
Abstract
Background:
Moral distress occurs when nurses experience ethical dilemmas. Issues related to these dilemmas are addressed in some nursing education courses. Nurses’ reaction to dilemma such as moral distress is relatively less noticed.
Objective:
This study aimed to identify and describe the various types of perceptions of moral distress exhibited by nurses.
Research design:
This study applied Q methodology to explore the perspectives of nurses regarding moral distress. Data were collected in two stages. First, in-depth interviews were conducted to collect nurses’ opinions. Sentences that best fit the concepts of moral distress were extracted for the construction of Q statements. Second, nurses subjectively ranked these Q statements so that the relevant severity of moral distress could be determined using Q sorts. The study participants were nurses at a regional teaching hospital in northeast Taiwan. A total of 60 participants were invited to rank 40 moral distress Q statements.
Ethical considerations:
The study protocol was approved by the institutional review board of National Yang-Ming University Hospital. Only the participants who signed an informed consent form participated in the study. The respondents’ right to withdraw from the study was respected.
Findings:
Five types of responses were identified regarding the nurses’ perspectives. These types were “conflict with personal values,” “excessive of workload,” “curbing of autonomy,” “constraint engendered by organizational norms,” and “self-expectation frustration.”
Conclusion:
The findings regarding nurses’ experiences of moral distress can be used to construct multifaceted policies and solutions and to incorporate ethical education in training programs.
Introduction
Ethics are especially relevant to nursing care and affect all areas of professional nursing. The main purpose of nursing is the provision of high-quality care for patients. However, the complexity of the healthcare environment has increased as technology and medicine have advanced. Nurses operate in a high-pressure environment and receive multiple requests from patients, patients’ families, medical teams, and hospital management. Furthermore, nurses regularly face complex practice-based ethical decisions. 1 A lack of congruence between practices and values causes ethical dilemmas for nurses, thereby compromising their ability to provide high-quality and compassionate care. An ethical dilemma is characterized by a conflict of values; therefore, a solution to a dilemma usually entails compromising personal values. 2 When nurses are obliged to compromise their values, they experience moral distress. In addition, studies reveal that nurses are not well equipped to address ethical dilemmas and tend not to think critically when making ethical decisions. 3 When nurses are confronted with ethical dilemmas under conditions of limited resources and time pressure, their moral distress intensifies.
Some nursing courses address issues related to ethical dilemmas. However, nurses’ responses to dilemmas such as moral distress have seldom received attention. Narvaez 4,5 has stated that the dominant moral development theories often ignore the influence of the unconscious and of emotions and focus more on deliberative reasoning and rule-based morality. According to Narvaez, 4,5 emotion does not occur without thought and most thoughts evoke emotion. The importance of understanding nurses’ perceptions of moral distress is therefore apparent.
Jameton 6 described moral distress as arising “when one knows the right thing to do, but institutional constraints make it nearly impossible to pursue the right course of action.” Moral distress is a negative state of painful psychological imbalance experienced when nurses wish to make a moral decision but cannot act accordingly because of real or perceived institutional constraints. 7,8 When healthcare providers believe that they cannot preserve all interests and values, a discrepancy occurs and they are likely to experience troubled consciences as a result. 9 Consequently, nurses find themselves in situations that require them to compromise between their ideal conception of healthcare and reality; their inability to satisfactorily resolve such a situation results in moral distress. 2
Moral distress is frequently observed in nurses 10 and results in negative consequences such as compromised nurse and patient well-being, fatigue, 11 high turnover rates, staff shortages, 12 alienation from patients, 13 negative feelings, psychological imbalance, job dissatisfaction, 14 severe physical or mental harm, and possibly the burnout of nurses. 15,16 Hence, moral distress is a topic that deserves thorough attention. To prevent adverse consequences resulting from moral distress, we must first understand nurses’ perspectives on moral distress and the types of moral distress that occur.
Objectives
This study identified and described nurses’ perceptions of moral distress and proposes appropriate solutions based on the results.
Method
Q methodology
William Stephenson 17 introduced Q methodology in 1935. The technique combines qualitative and quantitative approaches; participants’ attitudes toward subjective topics are analyzed by categorizing the participants according to their opinions. 18 The participants are requested to determine the magnitude of what is meaningful from their perspective. The key to this approach is to consider data with regard to individual participant response patterns, instead of seeking patterns among several participants. 19 Akhtar-Danesh et al. 20 reported that Q methodology was useful in qualitative nursing studies and that it emphasized the exploration and comparison of subjective perceptions. Q methodology sorts Q statements in accordance with respondents’ viewpoints of a subjective issue. Through this procedure, personal viewpoints are evaluated systematically according to personal experience. 21
Moral distress is an inevitable part of the ethical development process in nursing; however, it may prevent nurses from developing ethical maturity. Because of the effectiveness of Q methodology, it is appropriate for use in investigating opinions regarding moral distress in nursing.
Q statement development
Developing Q statements is an essential part of Q methodology. 22 Such statements can identify problems that researchers consider to be related to a specific study. In this study, Q statements were obtained from the following sources: (a) studies related to moral distress, (b) opinions from in-depth interviews with respondents from various nursing backgrounds (i.e. their descriptive sentences that best fit the concepts of moral distress), and (c) experts and scholars with related specialties who were invited to examine the appropriateness of the Q statements.
Participant selection (P sample)
We selected nurses at a regional teaching hospital in northeastern Taiwan. The inclusion criteria were as follows: (a) age ≥ 20 years, (b) more than 1 year experience of clinical nursing, (c) a general awareness and understanding of nursing ethical issues, and (d) voluntary participation in this study and signing of informed consent documents. A total of 15 nurses were interviewed to obtain their opinions for developing Q statements. In all, 60 nurses participated in Q sorting. Q methodology is a type of exploratory factor analysis and is not designed for inferring the characteristics of an entire population. 23 A purposive sample of nursing staff was recruited to obtain various perspectives on moral distress. The criteria applied in selecting staff members were based on work units (medical, surgical, and special ward). At least one participant was recruited from each work unit. The purposive sampling strategies employed in this study were intended to address the heterogeneity rather than the representativeness of the population. According to previous research, 40–60 participants is a suitable number of participants. 24 Therefore, a sample size of 60 was selected.
Data collection
A two-stage data collection design was adopted. During the first stage, in-depth interviews were conducted to obtain a sample of nurse perceptions related to moral distress. Interviews were conducted from January to February 2014. The interview duration for each respondent was approximately 60 min. Data obtained from the interviews were analyzed using ATLAS v5.2 qualitative analysis software. Less crucial sentences, or those with less representation, were omitted. Those that optimally fit the concepts of moral distress were extracted for constructing Q statements. In May 2014, nurses were requested to subjectively rank these Q statements so that the relevant severity of moral distress could be established using Q sorts.
We developed an e-platform to enable participants to perform Q sorting online. An example of the user interface was demonstrated in our previous study. 25 The screen was divided into two panels: the left panel displayed a list of the final Q statements and the right panel showed the scoring system in the form of a Q-sort grid. In total, 40 Q statements were selected and scored on the basis of nine degrees, ranging from −4 (the least distress) to +4 (the most distress), with 0 representing neutrality (Figure 1).
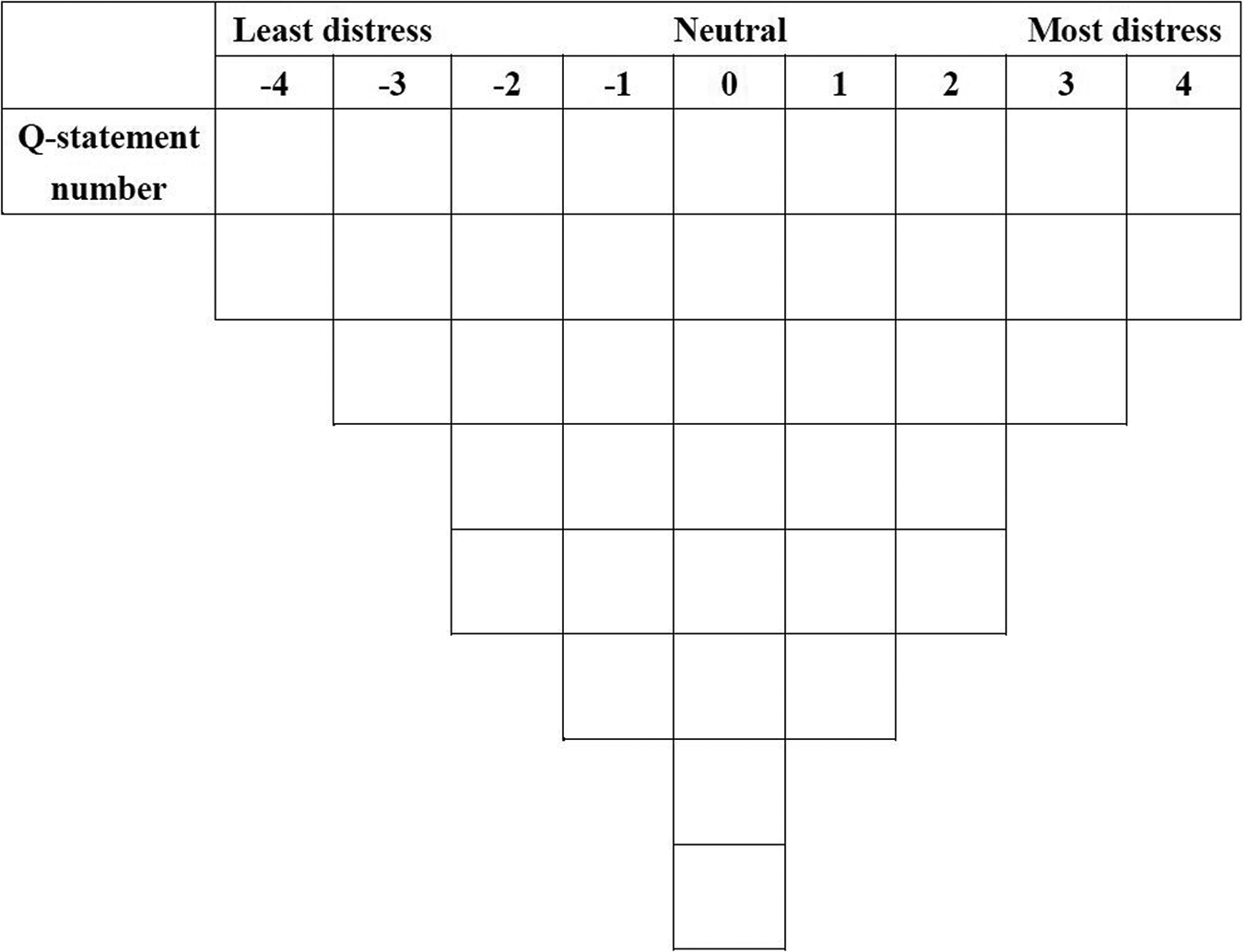
A Q-sort grid for rank-ordering Q statements.
Validity
The content validity index (CVI) was adopted to establish the validity of Q statements. 26 Six experts specializing in either nursing ethics, nursing education, or Q methodology were invited to assess the Q statements for content validity.
Q statements of CVI > 0.8 were selected. The assessment results were used as references for constructing Q statements. After assessment by the experts, words and sentences that were semantically confused or ambiguous were corrected. According to the experts’ feedback, 40 Q statements related to moral distress were obtained.
Data analysis
The data were analyzed as follows: 1. Data on nursing staff background
After completing data collection, we employed SPSS 20.0 (IBM Corp, Armonk, NY) to perform descriptive statistical analysis. Characteristics of nursing staff background were determined in terms of percentage, mean, and standard deviation. Items used were gender, age, degree of education, position of employment, service divisions, and total years of work experience.
2. Interview data
After recording interviews with 15 nursing staff, we transcribed the records. Files of the transcripts were loaded into ATLAS v5.2 to identify potential Q statements.
3. Q-sort results
The Q-sort results were inputted to PQMethod Version 2.35. 27 The data were analyzed using principal component analysis and varimax rotation. The procedure was as follows: (a) principal component analysis, (b) determination of the number of factors, (c) varimax rotation, and (d) classification of respondents by the number of load factors.
Ethical considerations
Approval was obtained from the Institutional Review Board of National Yang-Ming University Hospital, Taiwan (2013B010). After ethical approval was received, the nurses who met the inclusion criteria were sent an invitation letter. The research team visited potential participants at their hospitals and arranged appropriate times to demonstrate the Q-sort procedure. The participants were given a packet containing a study information sheet, Q-sort instructions, a list of Q statements, and personal account names and passwords for logging in to the research web page. All of the participants provided informed consent before participating in the study. Respondent names were substituted with a code and personal information was kept strictly confidential. The respondents’ right to withdraw from the study was respected.
Results
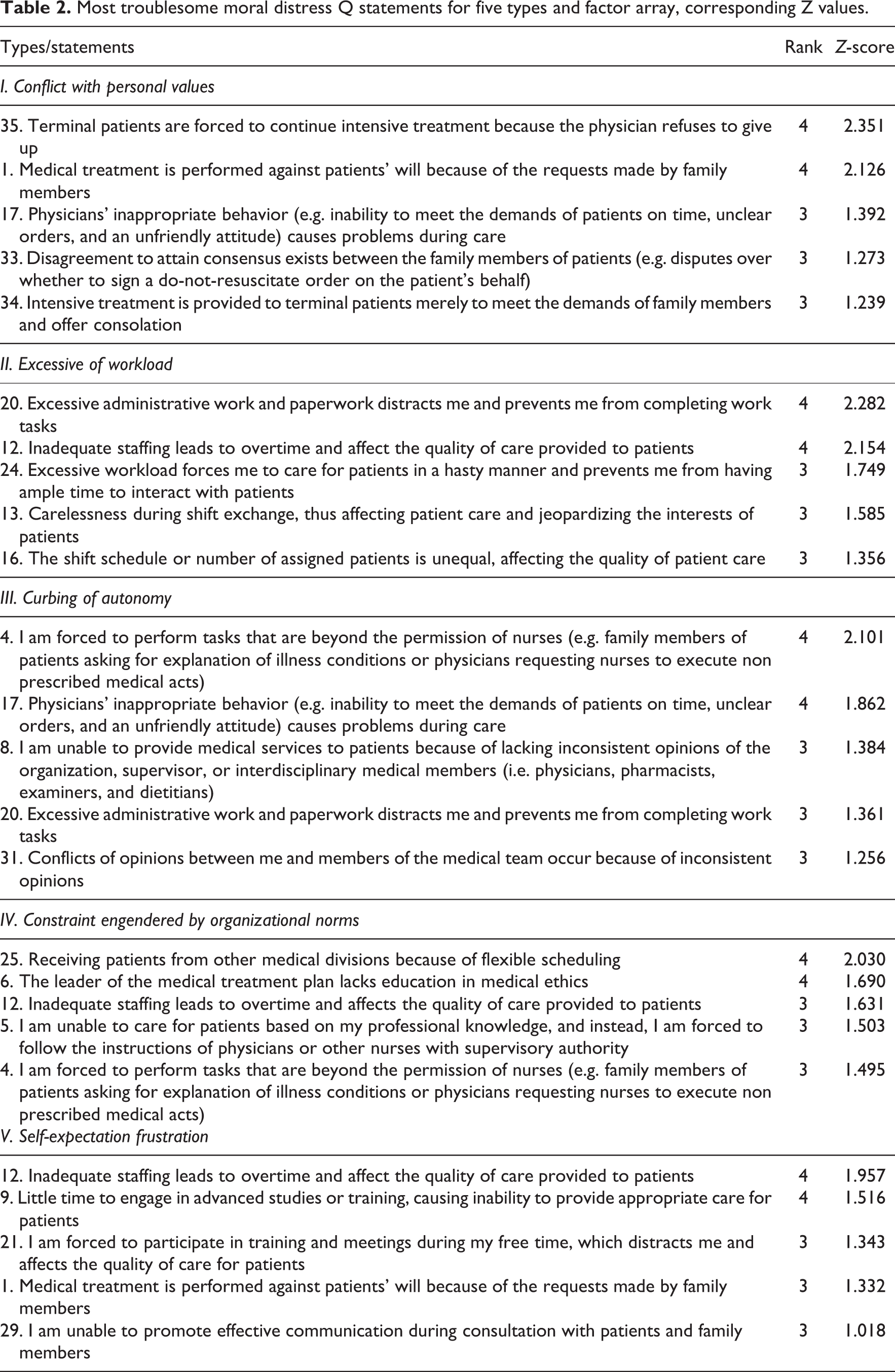
We obtained five response types regarding the nurses’ perspectives; these corresponded to five types. A total of 52 participants were classified into the five types, which were as follows: conflict with personal values (19 nurses), excessive of workload (11 nurses), curbing of autonomy (12 nurses), constraint engendered by organizational norms (8 nurses), and self-expectation frustration (2 nurses). The background information presented in Table 1 indicated that the nurses experiencing constraint engendered by organizational norms were relatively young (average age = 31.5 years) and possessed limited nursing experience (average = 10 years). By contrast, nurses in the self-expectation frustration group were relatively old (average age = 44.5 years) and had been nurses for a longer period (average = 21.5 years). Most of the nurses in the curbing of autonomy and self-expectation frustration groups were administrators. Finally, most of the nurses in the conflict with personal values and curbing of autonomy groups served in special wards (63.1%–75.0%). Table 2 shows a comprehensive comparison of the most troublesome Q statements. The factor array and Z value of each statement determined the distinguishing statements (p < .05).
Background information of nurses.
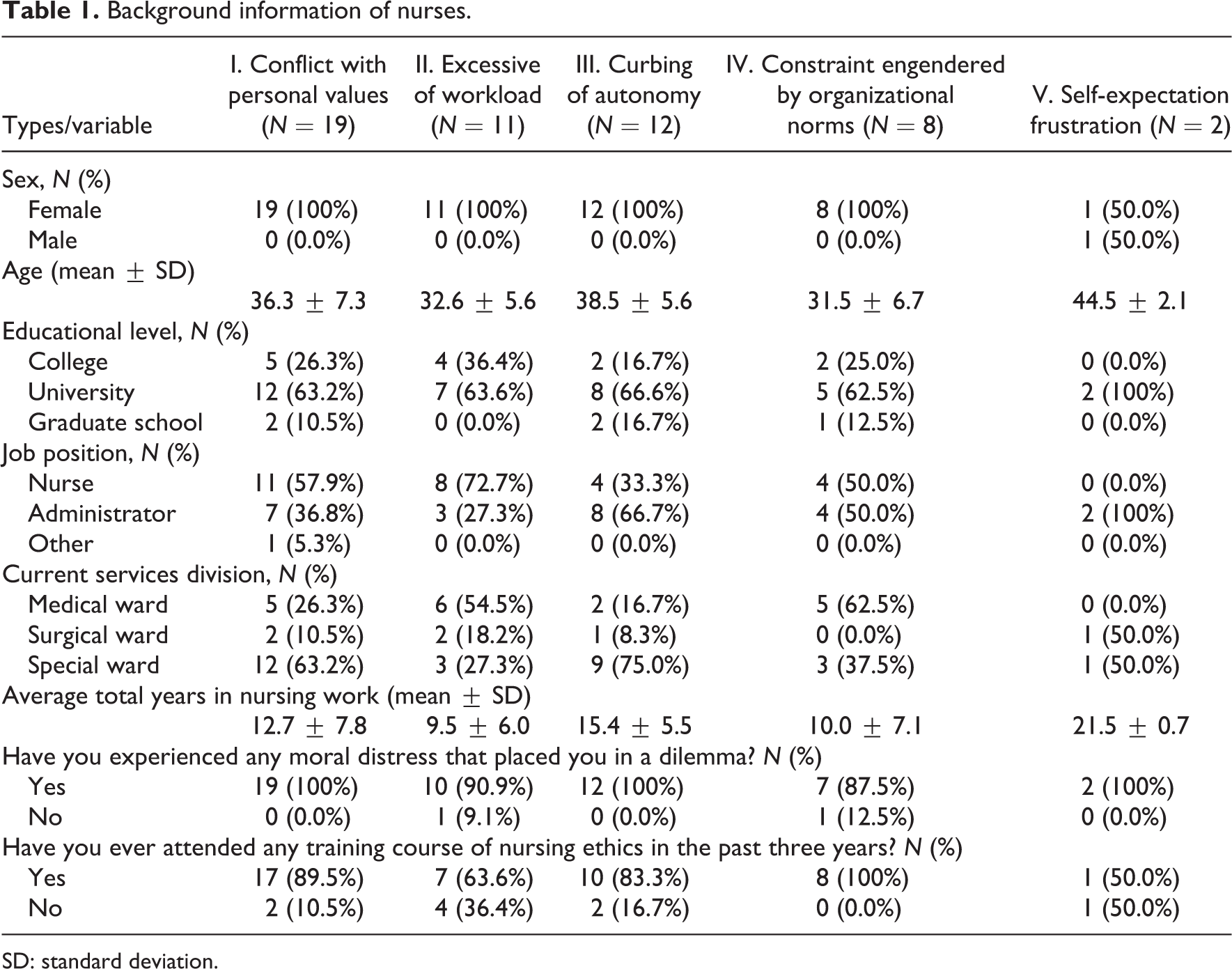
SD: standard deviation.
Most troublesome moral distress Q statements for five types and factor array, corresponding Z values.
Type 1: conflict with personal values
This type comprised 19 nurses. All of them were female (average age = 36.3 years). Type 1 respondents stated that in the process of care they encountered situations that conflicted with their personal values, such as requests necessitating following doctors’ orders or family requests and ignoring patients’ wishes, administering treatment that they did not wish to provide, administering aggressive treatment against their will because of physician or family member recommendations, and being unable to provide satisfactory hospice care to terminally ill patients. Therefore, dilemmas with no clear solution emerge among physicians, patients, and family members. Furthermore, when disagreement exists among family members, nurses must assume the role of coordinator and communicator. In such situations, regardless of the outcome, not all family members can be satisfied with the treatment of the patient. Therefore, obtaining a balance between the values of the family and nursing staff is difficult. Illustrative comments loading on this factor included the following: We felt distressed, because death was inevitable for this patient but the nephrology specialist insisted on aggressive treatment.
Type 2: excessive of workload
This type comprised 11 nurses. All of them were female (average age = 32.6 years). Type 2 respondents stated that in the course of care, in addition to basic clinical care, they were required to complete excessive general administrative tasks and written assignments. Furthermore, the current shortage of nursing professionals resulted in a higher workload for each nurse, necessitating overtime work. Nurses were forced to provide care as quickly as possible and had insufficient time to provide more comprehensive patient treatment. The increased workload caused loss of concentration and affected the quality of the patient care the nurses were able to provide, thus producing moral distress. Illustrative comments loading on this factor included the following: I felt unable to adequately perform the administrative tasks required by the organization. They were too demanding, disrupted my concentration, and prevented me from learning thoroughly.
Type 3: curbing of autonomy
This type comprised 12 nurses. All of them were female (average age = 38.5 years). Type 3 respondents stated that nurses were required to perform tasks at the request of physicians or families that conflicted with their own opinions and that they therefore experienced moral distress. Furthermore, they were unable to provide certain medical services to patients because of inconsistent opinions from the organization, supervisors, or interdisciplinary medical staff (i.e. physicians, pharmacists, examiners, and dietitians). They were not free to make decisions in accordance with their professional knowledge and therefore experienced moral distress. Illustrative comments loading on this factor included the following: It was not absolutely certain that this was what I should do, and this action was quite contrary to my own conscience. What should I do if something goes wrong?
Type 4: constraint engendered by organizational norms
This type comprised eight nurses. All of them were female (average age = 31.5 years). Type 4 respondents stated that because the beds in their wards could be adjusted flexibly, patients from other wards were transferred into their wards, thus increasing the complexity of managing patients because of the wider variety of disease attributes. Although nurses must act in accordance with organizational rules and norms, patients transferred from other wards often required treatment beyond nurses’ specialty and had diseases the nurses were not familiar with, resulting in reduced quality of care and moral distress. The shortage of nursing professionals necessitated demanding overtime work. Consequently, nurses were constrained to act only in accordance with organizational norms and forced to provide care to a higher number of patients, thus affecting the quality of patient care. Illustrative comments loading on this factor included the following: I am so overwhelmed by the workload and the many different conditions of the patients in the wards.
Type 5: self-expectation frustration
This type comprised two nurses, one male and one female (average age = 44.5 years). Type 5 respondents stated that because work occupied most of their time, they had little time to engage in advanced studies and training, resulting in an inability to provide appropriate care for patients and thereby causing moral distress. Furthermore, they were required to spend their leisure time attending seminars held by the hospital and ward meetings, resulting in a lack of sufficient rest and thus negatively influencing their work performance. This is a vicious cycle that prevents nursing staff from realizing self-expectation because they are unable to provide high-quality care for patients. Illustrative comments loading on this factor included the following: There are only seven or eight days off in a month. We all have family and children. It is not possible to take those days off to take classes or something like that. You definitely can’t spare extra time to do advanced study.
Discussion
This study identified five types of shared perspective, thereby enabling nurses’ perspectives on moral distress to be analyzed. Clustering nurses into such types facilitates determining a strategic approach for effectively assisting nurses who experience moral distress. The five types were as follows: conflict with personal values, excessive of workload, curbing of autonomy, constraint engendered by organizational norms, and self-expectation frustration.
This study contributes to the understanding of the moral distress experienced by nurses. Furthermore, it enables the development of policies and solutions that are appropriate for nurses with specific characteristics and requirements. This can facilitate the development of educational planning and ethical training. The Q method is a technique for examining personal perspectives on topics by categorizing participants according to their opinions. 18 The approach has seldom been used for exploring moral distress among nurses. The current participants were asked to decide the magnitude of what was meaningful from their perspective (rather than patterns being sought within a sample of nurses), 19 and five types of shared perspectives were identified. These findings contribute to the field by revealing different perspectives on moral distress.
The respondents in this study comprised nursing staff from various divisions. Of the five moral distress types, we determined that type 1 (conflict with personal values), type 3 (curbing of autonomy), and type 5 (self-expectation frustration) tended to be intrinsically caused. By contrast, type 2 (excessive of workload) and type 4 (constraint engendered by organizational norms) tended to be caused by external factors.
Investigating the background of the type 1 respondents, we found that, regardless of their educational level and title, they were likely to experience moral distress related to conflict with personal values. We evaluated the distribution of the nurses on the basis of the departments they were currently assigned to. Nurses working in medical wards and intensive care units accounted for most of the study population. Patients in medical wards and intensive care units exhibited diverse conditions and degrees of severity, which increased the difficulty of decision making. We inferred that this exposed nurses to moral distress regarding conflicts with personal values. The results of former studies are consistent with this finding. 28
The average age of the type 2 respondents was slightly lower than that of all the respondents. Younger nurses’ unfamiliarity with clinical routines, written assignments, and other administrative affairs was caused by their having less experience. Being overwhelmed by the workload was likely to trigger their moral distress. This result is confirmed by those of previous studies. 29
Exploring the background of the type 3 respondents revealed that nearly 70% of them were administrative supervisors. Administrative supervisors presumably had to resolve affairs at a higher level and address staff-related problems. Assuming such bridging roles, they must make appropriate decisions to counter these problems. However, this was usually difficult.
Respondents belonging to type 4 exhibited the lowest average age among all respondents. Some of them had been engaged in clinical care for only 2 years. They possessed less experience compared with the other respondents. We conclude that nursing staff who are younger and have less working experience are prone to feel constrained by organizational norms, resulting in moral distress.
Type 5 comprised only one male and one female respondent. This type had an older average age compared with the other types and the two respondents were head nurses. We conjecture that these participants wished to act in a manner appropriate for their superior role. They believed that having self-expectations and requirements for work was necessary. They felt distressed when they could not achieve set goals.
Ulrich et al. 1 stated that (a) protecting patient rights, (b) autonomy and informed consent to treatment, (c) staffing patterns negatively affecting work, (d) advanced care planning, and (e) surrogate decision making comprise the most frequent causes of moral distress for registered nurses (RNs). Eizenberg et al. 30 described the causes of moral distress in nursing staff as follows: (a) problems caused by work relationships among staff, (b) problems attributable to lack of resources, and (c) problems caused by time constraint pressure. Redman and Fry 31 determined that the most common ethical issues are (a) protecting patient rights and human dignity, (b) determining whether to respect informed consent to treatment, (c) determining whether to use physical or chemical restraints, (d) providing care with possible risks to RN health, (e) determining whether to follow advanced directives, and (f) staffing patterns that limit patient access to nursing care. The findings of this study mainly emphasize individual characteristics and are divided into five moral distress types. These findings are consistent with those of previous studies. 1,30,31 However, we determined that self-expectation frustration has been mentioned less frequently in previous studies. Although only two respondents in this study were classified into this type, the moral distress related to this type can be further investigated. Moreover, the Q statements in this study were obtained from qualitative interviews and accurately represent the respondents’ working experience. Therefore, the questionnaires employed in this study more closely corresponded with real experiences compared with questionnaires used in previous studies.
Most quantitative studies of ethical issues have used a moral distress scale and ethical issue rating scales. 16,32,33 These studies are likely to have ignored region-specific clinical moral distress types by applying ethical scales that did not account for variations in customs and cultures. In addition to conducting qualitative interviews for examining the feelings and emotional reactions of nursing staff when they experience moral distress, we requested all respondents to simultaneously compare, rank, and score Q statements according to degree of distress. These Q statements were obtained from analyzed interview data. Through this method, we were able to review data to determine the respondents’ personal experiences and viewpoints of moral distress. Furthermore, we could classify the respondents into several types on the basis of the analyzed results, revealing distinctive properties and causes of moral distress specific to members of a type. These results can facilitate implementing appropriate ethical education and training programs that fit individual requirements.
Limitations and suggestions
The respondents of this study were selected from a regional teaching hospital in northeastern Taiwan. Through Q methodology, nurses exhibiting different characteristics and respective forms of moral distress were identified accurately. However, the characteristics of the nurses and the moral distress experienced varied because of the diverse attributes of their hospitals (e.g. level, region, labor distribution, numbers of beds, and disease types). The diversity of the hospitals participants are drawn from should be considered before applying Q methodology. However, when applied appropriately, Q methodology can be an effective tool for the identification of different types of nurses and the respective types of moral distress that occur in each hospital.
Of the 60 respondents in this study, only one was male. Therefore, we were unable to obtain a comprehensive male perspective and related data. The number of male respondents should be increased in future studies to obtain more comprehensive viewpoints of moral distress in both genders. We employed a categorized assessment structure ranging from −4 to +4. The results may have varied because of the varying structural design. Additional interviews could be conducted after the respondents complete the Q-sort process to facilitate interpreting the quantitative analysis. This study involved collecting Q statements through qualitative interviews. Q statements can serve as the foundation for developing a quantitative questionnaire on moral distress. Finally, the results of this study can be grouped on the basis of the individual participant. Because nursing staff belonging to various types tend to have distinctive moral distress characteristics, ethical education and training should be designed according to those distinctive characteristics instead of general principles.
Conclusion
Moral distress is an inevitable part of the ethical development process within nursing practice and may prevent nurses from or slow them in developing necessary ethical maturity. Our findings illustrate the variety of perspectives on moral distress existing among nursing staff in clinical situations. Identifying these views can advance the understanding of nurses’ experience of moral distress. The five identified types can facilitate the development of customized strategies for coping with distress. To prevent the negative consequences of moral distress, it is crucial to motivate hospital managers to acknowledge the differences among staff. If hospitals apply these perspectives to adjust work allocation and operational methods, then the mobilization of resources can be arranged more specifically according to the various types of nurses. Different methods of counseling that target each type should be developed to equip nurses with the ability to resolve moral distress.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Science Council, Taiwan (NSC 102-2511-S-010-005).