
Abstract
Background:
The ability to consent promotes children’s access to health services. Healthcare providers should assess and arrive at a clinical judgement about the child’s maturity and mental capacity to obtain valid consent.
Research objective:
The objective of the study was to determine practices employed by South African healthcare providers to obtain consent for treatment from children.
Research design:
A qualitative, explorative, descriptive research design was used and the study was contextual.
Participants and research context:
In all, 24 healthcare providers (professional nurses and medical practitioners) were purposively sampled from a hospital and primary health clinics. Semi-structured interviews were used.
Ethical consideration:
Ethical approval was obtained from the Institutional Review Board and gatekeepers. Written informed consent was obtained from each participant.
Findings:
Healthcare providers’ current practices in obtaining consent from children revealed inconsistency in implementation as well as the yardstick used to determine children’s mental capacity. Building trust with children, sharing information and assessment were interlinked in obtaining consent.
Discussion:
The inconsistent practice has implications for children’s access to healthcare services.
Conclusion:
Inconsistent practices in the implementation of consent laws have the potential to violate children’s rights to bodily and psychological integrity, access to health services and having their opinions heard and be taken into consideration. Through uncovering the current perceptions and practices and a literature review, guidelines intended for use by the Department of Health could be developed.
Keywords
Introduction
Children have the right to enjoy the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. The United Nations Convention on the Rights of the Child (UNCRC) expects State Parties to strive to ensure that children are not deprived of their right of access to such healthcare services. 1 Children’s ability to consent promotes access to health services. Furthermore, children have the right to express their views in all matters that affect them and have their views be given weight in accordance with their age and maturity. 1 This also relates to their healthcare, treatment and rehabilitation.
Background
In South Africa, the State has a duty to ensure accessible healthcare services for all children and that their health needs are met at all levels of health service delivery. The State discharges its duty to accessible health services through healthcare providers. 2
Internationally, there has been a trend to lower the age of consent to healthcare and treatment ranging from 12 to 19 years. In countries influenced by British law, the ability rather than age of consent is considered. In these countries, the Gillick ruling applies where a competent child is seen as one who ‘achieves a sufficient understanding and intelligence to enable him or her to understand fully what is proposed’ and has sufficient discretion to enable him or her to make a wise choice in his or her own interests. 3
In South Africa, 24% of children live with neither of their biological parents. Contributing factors are urban migration, poverty, educational opportunities, cultural practice and children being orphaned in the aftermath of the HIV/AIDS pandemic. These children live with neighbours, aunts, grandparents or in child-headed households. 4,5 The conditions for full parental rights of biological parents are stipulated in the Children’s Act 38 of 2005. 6 In the case where neither parents are available, parental rights and responsibilities may be transferred under certain circumstance to other persons. 6 If the parents or guardian is not available and the child cannot consent, a caregiver may consent to a medical procedure or an HIV test or HIV disclosure in younger children (Sections 129 and 130). 4,6 Only parents and legal guardians may assist a minor to consent to a surgical operation (Section 129). 6 If medical treatment or a surgical operation is necessary to preserve the life of the child or to save the child from serious or lasting physical injury or disability, and the need for the treatment or operation is so urgent that it cannot be deferred for the purpose of obtaining consent the superintendent of a hospital or in his or her absence, the person in charge of the hospital may consent to the medical treatment or a surgical operation on a child if the treatment or operation is (Section 129 (6)). 6 In the cases where limited time is at hand and a parent, guardian or caregiver is deceased or cannot be traced, consent may be given by the Minister of Social Development. 4 For matters where consent is urgent, applications can be made to the High Court or the Children’s Court (Section 129). 4,6
Enabling all children to access health services autonomously has led to progressive law reforms in South Africa 2 with the promulgation of the Children’s Act 38 of 2005 (Section 129) 6 outlining the consent requirements. According to this Act, the age of majority is 18 years and the age of consent was lowered to 12 years (subject to conditions).
This lowered age threshold has significant implications for healthcare providers when providing healthcare to children 2 as they are not only required to know the consent requirements but also ensure that the specific conditions for obtaining valid consent (in addition to age) are met. Healthcare providers furthermore have a moral responsibility to protect the best interest of the child 1 when they are not able to make informed decisions and to protect the child’s autonomy when they do. 7
According to South African legislation, for consent to be valid it must be given by a person capable in law to do so, must be informed, unambiguous, comprehensive and voluntary. 8,9 Being capable in law means that a person has reached the threshold age stipulated by law and has decisional capacity. 6,9 Decisional capacity is also referred to as mental capacity 9 and has been used interchangeably in this article.
In order to obtain valid consent, the requirement of mental capacity should be determined by the healthcare provider. Health-related decisional capacity is the ability to make rational informed choices about accepting or refusing treatment or investigations.
10
Children are viewed to have decisional capacity if they seem to understand information relevant to their level of comprehension and appropriate to the specific nature and scope of the decision.
11
The four domains to health-related decisional capacity assessment are as follows:
12
–14
Understanding of the fundamental meaning of the condition, diagnostic investigation and treatment; Appreciation of the situation and consequences relative to the child’s own situation; Reasoning by comparing the alternatives in light of the consequences; Communicating a choice in a consistent manner.
A multitude of factors influence children’s decisional capacities. 3,15,16 Some of these factors include the child’s cognitive maturity, 17,18 disability and presence of a chronic illness, 6 their personal social experience with illness and healthcare, 3,17 the seriousness and type of the health decision, 4,19 and constructive parental support and parental attitudes. 17,20
Healthcare providers’ attitudes, competencies to share information and respect for children’s views and perspectives play pivotal roles in children’s decisional capacity. 13 Furthermore, healthcare providers’ competence in providing information to children and performing capacity assessments has an influence on their decisional capacity. 3,20 These decisional capacity assessments could be challenging to healthcare providers as they are time-consuming 4 and require the competence to communicate with children and assess their cognitive development and mental health. 3,13
Problem statement
Currently, there are no clear guidelines in the Children’s Act 6 or its regulations to assist healthcare providers with maturity and mental capacity assessments with limited guidance in literature especially for children. 4,9 In addition, many healthcare providers have been inadequately trained to do these assessments 21 and currently these assessments are not standardised. 22
These current limitations could lead healthcare providers to use intuition in their assessments 11 and consent laws being implemented inconsistently. 4 In practice, it was noticed that out of fear for litigation healthcare providers tend to obtain consent from parents regardless of the consent requirements specified in the Children’s Act. 6 A guide that is context specific and relevant needs to be developed to assist healthcare providers; however, the first step would be to determine what the current practices and perceptions are of healthcare providers, who have to enact the laws. Based on this information, literature sources should be used to propose a guide for assessment of children’s decisional capacity.
Objective
The objective of the study was to determine the practices employed by healthcare providers working in Tshwane, South Africa, to obtain consent from children for treatment.
Methods
A qualitative, explorative, descriptive research design was used. 23
Setting and population
The target population comprised all professional nurses (PNs) and medical practitioners (MDs) working in a hospital, community health centres and clinics in the northern regions of the city of Tshwane, in South Africa. The City of Tshwane is the administrative capital of South Africa with an estimated population of 2 million, with about 18% of people living in informal settlements.
24
Health services are provided through regional hospitals, district hospitals, community health centres, clinics and satellite service units.
24
PNs and MDs were sampled purposively.
23
At the time of data collection, from the sampled clinics, there were 118 PNs and 15 medical doctors. The participating hospital had a total of 143 PNs; six PNs were specialised in child nursing and one in psychiatric nursing science. During the same period, there were 22 MDs. Diversity of sampling participants was ensured based on the following inclusion criteria: Healthcare providers who were registered as either MDs or PNs; Healthcare providers working in two practice settings, namely a hospital and clinics; Healthcare providers with at least 1 year experience in providing healthcare services to children; Healthcare providers who consented to participate in the study.
The sample size of 24 healthcare providers depended on the saturation of data. Saturation was reached after 20, but four more interviews were conducted to confirm the data saturation. The researcher, supervisors and independent coder who are knowledgeable about qualitative data analysis confirmed the data saturation.
Data collection and procedures
Data were collected between March 2014 and December 2014. Semi-structured interviews were used to enable participants to openly discuss their current practices and perceptions when assessing children’s maturity and mental capacity when obtaining consent from them. Individual interviews were deemed most appropriate as it provided an opportunity to provide maximum information in a non-threatening environment. Furthermore, an interview allowed for both verbal and non-verbal interactions between the researcher and participant, enabling the researcher to obtain multiple responses to questions and allowing for detailed responses. 25
Interviews were conducted in English for 30–60 min, in a private venue in the workplaces during times when there were no patients or they were available to be interviewed. All participants could speak English. An interview schedule was developed and used as the data-gathering tool. The interview schedule (refer to Table 1) aimed at gaining participants’ perspectives but at the same time gave the researcher control of the interview so that the purpose of the study could be achieved and the research topic could be adequately explored. 25 The interview schedule was pre-tested by the researchers with two participants. The data were included as no changes were required and relevant information rich data was obtained.
Interview schedule.

Data analysis
Data were analysed using descriptive qualitative content analysis. 23 After interviews were conducted, the audio recordings were transcribed verbatim and field notes were added to individual interviews in order to enhance data triangulation, and enhance meaning and detail to the findings. 23 During the process of analysis, patterns and similarities in the interviews were identified with the focus on their practices employed by healthcare providers when obtaining consent from children for treatment. Themes were identified and recorded. The researchers and independent coder reached consensus regarding the themes, categories and subcategories identified in the data.
Trustworthiness
Trustworthiness was enhanced through the criteria of credibility, transferability, confirmability, dependability and authenticity. 26 Adequate time was spent with participants to enhance prolonged engagement. The methods and findings were described densely and purposive sampling ensured that persons with knowledge and experience about the topic would be included. The interview schedule was pre-tested and the data analysed by an independent coder who reached consensus with the researcher on the themes, categories and subcategories. All data and supporting documents were kept to ensure an audit trail.
Research ethics
Ethical approval was obtained from the Tshwane University of Technology Research Ethics committee as well as the Tshwane Regional Ethical committee. Permission was granted by the Chief Executive Officer of the hospital and manager of the relevant clinics included. Informed consent was obtained from participants and interviews were conducted during times when the health service was not offered or not busy. All participants’ names were coded and excluded from transcripts and in all forms to ensure confidentiality and anonymity. All data had been password protected and would be stored securely for 3 years at the university where after it would be destroyed.
Results
In all, 24 healthcare providers participated in the study. Totally, 19 participants were PNs and 5 were MDs. In all, 8 worked at the hospital and 16 at primary healthcare clinics. No mentionable differences were identified between the medical doctors and PNs. However, there was a greater tendency in the data from the participants in the hospital to enforce parental consent at all times, possibly based on hospital policies; however, this phenomenon would require further exploration. No biographical data on ethnicity were obtained, which might have been relevant in influencing attitudes of healthcare providers. All the data of the MDs and PNs were merged.
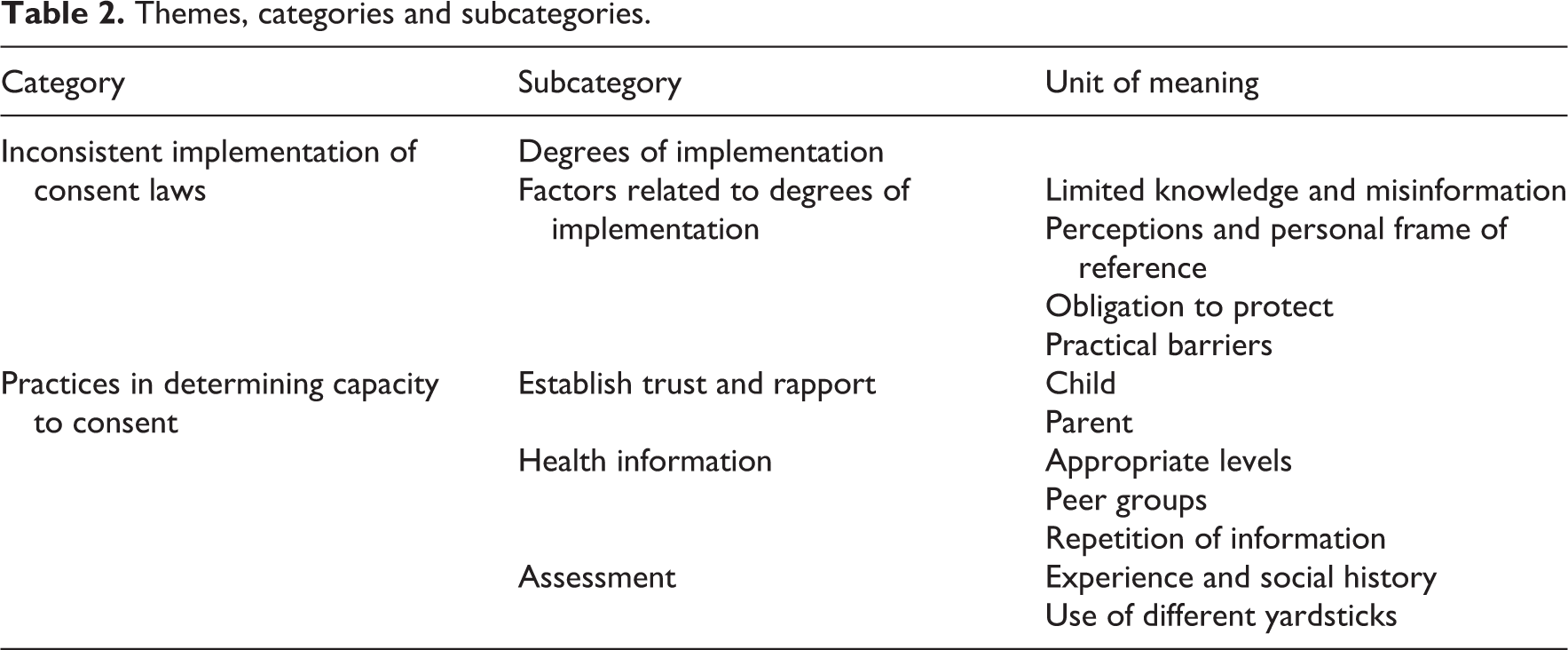
From the data, two themes related to the practice of healthcare providers were identified, namely, inconsistent implementation of consent laws and practices in determining children’s capacity to consent. The themes, categories and subcategories are summarised in Table 2.
Themes, categories and subcategories.
Inconsistent implementation of consent laws
When obtaining consent from children, healthcare practitioners applied the consent laws inconsistently evidenced by varying degrees of implementation influenced by a number of factors.
Varying degrees of implementation of consent laws were evidenced in the data by some healthcare providers’ refusal to provide health services to children if no parent was present to consent as explained: ‘Parents are needed for consent, children without parents are sent home’ (PN). On the other end of the continuum treatment was provided regardless of the child’s capacity to consent, as a participant explained: ‘You just give them everything they want … We don’t ask many questions’ (PN).
In between these extremes were healthcare providers providing health services to children but cautioning them to be accompanied by a parent or by obtaining dual consent from parents and children in future. One PN explained, ‘I will never send them away with no kind of treatment but I will ask them to come back with someone they trust that I can speak to’.
The factors that contributed to the inconsistent implementation by healthcare providers of the consent laws were some due to limited knowledge or misinformation about consent laws, perceptions and personal frames of reference influencing healthcare providers’ practice, feeling obligated to protect both children and their parents and practical barriers influencing obtaining consent from children.
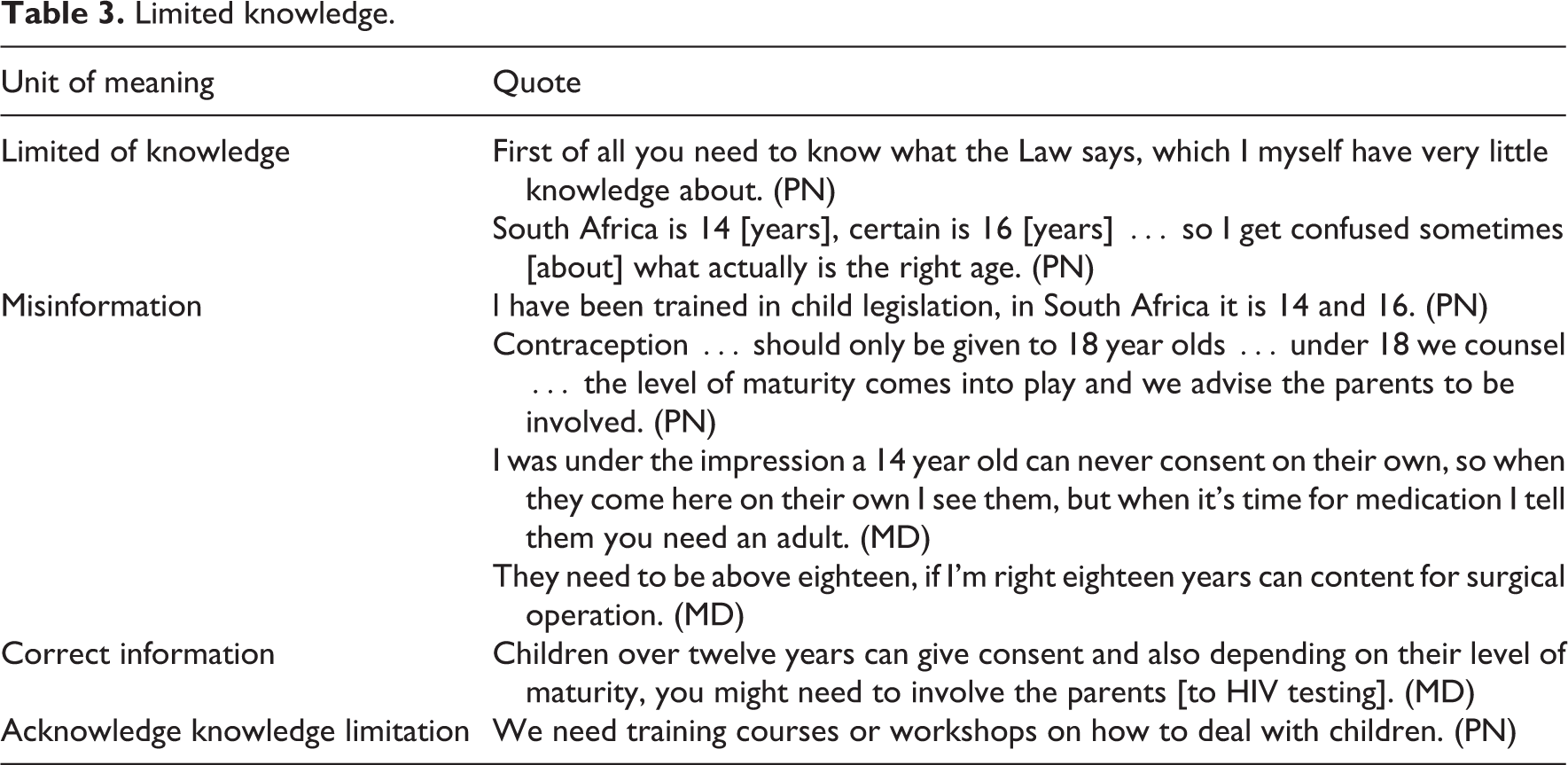
Some participants were conversant with the consent laws. Others acknowledged their limited knowledge with regard to the Children’s Act 6 and its provisions. Some stated that they were knowledgeable. However, during the interview, it became evident that they were referring to the previously repealed Child Care Amendment Act 27 or had misinformation about the present Act’s age limits. Some healthcare providers verbalised that they were aware that the Act had been revised but were uncertain about the details thereof and how it impacted on their current practice. Very few healthcare providers were aware of the requirement to assess children’s maturity and mental capacity and expressed anxiety and distress as they felt ill equipped to do so. However, they acknowledged the importance of being knowledgeable about the consent legislation (Table 3).
Limited knowledge.
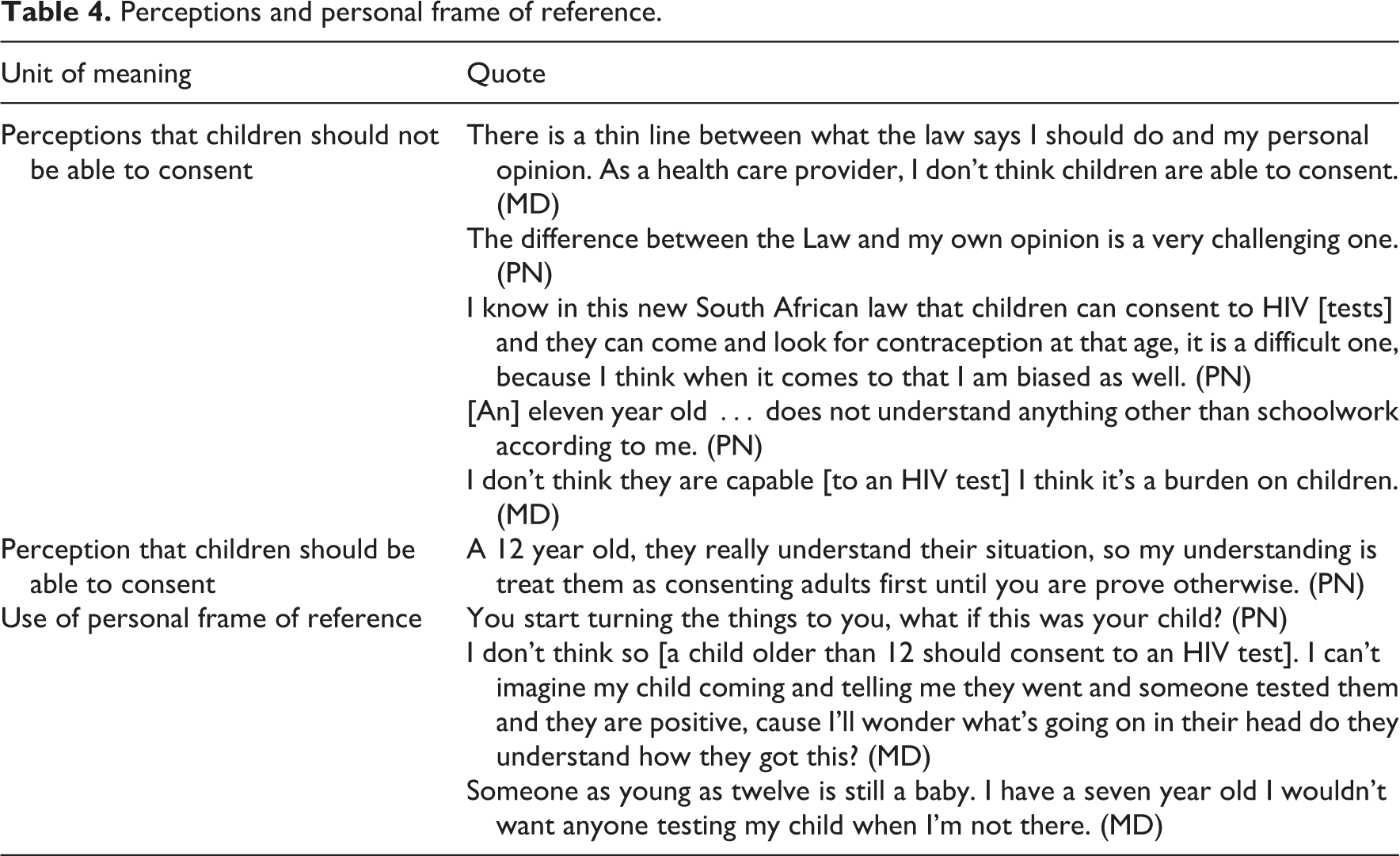
Healthcare providers’ perceptions and personal frame of reference about the appropriateness for children to give consent influenced practice which contributed to inconsistent implementation practices. Many healthcare providers felt that children were not supposed to consent. Table 4 provides the units of meaning and quotes about healthcare providers’ perceptions and personal frame of reference.
Perceptions and personal frame of reference.
Another factor leading to inconsistent implementation of consent laws was that healthcare providers felt obliged to protect children and themselves taking on a parental role as one participant explained: ‘I just speak to her as a mother … protect her …’ (PN) and ‘… they don’t really know what they are doing to their bodies, they need to be protected’ (PN). An MD explained his or her concerns about disclosing HIV status to a child without a parent for support: ‘I always have this feeling, “what if I test this child, this child is positive and they don’t really understand and they go and commit suicide?”‘ Some healthcare providers personalised the fact that parents might be excluded from the consent process and wanted to protect what were in their perception parental rights. One participant said, ‘I think a parent has a right to know what is happening with their child. I would want to know’ (PN).
Some of the practical barriers that influenced implementation of consent laws were the limited time due to human resource shortages and needing more time to work with children, a need for multi-professional support and guidelines to implement the consent laws and to perform mental capacity assessments. Table 5 outlines these units of meaning and supporting quotes.
Practical barriers.

Practices used when determining capacity to consent
Healthcare providers explained their current practices when assessing children’s capacity to consent starting with building a trusting relationship and rapport, then providing information followed by assessment practices.
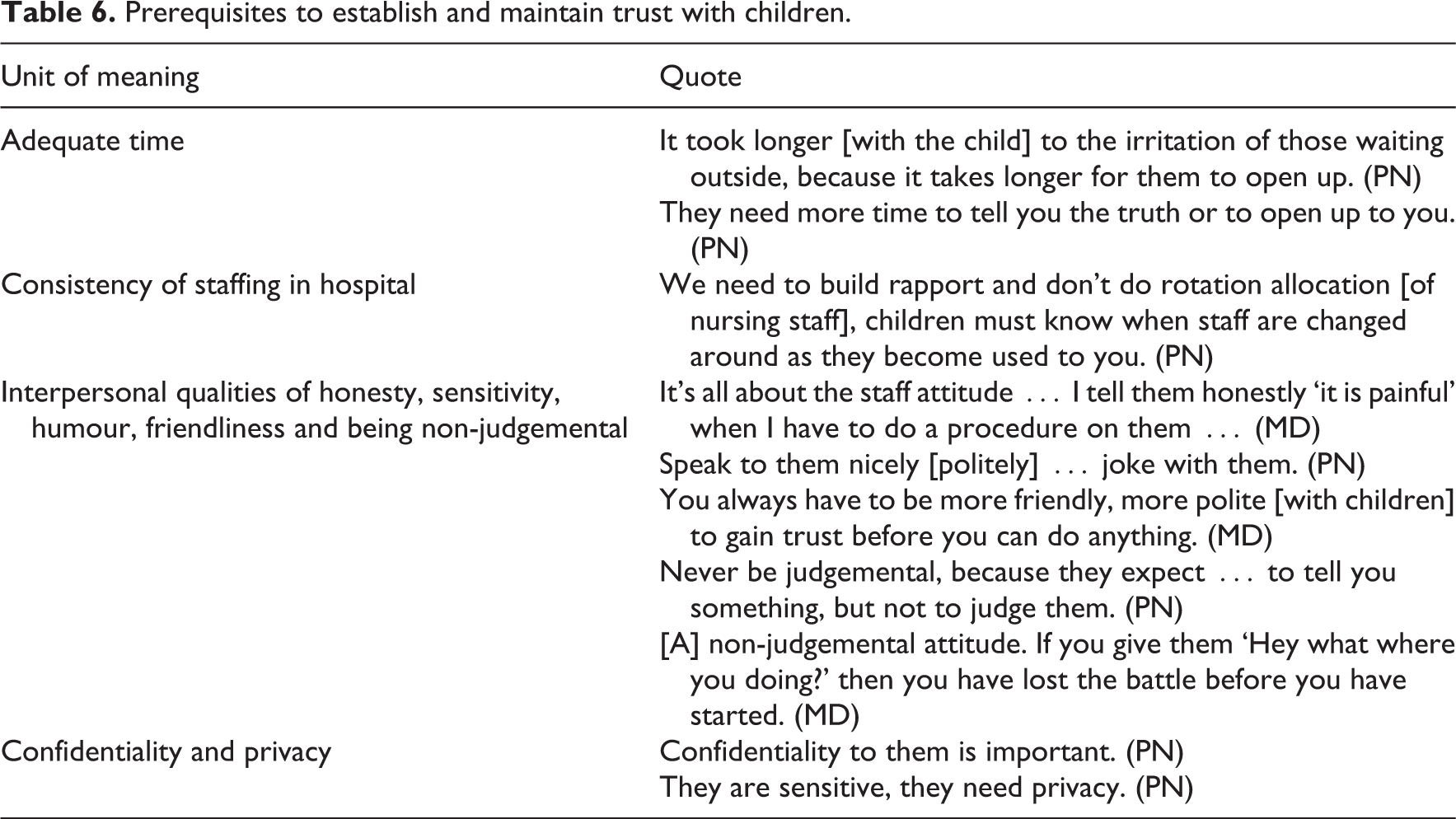
Establishing a trusting relationship with both the parent and the child was explained as a precursor to meaningful interaction with children and essential in the process of obtaining their consent. One participant explained, If you talk in a very formal way, above their heads [children], … they won’t really … feel that we care about them … they will consent without really understanding all the implications, but if they learn to trust you, then they will ask all the questions to know exactly what is going on with their bodies. (PN) Under twelve they have stranger anxiety, that’s number one, and when we come with an unfriendly face, you will not warm up to them in one second, so we need a more friendlier approach, and when you treat the parent with respect, ‘mommy are you fine?’ and start working with mommy … then go to the child, the child can now say ‘okay this person is supposed to be a doctor or a nurse I don’t have to be afraid as she is talking to my parent’ … its winning the trust for both the mother and the child for [the] under twelve [year old child]. (MD)
Prerequisites to establish and maintain trust with children.
When giving information to children, healthcare providers explained that they did so at the appropriate level for the child, repeated the information and made use of peer group discussions. Information given was often about treatment and the importance thereof. Some comments were ‘… when they get medication, you must teach her if she is getting antibiotics …’ and ‘… you tell these children about the importance of treatment, if you don’t take treatment, you will come back again …’ (PN).
Healthcare providers stated the importance of giving information on the child’s level, this included in a language understandable to the child, and on the child’s social and cognitive level and by reinforcement of the information. Some of the healthcare providers cautioned against the use of age to determine the level of information as children’s experiences and social contexts also played a role. As one healthcare provider explained, ‘[One] child develop[s] very fast according to the stages [of development] and the other [child] develop[s] very slow’ (PN).
Information had to be adapted not only to the child’s level of development but also to their informal language: ‘Use the language they use [on] the street so that they [connect] with you. Don’t use those sophisticated medical terms … even your English must be simple’ (PN).
Healthcare providers explained that using peer group education when sharing information is valuable and that children often accessed health services with their peers explained by healthcare providers as follows: ‘They normally come in groups; you find they are 3 or 4’ (PN) and ‘Children tend to come to facilities in groups and healthcare providers were happy to talk to them together or provide education or information in a group’ (PN).
Information was reinforced though repetition and the use of other sources of information such as pamphlets, posters and plays. The following quotes provide evidence for these sentiments: ‘Talking and talking and talking to them just reinforcing information all the time’, ‘[give information] in the form of an act or a play or something they understand’ and ‘show them posters’ (PN).
The practices implemented by healthcare providers when assessing children’s capacity to consent included investigating their history and social circumstances. Different yardsticks were used for assessment which was at times based on intuition. Healthcare providers explained how children’s social circumstances informed them about a child’s understanding of health conditions. One healthcare provider explained that, how she concluded that a child understood the condition as his or her parent had died of HIV: ‘If the child is less than 12 years but she is matured … she comes here and […] tells you that “my mother or my parent [is] dead because of HIV” then you can see that this child [has] knowledge about HIV’.
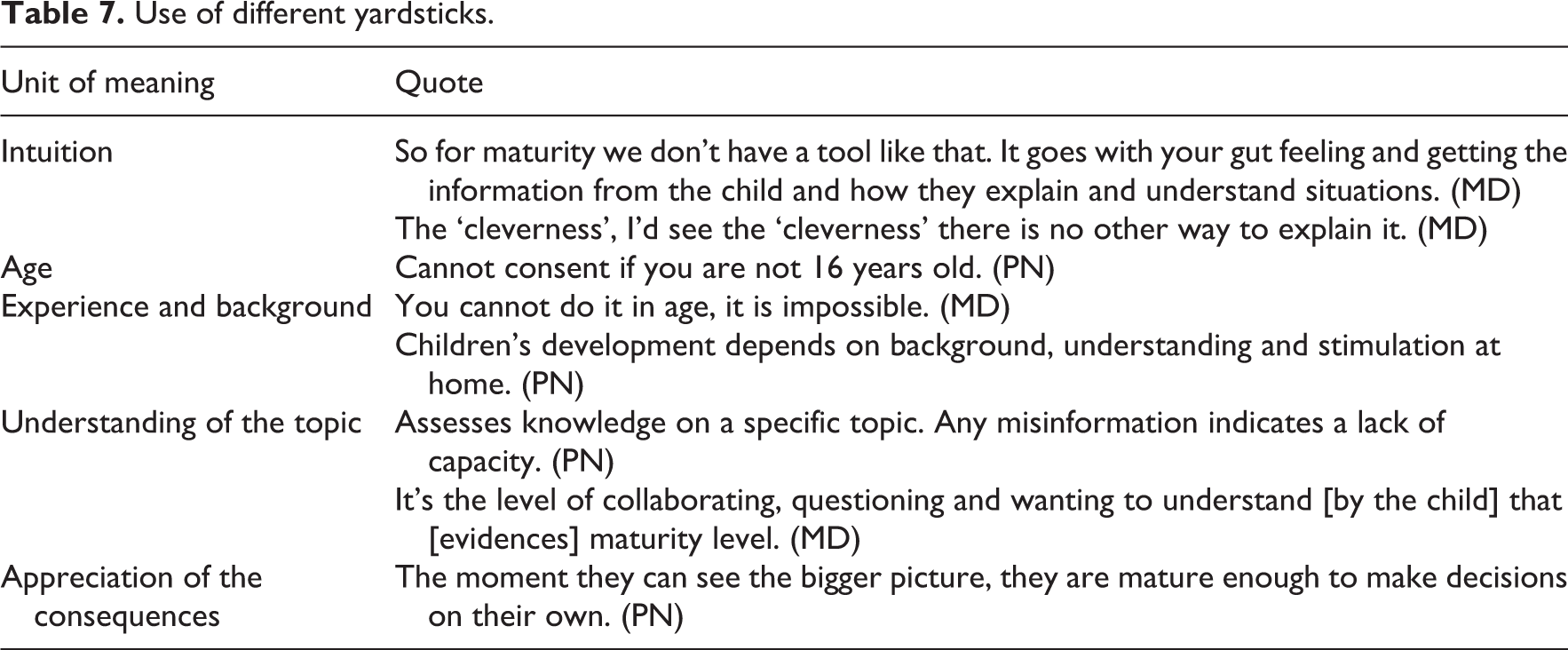
Healthcare providers used different yardsticks when assessing children’s capacity to consent, namely, intuition, age, experience and background, understanding of the topic and appreciation of the consequences. Supporting quotes for these units of meaning are summarised in Table 7.
Use of different yardsticks.
Discussion
Inconsistent implementation of consent laws was evidenced in this study by the different degrees of implementation and different yardsticks used to assess a children’s mental capacity during the consent process. The use of intuition and age as a yardstick is consistent with a study by Hein et al. 11 who proposed that intuitive assessments, due to the lack of an objective assessment tool, is influenced by the age prescribed by law.
Obtaining consent from parents, regardless of the current consent laws, is a practice described by Crosbie 28 as related to health professionals’ anxiety about potential litigation, which leads to defensive practices by obtaining consent from parents or guardians regardless. However, when the consent process with children is conducted correctly, it actually serves as protection from criticism, complaints and lawsuits. 3 On the other hand, if, due to misinformation, a healthcare provider allows a child to consent without the capacity to do so, the child could be burdened with a decision with which he or she might not be ready to deal with 4 and the consent would not be valid. The benefit, when including children in decision-making according to their maturity, is that they are able to practise and develop their decision-making skills and are more inclined to adhere and cooperate with treatment requirements. 4,29
Limited knowledge and misinformation contributed to inconsistent and incorrect practices in obtaining consent from children in this study. Perceptions, personal frames of reference and an obligation to protect influenced healthcare providers’ practices of obtaining consent from children. Attitudes and perceptions influenced behaviour, and in this case their behaviour when assessing children’s decisional capacities. 21 ‘These perceptions and beliefs are grounded in healthcare providers’ own parenting experiences 19 and their own religious, demographic and socio-cultural backgrounds 22 of which they should be mindful when interacting with children.
Limited time, due to human resource limitations, is a global concern in health service delivery. Sometimes when health services are provided to children, more time is needed to build a trusting relationship, to share information and engage the child in the process of decision-making. 30 Staffing levels in hospitals and clinics should consider the time related to seeing children and ensure that healthcare providers with specific skills in communicating and assessing children’s cognitive functioning and mental health are part of the multi-professional team. The need for a standard guideline, expressed by participants in this study, is confirmed by Hein and colleagues. 11,22 Guidelines should, however, allow flexibility as Alderson 31 cautions that protocols and regulations could in fact serve as constraints that could limit the options healthcare providers are able to offer children. In addition, with the already constrained resources, the burden of performing capacity assessments using a specific instrument could burden children, healthcare providers and the health system. 32
Assessment of children’s capacity to consent was described by healthcare providers to have three essential components, namely, a trusting relationship, providing of information and discussion, and assessment of children’s decisional capacity. This is confirmed by Alderson 3 who stated that information and assessment go hand in hand and that children’s capacity to consent is a reflection of healthcare providers’ abilities to inform children and support them in their decision making.
Study limitation
The study was contextual and exploratory in nature and cannot be generalised; however, findings might be transferrable to other contexts. The opening questions, ‘please tell me about your experience with obtaining consent from children’ and the first probe ‘How do you go about obtaining consent from a child’ could have been leading implying that healthcare providers did obtain consent from children. A more open-ended question would be to ask, ‘When, if ever, do you go about obtaining consent from a child?’
Conclusion
Inconsistent practices in the implementation of consent laws have the potential to violate children’s rights to bodily and psychological integrity, access to health services and having their opinions heard and be taken into consideration. Obtaining consent from children is a responsibility and requires attitudes, knowledge and skills to practice safely within the legislative and ethical framework of the healthcare providers’ scope of practice when obtaining consent from children. Not all healthcare providers are adequately prepared to do children’s capacity assessments. They require adequate training, multi-disciplinary support and clear guidelines on the implementation of consent laws and mental capacity assessments.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on the research supported, in part, by the National Research Foundation of South Africa for the grant, Unique Grant No. 84260. Any opinion, finding and conclusion or recommendation expressed in this material is that of the authors and the NRF does not accept any liability in this regard.