
Abstract
Background:
The theoretical framework of Jϋrgen Habermas suggests that effective communication requires competent participants with an objective attitude that complies with the rules and worlds designated as objective, social and subjective. This situation determines communicative action, which stimulates the search for mutual understanding and results in a process of interaction that promotes self-determination.
Objectives:
In this study, the discharge letters of patients with myocardial infarction were explored regarding the provision of information. The patient’s right to information and the duty of informing were analysed according to the perspective of Jϋrgen Habermas.
Research design:
This was a cross-sectional analysis (from a broader longitudinal study) of all discharge letters that were directly related to nursing interventions regarding the provision of information to 106 patients. In this major study, the difficulties faced by patients who experienced a myocardial infarction and the changes in their lifestyles were analysed based on the type of information received.
Ethical considerations:
The hospital Ethics Committee approved the study, which complied with ethical principles and required informed consent.
Findings:
In the nursing letters, interventions related to the provision of information were conducted at an average of 3.59 interventions per patient. For 8.5% of the patients, however, no interventions related to the provision of information were performed. The most common area of information during hospitalisation was related to the management of signs and symptoms and applied to 90.6% patients.
Discussion:
The nursing interventions did not cover patient education, transition processes or awareness of the disease. Thus, the right to information can be questioned.
Conclusion:
Information is a right, and communication is extremely important. Health professionals should be aware of this importance regarding both care management and the satisfaction guarantee. The sharing of information by health professionals based on their competency is essential for patients to exercise their right to self-determination and decision-making.
Keywords
Introduction
Cardiovascular diseases are a cause for serious concern due to their extremely high mortality and morbidity 1 and their association with common lifestyle choices, resulting in a high cost for individuals and the community. 2 Health systems and people are affected by the sequence of events related to the adoption of unhealthy lifestyles, the development of illness and a lack of adequate treatment for these diseases, which lead to losses at the personal, family and labour levels. 3,4 Providing information and facilitating awareness about cardiovascular disease and the importance of proper treatment to prevent the above-mentioned consequences are essential. 5,6
Information and its provision are essential elements in this dynamic because information is widely disseminated through multiple communication systems. Additionally, patients have the right to be informed about several aspects of their disease to be competent at self-determination and to be able to make decisions accordingly.
Based on these concerns, this article explores the right of cardiac patients to information about managing their disease by considering the theoretical framework of Habermas.
Background
Hospitalisation for acute events, such as myocardial infarctions, often leaves patients vulnerable. The entire hospitalisation process, from patient admission to discharge, reveals the importance of helping patients navigate the resulting challenges. The clinical discharge process and the information that is provided to the patient are essential in supporting this complex process. 7,8
Based on evidence from previous studies, difficulties in terms of patients’ return to home life after discharge reveal a lack of adaptation that often results in re-hospitalisation. 9,10 One of the studied factors is the existence of an information gap between the patient and the health professional throughout the hospitalisation process. Thus, it is crucial to determine what type of information is needed by patients (based on their specific disease) and what information is actually provided. 11,12
The Constitution of the Republic of Portugal establishes the right to health protection, and the Portuguese State promotes and protects citizens’ health and moderates the needs of healthcare consumers. 13
The Portuguese Health System and patient rights have encountered difficulties due to the economic recession. The financial crisis has led to austerity policies that have affected the social and healthcare domains. Some of these healthcare budget cuts influence health professionals’ practices 14 as well as some patient rights, such as the right to information. Nevertheless, health professionals are working to maintain the standards of good practice described in their deontological codes and in the ‘Laws of the National Health System’. 15
In this context, the ‘Charter of Rights and Duties of Patients’ represents the importance of dignity in healthcare, where these principles are extended to all citizens to achieve continuous improvement of services. Thus, the citizen is the central figure of the National Health System (NHS). It is important to reaffirm the citizen’s rights, such as the right to human dignity and integrity, and to simultaneously protect his right of self-determination. To achieve this goal, there must be a good relationship between patients and healthcare providers that encourages the active participation of the patient. Thus, this document details the patient’s right to receive appropriate care for his health status and the right to be informed of the available health services. Moreover, the patient has the right to choose not be informed of his health status and to indicate who can receive information about his continuing healthcare. In turn, it is the patient’s duty to provide all information necessary for correct diagnosis and treatment. Among these duties, the patient should optimise his health status by participating actively in his own health and should cooperate with healthcare professionals by following recommended indications. 16,17
Information is essential for patients to give appropriate consent and to participate actively in their therapeutic choices. The ‘European Charter of Patients’ Rights’ highlights the patient’s right to free choice, the right to consent given all possible access to information and the right to own his clinical information. 18
In Portugal, article 78 and article 84 of the Deontological Code of Nurses 19 state that nursing interventions must be oriented towards freedom and human dignity, and nurses have the duty to inform patients while respecting their self-determination and promoting their right to informed consent. In addition, in articles 31, 44, 45 and 50, the Deontological Code of Physicians 20 states that physicians must respect human dignity and autonomy and must provide clarification of their diagnosis, treatment and prognosis and any necessary information for making informed decisions. Based on these guidelines, there are concepts that govern the process of providing information to the patient related to autonomy, decision-making, self-determination, awareness, dignity and responsibility. 21,22
In the current political system, personal responsibility is a core concept and has instrumental value. People are responsible for the choices they make, and this responsibility promotes proper behaviour. 5 This responsibility is directly applicable to the context of the financial crisis, in which resources are not sufficient and health professionals must guarantee patients’ rights. 23
Fundamental values such as equality and autonomy are often referred to in democratic societies. These values guide rights, freedoms and non-discrimination policies, making it important to develop measures to protect these values. 24 This ideology is adaptable to health systems in which citizens require information to exercise their autonomy responsibly. There must be different commitments between patients, health professionals and their institutions for the responsible practice of human rights, which lead to healthcare regulations that increase social responsibility. 25
In this context, it is helpful to perform an overall analysis based on the theoretical framework of Habermas. This German philosopher and sociologist, who was the successor to the second generation of the Frankfurt School, developed the ‘theory of communicative action’, in which action is a process where the actor is the initiator as well as the product considering the culture and the environment in which he operates. 22,26,27
According to Habermas, modern societies are shaped by human systems (including economic and political systems) and are oriented for success in the life world (the natural habitat of corporate spaces with the goal of understanding, guided by communicative action). 28 The ‘life world’ is part of the concept of communicative action and involves culture, personality and society. 29 The life world reflects their aims in the public sphere of relationships between people and their families but contrasts with the idea of the ‘system’, which includes the political and economic spheres. 30
Habermas’ theory features a person in a being dominated and converted by technology as a result of industrial society at the expense of nature. Thus, technical–scientific developments result in the construction of means to achieve ends. The core of the theory of communicative action promotes the changing of asymmetrical relationships to promote interaction between humans. 27,31 This theory leads to the assumption of a model for oriented action and mutual understanding. Thus, actors need to harmonise their objectives and actions to result in communication. 32 There must be a coordination of actions and consent that is rationally motivated towards common agreement. Although each person has expectations and perspectives, these individual expectations should be consolidated to come to an understanding. 26
As discussed by Habermas, 33 ‘social integration’ underlies norms and values and is a task of people who act communicatively. Therefore, communication is an anchor for coordinating the activities of the participants of interaction networks. Communicative action, 22,34 which is oriented towards understanding the process, corresponds to the validity claims discussed by participants, in which language is central. In communication, participants combine their efforts for mutual understanding based on a system of three worlds (objective, social and subjective). The interaction between them leads to the ‘life world’, which reflects the formation of the processes of understanding. The objective world reflects the sphere of learning and knowledge, where participants extract their interpretations. The social world is where the production and renewal of interpersonal relations is performed. The subjective world includes the manifestation of experiences and self-representation. 27
The practice of self-determination and the exercise of communicative freedom
22,26
are essential in this context. Therefore, taking into account the above factors and the importance of providing information to patients in the context of clinical discharge, the aims of this study are as follows: To explore the frequency and type of nursing interventions described in the discharge letters related to providing information to patients with myocardial infarction; To explore the relationship between the information needs of the patient and the theoretical framework of Jϋrgen Habermas.
Methods
We performed a cross-sectional analysis from a broader longitudinal study to determine the type of information that is provided to patients regarding nursing discharge letters. In the major study, we analysed patients’ perceptions and changes in the lifestyles of patients who experienced a first episode of myocardial infarction in the hospital and at home. Subjects were selected from a convenience sample of patients recruited over 13 months (March 2010 to April 2011) using the following inclusion criteria: first episode of acute myocardial infarction, two or more modifiable cardiovascular risk factors and age between 35 and 64 years. The existence of other chronic diseases (except diabetes), autoimmune diseases and addictions to alcohol and/or psychoactive substances were among the exclusion criteria. In an attempt to study the type of information provided to patients, only native Portuguese patients were recruited. Patients who lived in a foreign country, for whom the influence on changes in lifestyles could not be studied, were excluded.
Based on the major findings of this research 5,35 and given the need to determine the type of information that is provided to patients, a retrospective and descriptive analysis of all nursing discharge letters was performed in relation to nursing interventions that were directly related to the provision of information to the patients. After compiling the list of 106 patients and using the nursing information system, the discharge letters were collected and analysed individually regarding interventions related to the provision of several types of information to patients, including changes in lifestyle, management of signs and symptoms, and medication changes at the self-care level. We tallied the patients who received some type of information and investigated the frequency of the different types of interventions performed.
The data analysis was performed using SPSS version 17 and included a descriptive analysis using absolute and relative frequencies to describe the type of nursing interventions in the provision of information to patients. In addition, the means and standard deviations (SDs) of the interventions were calculated.
Ethical considerations
The study was approved by the Ethics Committee of Centro Hospitalar de S. João, EPE, where the study (project number 93/08) was developed. This study complies with the principles outlined in the Declaration of Helsinki. 36
Results
Based on the analysis performed on the patients’ discharge letters, we found that interventions related to the provision of information were conducted at an average rate of 3.59 interventions (SD = 2.37) per patient, with a minimum of 0 and a maximum of 10 interventions per patient. In 8.5% of the patients (n = 9), no interventions related to the provision of information in any of the domains were performed, as shown in Table 1.
Type and frequency of information provided to the patient, revealed in the nursing discharge letters.
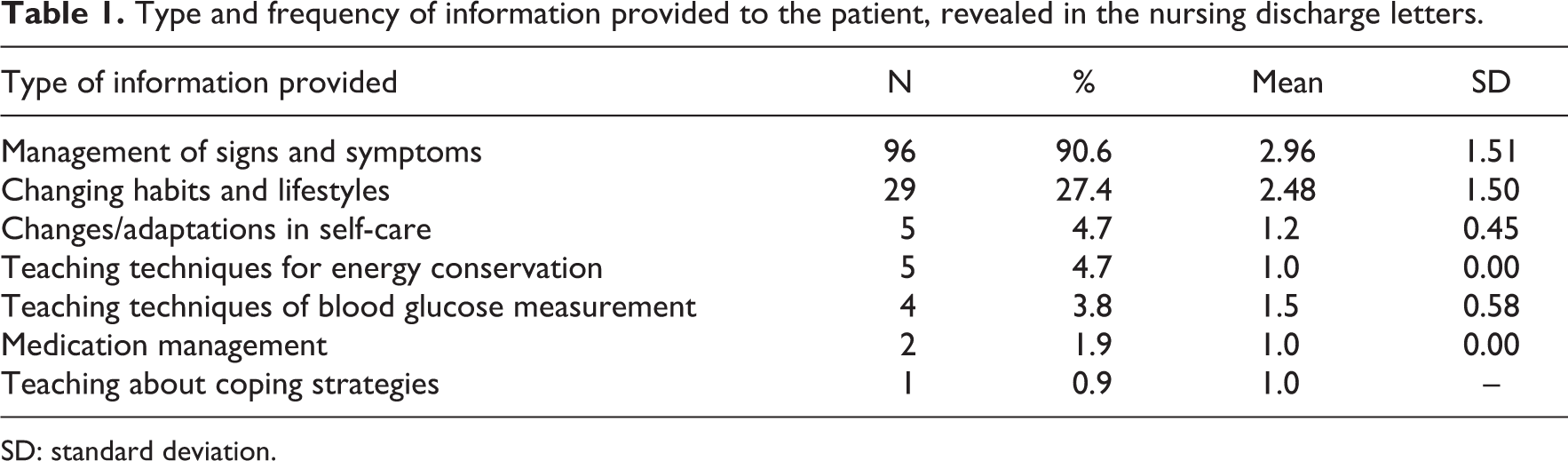
SD: standard deviation.
In the discharge letters of 91.5% (n = 97) of the patients, some type of intervention related to information was performed. Based on this analysis and as shown in Table 1, the information provided to patients during hospitalisation and before discharge in the discharge letter was related to the management of signs and symptoms for 90.6% of patients. For 27.4% (n = 29) of the patients, interventions informing patients about changes in lifestyles were performed. These interventions were related to eating habits, exercise and tobacco use.
Information regarding changes/adaptations in self-care and teaching techniques for energy conservation was provided to 4.7% of the patients. For 3.8% of the patients, the techniques of blood glucose measurement were demonstrated, and advice and guidance regarding the management of medication were provided to 1.9% of the patients. Coping strategies were offered to only 0.9% of the patients.
An analysis of the frequency of different interventions and the different types of information provided to patients showed that an average of 2.96 (SD = 1.51) interventions per patient was performed in relation to the management of signs and symptoms, an average of 2.48 (SD = 1.50) interventions per patient was performed in relation to lifestyle and an average of 1.20 (SD = 0.45) interventions per patient was performed in relation to self-care and changes.
Discussion
Considering the first aim of the study, we verified that 8.5% of the patients did not receive any information. Most information was related to the management of signs and symptoms (90.6%) and interventions associated with lifestyle modification (27.4%). Interventions associated with changes/adaptations to self-care, the teaching of energy conservation techniques and the teaching of coping strategies and medication management were observed at very low percentages and were most likely associated with the type of disease.
Overall, the average number of interventions performed per patient was low and did not cover the entire spectrum of education provided in relation to health education, 3,4 the transition processes for patients 7,11 or disease awareness. 5 According to myocardial infarction guidelines, 37 patients require rehabilitation after discharge to restore their lives and return to work. This process must consider physical, psychological and socio-economic factors and must begin as early as possible. The main aspects of advice and health education that should be provided in this context should address healthy diet, smoking cessation, weight control and exercise. 2,37 Information involving the control of anxiety and other psychological issues is also very important for a health education programme with global coverage.
As mentioned previously, effective communication is essential for discharge planning and health education management. The analysis of data given the set objectives is based on ‘communicative action’ and the relationship between the ‘life world’ and the ‘system’ and on the theoretical framework of Habermas, as demonstrated in the following aim.
Dialogue is important for patients’ decisions. Health professionals must consider the basic requirements of this process, such as communicative competence, equality, self-determination and openness about motives for changing patients’ habits and lifestyles. 32 Talking with patients about their lives and helping them determine their own goals for disease management and consider their own decisions are fundamental. Health professionals must also consider their patients’ practical circumstances, emotions and preferences so that decisions are relevant to individual patients’ lives. Offering information and clarifying the reasons for lifestyle changes is part of a balanced conversation. 22
Considering these issues, questions regarding the way that communication should occur, potential changes in professionals’ positions and patients’ exercise of autonomy and right to be informed are important when reflecting on the ‘theory of communicative action’.
Regarding the second aim of this study, to explore the relationship between the information needs of the patient and the theoretical framework of Jϋrgen Habermas, we believe that this theoretical framework can provide important clues to understanding the discharge process and the need to provide information to the patient. Taking into account the standards of medical paternalism, which has influenced health practices for decades, 38 the curricula of future health professionals have been changing over time. At one time, the curricula prioritised disease at the expense of health. This perspective is evidenced in the theory of Habermas, where educational practices prepare future professionals. 26,27,28
Habermas’ theory of communicative action is based on two main pillars. The first is formal and pragmatic critique based on the analysis of language, and the second is the theory of social modernisation. Much of Habermas’ work as a philosopher focused on the process rationalisation and disenchantment that comes from modern capitalist society. 29
In a democratic society, rights contribute to the integration of individuals and should be available to help individuals participate legitimately. Habermas states that the principle of rights mediates the relationship between the principles of morality and democracy, where human rights are based on the morals and autonomy of individuals. 29,31,39
We can link this design to the hospitalisation of a patient with cardiovascular disease. The patient affected by an acute event suffers some limitations that compromise his reintegration back into society. Due to the peculiarity of this situation and the goal of authentic and effective reintegration into society, health professionals must provide the means for patients become conscious and responsible. 2,37
Habermas stated that the conscious conduct of one’s life can be measured by the possibility of the expression of self-realisation. Therefore, cultural traditions and socialisation processes are implicit in the structures of action guided by understanding. 39 Citizens must exercise their autonomy 29,38 in a system of rights based on a collective understanding and the rational choices of strategies and established purposes. Individually, a person with a moral conscience guides his action with self-determination. The instrumentalisation of citizens as required by communicative action arises from the interaction with the democratic principle because claims are constantly problematised. 39
In the context of health, nurses should develop a plan that is customised and properly articulated with the necessary resources to promote patients’ participation in their treatment in preparation for discharge and home care to achieve patients’ reintegration into society. 2,10,37 For this process to be operational, communicative action is essential because only a well-informed person can make decisions responsibly.
Article 64 of the Portuguese Constitution states, ‘Everyone has the right to protection of health and the duty to promote’. These rights are governed by a set of NHS stipulations, such as ensuring access to healthcare in all areas where management is decentralised and participatory. Similarly, Article 1 of the Universal Declaration of Human Rights states, ‘All human beings are born free and equal in dignity and rights’ and are always ‘endowed with reason and conscience’. 13 Thus, the patient has the right to all available information.
The responsibility for health is becoming an increasingly popular topic in the context of health policies. 5,40 However, the concept continues to be misunderstood in two different aspects identified in the philosophical literature: reactive attitudes and accountability. Three aspects of the application of this concept must be considered: a responsible agent, duties/responsibilities and the susceptibility to be held accountable. However, this application becomes problematic in healthcare, where the concept of responsibility often collides with the concept of autonomy. 40
According to Furger, 41 a bioethics structure that is politically responsible and interested in society respects the right to information by considering citizens in their capacity as full decision-makers. Active and passive information is not only a right of the individual but also a responsibility of institutions and professionals.
Thus, nurses must possess the ability to understand the patient and his level of understanding and competence to receive certain information. 19 There will always be a gap in information, but health professionals should be able to break the barriers of information (such as language and cultural environment) to ensure that patients have the true capacity for decision-making. 42,43
As mentioned, cardiovascular disease is directly linked to lifestyle and culture. 3,4 Thus, patients require a detailed and comprehensive approach in which the management of the disease is a central concept. The patient must be involved in this process.
The concept of disease management as ‘a system of interventions and communications coordinates healthcare for populations with conditions in which self-care efforts are significant’ is supported by many factors. Perhaps the most decisive is the empowerment of the patient for education about and self-management of the disease based on effective information systems between health professionals and patients (with active participation in the exercise of their individuality). 44,45
Therefore, the concept of empowerment reflects increased power that allows individuals to exercise their right of citizenship and to decide based on their authority and capacity. This concept is manifested as a strategy for self-determination in the case of the patient who can promote his own health with proper empowerment, information and knowledge and can decide and act accordingly. 21,46 Empowerment cannot be accessed by outsiders because it comes from within a person. Thus, the health professional is a partner in this dynamic. 47 By promoting change within themselves, patients participate in decision-making by building a relationship of trust and awareness of rights and duties.
Among the key elements of the process of empowerment, access to information provides patients with the ability to exercise their rights. Clinically, the empowerment process involves the perception of control over one’s health status, participation in decision-making and patients’ perceptions of education. 2,10,37
Habermas introduces the term colonisation, suggesting that the life world is colonised by the systemic revealing of modern pathologies. 28 This colonisation by the system affects people who are vulnerable during hospitalisation, making clinical discharge and homecoming a complicated process.
Health education is essential for building an educational project that has roots in the life world. Society is often confined to the prescriptions of technicians who dictate standards for life. The challenge is to implement systemic and instrumental actions that underlie the function of the life world. This interaction leads to dialogue, respect, freedom and an appreciation of culture. 22,28
Health institutions involve a panoply of professionals acting almost individually, leading to the loss of the sense of interdependence and complementarity. It is necessary to return to the previous principles and to review the extent of care to help professionals understand each other and their patients. Another challenge is enhancing the areas of intervention of various professionals and placing them at the service of the patient, returning to the previously mentioned challenge. 22,31,48
For Habermas, the major problem of modernity is the segregation of reason. Communicative reason that takes into account the life world assumes an interrelationship of cognitive interpretations with moral expectations. 49 According to communicative reason, the health professional will interact with the patient and family to link health actions that provide the participants in this dialogue with the capability for mutual and real understanding. 39 Habermas classifies communicative rationality as a synonym for communicative action that involves awareness of what we do and say. 29
We acknowledge the important task of valuing the person in his circumstances, including cultural issues. This means that as health professionals, we must be rational and make others receptive to this rationality by highlighting all of these aspects.
According to Habermas, cultural value spheres are characterised by a continuous and differentiated production of knowledge. Through the process of learning and reflection, we move towards ‘valid universal pretension’. 29,48 Therefore, we return to the previously mentioned concept of the colonisation of the life world, where ethics and aesthetics are suppressed by economic rationality. This colonisation must be avoided in the relationship and communication with the patient because it weakens communicative action. In this formation process and based on a complex network of communicative interactions, the intersubjectivity of the individual is created. Given this assumption, there is a need for at least two participants to understand each other through language. 22,29
We also adapt the notion of understanding and success in the context of health. Through the correct process of language and communicative action, professionals’ duties to the patient regarding technique and treatment can be fulfilled to support various levels of mutual understanding. 22 Based on human action, including the concept of sensitive human activity characterised by Marx, there are two areas, designated work and social interaction. Work is focused on the rationality of science and technology and on organising and choosing means to ends (technical and strategic action). Interaction is guided by the continuous search for knowledge and understanding through language (communicative action). 29 Following this, Habermas states that when subjects establish communication with each other, they consider three worlds present in all interactions, even if disproportionally: the social world of standards, the objective world and the subjective world. The first reveals the condition of things and depends on the success or failure of joint actions, and the second is featured within individuals. 29 According to Habermas, the communication process is highlighted along with an emphasis on inclusion and egalitarianism. Respect for individual dignity and justice issues is supported by the universalism that operates in the public sphere. Through communication, individuals develop moral agency and autonomy. 30
This last question brings us back to the previously cited promotion of self-determination. Analysing studies on the theory of self-determination, we can verify that this theory is a stimulus and support for the autonomy and competence of patients in disease management and improved quality of life. 50
Evidence of the use of this theory suggests improvements to patients’ psychological support, autonomy and competence, which improve patient outcomes and allow the patient the true power of autonomy in decision-making. 43,50 In this context, patients’ autonomy and competence lead to documented gains in mental health (less depression and anxiety) and physical health (not smoking, exercise, glycaemic control and the correct use of medication). 51 Thus, the two types of rationality in communication theory according to Habermas, communicative reason and emancipatory or instrumental strategic thinking, may provide information to patients regarding health education and lifestyle changes.
This strategic action is oriented towards success; it is a purposive-rational action with a utilitarian point of view. In contrast, communicative action is oriented towards understanding and resolving conflicts by mutual agreement. In the former, one participant aims to achieve his own ends. In the latter, there is a harmony of action plans among all participants; this action is most appropriate in the planning phase of clinical discharge.
According to Habermas, the original mode of language is language with guidance for understanding, in which communicative reasoning should prevail. 52 Communicative action that integrates the three worlds is always present in acts of reflective understanding that encompass pure communication and speech that corresponds to the development of a fluid, communicative relationship. 39
In summary, there is a need for a strong communication component during hospitalisation. Based on the results of this study, we have found that this communication does not always happen. When it does, information is almost always directed towards the biomedical model, to the detriment of the person as a bio-psycho-socio-cultural entity.
Through mutual understanding, we can develop actions that allow patients to exercise their autonomy, self-determination and freedom by acting responsibly in the context of society.
To avoid living a ‘life world colonised’, health professionals have, through the political arena, the duty to inform patients about all aspects that might affect them during their hospital stay and beyond. It is necessary to listen to patients to understand and help them with their needs, including disease management and changes or adaptations to self-care (which is essential in the household) that become crucial in the context of cardiovascular diseases.
Conclusion
We are gradually advancing to a more democratic society in which the citizen, who is the holder of rights and duties, tends to not accept impositions on his individuality. The concepts of autonomy and freedom are important, but sometimes these concepts conflict with the concept of responsibility. 5 The right to self-determination reflects the enhancement of the previous concepts in a universe of common good, although there are several actors, each with his own vision. 21,26
The life world can be ‘colonised’ by the energies of the system. Therefore, it is important to understand the ideas and opinions of the people who operate in the public sphere. The risk of keeping these two worlds in conflict is the loss of personal autonomy, resulting in higher passivity and dependence on the system and decreasing the capacity for individual freedom. 30
According to the study results and discussion based on Habermas’ theoretical framework, we can state that the biomedical model is still widely implemented, and the patient is not seen as a complex being within the biological, social, psychological, emotional and cultural scope. The information given to patients is insufficient and is overly oriented towards the management of signs and symptoms. In this situation, healthcare is oriented towards the rapid resolution of problems rather than long-term resolution over time.
It is necessary to take on challenges in health that reflect the search for ethical understanding between health professionals and patients to achieve the reintegration of patients into society and success in the management of care.
Limitations of the study
This study was based on a sample from a larger study, in which we observed some failures in the patient discharge process. Thus, the analysis performed to determine nursing interventions described in the discharge letters of patients is confined to what was recorded. However, it is unclear whether patients were given additional information that was not registered.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Foundation for Science and Technology (grant number SFRH/BD/65777/2009).