
Abstract
Background:
Preparing tomorrow’s healthcare workforce for managing the growing complexity of care places high demands on students, educators, and faculties. In the light of worrying data about study-related stress and burnout, understanding how students manage stressors and develop resilience has been identified as a priority topic of research. In addition to study-related stressors, also moral stressors are known to characterize the students’ first clinical experiences.
Objectives:
However, current debates show that it remains unclear how healthcare ethics education should address them. In order to clarify this issue, this study first develops the notion of moral resilience as a response to moral stressors involving both situations of moral complexity and moral wrongness. Second, it explores the potential of healthcare ethics education in fostering moral resilience. For this purpose, it defines moral resilience operationally as a reduction of moral distress in a given axis of time measured by a validated tool.
Research design, participants, and context:
The educational transferability was assessed within an explorative, quantitative pre–post interventional study with a purposive sample of 166 nursing students. The educational intervention comprised a lecture introducing the typology of moral stressors. Before and after the lecture, students were presented vignettes depicting morally stressful situations.
Ethical considerations:
The competent research ethics committee confirmed that no ethical approval was needed. Informed consent was obtained from participants.
Findings:
Three of four vignettes showed a modest but statistically significant reduction in measured levels of distress after the lecture (p < 0.05, α = 5%).
Discussion:
The study shows the potential of healthcare ethics education in providing students with transformative knowledge that fosters moral resilience.
Conclusion:
In times of global scarcity of educational resources, healthcare ethics education has an important contribution to offer in the promotion of students’ mental and physical health by strengthening the knowledge base of moral resilience. This legitimates its costs for societies, faculties, and professional bodies.
Keywords
Introduction: Right, wrong, and what lies behind them
“The most important lesson I have learned is that there is no right nor wrong when talking about ethics.” With this statement, a nursing student closed the final discussion round of an ethics module within a Master’s program in nursing science, just before the noon break. I was definitely not prepared for it, so I simply nodded my head. However, what is wrong with the student’s answer? Maybe it is not too bad, provided we know the assumptions behind it. Healthcare ethics educators may not be the only ones who experience this kind of classroom talk. What is so special about this setting? A closer look at the literature on healthcare ethics education (HCEE) is revealing: In the last four decades, research in HCEE has been enriched by different lenses and methodologies which are helpful in our case. 1 In what follows, they will be described as the philosophical, the behavioral, and developmental lens.
Moral experts, trustworthy clinicians, or self-reflecting thinkers?
When asked about the essential features of HCEE, educators would most likely first mention objectives within the cognitive domain. 2 Through the philosophical lens, HCEE first unfolds with the identification of clinical problems and philosophical aspects that illuminate the ethical dimension (e.g. ethical theories and concepts, ethical decision-making models) and inform principled ethical reasoning. Following established principles of educational science, educators align these contents with the general curriculum. Whether visible or not, curricular issues already imply considerable ethical choices. They are rooted in different theoretical assumptions about normative ethics and its relationship to clinical practice, metaethics, and the question about what constitutes moral expertise. Nevertheless, this is not the sole lens.
Following the title question of Alastair Campbell et al.’s 3 contribution, “How can we know that ethics education produces ethical doctors?”, measuring how students transform cognitive knowledge into practice can be seen as the highest taxonomical level of possible outcomes of HCEE, provided we could reach a consensus on the question what an ethical doctor or an ethical nurse actually is. Here, the moral behavioral lens builds on the consensus of learning theorists generally defining learning as sustainable and visible behavior modification. 4 HCEE therefore second unfolds by fostering in students those ethical competencies that make them “ethically fit” for practice. 5,6 Worrying evidence is given that poor ethical preparedness is associated with an increased risk of professional misconduct. 7,8 Professionalism expresses and professes that the healthcare professions’ mandate is not only a social or scientific one but also an imminently ethical one.
Third, when considering the moral developmental lens, healthcare ethics educators experience young people living in particular circumstances. Students have to balance not only the intellectual and organizational demands of their studies but also social lives within families and peers, as well as the first clinical experiences. Parallel to their academic studies, they enter the cosmos of the ward as novices. Here, they are progressively socialized into the cultures of healthcare practice, learning that evidence-based knowledge and sound clinical reasoning are not the only driving forces but also gut feeling, intuition, authority, and even abuse of power. They soon become fast learners of the other curriculum, which is informal and hidden, ambivalent, but powerful. 9 At one moment, it submits them to the “brute” laws of the “ward jungle,” at another, it protects and directs them by authentic role models whom they will always remember and try to emulate. From starting as peripheral observers, students become more and more actors within the clinical realm. Patterns of cognitive and practical apprenticeship run parallel to their moral apprenticeship. 10 The latter reflects students’ moral development which is not only seen in terms of assessable cognitive stages or schemes that evaluate moral judgment, 11 but also in terms of psychological, social, and neurobiological determinants of moral functioning. 12 By adopting this lens, HCEE enhances the moral development in students that results from the interaction of knowledge and experience, may the latter be enactive within the patient encounter or vicarious in discussions within peers and educators in the classroom.
Recent research has highlighted the relevance of the three “lenses” in the delivery of HCEE. However, the coexistence of the underlying paradigms leads to considerable variations in contents and teaching formats of HCEE as well as student assessment. At this point, the hesitation in responding to the “not-right-not-wrong” statement in the introductory part can be explained as a tension concerning the “lens” that should be adopted in order to respond to the student in an appropriate way.
It is unlikely that educators think in terms of “lenses” they wear when planning and implementing an ethics curriculum. They may probably bear in mind some kind of vision how their students as future practitioners will hopefully put into practice what they have heard and learned from textbooks, discussions, direct observation, and experience. At a practical level, these tensions highlighted by the three lenses can be typified by three metaphors: Should HCEE “produce” knowledgeable moral experts (the philosophical lens), trustworthy clinicians (the behavioral lens), or self-reflecting thinkers (the developmental lens)? The relevance of this distinction becomes particularly visible in determining how, what, and when to assess HCEE in students.
13
At first sight, the moral expert, trustworthy clinician, and self-reflecting thinker are all justified by the ethical demands of professional practice. Nevertheless, if these models are unstated, combined at random or distributed unequally, they are likely to lead to discrepancies between contents, formats, assessment of student learning, and transferability into practice.
3
Manifestations of such a mismatch reported in the literature are Cognitive overload of students (as risk of the expert model);
14,15
Demands on students that are deemed as excessive or supererogatory (as risks inherent in the trustworthy clinician model);
16,17
Poor confidence in ethical decision-making, false beliefs about the nature of ethics resulting in trivialization (as risks of the self-reflecting thinker model).
15,17,18
Therefore, depending on the “lens” chosen, educators will focus on theoretical problem analysis and moral behavior or make inferences to the moral development. Of importance is that all these conceptualizations have a high degree of intrinsic plausibility. The question, which lens should be the dominating one, has no clear-cut answers. Whereas the majority of authors reasonably propose some combination, the variability of ethics curricula as related to contents, assessment, and reported outcomes 1,19 bears the risk of fragmentation and randomness. The difficulties in establishing which “lens” should be the dominating one are by no means just of theoretical nature, but a threat to the effectiveness of HCEE, as research on students’ confidence in connecting ethics teaching and practice suggests. 17,18 As an attempt to overcome these difficulties, moral resilience is proposed as the unitary “lens” of HCEE which departs from the ethical demands of practice and arranges the other “lenses” around this gravitational focus.
Shifting from the complaint about moral distress to the development of moral resilience
To look at education from the perspective of resilience presupposes a conceptual shift from traditional content orientation to experience orientation. 20 It implicates uncovering the different stressors students experience in the classroom and on the ward. Dealing with complexity—as resulting from the novice status of students in science and practice, but also intrinsic to both science and practice—constitutes a major stressor in students’ lives. 21 Promoting psychological resilience in the light of this stressor asks from educators and mentors to foster in students self-efficacy and self-control, but also to help them in managing learning, overcoming learning resistances, and coping with learning “failures.” 22 In addition to stressors caused by the demands of their studies, students also experience moral stressors. 23 Importantly, both study-related and moral stressors can be ascribed to causal or hermeneutic complexity. 24,25 If psychological resilience has to be strengthened in students in order to help them to manage study-related complexity, then moral resilience helps them in managing moral complexity. Yet, there is a major limitation in trying to “align” psychological and moral resilience which lies in the diversity of the concepts: In general, instruments that measure psychological resilience depart from psychological constructs describing processes, outcomes, or developments of individuals exposed to risk or experiencing adversity. 26,27 The ethical dimension—albeit present—is not specifically addressed. When looking at the typologies of stressors and vulnerabilities that underlie the psychological resilience construct, there are undoubtedly close similarities between moral resilience and psychological resilience. This holds especially true when considering those stressors that involve witnessed or perpetrated moral injury, understood as the psychological outcome of a morally challenging situation (e.g. nursing students witnessing the force-feeding of patients). Nevertheless, for the purposes of education, it is heuristically useful to maintain the distinction of moral stressors—in terms not of an outcome, but of the underlying etiology—as being triggered on the basis of moral intuitions and values or (by referring to Andrew Jameton’s 28 influential definition of moral distress) moral judgments. Given the difficulty in assessing moral resilience directly with the instruments of psychological resilience, moral resilience seems to be best approached indirectly by referring to measurements of moral distress. Unlike psychological distress, moral distress is a construct with an explicit ethical connotation. Nowadays, an impressive body of empirical research is available to address moral distress in nursing, medical, and allied professions as well as in students of both professions. 29 –31 Serious philosophical questions have been raised, marking an important step in the history of this concept. 32 –34 Although moral distress serves as the experiential starting point of HCEE, the critiques addressing the normative validity of this construct must not be ignored. This applies especially to moral distress as already implying a moral judgment in a given situation. From an ethical point of view, it is consistent to define moral distress as “a psychological response to morally challenging situations such as those of moral constraint or moral conflict, or both” (p. 7). 32 Yet, the morally challenging situation is never statically given, but results from an interaction of personal intuitions, values, and norms with a given situation, which may also (but does not have to) give rise to moral judgments. In order to preserve this normative caution, the term “perceived moral distress” (PMD) is advocated here as comprising psychological outcomes based on a specific etiology recalling the moral realm.
Moral resilience can therefore be operationally defined as an outcome based on a change in PMD in a given axis of time. In this line of thinking, the goal of HCEE is to enable students to understand and master the moral stressors they experience in practice 35 or they learn about from the experience of others. This goal is seen as the unifying lens that aligns the three lenses mentioned: HCEE provides those knowledge bases (e.g. moral theories, methods in applied ethics, concepts, history of healthcare ethics), trains those relevant skills (e.g. ethical decision-making, communication), and promotes those attitudes (e.g. truthfulness, confidentiality, self-reflexivity, responsible scholarship) that are needed to reach this goal.
Knowing and not knowing: moral transparence and moral opacity
How to start educational activities within a resilience framework? Most students would presumably not care about different lenses or approaches, but expect some clear-cut solution to the situations they witness in practice. 18
From the author’s experience, the epistemic distinction between morally wrong and morally complex situations offers a good starting point within the context of teaching that allows students to bring in their experiences to the classroom: Both situations, although differing in their normative character, can result in moral distress. Based on this distinction, a first learning objective is that students recognize situations of moral wrongness and name them in terms of malpractice or misbehavior. 15 Morally wrong situations call for a moral response based on professional values, as in the case of a first semester student witnessing an act of bribery by a head nurse while talking with worried relatives. Here, by following acquired ethical orientations and sharing pertinent knowledge, the professional knows the right thing to do and experiences considerable moral distress by not being able to change the course of action. 36 These situations can be considered as “morally transparent,” as they involve a moral judgment and require an ethical argumentation. Despite this transparence, the psychological outcomes are likely to affect the healthcare professional’s well-being negatively. By contrast, students and later professionals may also be exposed to situations in which different moral judgments can be made, implying a genuine uncertainty about which of prima facie equally plausible ethical principles or orientations apply, which may also result in moral distress (e.g. when caring for a patient with mild cognitive impairment who refuses to drink and to eat). Therefore, a second objective is that students recognize such situations of complexity 24 and frame them by means of ethical theories, concepts, and methods that inform ethical reasoning. 15 Here, the professional does not [yet] know the right thing to do and experiences moral distress. Importantly, complexity is person and case specific. It may have originated either through a lack of knowledge, a lack of experience, a novice status in moral reasoning, or through the situation itself entailing different ethical principles and professional duties. These factors hinder a clear-cut solution, as in the case of outdated and unclear advance directives in situations of dementia. Here, the resilience perspective enhances a deepened understanding of such “morally opaque” situations. Rather than creating operational solutions, it enhances moral understanding that paves the way for a careful evaluation of different options. 15 In the teaching context, a morally opaque situation may be transformed into a morally transparent situation through better information, increased orientative knowledge (e.g. about professional values and virtues), skilled reasoning, or a deepened understanding of the circumstances. For example, after the ethics course, the student witnessing bribery feels vindicated and addresses her observation in a confidential talk with her ward preceptor. Conversely, an apparently morally transparent situation may be transformed into a morally opaque situation when the ethical argumentation is proven unstable or resting on false assumptions. For example, a student is claiming that advance directives should be fully respected in the case of a stroke patient she actually cares for. She feels morally distressed when learning that major elective surgery is planned. After the ethics course covering different aspects of patient autonomy and surrogacy, she overcomes her shyness and speaks with the physician in charge. Although she is firmly convinced that advance directives are binding, she shows an understanding for the physician’s doubts as to the validity of the document in the given situation (imprecise formulations, outdated document, and probable reversibility of the clinical symptoms).
Both complexity and wrongness hide moral stressors that are known to have a wide range of adverse outcomes on students, professionals, and patients. Moral resilience as here understood enables students and future practitioners to circumnavigate two “extremes”: The shallows of moral acquiescence on the one hand in “transparent” situations which require a moral response (in terms of recognizing what is morally wrong, but not changing the course of action and tolerating the adverse consequences at a personal and systemic level); The shallows of moral burnout in “opaque” situations that require a deepened understanding (in terms of feeling overwhelmed by the ethical complexity and refraining from making any decision under moral uncertainty at a personal and systemic level).
To start by helping students to make the epistemic distinction between morally wrong and morally complex situations can lead them from not knowing to knowing, but also from pretending to know to not knowing or knowing better. In a developmental perspective, these “shifts” can cause value crises that require a respectful learning climate, as shown in the case of the “not-right-not-wrong” statement. 37 Whatever the direction of learning is, it is transformative and changes the students’ perception not only of the situation, but also of themselves as moral agents perceiving moral distress (or not doing so). The basic assumption is that both “shifts” stand for effective teaching and that such a “reframing” of the situation results in lowered levels of PMD, which is indicative for moral resilience. This assumption is investigated in the next section.
Exploring moral resilience in students
Design
Using an explorative design, this study aims at demonstrating the educational transferability of the moral resilience approach (as operationally defined by a decrease in PMD) in baccalaureate students in nursing science through an educational intervention. The study has been performed with a purposive sample of 166 nursing students distributed on three sites. Before and after the intervention, four hypothetical case vignettes were presented. Levels of moral distress were measured by means of a validated tool, the Moral Distress Thermometer (MDT). 38 The author of the tool granted the permission to use the tool for the purpose of this study. After translation into German by means of back-translation technique, the translated version was pretested. In order to reduce recall bias, students were asked to put the rating sheets in the envelope immediately after completion. Additionally, a baseline measurement (with no vignette) was performed before and after the lecture in order to assess potential situational stress or detect possible effects of habituation.
Ethical considerations
The aims and contents of the study were presented to the Research Ethics Committee of the Canton of Zurich, which confirmed that no formal approval by the Committee was needed. After obtaining permission from the study program directors of the Zurich, Darmstadt and Kalaidos University of Applied Sciences, the study was carried out during a regular lecture of an ethics course given by the author. At the beginning of the lesson, students were given oral and written information about the study. Those who wanted to participate filled out the informed consent form and left it in a separate box. After completion, they put the anonymous survey sheets in a neutral envelope and sealed it. Those who did not want to participate in the study attended the lesson and simply kept the study materials (n = 15 in total). Anonymity, voluntariness, and confidentiality were guaranteed at every stage of data collection and elaboration.
Study conduct and schedule
The study schedule comprised three steps: First, participants were given four case vignettes inspired by former students’ narratives depicting morally stressful situations (Table 1). The vignettes were not presented at once, but consecutively projected by means of a beamer. After reading the vignette, students were asked to fill out the MDT for each individual vignette, imagining that they were in the given situation (MDT1-MDT4). The tool uses a scale from 0 to 10 (with 0 described as “no distress” and 10 the “worst possible”). Second, a lecture of 30 min introduced the distinction between two types of potentially stressful situations that require different strategies and courses of action: situations entailing moral complexity on the one hand and moral wrongness on the other.
15
In a subsequent short discussion, students were encouraged to provide their own examples deriving from their practical experiences on the ward. The vignettes were not invoked at any point of the lecture and discussion. Third, after the short lecture, the same measurement procedure was repeated: After a baseline measurement by means of the tool (MDT5), students were again confronted with the same vignettes and asked to rate their levels of moral distress on the MDT (MDT6–MDT9). After the last measurement, those students wanting to participate sealed the envelope, which was collected during the following break.
Vignettes and measurements of moral distress by means of the MDT.
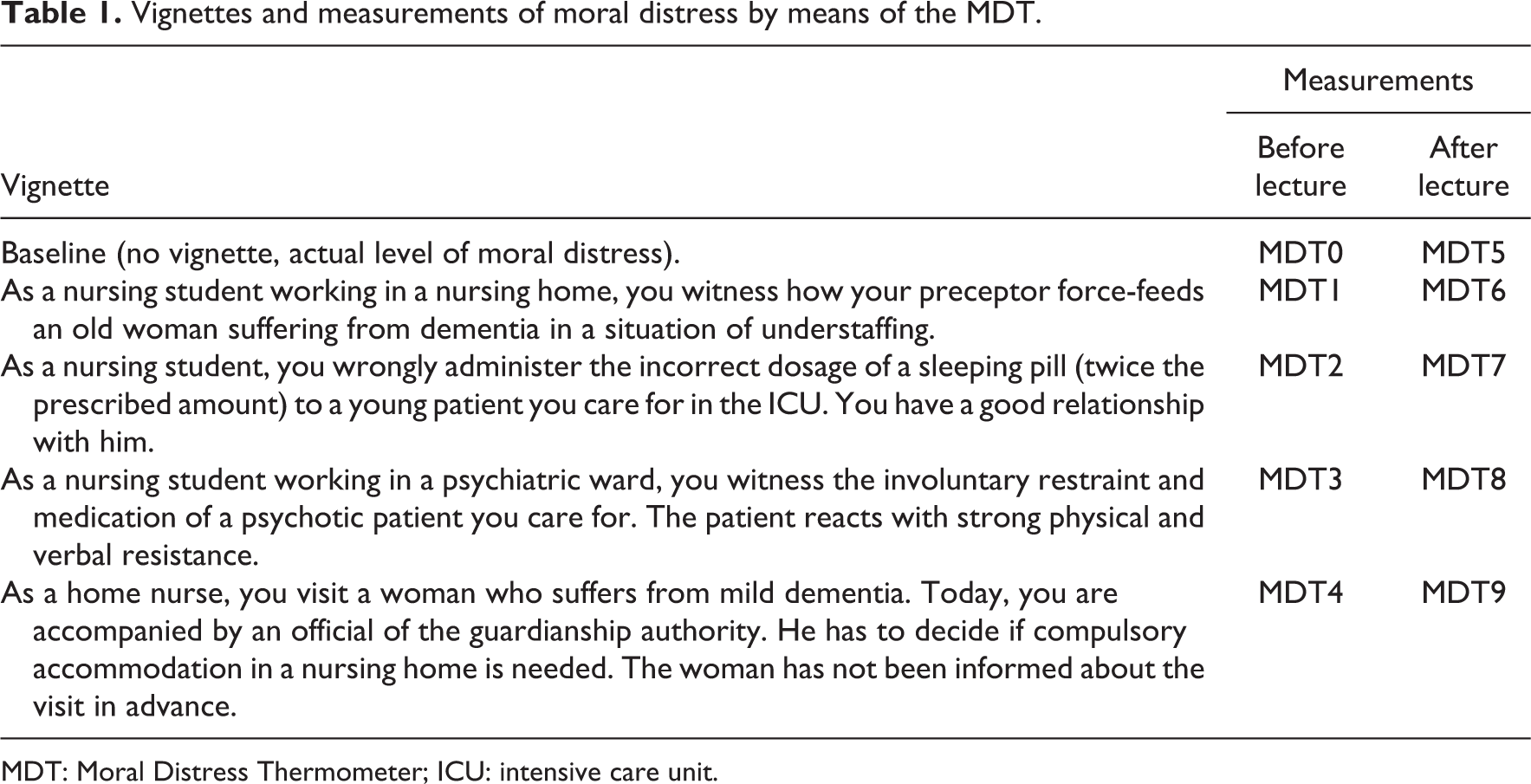
MDT: Moral Distress Thermometer; ICU: intensive care unit.
Data analysis
A total of 166 bachelor students in nursing science participated in the study at three sites. A total of 35 students were enrolled in an extra-occupational program and 131 in a basic education program. One to four data sets per vignette dropped out due to incomplete information. At each site, data were collected by following exactly the same procedure. After collection, SPSS® statistics software for Windows®, version 22 was used for analysis. Due to the non-normal distribution and the dependence of the data, a non-parametric test, the Wilcoxon Two-tailed Ranks Test (α = 5%), was chosen for test statistics. A comparison of means was performed in order to show the significance of the data. The test was performed for each site and vignettes individually. The results of the sites matched as related to the significance with the exception of two vignettes measured in one site, which is attributable to the small size of the local sample (n = 16). The same conformity applies for the basic education and extra-occupational education subgroup. Therefore, the data could be pooled (Table 2).
Descriptive statistics.

SD: standard deviation; MDT: Moral Distress Thermometer.
In three of four vignettes, the data demonstrate a statistically significant decrease in reported levels of moral distress in comparison to the first measurement (MDT1 and MDT6 (p < 0.05); MDT2 and MDT7 (p < 0.05); MDT3 and MDT8 (p < 0.05)). The pair MDT1 and MDT6, which had the most pronounced difference, is illustrated in Figure 1. Although the difference is rather modest in absolute terms, it has to be noticed that the second measurement already took place after a short lecture of 30 min and that a p value of <0.05, which supports significance, emerges in all these pairs. Conversely, no statistically significant difference was given for the fourth pair (MDT4 and MDT9 (p = 0.308)). Also, the baseline measurement with no vignette (M0 and M5) did not show a statistically significant difference between the first and the second measurements (p = 0.409). In addition, these measurements show the lowest levels of distress.
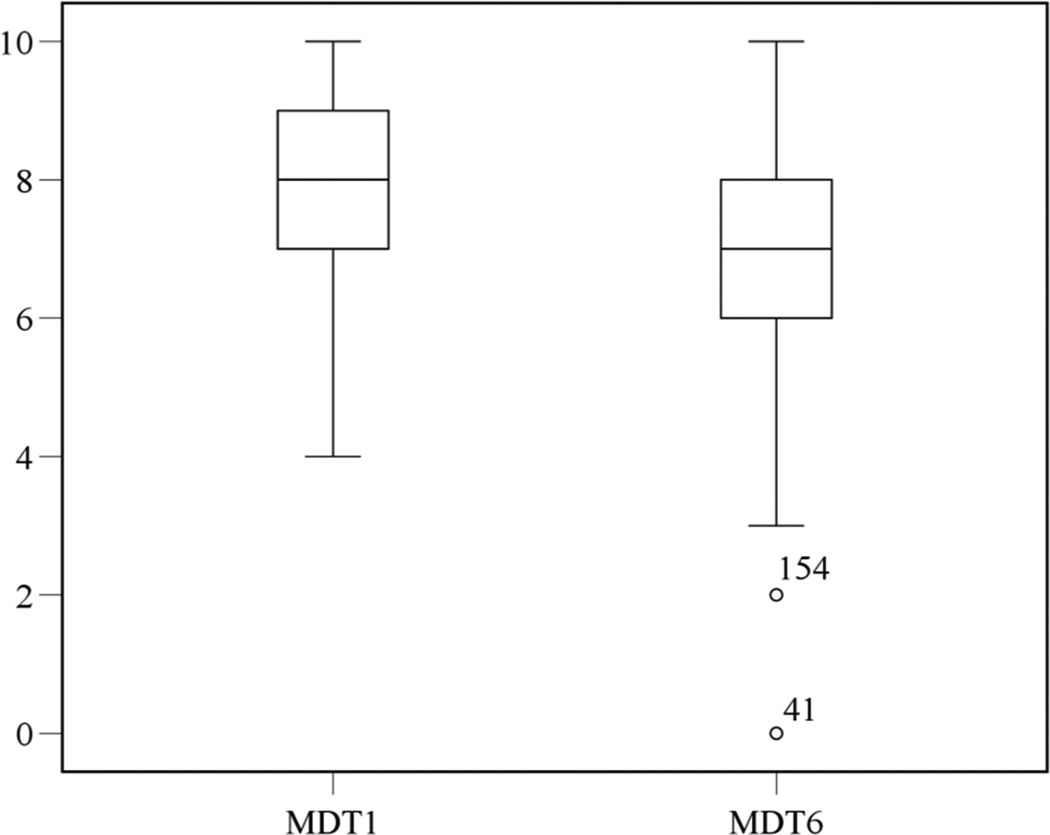
Comparison between MDT1 and MDT6 (boxplots).
Discussion
The study aimed at exploring the educational transferability of fostering moral resilience in the context of ethics teaching by adopting an experimental design consisting of vignettes ratings and an educational intervention. In three of four vignettes, a statistically significant decrease in PMD could be shown. By having the knowledge of how the situations in the vignettes can be understood, students’ locus of control over the situation is enforced, 39 which results in lower levels of PMD. Following the operational definition, this tendency is assumed to indicate moral resilience and basically confirms the feasibility of implementing the chosen approach within HCEE.
The fourth vignette (MDT4 and MDT9) was the only one where the lecture did not show a statistically significant effect. At the same time, the absolute levels of moral distress measured here were the lowest of all the vignettes (MDT0 and MDT5 had lower values, but with no vignette). This can be explained by assuming that this situation was neither morally complex nor morally wrong for the students, but just bearing another problem (e.g. the guardianship authority’s duty to announce the visits of its officers) and presumably causing notable psychological (but not moral) distress. The low baseline measurements before and after the intervention (MDT0 and MDT5) show that an influence of the study setting itself on perceiving distress can be excluded. Both the fourth vignette (MDT4 and MDT9) and the baseline measurements (MDT0 and MDT5) show low levels of moral distress with no statistically relevant differences, which speaks against habituation bias.
Limitations and future research
This study has several limitations. First, like for all empirical studies, statistical significance has to be distinguished from practical relevance. One could, of course, criticize that the PMD levels decreased “only” from 0.8 to 0.5 points on average, even though the difference is statistically significant. But the primary focus was not to measure moral resilience, which would have implied a comprehensive “phenomenology” of moral stressors, but to demonstrate the possibility and feasibility of fostering it within the boundaries of HCEE. This claim has a methodological, conceptual, and instructional dimension. Whereas the methodological dimension addressed the feasibility of the proposed approach, the conceptual one contended that moral resilience can be approached by comparing PMD levels before and after an educational intervention. Finally, the instructional dimension addressed the question what educators can do within the context of teaching in order to promote effective ethics teaching. Assuming that the cognitive domain is particularly apt for the domain of instruction, an intervention introducing an epistemic distinction (wrong-complex) was chosen. Feasibility, concept validity, and educational aim were basically confirmed (a) by a statistically significant difference in PMD in the vignettes with an initial high level of PMD, (b) by nearly no difference in the vignettes with an initially low level of PMD (organizational or other problem), and (c) by a baseline measurement (no vignette) with no difference in (generally low) PMD levels before and after the lecture. Although the results are modest, it has to be noticed that the data were gathered in a very short time frame, the intervention consisting in a short lecture, followed by a second measurement. Therefore, it can be assumed that—if already a short classroom intervention is able to demonstrate statistical significance in PMD levels—introducing and enforcing the resilience approach and its epistemic implications throughout the curriculum and in the clinical education will decrease levels of PMD the higher these levels initially are.
As a matter of course, moral resilience of healthcare professionals is not an end on its own. Transforming attitudes and beliefs into planned behavior and moral action can be considered as the ultimate outcome of moral resilience within healthcare settings which at first sight has not been addressed by this study. But within the proposed conceptualization, moral resilience (understood as the capability to “name” and “frame” ethical issues) can be seen as a necessary condition for moral action: In settings of moral opacity (issues of “framing”), it nurtures moral imagination; in settings of moral transparence (issues of “naming”), it fosters moral courage.
The second limitation relates to the design. Exposing students twice to the same vignettes may bear the risk of threatening internal validity. However, the baseline measurements (MDT0 and MDT5) and the vignette with the lowest level of PMD (MDT4 and MDT9) show no statistical significance and therefore support validity. Dividing each study site in a control group and an intervention group would have produced smaller local samples and reduced the chance of reaching statistical significance. Therefore, given the identical intervention at three sites, the risk of bias by renouncing to a control group in favor of a bigger sample was deemed to be lower than the risk of bias by creating three interventional and three control groups. Third, the MDT tool has been developed for clinical settings with real scenarios and single measurements. 38 Using it in educational settings with hypothetical scenarios and an interventional design may not reflect its original intentions. Nevertheless, the vignettes chosen are taken from the experience of peer students sharing a similar educational background.
As to the future, it is to hope that psychological resilience and moral resilience research will merge into an interdisciplinary effort with educational science. A closer analysis is needed to better describe the etiology and phenomenology of moral stressors, which undoubtedly have psychological outcomes and depend on developmental stages and processes, but also require a specific moral response. How HCEE can help students in understanding the questions and finding the answers has been demonstrated here to some extent, but it awaits further evidence that should be given by all the disciplines interested in the topic.
The perils of resilience
Although approaching moral resilience within HCEE opens promising perspectives, it needs further conceptual clarifications. As evidence suggests, the actual talk of resilience in healthcare education and of moral resilience in HCEE is not a temporary fashion or an ephemeral buzzword, but it is neither the panacea curing all the problems of today’s healthcare students and future workforce. If moral resilience does not encourage moral action or a deepened moral understanding, it can even be dangerous: One major danger consists in a too narrow approach to moral stressors that considers only the individual level, risks to generate moral burnout and overlooks the framework conditions under which these stressors appear, and the responsibilities of the organization to address them. Since moral stressors are generated and managed at an individual and systemic level, also moral resilience does. Another danger is the failure to distinguish “naming” from “framing” issues with two possible manifestations:
Confusing a situation of moral wrongness (e.g. elder abuse) with moral complexity can easily lead to moral apathy and acquiescence in the sense of healthcare professionals “bouncing back” from observed malpractice or injustice and leaving aside moral judgment even when this implies that patients, families, professionals, and co-workers are exposed to physical, psychological, or moral harm. 23
Conversely, confusing moral complexity with moral wrongness and not being willing to question personal values and judgments bears the risk of moral fanaticism. In such situations, professionals insist on the moral wrongness of a given course of action and fail to recognize that the situation comprises moral complexity. For example, a patient with life-limiting illness has previously expressed her wish not be fed artificially and is now in a situation of unclear prognosis. 40 By insisting on the morally wrong character of withdrawing nutrition, the professional would certainly abide by the principle of avoiding harm, but he would certainly disregard the overriding professional and moral duty to respect patient autonomy. If a “deviation” from one’s own moral viewpoint is considered as a threat for moral integrity, there is no space for moral negotiation or compromise, which are two necessary conditions for effective deliberation in situations of moral opacity. Considering moral resilience as an imperative not to challenge one’s own values even in the face of overriding ethical concerns recalls Oser’s and Reichenbach’s 41 outstanding description of the phenomenon of the “unhappy moralist.”
These challenges not only show the perils of moral resilience and the need for further conceptual clarification and differentiation in the context of healthcare professions. They also depict the potential of HCEE in helping professionals and students to understand and to address situations which are associated with moral distress and which call for an appropriate moral response.
Conclusion
The importance of promoting psychological and moral resilience in students responds to an urgent need in the healthcare professions’ education and practice. It joins the lenses through which HCEE is seen today. Healthcare professionals increasingly act as providers, managers, and gatekeepers at once. In times of growing global disparities as to the access to healthcare services and effective medical and nursing care, situations that are morally complex or morally wrong are likely to rise. In this perspective, “not-right-not-wrong” statements can demonstrate that students are able to deal with moral complexity. But they should certainly not assuage moral wrongness. Fostering moral resilience in future professionals helps them to circumnavigate both the shallows of moral burnout and moral acquiescence. In order to reach this goal, HCEE has an important contribution to offer by strengthening the knowledge base of moral resilience. This knowledge contributes to the promotion of the mental and physical health of those who give and those who receive care. Training students in transforming this kind of knowledge into practice legitimates HCEE and its costs for societies, faculties, and professional bodies.
Footnotes
Acknowledgments
Daniel Schnyder (statistical support), Prof. Dr Susanne Boshammer, Dr Verina Wild, Dr Carina Fourie.
Conflict of interest
The author hereby declares to have no conflict of interest.
Funding
Careum Foundation Zurich (Fellowship).
Ethical approval
The aim of the research project was presented to the Research Ethics Committee of the Canton of Zurich which stated that no ethical approval was needed for this kind of research (educational setting, no patient data); all students were provided with written information about the project and gave written informed consent prior to participation.