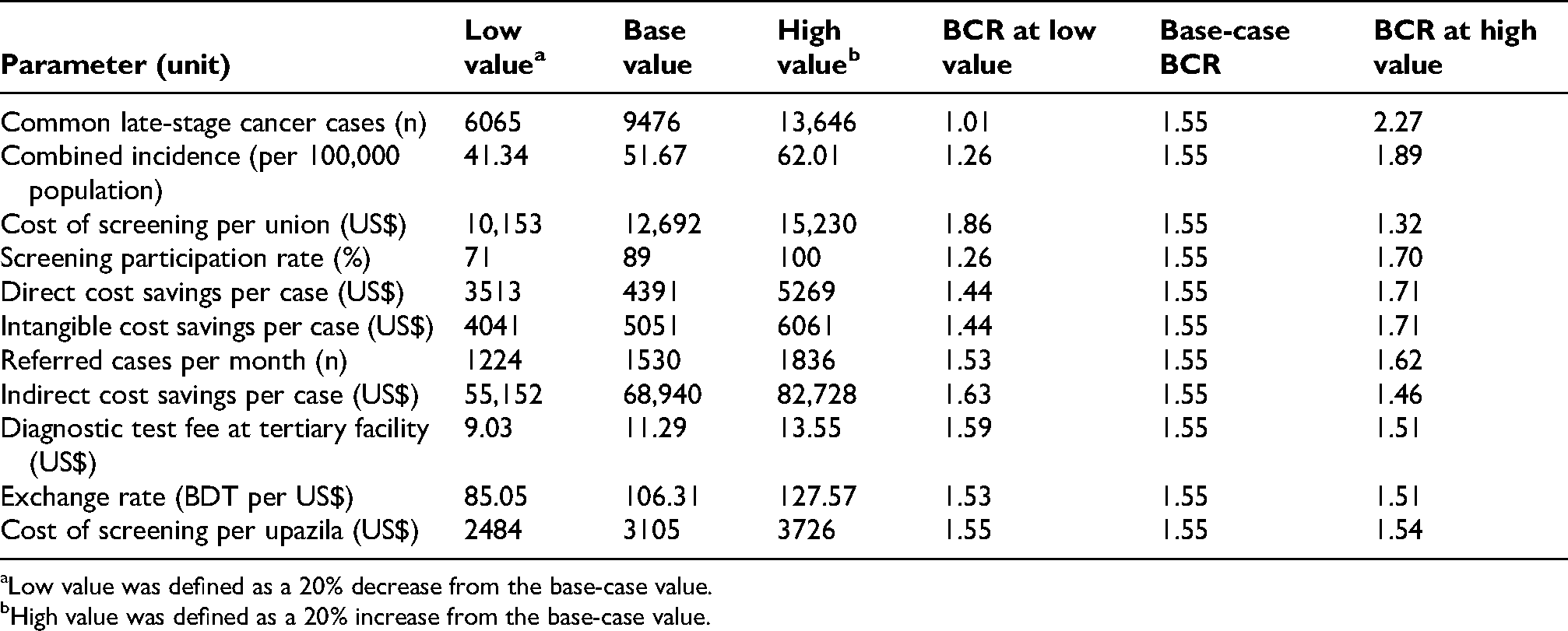
A one-way sensitivity analysis was conducted to assess the impact of uncertainty on individual parameters in the results. The findings are visually summarized using a tornado diagram, which highlights the relative influence of each parameter, and are also presented in Appendix 2. Each uncertain parameter was systematically varied by increasing and decreasing its baseline value by 20% to evaluate how these changes affect the outcome (BCR).
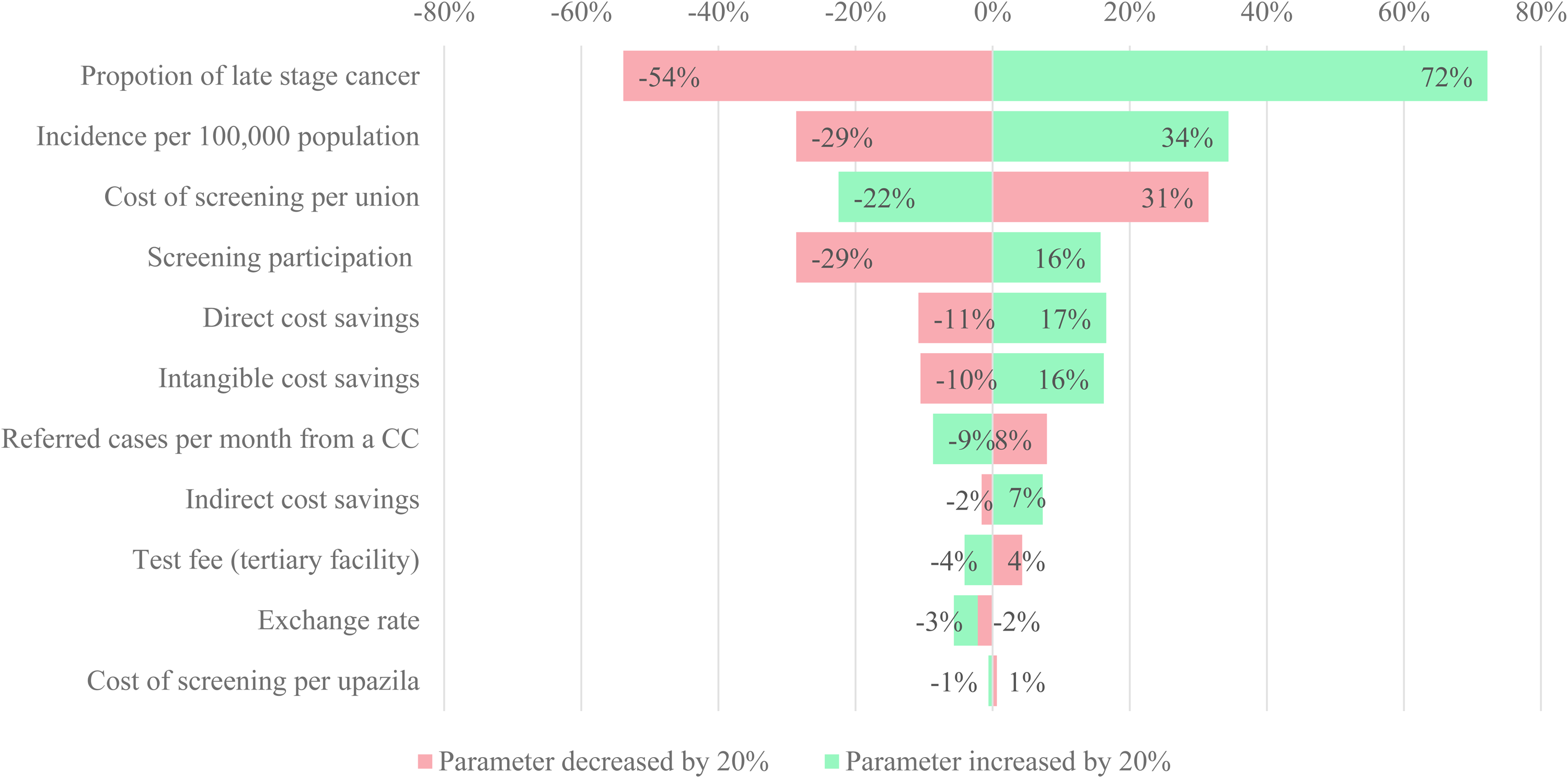
Tornado plot of the effect on the benefit–cost ratio of changing 20% of each parameter.
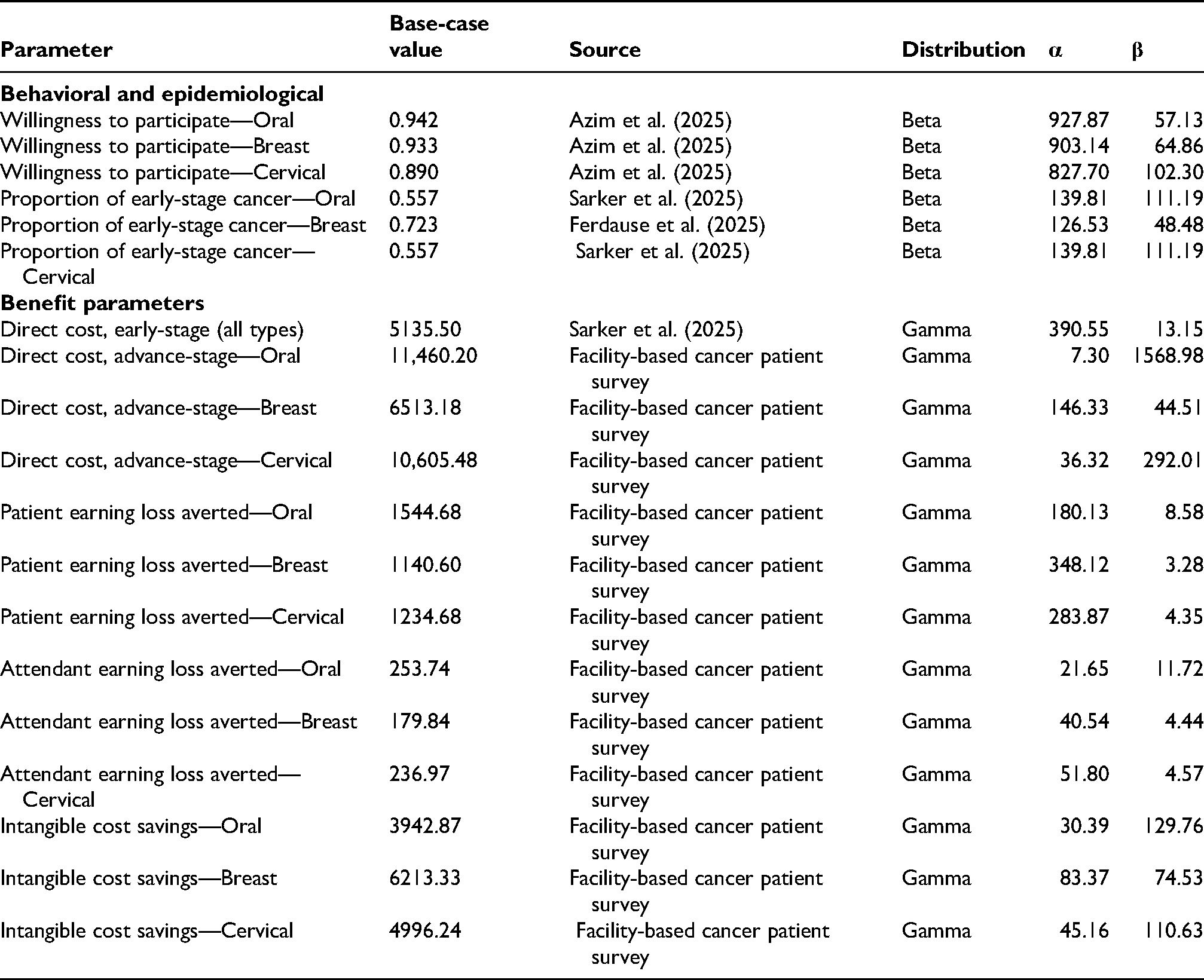
Probabilistic sensitivity analysis was also performed by assigning probability distributions to key model parameters based on observed means and associated statistical dispersion. Parameter uncertainty was primarily applied to benefit, behavioral, and epidemiological parameters (Appendix 3). Random samples were generated using inverse cumulative distribution functions in Microsoft Excel over 1000 Monte Carlo iterations. Model outputs were summarized using descriptive statistics and visualized through histograms to characterize uncertainty.
Results
Costs of screening
Table 1 presents the annual cost structure of the screening program by service delivery level and the corresponding projected financial requirement for rural areas. Costs are disaggregated into capital and recurrent components to reflect the operational design of the program. At the union level, which represents the primary platform for screening delivery, the estimated annual cost per unit is US$12,692, with recurrent expenditures accounting for the majority of total costs. Staffing constitutes the dominant cost driver, reflecting the labor-intensive nature of community-based screening delivered through existing health infrastructure. In contrast, capital requirements are limited since CCs are already established. When scaled to all 4596 unions, union-level activities are expected to account for US$58.33 million per year.
Annual cost structure by service delivery level and projected rural financial requirement of the screening program.a, d
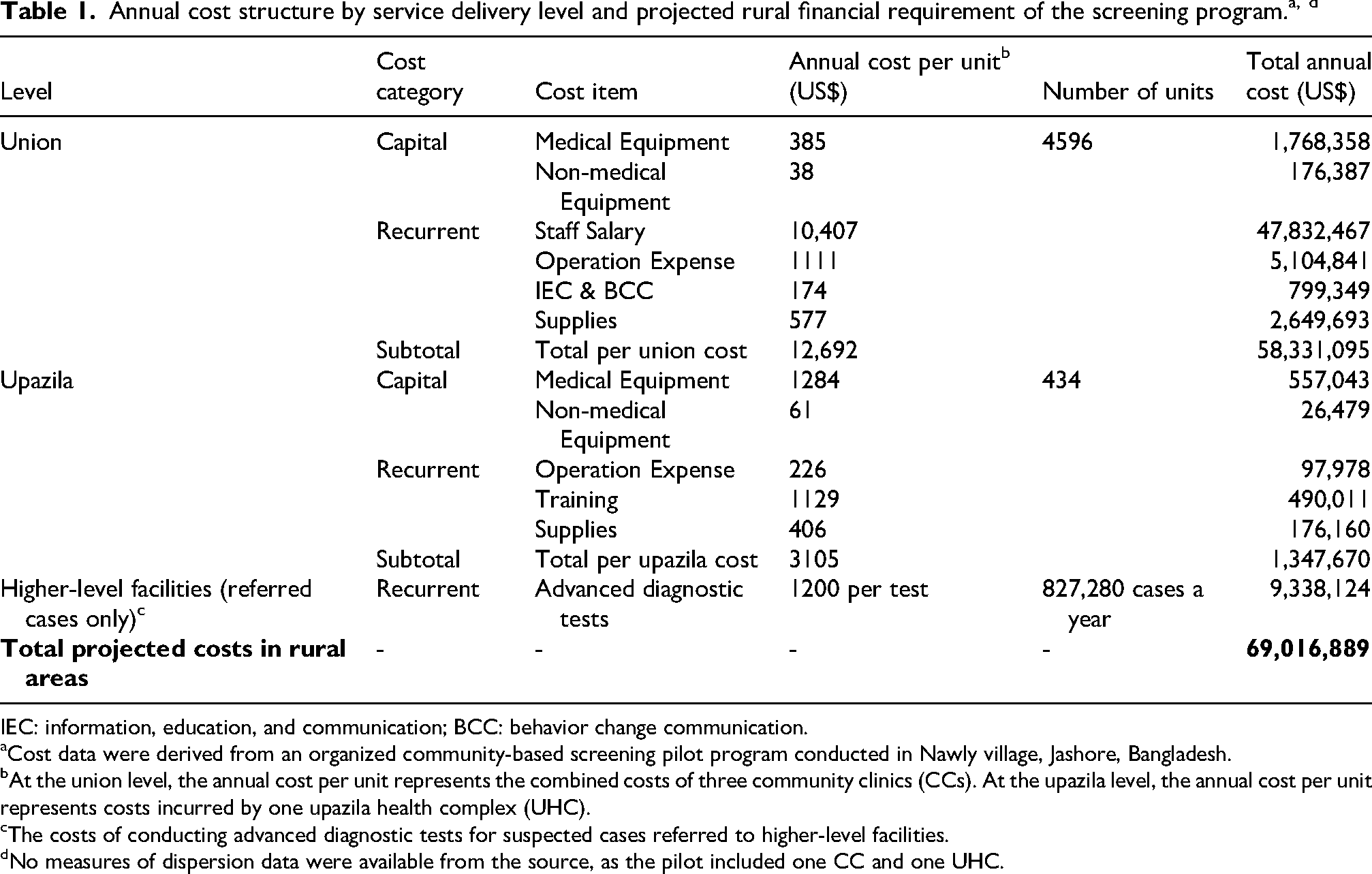
IEC: information, education, and communication; BCC: behavior change communication.
Cost data were derived from an organized community-based screening pilot program conducted in Nawly village, Jashore, Bangladesh.
At the union level, the annual cost per unit represents the combined costs of three community clinics (CCs). At the upazila level, the annual cost per unit represents costs incurred by one upazila health complex (UHC).
The costs of conducting advanced diagnostic tests for suspected cases referred to higher-level facilities.
No measures of dispersion data were available from the source, as the pilot included one CC and one UHC.
At the upazila level, which functions as the first referral tier, the annual cost per UHC is estimated at US$3105. Across 434 UHCs, this corresponds to a total annual rural cost of US$1.35 million (Table 1). Compared with union-level screening, upazila-level costs are estimated to be lower due to the smaller number of facilities and a narrower service scope, with equipment purchase and training activities emerging as the principal cost drivers at this level. In addition to primary and secondary screening costs, advanced diagnostic testing of referred cases at higher-level facilities is expected to account for US$9.34 million annually, based on projected referral volumes.
Overall, the total projected annual cost of the screening program in rural areas is US$69.02 million, with union-level service delivery emerging as the principal cost driver, followed by referral diagnostics and upazila-level services.
Benefits of screening
Table 2 summarizes the estimated per-case benefits of screening through the avoidance of advanced-stage cancer and the resulting projected annual benefits in rural areas. At the per-case level, the total cost saving associated with averting an advanced-stage diagnosis amounts to US$12,066 for oral cancer, US$8911 for breast cancer, and US$11,938 for cervical cancer. These savings are driven by a combination of reduced direct medical costs, averted income loss for patients and caregivers, and intangible benefits related to avoided pain and suffering.
Average per-case benefit and projected annual benefit in rural areas from the screening program (US$).a
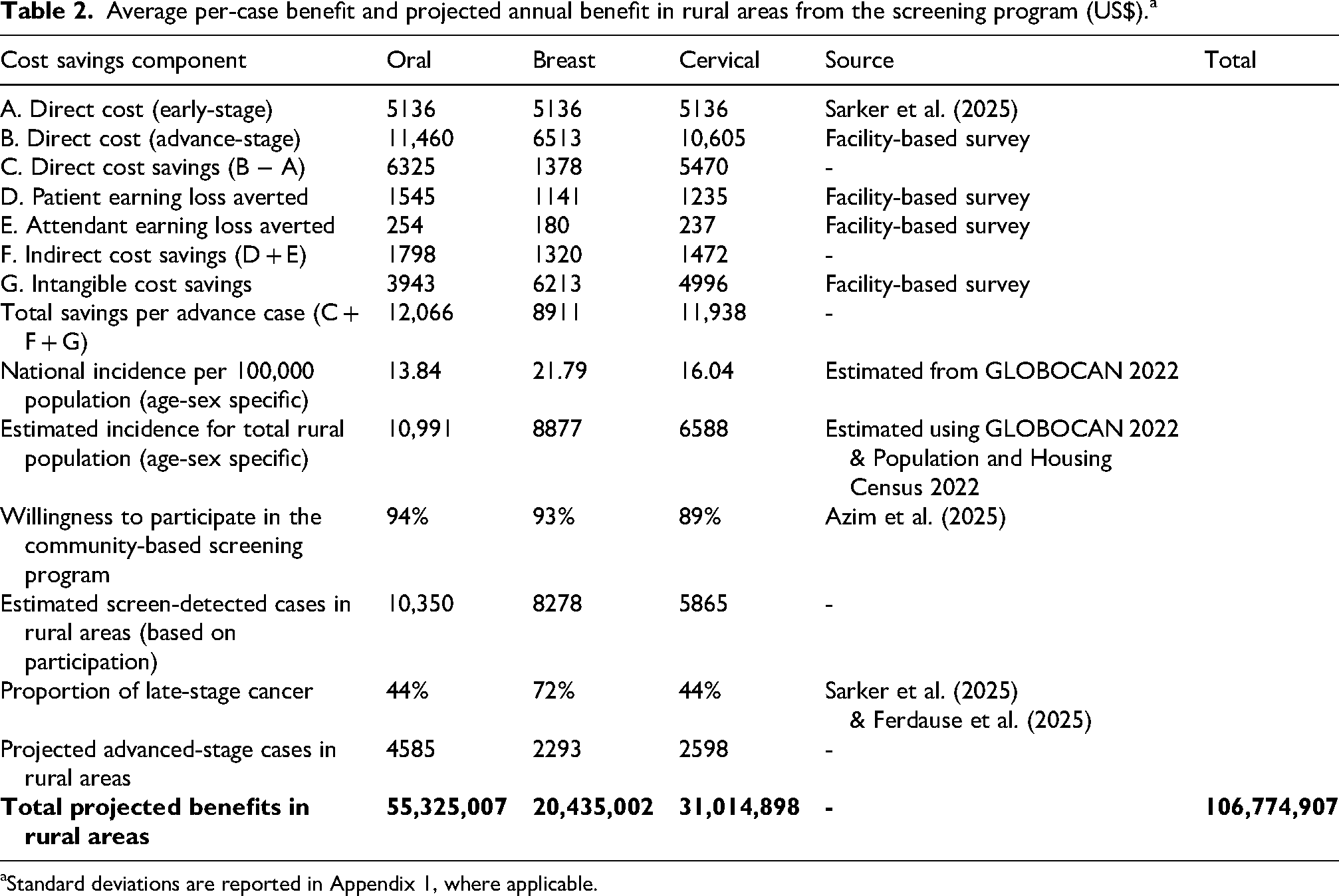
Standard deviations are reported in Appendix 1, where applicable.
Direct cost savings are highest for oral cancer and lowest for breast cancer, reflecting larger differences between early- and advanced-stage treatment costs. Indirect cost savings are highest for oral cancer and lowest for breast cancer. In contrast, intangible cost savings are highest for breast cancer and lowest for oral cancer, reflecting differences in the valuation of psychological distress across cancer types.
To estimate population-level benefits, these per-case savings were extrapolated to rural areas using a multi-step process. Age- and sex-specific incidence rates were first applied to the rural at-risk population to estimate expected cancer cases, which were then adjusted for screening participation rates (89–94%) to derive the number of screen-detected cases. Using the observed proportions of late-stage disease among detected cases, screening is expected to prevent approximately 4585 advanced-stage oral cancer cases, 2293 breast cancer cases, and 2598 cervical cancer cases annually. These estimates were multiplied by the corresponding per-case savings to calculate total annual benefits (Appendix 1 and online Supplemental Material, pp. 4–5).
Based on this extrapolation, the screening program is projected to yield annual benefits of US$55.33 million for oral cancer, US$20.44 million for breast cancer, and US$31.01 million for cervical cancer, resulting in a combined annual benefit of US$106.77 million in rural settings.
Cost–benefit results and sensitivity analysis
The CBA results are summarized in Table 3. The screening program is expected to generate total annual benefits of US$106.77 million, compared with total annual costs of US$69.02 million, yielding a BCR of 1.55. This indicates that the economic benefits of screening exceeded program costs by approximately 55%. In absolute terms, the program is expected to produce an estimated net annual benefit of US$37.76 million.
Cost

The tornado diagram indicates that the proportion of late-stage cancer cases exerts the greatest influence on the BCR, followed by cancer incidence per 100,000 population and the cost of screening per union (Figure 3). A 20% decrease in the proportion of late-stage cancers reduces the BCR by approximately 54%, whereas a 20% increase raises the BCR by 72%, highlighting the central role of stage shift in determining program value. Variations in cancer incidence and screening participation also have a moderate effect on the BCR, while changes in direct, indirect, and intangible cost savings produce smaller but directionally consistent impacts. The BCR remained above 1, ranging from 1.01 to 2.27 across all one-way sensitivity scenarios (Appendix 2).
The histogram of probabilistic sensitivity analysis results (Figure 4) indicates that most simulated BCR values are concentrated around the central estimate (mean: 1.55; median: 1.52). The 95% credible interval ranged from 1.05 to 2.29, with only a small proportion of simulations falling below unity (minimum: 0.78). The probability of BCR > 1 was 98.9%. The distribution exhibited moderate dispersion (SD: 0.31) with an upper tail approaching 3.0, indicating robust cost–benefit performance under uncertainty (Supplemental Material, Table S14).
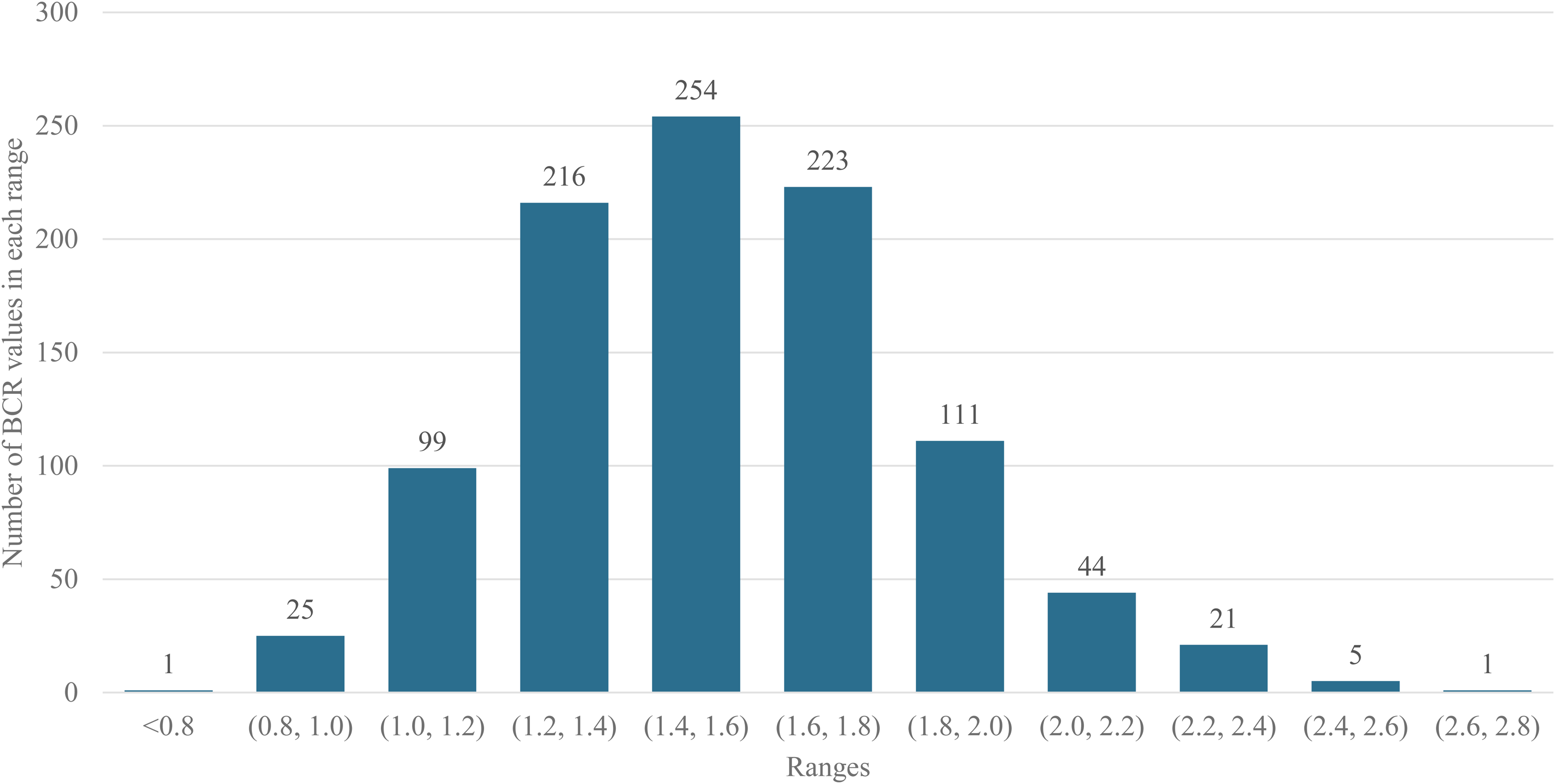
Histogram of probabilistic sensitivity analysis results showing uncertainty in the benefit–cost ratio (BCR) estimates.
Discussion
This study identifies three key findings. First, an organized community-based screening program for oral, breast, and cervical cancers in rural Bangladesh is economically favorable, generating a BCR of 1.55. Second, per-case economic returns are particularly high for oral and cervical cancers, driven by large differentials between early- and advanced-stage treatment costs. Third, the costs of the rural-focused screening strategy are dominated by recurrent staffing expenditures rather than capital investment.
It is important to interpret the estimated BCR of 1.55 in light of the analytical perspective adopted in this study. The CBA was conducted primarily from a household perspective. As a result, the estimated BCR represents a conservative lower-bound estimate of the program's economic value. Inclusion of additional benefit dimensions from broader perspectives, such as productivity gains accruing to employers, cost savings to the health system through reduced demand for advanced care, fiscal benefits to government through preserved labor supply, and wider societal welfare gains, would be expected to substantially increase the overall return on investment. Given existing resource and data limitations, the present analysis provides a baseline foundation for economic evaluation of cancer screening programs in Bangladesh. Future studies incorporating multi-sectoral and longer-term benefits are likely to demonstrate substantially higher returns and further strengthen the case for adopting organized community-based cancer screening at scale.
The existing economic evaluation literature also provides strong evidence that organized breast and cervical cancer screening programs are cost-effective. In high-income settings such as Hong Kong and Austria, organized screening has been shown to be more cost-effective than opportunistic programs.20,22 However, economic evaluations of organized screening programs in LMICs remain limited. A multi-center study from China assessing a government-organized cervical cancer screening program found a significant reduction in economic burden, driven by earlier-stage diagnosis, a finding that is consistent with the mechanisms underpinning the cost–benefit gains observed in our study. 36 Similarly, a study from Brazil evaluating an organized breast cancer screening program found the program to be cost-effective, particularly in regions with high breast cancer incidence. 37 This finding is consistent with our results, which indicate that the economic returns of organized screening are sensitive to underlying cancer incidence and the proportion of late-stage cases. In this context, prioritizing implementation in rural areas, where disease burden and late-stage presentation are comparatively higher, represents an appropriate and economically efficient strategy for program initiation.
Our findings have important implications for cancer control policy in Bangladesh. Despite long-standing national strategies and action plans, cancer screening in Bangladesh remains predominantly opportunistic, fragmented, and characterized by low population coverage. This study indicates that transitioning from opportunistic to organized screening is likely to be economically justified. Given the concentration of disease burden and late-stage presentation in rural areas, prioritizing rural implementation represents an economically efficient and equity-enhancing strategy.17,27 In addition, the proposed program leverages existing primary healthcare infrastructure, particularly the extensive CC network in rural areas, thereby minimizing capital investment requirements. Importantly, the inclusion of oral cancer screening extends economic evaluation evidence to a cancer type that imposes a substantial burden yet has been largely absent from prior analyses of organized screening in LMICs. In Bangladesh, OVE can be readily integrated into existing screening programs with minimal additional resource requirements, while targeting a cancer with the second highest annual incidence in the country. 7
Although grounded in the context of Bangladesh, these findings are relevant for other LMICs with comparable primary healthcare platforms and similar cancer epidemiology, particularly those relying on opportunistic screening approaches. Many South Asian countries currently depend on opportunistic screening for oral, breast, and cervical cancers and continue to experience low population coverage.38–40 In these contexts, the absence of robust economic evidence has, to some extent, constrained large-scale investments in organized screening approaches. In this regard, our analytical framework, particularly the integration of community-based delivery platforms, incidence-based benefit extrapolation, and sensitivity analysis, offers a transferable model for evaluating organized screening programs in similar resource-constrained settings.
Limitations of the study
This study has several limitations. Direct costs for early-stage cancers (stages I and II) were drawn from a single study rather than our facility-based survey, which may limit contextual relevance. However, the source study also employed a multi-centered cross-sectional design across multiple districts in Bangladesh, providing a broadly comparable empirical basis.
In addition, benefits were estimated primarily from a household perspective, focusing on OOP expenditures. Provider-side cost savings were not included due to the limited availability of reliable cost data from public facilities, which may lead to an underestimation of overall societal benefits. The analysis captures only short-term, observable benefits and excludes longer-term productivity gains, and mortality reductions associated with earlier detection, indicating that the estimated BCR likely represents a conservative lower-bound estimate of the program's true economic value. Furthermore, the analysis is based on an incidence-based framework and does not employ a formal decision-analytic model. As a result, the estimates do not explicitly capture disease progression, recurrence, or survival over time. The approach may lead to over- or under-estimation of total costs and benefits compared with lifetime modeling.
The model assumes that a proportion of cases shift from late-stage to early-stage diagnosis based on observed stage distribution and screening participation. It does not account for residual late-stage diagnoses among screened individuals due to factors such as test sensitivity, incomplete follow-up, or disease progression, which may lead to an overestimation of benefits.
Additional limitations relate to data and modeling assumptions. Due to the lack of early-stage patient cost data, indirect and intangible benefits were treated as full savings rather than differences between disease stages, which may overestimate benefits associated with early detection. The program costs were based on a single pilot program implemented in one CC and then extrapolated using standardized unit costs at CCs and UHCs, which may have led to oversimplification of underlying geographic, epidemiological, and health-system variation. Finally, cost parameters were not varied in the probabilistic sensitivity analysis, as they were based on a single pilot program, and no data on variability were available to define distributions.
Despite these limitations, the findings provide important policy-relevant evidence by demonstrating the economic feasibility of organized community-based cancer screening in a resource-constrained setting and by offering an implementable model for program delivery in Bangladesh and comparable LMICs. Beyond its policy relevance, the study also generates baseline empirical evidence that can serve as a foundation for future academic work on the economic evaluation of organized cancer screening programs in similar settings.
Supplemental Material
sj-docx-1-msc-10.1177_09691413261458098 - Supplemental material for Cost–benefit analysis of an organized community-based multi-cancer screening program in Bangladesh
Supplemental material, sj-docx-1-msc-10.1177_09691413261458098 for Cost–benefit analysis of an organized community-based multi-cancer screening program in Bangladesh by Md. Ragaul Azim, Quazi Nazmus Sakib, Md. Mahfujur Rahman, Md. Sirajul Islam, Md. Habibullah Talukder and Syed Abdul Hamid in Journal of Medical Screening
Footnotes
Acknowledgements
We received primary data on the cost of the screening program from a pilot project on implementing organized community-based screening for cervical, breast, and oral cancer in Bangladesh, which was funded by SingHealth Duke-NUS Global Health Institute (SDGHI), under their Global Health Pilot Grant.
ORCID iDs
Ethical approval
The Institutional Review Board of the Institute of Health Economics (IHE-IRB) granted ethical approval for this study (Reference: IHE/IRB/DU/55/2023/Final) on 4 November 2023. Data were collected in accordance with the regulations (i.e. the Declaration of Helsinki) designed to protect human subjects.
Consent to participate
Written or verbal informed consent to participate in the study was obtained from all participants prior to data collection.
Consent for publication
Informed consent for publication was obtained from the participants or, where applicable, from a legally authorized representative.
Author contributions
Md. Ragaul Azim: conceptualization, data curation, investigation, methodology, project administration, resources, validation, writing—review & editing. Quazi Nazmus Sakib: conceptualization, formal analysis, investigation, methodology, software, validation, visualization, writing—original draft, writing—review & editing. Md. Mahfujur Rahman: data curation, project administration, resources, writing—review & editing. Md. Sirajul Islam: data curation, project administration, resources, software, writing—review & editing. Md. Habibullah Talukder: conceptualization, project administration, resources, supervision, validation, writing—review & editing. Syed Abdul Hamid: funding acquisition, project administration, resources, supervision, validation, writing—review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received funding in the form of a grant (3/73659) by the University Grant Commission (UGC), Bangladesh.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data are available upon considerable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix 1. Parameter table.
|
|
|
|
|
|
|
|---|---|---|---|---|---|
|
|
|||||
| National Oral cancer new cases—Annual | 16,083 | No data | 2022 | Population factsheets, Cancer Today, IARC, WHO 7 | |
| National Breast cancer new cases—Annual | 12,989 | No data | 2022 | Population factsheets, Cancer Today, IARC, WHO | |
| National Cervical cancer new cases—Annual | 9640 | No data | 2022 | Population factsheets, Cancer Today, IARC, WHO | |
| Age Distribution of Oral cancer patients in Bangladesh | 15–80 years | NA | 2023 | Facility-based cancer patient survey | |
| Age Distribution of Breast cancer patients in Bangladesh | 15–80 years | NA | 2023 | Facility-based cancer patient survey | |
| Age Distribution of Cervical cancer patients in Bangladesh | 15–85 years | NA | 2023 | Facility-based cancer patient survey | |
| Percentage of oral cancer cases in the age group 30–59 years | 53.03% | [40.82–64.88%] | 2023 | Facility-based cancer patient survey | |
| Percentage of breast cancer cases in the age group 30–59 years | 71.86% | [64.51–78.20%] | 2023 | Facility-based cancer patient survey | |
| Percentage of cervical cancer cases in the age group 30–59 years | 67.26% | [58.00–75.34%] | 2023 | Facility-based cancer patient survey | |
| National population | 165,158,616 | NA | 2022 | Population and Housing Census 17 | |
| National population distribution by age and gender | - | 2022 | Calculated from Population and Housing Census (See Table S15, Supplementary Material, for detailed population distribution) | ||
| Percentage of urban population | 31.66% | NA | 2022 | Population and Housing Census | |
| Percentage of rural population | 68.34% | NA | 2022 | Population and Housing Census | |
| Total rural population (15 + years) | 80,583,747 | NA | 2022 | Population and Housing Census | |
| Total rural population (15 + years)—Female | 41,361,875 | NA | 2022 | Population and Housing Census | |
| Rural population aged between 15 and 80 years | 79,407,679 | NA | 2022 | Calculated from Population and Housing Census | To calculate rural at-risk population for oral cancer |
| Rural female Population aged between 15 and 80 years | 40,741,263 | NA | 2022 | Calculated from Population and Housing Census | To calculate rural at-risk population for breast cancer |
| Rural female Population aged between 15 and 80 years | 41,067,467 | NA | 2022 | Calculated from Population and Housing Census | To calculate rural at-risk population for cervical cancer |
| Willingness to participate in community-based screening in rural area for Oral cancer | 94.17% | 92.57–95.51% | 2024 | Azim et al. (2025) 30 | |
| Willingness to participate in community-based screening in rural area for Breast cancer | 93.26% | 90.78–94.06% | 2024 | Azim et al. (2025) | |
| Willingness to participate in community-based screening in rural area for Cervical cancer | 89.02% | 86.85–90.75% | 2024 | Azim et al. (2025) | |
| Average annual direct costs of early-stage cancer patients | US$5136 | $4117 |
2025 | Sarker et al. (2025) 9 | See section 2.3, “Calculations of direct benefits”, of Supplemental Material (online only) |
| Average annual direct costs of advance-stage cancer patients—Oral | $11,460 | $34,449 |
2023 | Facility-based cancer patient survey | |
| Average annual direct costs of advance-stage cancer patients—Breast | $6513 | $6958 |
2023 | Facility-based cancer patient survey | |
| Average annual direct costs of advance-stage cancer patients—Cervical | $10,605 | $18,707 |
2023 | Facility-based cancer patient survey | |
| Average patients patient earning loss averted—Oral | $1545 | $935 |
2023 | Facility-based cancer patient survey | |
| Average patients patient earning loss averted—Breast | $1141 | $790 |
2023 | Facility-based cancer patient survey | |
| Average patients patient earning loss averted—Cervical | $1235 | $779 |
2023 | Facility-based cancer patient survey | |
| Average attendant earning loss averted—Oral | 254 | $443 |
2023 | Facility-based cancer patient survey | |
| Average attendant earning loss averted—Breast | 180 | $365 |
2023 | Facility-based cancer patient survey | |
| Average attendant earning loss averted—Cervical | 237 | $350 |
2023 | Facility-based cancer patient survey | |
| Average intangible cost savings—Oral | 3943 | $5811 |
2023 | Facility-based cancer patient survey | |
| Average intangible cost savings—Breast | 6213 | $8794 |
2023 | Facility-based cancer patient survey | |
| Average intangible cost savings—Cervical | 4996 | $7903 |
2023 | Facility-based cancer patient survey | |
| Percentage of early-stage oral and cervical cancer patients in Bangladesh | 55.70% | 51.05–60.43% | 2023 | Sarker et al. (2025) | See section 2.3, “Calculations of direct benefits”, of Suppl. Material |
| Percentage of advanced-stage oral and cervical cancer patients in Bangladesh | 44.30% | 39.57–48.95% | 2023 | Sarker et al. (2025) | See section 2.3, “Calculations of direct benefits”, of Suppl. Material |
| Percentage of early-stage breast cancer patients in Bangladesh | 72.30% | No data | 2023 | Ferdause et al. (2025) 32 | |
| Percentage of advanced-stage breast cancer patients in Bangladesh | 27.70% | No data | 2023 | Ferdause et al. (2025) | |
| Official exchange rate—USD to BDT | 106.31 | 2023 | World Bank Data 41 | ||
|
|
|||||
| Number of community clinics (CCs) | 14,377 | NA | 2025 | DGHS Facility Registry 29 | |
| Number of upazila health complexes (UHCs) | 437 | NA | 2025 | DGHS Facility Registry | |
| Number of unions | 4596 | NA | 2022 | Population and Housing Census | |
| List of medical equipment for screening (CC & UHC) | - | 2023 | Pilot program | ||
| List of non-medical equipment (CC & UHC) | - | 2023 | Pilot program | ||
| List of supplies (CC & UHC) | - | 2023 | Pilot program | ||
| Operational expenditure (CC & UHC) | - | 2023 | Pilot program | ||
| Cost of IEC & BCC (CC & UHC) | - | 2023 | Pilot program | ||
| Amount and unit cost of supplies and equipment | - | 2023 | Pilot program | ||
| List of personnel (per union) | Nurse (× 1) Nurse assistant (× 1) Registration booth assistant (× 3) Volunteer (× 6) | 2023 | Pilot program | ||
| Monthly salaries/incentives | - | - |
1. Bangladesh National Pay Scale 2015 2. Pilot program |
Nurse (Grade 10) Nurse Assistant (Grade 13) |
|
| Annual training costs | $1129 | NA | - | Expert opinion | |
| Referred cases per month from CC to higher-level facilities | 5 | NA | 2023 | Pilot program | |
| Average fee per advanced-diagnostic testing | $11.29 | NA | 2023 | Private sector price | |
| Lifetime of medical and non-medical equipment | - | - | Internet | ||
Appendix 2. One-way sensitivity analysis of the benefit–cost ratio (BCR).
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Common late-stage cancer cases (n) | 6065 | 9476 | 13,646 | 1.01 | 1.55 | 2.27 |
| Combined incidence (per 100,000 population) | 41.34 | 51.67 | 62.01 | 1.26 | 1.55 | 1.89 |
| Cost of screening per union (US$) | 10,153 | 12,692 | 15,230 | 1.86 | 1.55 | 1.32 |
| Screening participation rate (%) | 71 | 89 | 100 | 1.26 | 1.55 | 1.70 |
| Direct cost savings per case (US$) | 3513 | 4391 | 5269 | 1.44 | 1.55 | 1.71 |
| Intangible cost savings per case (US$) | 4041 | 5051 | 6061 | 1.44 | 1.55 | 1.71 |
| Referred cases per month (n) | 1224 | 1530 | 1836 | 1.53 | 1.55 | 1.62 |
| Indirect cost savings per case (US$) | 55,152 | 68,940 | 82,728 | 1.63 | 1.55 | 1.46 |
| Diagnostic test fee at tertiary facility (US$) | 9.03 | 11.29 | 13.55 | 1.59 | 1.55 | 1.51 |
| Exchange rate (BDT per US$) | 85.05 | 106.31 | 127.57 | 1.53 | 1.55 | 1.51 |
| Cost of screening per upazila (US$) | 2484 | 3105 | 3726 | 1.55 | 1.55 | 1.54 |
Low value was defined as a 20% decrease from the base-case value.
High value was defined as a 20% increase from the base-case value.
Appendix 3. Parameter distributions used in the probabilistic sensitivity analysis.
|
|
|
|
|
|
|
|---|---|---|---|---|---|
|
|
|||||
| Willingness to participate—Oral | 0.942 | Azim et al. (2025) | Beta | 927.87 | 57.13 |
| Willingness to participate—Breast | 0.933 | Azim et al. (2025) | Beta | 903.14 | 64.86 |
| Willingness to participate—Cervical | 0.890 | Azim et al. (2025) | Beta | 827.70 | 102.30 |
| Proportion of early-stage cancer—Oral | 0.557 | Sarker et al. (2025) | Beta | 139.81 | 111.19 |
| Proportion of early-stage cancer—Breast | 0.723 | Ferdause et al. (2025) | Beta | 126.53 | 48.48 |
| Proportion of early-stage cancer—Cervical | 0.557 | Sarker et al. (2025) | Beta | 139.81 | 111.19 |
|
|
|||||
| Direct cost, early-stage (all types) | 5135.50 | Sarker et al. (2025) | Gamma | 390.55 | 13.15 |
| Direct cost, advance-stage—Oral | 11,460.20 | Facility-based cancer patient survey | Gamma | 7.30 | 1568.98 |
| Direct cost, advance-stage—Breast | 6513.18 | Facility-based cancer patient survey | Gamma | 146.33 | 44.51 |
| Direct cost, advance-stage—Cervical | 10,605.48 | Facility-based cancer patient survey | Gamma | 36.32 | 292.01 |
| Patient earning loss averted—Oral | 1544.68 | Facility-based cancer patient survey | Gamma | 180.13 | 8.58 |
| Patient earning loss averted—Breast | 1140.60 | Facility-based cancer patient survey | Gamma | 348.12 | 3.28 |
| Patient earning loss averted—Cervical | 1234.68 | Facility-based cancer patient survey | Gamma | 283.87 | 4.35 |
| Attendant earning loss averted—Oral | 253.74 | Facility-based cancer patient survey | Gamma | 21.65 | 11.72 |
| Attendant earning loss averted—Breast | 179.84 | Facility-based cancer patient survey | Gamma | 40.54 | 4.44 |
| Attendant earning loss averted—Cervical | 236.97 | Facility-based cancer patient survey | Gamma | 51.80 | 4.57 |
| Intangible cost savings—Oral | 3942.87 | Facility-based cancer patient survey | Gamma | 30.39 | 129.76 |
| Intangible cost savings—Breast | 6213.33 | Facility-based cancer patient survey | Gamma | 83.37 | 74.53 |
| Intangible cost savings—Cervical | 4996.24 | Facility-based cancer patient survey | Gamma | 45.16 | 110.63 |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.