
Abstract
Background:
Moral distress, moral sensitivity, and moral courage among healthcare professionals have been explored considerably in recent years. However, there is a paucity of studies exploring these topics among baccalaureate nursing students.
Aim/objective:
The purpose of this study was to explore the relationship between and among moral distress, moral sensitivity, and moral courage of undergraduate baccalaureate nursing students.
Research design:
The research employed a descriptive-correlational design to explore the relationships between and among moral distress, moral sensitivity, and moral courage of undergraduate nursing students.
Participants and research context:
A total of 293 baccalaureate Filipino nursing students who have been exposed to various clinical areas participated in the study.
Ethical considerations:
Institutional review board approval was sought prior to the conduct of the study. Self-determination was assured and anonymity and confidentiality were guaranteed to all participants.
Findings:
Results indicate that a majority of the nursing students in the clinical areas encounter morally distressing situations that compromise quality patient care. However, despite the fact that they want to do what is in the best interest of their patients, their perception of being the inexperienced among the healthcare team drives the majority of them to ignore morally distressing situations to avoid conflict and confrontation. Another interesting finding is that 79.20% of the respondents hardly consider quitting the nursing profession even if they frequently encounter morally distressing situations. Analysis also shows associations between moral distress intensity and frequency (r = 0.13, p < 0.05) and moral distress intensity and moral sensitivity (r = 0.25, p < 0.05). The dimensions of moral courage are also related to both moral distress and moral sensitivity.
Conclusion:
Results of the study imply that moral distress is a reality among all healthcare professionals including nursing students and requires more consideration by nurse educators.
Introduction
Nurses often encounter ethically laden situations in their clinical practice that conflict with their professional and personal values. Working with incompetent healthcare personnel, unsafe working conditions, organizational constraints, and inadequate staffing have contributed to the rise of ethical dilemmas encountered by professional nurses. 1 –3 Many of these nurses who come across these situations become frustrated in their efforts to uphold their professional commitment to their patients in ways that are acceptable to them, thus leading to moral distress. Webster and Baylis 4 define moral distress as “situations in which nurses cannot fulfill their ethical obligations and commitments, thus they fail to pursue what they believe to be the right course of action.” Moral distress has serious ramifications to nurses since it can lead to professional burnout, physical and emotional distress, moral apathy, and even nurses leaving the profession. 5 –13 Addressing moral distress is imperative because it can reduce its negative consequences, preserves the moral sensitivity of nurses, and promotes moral courage, which can ultimately promote safe and quality patient care.
Lovett and Jordan 14 stated that moral sensitivity is the “the ability to recognize the presence of moral issues in real-world situations.” Nurses belong to a profession where caring is inherent and they are expected to always act in an ethical manner as part of their professional ethos. Despite the various ethical dilemmas that nurses might encounter, it is crucial that nurses remain sensitive and express concern about the consequences of one’s actions for others. Being a patient advocate, nurses need to be actively involved in the decision-making process regarding ethical dilemmas and assist patients to voice their moral concerns. However, there are cases when moral problems exist and they may not be prepared to resolve it. Nurses in these cases need moral sensitivity as it can assist them in engaging in moral reasoning and behavior. The ability to be sensitive and responsive to difficult ethical situations can lead them to have courage to act on their convictions and enhance their sense of commitment and hope in their work.
An important virtue in nursing that contributes to the personal and professional development of a nurse is moral courage. On one hand, courage according to Murray 3 is the “energy that commits the nurse to her work.” It is the person’s ability to overcome fear, to stand up to their own values and principles, to listen and be an advocate despite conflicting obligations. On the other hand, nursing literature on moral courage have documented that many nurses may be reluctant to stand up and speak out when faced with known risks to patients as well as to themselves. 15 –19 Stress, anxiety, fear of reprimand, isolation from colleagues, and threats to employment 19 are some of the negative consequences that can be brought about by morally courageous behavior. These consequences combined with other barriers such as organizational culture, lack of concern by colleagues who do not have the moral courage to take action, and preference for redefining unethical actions as acceptable can lead a nurse to avoid exhibiting moral courage. When nurses lack moral courage, their commitment to the patients under their care is affected, leading to moral distress and even possible unethical behavior. 9,19
While moral distress, moral sensitivity, and moral courage have been addressed in previous research among registered nurses, 15 –17 there is paucity of studies on these topics among nursing students. 20 –23 Ethical dilemmas and moral distress are not only experienced by practicing nurses but are also prevalent among nursing students. Despite the fact that ethics courses are an integral part of undergraduate nursing curriculums, nursing education programs have not adequately prepared young nurses to face and manage ethical dilemmas and morally distressing situations. Comrie 24 espouses that limited clinical experience, poor self-confidence, inadequate professional judgment, and limited ethical knowledge and training all contribute to nursing students’ being unable to cope with moral distress, which can ultimately decrease their moral sensitivity and capacity to be morally courageous. Nursing students need the abilities and skills to effectively manage moral distress, and nursing educators have the responsibility to prepare beginning nurses by facilitating learning experiences that allow them to reflect on and confront ethical dilemmas. To do this not only requires moral knowledge but moral sensitivity and courage as well. 25 –27 Hence, the overall purpose of this article is to explore the relationship between and among moral distress, moral sensitivity, and moral courage of undergraduate baccalaureate nursing students. It is hoped that the results of this study will assist nursing educators in developing a more effective ethics education for nursing students which can better prepare them for the ethical realities in clinical settings.
Methods
Design, study site, and sample
A descriptive-correlational design was utilized to explore the relationships between and among moral distress, moral sensitivity, and moral courage of undergraduate nursing students. The locus of the study was a comprehensive university in Manila, Philippines that has a 4-year Bachelor’s degree in nursing program. Inclusion criteria for the respondents were based on the following: (a) undergraduate students who have been exposed to clinical areas for at least two to three rotations regardless of the specialty areas, (b) must be 18 years old and above, and (c) had a basic course in ethics in their undergraduate program.
The demographic profile of the respondents is shown in Table 1. The respondents were primarily comprised of females (75.4%) with the participants’ mean age being 19.09 years (±0.91). A majority of the respondents were senior nursing students (55.6%) and 54.6% of them have been exposed to medical surgical units in the past 2 years.
Demographic profile (N = 293).

SD: standard deviation.
Outcome measures and data analysis
To gather data, four instruments were used: first, a robotfoto was utilized to establish the characteristics of the respondents. Robotfoto is a Dutch term that serves as a preliminary sketch to identify a subject. 28 Second, the Moral Distress Questionnaire developed by Hamric and Blackhall 11 which measured the frequency and the level of distress the situation causes on a scale from 0 to 4 was employed. The left part of the scale is the frequency scale, which goes from 0 (never occurred) to 4 (very frequently). The right part of the scale measures how distressing the situation was to the nurse with the scale from 0 (not distressing) to 4 (greatly distressing). The tool has been established to be reliable with Cronbach’s alpha coefficient of 0.89. Third, moral sensitivity was measured using the Revised Moral Sensitivity Questionnaire developed by Lutzen et al. 29 The revised instrument had nine items with six possible responses from 1 (total disagreement) to 6 (total agreement) and was deemed to be a valid instrument to measure moral sensitivity. It measures three factors related to moral sensitivity, which include moral burden, moral strength, and moral responsibility. Finally, the Professional Moral Courage (PMC) Scale designed by Sekerka et al. 30 was utilized to measure the moral courage of the nursing students. PMC has five themes: moral agency, multiple values, endures threat, goes beyond compliance, and moral goal. It has 15 items answerable from 1 (never true) to 7 (always true). Permission was obtained from the corresponding author to change some words in the tool as the scale pertains to working professionals. Since the study was conducted among nursing students, some words were changed to fit the profile of the respondents. Question #1 and #13 which used the word “work” was changed to “in my clinical rotation”; in Question #3, “work associates” was changed to “groupmates”; in Question #6, “my boss” was changed to “team leader or clinical instructor/preceptor” and finally, in Question #10 “co-workers” to “groupmates.” Data were collected from September to October 2015.
Gathered data from the robotfoto were analyzed descriptively using SPSS version 21. To examine relationships among variables, data were analyzed using Pearson’s correlation. p values <0.05 were considered statistically significant. Cronbach’s alpha reliability generated 0.96, 0.83, and 0.91, respectively, for all the tools.
Ethical considerations
Institutional review board approval was sought prior to the conduct of the study. After seeking approval from the Dean of the College of Nursing, the qualified respondents were given information about the aim of the study. Anonymity and confidentiality were guaranteed. All responses from the respondents were kept anonymous and non-traceable to individual student nurses. All the respondents signed a consent form. Permission to use all the instruments in the study was obtained from the authors.
Data gathering procedure
Based on the inclusion criteria, junior and senior nursing students were included. The survey questionnaires were distributed to qualified respondents during their free time in class. To maximize participation of the respondents, the instruments were also made accessible online in the learning management system of the university (community site), and the nursing students were requested to answer the survey in their most convenient time. The survey was implemented for 4 weeks from September to October 2015.
Findings
Moral distress
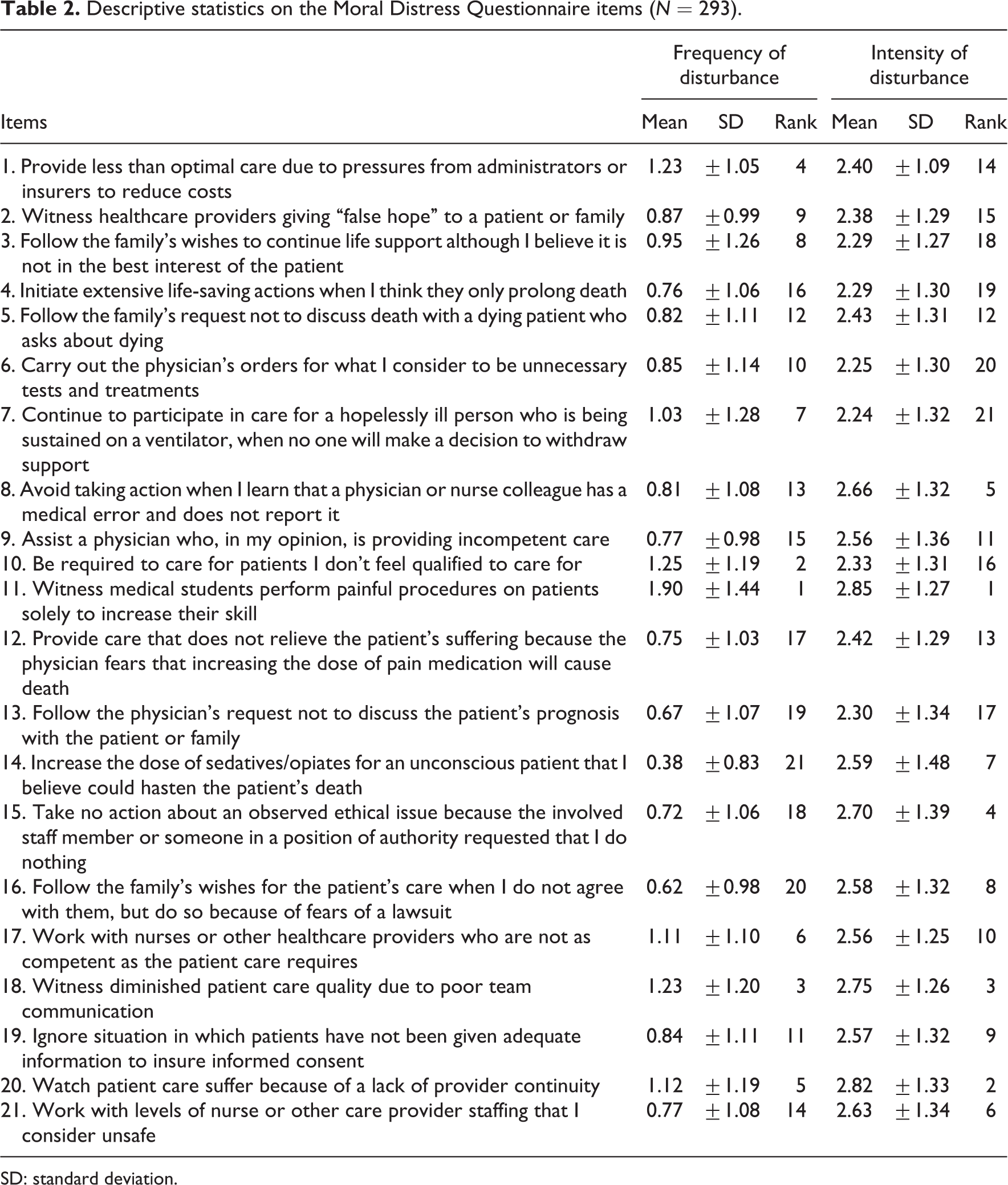
Table 2 shows the nursing students’ responses to the moral distress questionnaire. Based on the results, the nursing students frequently encounter morally distressing situations such as “witnessing medical students perform painful procedures on patients solely to increase their skill” (M = 1.90, standard deviation (SD) = ±1.44), “being required to care for patients I don’t feel qualified to care for” (M = 1.25, SD = ±1.19), and “witnessing diminished patient care quality due to poor team communication” (M = 1.23, SD = ±1.20) in their clinical rotations. Furthermore, the situations that cause the most distress to the nursing students are “witnessing medical students perform painful procedures on patients solely to increase their skill” (M = 2.85, SD = ±1.27), “watching patient care suffer because of a lack of provider continuity” (M = 2.82, SD = ±1.33), and “witnessing diminished patient care quality due to poor team communication” (M = 2.75, SD = ±1.26). These results show that a majority of the nursing students in the clinical areas encounter morally distressing situations that compromise quality patient care due to lack of competence and poor communication and collaboration among the healthcare providers. It is also interesting to note that among the top three frequently encountered distressing situations, two are also included in the most morally distressing situations for them.
Descriptive statistics on the Moral Distress Questionnaire items (N = 293).
SD: standard deviation.
Moral sensitivity
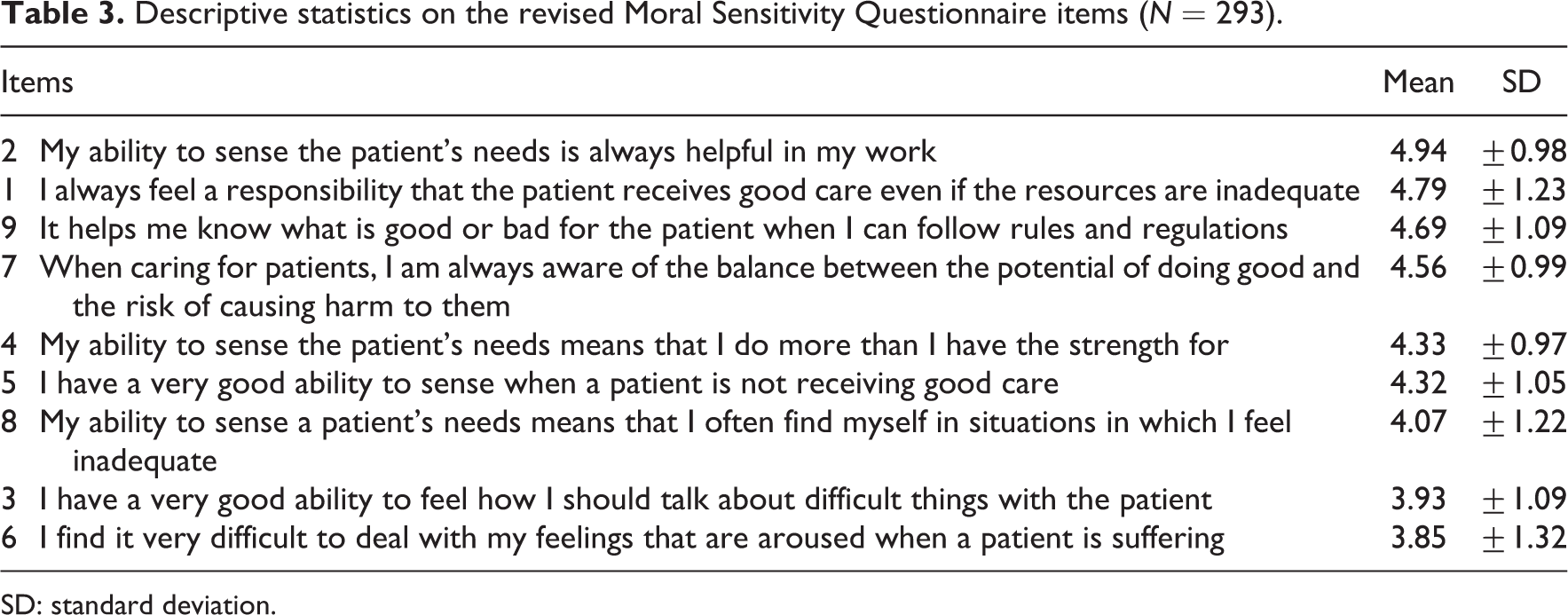
With regard to moral sensitivity, Table 3 illustrates the results to the Revised Moral Sensitivity Questionnaire. Results show that the item under the moral dimension of moral strength, “My ability to sense the patient’s needs is always helpful in my work,” received the highest mean score of 4.94 (±0.98) followed by the two items under the moral responsibility dimension, “I always feel a responsibility that the patient receives good care even if the resources are inadequate” (M = 4.79, SD = ±1.23) and “It helps me know what is good or bad for the patient when I can follow rules and regulations” (M = 4.69, SD = ±1.09). These results reflect the general desire of the nursing students to help patients, reinforcing the basic ethical principle of beneficence among healthcare practitioners. Furthermore, it also shows that for nursing students, knowledge about ethical principles and rules and regulations is essential so as to guide them in making well-grounded moral decisions.
Descriptive statistics on the revised Moral Sensitivity Questionnaire items (N = 293).
SD: standard deviation.
Moral courage
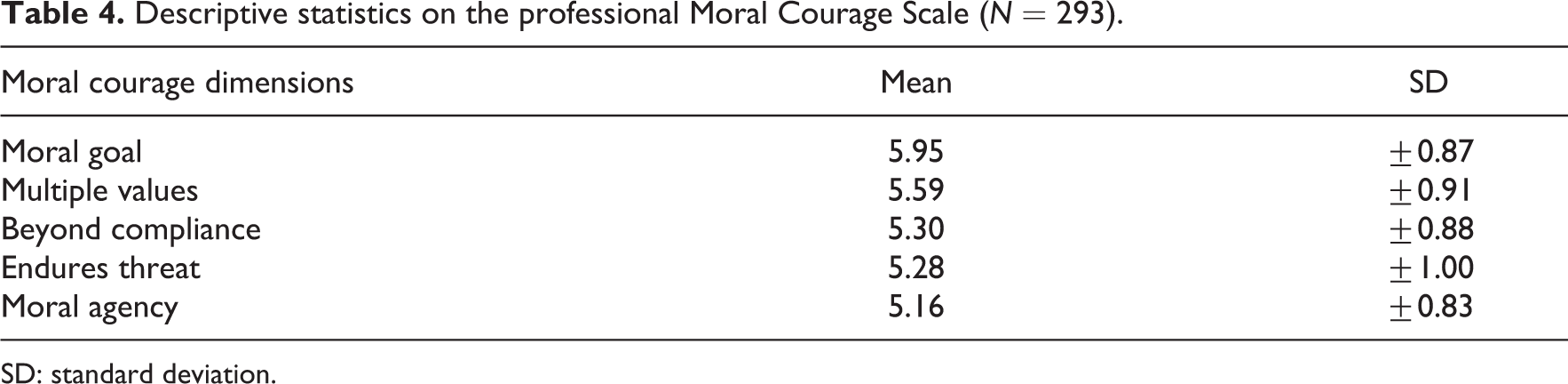
Table 4 presents the responses of the nursing students to the PMC Scale. The theme of moral goals garnered the highest mean score of 5.95 (±0.87) followed by the theme of moral values (M = 5.59, SD = ±0.91). Results show that prudence and guidance about the rightness and appropriateness of what is to be done and be motivated by these judgments to act in accordance with them is crucial for the respondents. Moreover, these findings also confirm that personal and organizational values do influence their ethical decision-making and moral behavior.
Descriptive statistics on the professional Moral Courage Scale (N = 293).
SD: standard deviation.
Relationship among moral sensitivity, moral distress, and moral courage
The relationship among moral sensitivity, intensity and frequency of moral distress, and moral courage subscales is presented in Table 5. On one hand, results revealed that moral distress frequency is significantly related to moral distress intensity (r = 0.13, p < 0.05) which can indicate that encountering moral situations frequently can cause the nursing students to be morally distressed; intensity of the moral distress, however, would depend on the situations that cause it. Moreover, it was shown that moral distress frequency has a negative relationship to the subscale of moral courage-multiple values (r = −0.13, p < 0.05) suggesting that frequently encountering morally distressing situations, nursing students are not yet able to draw from their set values fully and make firm decisions when external demands or concerns arise.
Correlation analysis among moral distress frequency and intensity, moral sensitivity, and moral courage dimensions (N = 293).
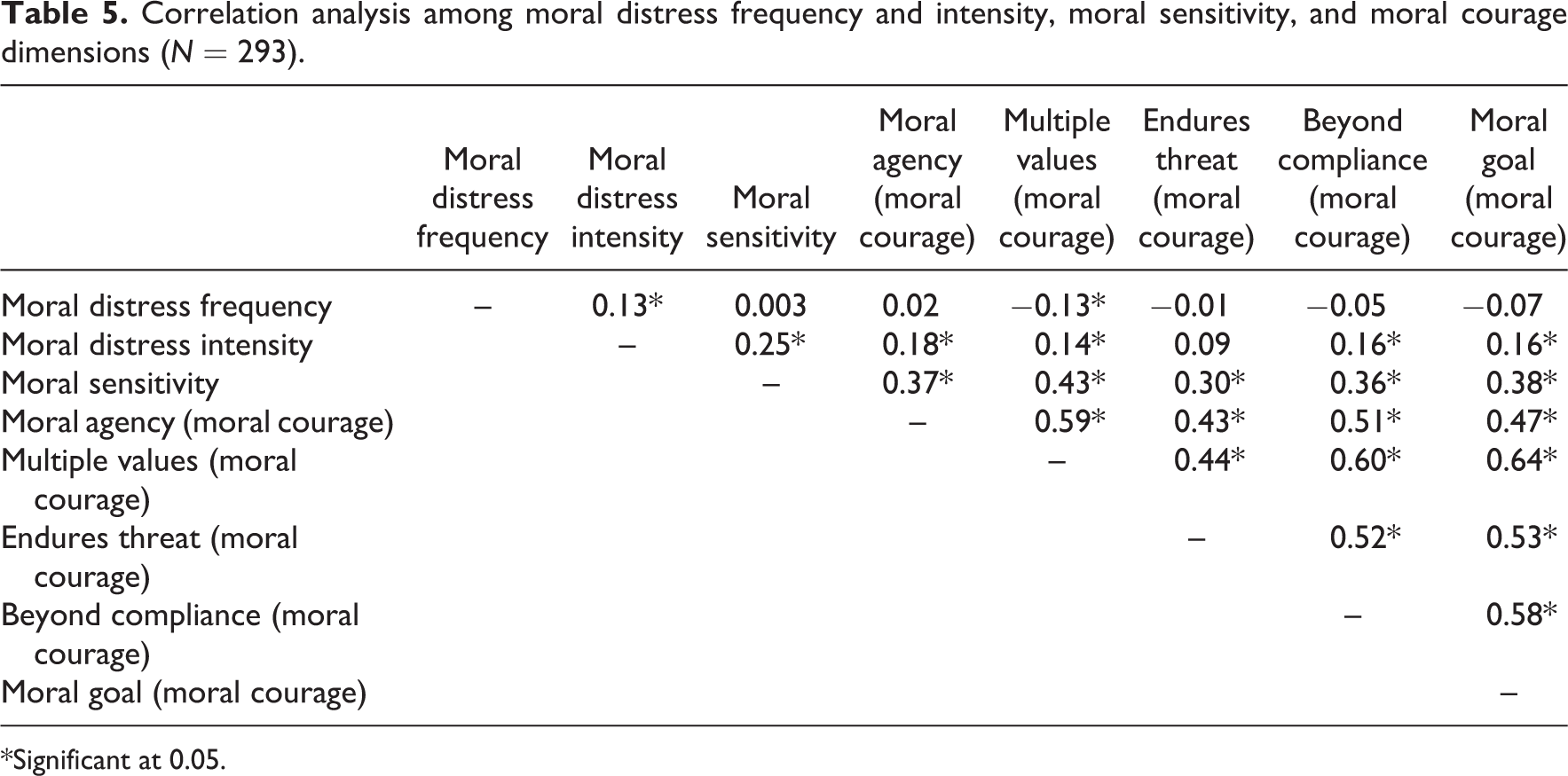
*Significant at 0.05.
On the other hand, moral distress intensity was shown to be positively correlated to the moral courage themes of multiple values (r = 0.14, p < 0.05), moral agency (r = 0.18, p < 0.05), endures threat (r = 0.16, p < 0.05), and goes beyond compliance (r = 0.16, p < 0.05) subscales. Morally distressing situations can provide students situations in which they can draw from their values taught to them, but having the courage to do something about it because they know that it is the right and moral thing to do depends on the intensity of the situation. Furthermore, there exist a positive and significant relationship between moral sensitivity and moral distress intensity (r = 0.25, p < 0.05). This suggests that in encountering morally distressing situations, nursing students are able to have an insight about the action of others and identify moral issues which may affect the patient. This result reinforces the fact that inherent to the profession of nursing is being sensitive to the needs of others. It is also interesting to note that 79.2% of the respondents hardly consider quitting the nursing profession despite the fact that they frequently encounter morally distressing situations.
Moral sensitivity dimension was also found to have a positive relationship to moral courage themes: moral agency (r = 0.37, p < 0.05), multiple values (r = 0.43, p < 0.05), endures threat (r = 0.30, p < 0.05), beyond compliance (r = 0.36, p < 0.05), and moral goal (r = 0.38, p < 0.05). Results indicate that when student nurses are morally sensitive, the more they exhibit their predisposition to act as moral agents. However, they might encounter circumstances that can limit their capacity to do what they believe is right and fair.
Discussion
Results of this study yielded an interesting portrait of the moral sensitivity, moral distress, and moral courage of undergraduate Filipino baccalaureate nursing students. Several key findings emerged from the study. First, while varying situations can cause moral distress, lack of competence, poor quality patient care and inadequate communication, and collaboration among healthcare providers were seen by the student nurses as the most frequently encountered morally distressing situations in their practice. These findings run parallel to that of Cronqvist and Nystrom, 31 Hamric and Blackhall, 11 and Zuzelo 32 that assert that moral distress occurs among student nurses due to perceived internal and external constraints such as inexperience, decreased confidence and competence, unethical patient care practices, and infrequent collaboration. However, facing morally distressing situations often does not necessarily indicate that it will cause intense distress on their part. Epstein and Delgado 2 noted that nurses perceive morally distressing situations in various ways and, therefore, will respond to it differently as well. Multiple studies 1,27,32 –34 have shown that nurses are more likely to experience intense moral distress when these situations threaten indispensable patient rights such as right to safe and quality care, right to information and right to consent and refuse treatments. Violations of these rights can lead to frustration and anger and, more importantly, can threaten one’s moral integrity.
Surprisingly, a noteworthy finding of this article is that although student nurses experience moral distress, which as Epstein and Delgado 2 noted is inevitable, a majority of them hardly consider quitting the profession. This finding is encouraging because most studies have shown that experiencing moral distress can lead new nurses especially the younger ones to leave the workplace just to maintain their moral integrity and prevent burnout. 1,35,36 Hence, it is critical that student nurses recognize these situations and to learn how to deal with them, as negative experiences and environments can be significant deterrents to their stay in the nursing profession.
Findings of the study also revealed that student nurses are able to recognize morally distressing and challenging situations which is important is honing their moral sensitivity. Lutzen et al. 29 posit that individuals who possess moral sensitivity are more capable of resolving ethical conflicts and make morally grounded decisions. Thus, promoting the moral sensitivity of nursing students can increase their moral competence and decrease the impact of moral distress. Furthermore, the student nurses also recognize their role as patient advocates. Consistent with the findings of Altun and Ersoy, 27 student nurses can demonstrate considerable insights to moral issues and espouse strongly for patients especially on issues that affect their care. Since morally distressing situations do occur and tend to recur in clinical practice, providing student nurses ethics education and trainings can give them the necessary knowledge and skills needed for ethical decision-making.
Similarly, in resolving ethical dilemmas, prudence in action and personal and organizational values of the respondents also come into play. While most decisions are routine, ethical dilemmas in clinical practice can test a person’s deeply held values. Choices and decisions usually reflect the professional and personal values of a person and as Murray, 3 Clancy, 37 and Tenbrunsel and Smith-Crowe 38 noted, value awareness and clarification are needed to resolve value conflicts and morally distressing situations. The ability to recognize and resolve moral distressing situations can cultivate moral courage necessary in nursing practice.
Finally, it is important to note that despite the fact that student nurses are morally sensitive and have the capacity to be morally courageous, a majority of them encounter circumstances that hinder their ability to demonstrate their moral courage. Multiple barriers to showing moral courage, as put forward by Lachman 18 are organizational culture, lack of concern by colleagues, collective decision by individuals to look the other way, and the preference for redefining unethical actions as acceptable. Nursing education in the Philippines is highly patterned after Western nursing baccalaureate standards, which emphasizes the importance of developing critical thinking skills and collaboration among the healthcare team. 39 –41 However, in spite of this, the nurse–physician relationship in the Philippines remains to be a hierarchical one, with the physician mostly being in charge. 42 Nurses rarely question doctors’ orders even if, at times, they find it doubtful. Furthermore, being nursing students add more to their hesitation to exhibit the virtue of moral courage. Student nurses may be regarded as the novices in the profession and therefore maybe viewed by others to lack the experience and competence to question unethical practices. 6,31,32,43,44 Studies have also shown that student nurses also doubt their own confidence and competence to question the competence of other healthcare professionals because of their being junior members of the healthcare team. 45 In this study of Filipino undergraduate nurses, hesitation to respond to morally distressing situations may also be attributed to the Filipino value orientation of hiya 46 (roughly translated as shame). Student nurses may feel shame to express his viewpoints to someone in position or older because it may be regarded as a sign of disrespect. As Caparas and Hartijasti 47 pointed out, hiya drives the person to give in, to avoid the personal experience of shame and avoid being the cause of other people’s shame, thereby yielding to the group’s opinion or decision. Thus, suppressing moral courage due to hiya may lead to negative patient outcomes and moral distress.
Conclusion
Moral distress is undoubtedly a reality among all healthcare professionals including nursing students. Moral issues require moral sensitivity as it paves the way for healthcare professionals to advocate and protect their patient’s rights. Moral courage is an integral aspect of the formation of a competent and compassionate nurse who will speak up for his or her patients especially those who are vulnerable. In this study, moral distress, sensitivity, and courage of baccalaureate Filipino nursing students were explored. It is crucial to note that student nurses frequently encounter situations that make them morally distressed and these include lack of competence, poor quality patient care, and inadequate collaboration among healthcare professionals. Despite the fact that they want to do what is in the best interest of their patients, their perception of being the inexperienced among the healthcare team drives a majority of them to ignore morally distressing situations and look away to avoid conflict and confrontation. However, this practice can lead to young nurses getting disillusioned with the profession and causing the profession to lose potentially good and moral nurses. Clearly, this study affords some practical implications for nursing educators as they can take into account the findings of this study in planning future ethics learning programs for nursing students. Promoting ethics education among them is crucial to assist and to prepare them in their future role as patient advocates. Simulation and discussion of actual ethical dilemmas and morally distressing situations can allow them to realize their values and how it affects their behavior. It also provides them opportunities to express their views and hone their decision-making skills. Moreover, education and training on ethics should also not stop after graduation, but they should be encouraged to continue it throughout their entire nursing career so that they are able to cope better in their role as patient advocates. These measures can increase not only their moral sensitivity, but also their capacity to be morally courageous.
While there is enough literature that supports the findings of this study, the results reported above may not be generalizable to all nursing students. More comprehensive research needs to be done on a wider scale, which can include nursing students coming from different universities, with different educational and ethnic backgrounds as well as coming from other regions and countries to improve one’s understanding in this area. Moreover, it might also be useful to conduct a qualitative research to further explore the moral distress, sensitivity, and courage of nursing students. This is to validate the quantitative results so that the limitations of the study can be minimized and addressed. Additionally, longitudinal studies can be done to gain more insights into the effects of moral distress to future nurses and to explore the various ways on how they deal and cope with morally distressing situations.
Footnotes
Acknowledgements
The author would like to express her sincere gratitude and appreciation to the UST College of Nursing, especially to Dean Susan Maravilla, for supporting this research through their endorsement, the students who participated in this meaningful study for their cooperation and patience in accomplishing the questionnaires, and to Prof. Andrew Bernardo, Prof. Elmer Hibek, and Mr Les Paul Valdez for sharing their expertise in English and Statistics. The author also expresses her appreciation to Ms Josette Jurado and Mr John Rey Macindo for their professional assistance that led to the completion of this research.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the College of Nursing, University of Santo Tomas through the Commission on Higher Education (CHED) Research Grant. The funding source supported the study financially and had no involvement in the study design, data collection, analysis and interpretation of data, writing of the report, and decision to submit the paper for publication.