
Abstract
Background:
Previous research has linked missed nursing care to nurses’ work environment. Ethical climate is a part of work environment, but the relationship of missed care to different types of ethical climate is unknown.
Research objectives:
To describe the types of ethical climate in adult in-patient cancer care settings, and their relationship to missed nursing care.
Research design:
A descriptive correlation design was used. Data were collected using the Ethical Climate Questionnaire and the MISSCARE survey tool, and analyzed with descriptive statistics, Pearson’s correlation and analysis of variance.
Participants and research context:
All nurses from relevant units in the Republic of Cyprus were invited to participate.
Ethical considerations:
The research protocol has been approved according to national legislation, all licenses have been obtained, and respondents participated voluntarily after they have received all necessary information.
Findings:
Response rate was 91.8%. Five types identified were as follows: caring (M = 3.18, standard deviation = 1.39); law and code (M = 3.18, standard deviation = 0.96); rules (M = 3.17, standard deviation = 0.73); instrumental (M = 2.88, standard deviation = 1.34); and independence (M = 2.74, standard deviation = 0.94). Reported overall missed care (range: 1–5) was M = 2.51 (standard deviation = 0.90), and this was positively (p < 0.05) related to instrumental (r = 0.612) and independence (r = 0.461) types and negatively (p < 0.05) related to caring (r = −0.695), rules (r = −0.367), and law and code (r = −0.487).
Discussion:
The reported levels of missed care and the types of ethical climates present similarities and differences with the relevant literature. All types of ethical climate were related to the reported missed care.
Conclusion:
Efforts to reduce the influence of instrumental and independence types and fostering caring, law and code, and rules types might decrease missed nursing care. However, more robust evidence is needed.
Keywords
Introduction
The relationship of organizational environment with employees’ behavior has been confirmed experimentally, very early 1 with the function B = f (P × E), explaining that behavior (B) corresponds to a person (P) who interacts with the environment (E). Nowadays, the organizational climate which refers to the employees’ perception of the values, beliefs, and behaviors 2 is considered by almost all professional disciplines as one of the mechanisms that regulate employees’ behavior. 3 For example, it is broadly accepted that nursing practice is not solely influenced by each nurse’s decisions (micro-level) but additionally by organizational factors (meso-level) and the broader sociopolitical framework (macro-level). 4 Moreover, the nurses’ working environment has been associated with quality of care, mortality rates, 5 individualized patient care, 6,7 and missed nursing care. 8 Nevertheless, nurses may work in different working environments either in the community or in the hospitals (in different units) that may have different climates and/or sub-climates. The ethical climate is considered a part of the overall working environment 9,10 or a sub-climate of the whole organizational climate that refers to the employees’ collective perception of what is ethically acceptable within the context of an organization. 2 The ethical foundations of nursing call the nurses in any case to preserve human life; to protect the patients from harm; to respect human rights; 11 and to provide safe, high-quality, 12 dignified, compassionate, individualized, and comprehensive nursing care to patients without discriminations. 13 However, the prevailing ethical climate within their working environment may either facilitate or constrain nurses’ work. Indeed, competing forces within this context (e.g. competing values vs interests, personal values vs organizational values, and personal values vs values of others) may result in uncertainty regarding ethical decisions and may limit the ability for nurses to sustain their moral identity. 14
Moreover, finite resources or the unlimited nature of patients’ needs 15 –19 may lead to inability of nurses to provide all the needed care to their patients, a phenomenon characterized as rationing of care or missed care, 19,20 and considered increasingly prominent globally for all contemporary health professions. 15 –17,21 Its significance in nursing, however, lies in the fact that it may increase the risk of adverse patient outcomes, threaten patient safety, and reduce quality of care. 17,19 Thus, when resources are insufficient (e.g. poor practice environments and insufficient time), nurses may minimize the standards of care 18 or ration their attention across nursing activities or even across patients. 19,22 –24 Thus, certain activities such as patient mobilization and/or ambulation, patient hygiene, patient teaching, and emotional support were found in several studies to be omitted, 15 –17 or delayed, 20 or offered at a lower level of quality 18,22 in various clinical settings including cancer care units. 25,26 However, considering the ethical foundations of nursing, a zero tolerance for missed nursing care may be expected in any clinical environment, 8,18,26 while the phenomenon may contain an ethical element 22 that needs further examination.
Values, norms, beliefs, and habits shared by nurses in any clinical environment may be associated with their decisions when they ration nursing care. These elements that can lead to a common understanding of what is the ethically correct behavior and how ethical issues should be managed in a clinical environment in fact constitute its ethical climate. 9,27 The ethical climate is widely considered as an identifiable 10 part of the overall organizational environment 7,9,28 and as a dynamic construct 7 that can be modified 29 to improve the working environment 30,31 and guide nurses’ behaviors. Thereby the investigation of ethical climate is gradually becoming an important part of quality assessment in healthcare. 7,28 Some studies 3,29,31 –39 adopted a typology of ethical climate 9,10 and have examined the prevailing types of ethical climate in nurses’ workplace. Additionally, relationships of these types were found with organizational commitment and job satisfaction, 33,37 –39 teamwork, 29 staff turnover intention, 32 intent to leave job, 35 moral distress, 3 and nurses’ ethical behaviors. 34 Understanding the different ethical climate types that may exist in a particular care setting is important because any one of these types can influence in their own unique way how issues are identified and prioritized and what defines the existing process of decision making. 29
Since the quality of nurses’ practice environment has been linked to missed nursing care 8 and having in mind that ethical climate is a part of the overall working environment 2,9,10 as well as the results of our study of missed nursing care in cancer care units, as reported elsewhere, 26 this research further explores the phenomenon in this clinical setting. The understanding of how nurses perceive the different types of ethical climate in their workplace remains limited and explicitly less with regard to the cancer care setting. To the authors’ knowledge, only one published article 40 has examined the ethical climate of hospitals as it was perceived by 89 healthcare professionals responsible for the care of children with cancer. Moreover, no published studies were found that describe the types of ethical climate as perceived by nurses working in adult cancer care units and no study that attempted to relate these types with the perceived levels of missed nursing care.
This study contributes in the relevant literature by focusing on the association of missed nursing care with the types of ethical climate, as perceived by nurses working in adult in-patients cancer care (both oncology and hematology) units. Even allowing for the possible variability of ethical climate types at organization level, unit level, and job level of analysis, 9 one could expect that nurses working in the same unit will share the same ethical climate that give emphasis to the specificities faced by the cancer patients and their families, the complexities of their care needs, and the ethical challenges these needs pose on nurses’ role. The types of ethical climate may be related (or not) to the decisions of nurses when they ration nursing care.
Conceptual and theoretical framework
This study draws elements from the theoretical model for the types of ethical climate 9 and the Missed Care Model. 20 Victor and Cullen 9,10 developed the concept of ethical climate within organizations as “the shared perceptions of what is ethically correct behavior and how ethical issues should be handled in organizations,” 9 and this has also been informed in this study. Moreover, these scholars 9 devised a two-dimensional typology of ethical climate. The first (called ethical criterion) is based on the ethical theories 9,10 that may be considered when making decisions: egoism (if decisions are guided by personal interest), benevolence (if guided by the interest of as many as possible people), or principled (if guided by the adherence to essential principles). The second (locus of analysis) 9,10 includes three loci according to where the information guiding the decisions is received: individual locus of analysis (information comes from personal beliefs and values), local locus (when it is received by the surrounding environment such as organizational policies), and cosmopolitan locus (when it is received from the wider society outside the organization such as laws and regulations). 9,10,41,42 At the intersections of these two dimensions, they suggested nine a priori hypothesized types of ethical climate. 9 However, empirical testing indicated the existence for only six of them, 9 while only five (i.e. instrumental, caring, rules, law and code, and independence) appear frequently in organizations 10,41,42 including healthcare. 31 –33,35,36,39,43
Caring ethical climates is based on a common concern for the welfare for others 3,33,42 and encourage behaviors that yield the most positive result for the greatest number of people. 31,42 Instrumental ethical climates encourage decision making from a selfish standpoint 42 and of behaviors promoting self-interest or organizational interest. 31,33,42 Rules ethical climates is guided by an intense acceptance of local standards and regulations, such as codes of good practice and behavior 41,42 and by a clear expectation to follow the rules, procedures, and policies of the organization strictly. 33 However, in a law and code ethical climates, the compliance with external influences such as laws, external rules, professional standards, and codes of conduct is essential 33,42 and is required from everyone, over and above other factors. 37,39 Finally, in independence ethical climates, employees are expected to follow their own deeply held moral beliefs 33,39 to make decisions with minimal impact from external influences. 42
With regard to rationing of nursing care, a range of different definitions has been proposed 15 –18 such as missed nursing care or delayed care, 20 the withholding of, or failure to carry out necessary nursing tasks, 44 care needs not being met, 45 nursing care left undone, 46 unfinished care, 15 priority setting, 47 or care prioritization 23,24,48 that might occur when nurses are prioritizing care, within the context of scarce resources. This study principally adopts the term missed nursing care, but for ease of reference, also uses rationing of nursing care when it refers to the corresponding literature. Missed nursing care is defined as “any aspect of required patient care that is omitted (either in part or in whole) or delayed” 20 and is influenced by factors in the care environment, affecting nurses’ internal processes that guide them in deciding which nursing activity should be completed, should be missed, or should be delayed. 20 Similarly, rationing of nursing care was defined as “the withholding of or the failure to carry out all needed nursing interventions in the face of inadequate time, staffing or skill mix” (p. 885). 19
Missed Care Model 20 suggest that missed nursing care can occur at any stage of the nursing process and explains the internal processes and factors that guide nurses in deciding what care element should be given priority and thereby be completed, or else missed (omitted or delayed) until sufficient resources are available. Factors in the care environment (e.g. allocation of resources, demands for care, and relationships) that can either facilitate or inhibit nursing practice, characteristics of hospital units, and characteristics of nurses may all lead to the phenomenon. However, nurses’ decisions to complete certain care activities while omitting or delaying others is additionally influenced by the nurses’ intrinsic perceptions of processes such as team norms, decision-making practices and imbedded values, beliefs, habits, and attitudes, 20 according to which the nurses view their roles and responsibilities. 18
Aim of the study
This study attempts to describe the types of ethical climate as perceived by nurses working in adult in-patient cancer care units and explore whether there is any relationship between these ethical climate types and missed nursing care as reported by nurses on these units. More specifically, its objectives are as follows: To find out the different ethical climate types that are identified by nurses in cancer care units; To find out which type of ethical climate is prevailing; To investigate and describe the relationship (if any) between the identified types of ethical climate in cancer care units and the reported by nurses levels of missed nursing care.
Method
Design setting and participants
A descriptive correlation design was used. The research setting included all six oncology and hematology units in the Republic of Cyprus. One of these units is the only one available independent 15-bed hospice in Cyprus, providing exclusively palliative care to cancer patients and staffed by 20 nurses. This hospice is managed by a non-profit, non-governmental organization which is responsible for supporting cancer patients. Due to the limited bed capacity of this care unit, it is very common for the palliative care of patients with cancer to be provided also in all the five units of this study. These units are often utilized for patients at various stages of the cancer journey including those with advanced disease, those on active treatment and those requiring advanced symptom management or other needed care. Only some patients with cancer, who are having merely active treatment (e.g. chemotherapy), receive care in day care settings. Therefore, most patients that are often admitted in these six units cannot care for themselves and are depended on nurses to fulfill most of their needs. Four of the remaining five units (except the hospice) are small units (with bed capacity that ranges from 14 to 24 beds) and belong to the two larger hospitals of the country (one oncology and one hematology in each hospital). The number of nurses working in these units ranges from 21 to 31 nurses. The last care unit is an independent oncology center, with 40 beds and where 45 nurses are working to provide all the types of needed care to cancer patients. The nursing delivery system across all the six units is the team nursing while each nurse is usually responsible for the care of 6 to 10 patients per shift. All registered nurses, working in these units (N = 171) who met the criteria for recruitment in the study, were invited to participate. Further details of the setting and these criteria are described elsewhere. 26 In total, 157 self-completed questionnaires were returned (response rate = 91.8%, ranging from 81.8% to 97.8% across the units).
Data collection
Data collection was performed in 2014 and lasted for 1 month. The questionnaires were given to participants in sealed envelopes at their place of work, together with an empty envelope to place their completed questionnaire, before placing it in the box which was left at the nursing managers’ office for 2 weeks. A reminder to return the questionnaires was circulated a week after their initial distribution, a strategy proved valuable in increasing responsiveness.
Research instruments
In addition to demographics, the 26-item version of the Ethical Climate Questionnaire (ECQ-26) 10 and the 24-item (part A) of the MISSCARE survey—nurses version 49 were used on the basis of the objectives of this study. These were translated to Greek following the criteria of translation and cultural adaptation by Squires et al., 50 and the whole process used is reported elsewhere. 26 The construct validity of both instruments was not separately examined for the small sample of this study (n = 157), but it was examined using a larger sample (n = 782) that included all nurses working with adult in-patients in Cyprus. In this larger sample, the nurses working with adult in-patients with cancer were included. Some of the results of this validation are provided in this article in order to inform the reader, but the full details of the adaptation procedure and validation of the instruments will be reported elsewhere.
The ECQ measures five types of ethical climate, namely, caring (7 items), instrumental (7 items), independence (4 items), law and code (4 items), and rules (4 items), as perceived by employees, in a particular organization. All items are positively phrased. Responses are rated on a six-point Likert scale ranging from 0 (completely false) to 5 (completely true) A higher mean level of an ethical climate type reflects a higher level of respondents’ perception of it. Respondents are invited to answer what they consider it exists in their organizations and not on the basis of their preferred ethical climate type. 42 ECQ has been translated in other languages, used in different countries and organizations, and for various professional groups, including nursing, where its validity and reliability were obtained. 3,9,10,32,37,39,43,51 In order to examine whether the five-factor structure of the ECQ-26 questionnaire is valid in Cyprus Hospitals and see whether any modifications would be necessary, a confirmatory factor analysis was performed (in the larger sample n = 782) using the statistical software AMOS (IBM SPSS AMOS version 21.0). Model fit adequacy was evaluated with a number of model fit indexes, which are highly recommended in the literature. 52 –56 The original model (ECQ-26) 10 did not fit the Cyprus data well, since the criteria were not satisfied. However, the “modification indices” showed that a five-type structure is satisfied, but with slight modifications. The “Rules” factor remained fully unchanged, while the other factors in general remained unchanged (each type of ethical climate in ECQ-18 with its items gives about the same meaning with the original type). In total, eight items were removed (namely, items 2, 3, 4, 10, 11, 19, 24, and 25) and the resulting structure of ECQ-18 which actually used in this study was caring (five items), instrumental (four items), independence (two items), law and code (three items), and rules (four items). The internal consistency reliability for the different types of ethical climate in this study proved to be satisfactory (Cronbach’s alpha was as follows: instrumental = 0.947, caring = 0.965, independence = 0.837, rules = 0.847, and law and code = 0.888).
Part A of the MISSCARE survey 49 was rated on a five-point Likert scale starting from 1 (never missed) to 5 (always missed). Higher scores represent higher levels of missed care. Its psychometric properties (acceptability, content validity, congruent validity, contrast validity, and reliability) have been tested and reported 49 while it was satisfactorily translated and used in other languages. 57 The construct validity and underlying structure of the items related to Part A of the MISSCARE survey, with regard to Cyprus data, were examined using exploratory factor analysis. Initially, the data were examined and found to be appropriate for factor analysis, with a sufficient sample size and indication that the items align into more than one factor, with Kaiser–Meyer–Olkin (KMO = 0.900) and p < 0.001 for Bartlett’s test of sphericity. Following that and based on the recent literature, 58 oblique rotation was used for the extraction of the factors and more specifically principal component analysis with oblimin rotation. Factor loadings below 0.4 were suppressed. Two factors were extracted with eigenvalues 8.278 and 6.649, respectively. The first factor that includes 14 items was labeled as “Activities of Daily Living (ADL) Omissions” and the second factor that includes 10 items was labeled as “Acute Care Missed Nursing Care.” The justification to use oblimin rotation in the analysis was supported by the results, since the two resulting subscales had a significant Pearson correlation coefficient (r = 0.628; p < 0.001), and therefore, the independence of the factors could not be upheld. The internal consistency reliability in this study, for the total scale MISSCARE Part A (Cronbach’s alpha = 0.957) and for the two subscales (Cronbach’s alpha: “ADL Omissions” = 0.914 and “Acute Care Missed Nursing Care” = 0.877), proved to be very satisfactory.
Data analysis
Frequencies, percentages, mean value, and standard deviations (SDs) were used to describe the sample characteristics, the overall level of missed nursing care, the elements of nursing care that are most often missed, and the types of ethical climate as perceived by nurses. Pearson’s correlation coefficient was used to examine the relationship between the perceived types of ethical climate and the overall level of missed nursing care. A multivariate analysis of variance (MANOVA) was performed in order to test whether differences exist between care units in terms of the ethical climate types and following that a univariate analyses of variance (ANOVAs) was implemented to find out whether differences between the mean values of different care units, regarding the types of ethical climate are significant. ANOVA was also performed to test whether there are significant differences in the mean values of each type of ethical climate in relation to some characteristics of nurses (e.g. age, level in nursing education, and clinical experience) and then post hoc tests to find particular categories of each characteristic, between which the difference exist. An independent sample t-test was performed in order to see whether there are significant differences in the mean values of the perceived types of ethical climates, between male nurses and female nurses. All analyses performed at the individual level used the package SPSS 19.0 for Windows.
Ethical considerations
The research protocol was approved by the National Bioethics Committee (EEBK EΠ 2014.01.102), the Research Committee of the Ministry of Health (5.34.01.7.6E), and the Data Protection Commissioner (3.28.291) according to national legislation. Access to the setting was obtained from the administration board of each hospital. Permission for translation and usage of the instruments was granted by their respective authors. An information letter was provided to the participants explaining the aim and benefits of the study, its voluntary nature, and the data confidentiality guarantee, as well as an explanation that the completion and return of the questionnaire would be considered as informed consent. All questionnaires were anonymous and were kept securely so that only the primary investigator could have access to them.
Results
Sample characteristics
In all, 62.4% of nurses were women and 37.6% were men. Their age ranged from 24 to 56 years but the majority of them (60.5%) were less than 34 years old (M = 2.55 and SD = 0.843, where 1 ≤ 25 years, 2 = 25–34 years, 3 = 35–44 years, 4 = 45–54 years, and 5 ≥ 55 years). Of them, 82.8% had a bachelor in nursing science, while 12.7% of them held masters or PhD degree and only 4.5% had a diploma. Most of them (66.2%) had more than 5 years of clinical experience, while 33.1% had more than 10 years and 33.8 less than 5 years (M = 3.88, SD = 1.009, where 1 = up to 6 months, 2 = greater than 6 months to 2 years, 3 = greater than 2 years to 5 years, 4 = greater than 5 year to 10 years, and 5 = greater than 10 years).
The perceived types of ethical climate
Table 1 indicates the mean value and SDs for the types of ethical climate as perceived by nurses in all cancer care units. However, Table 2 indicates the mean values of nurses’ perception of the types of ethical climate according to some additional characteristics (namely, the gender, age, level of nursing education, clinical experience, and cancer care unit) and provides some evidence of further analysis performed and the differences found to be statistically significant.
Descriptive statistics of the perceived types of ethical climate.a
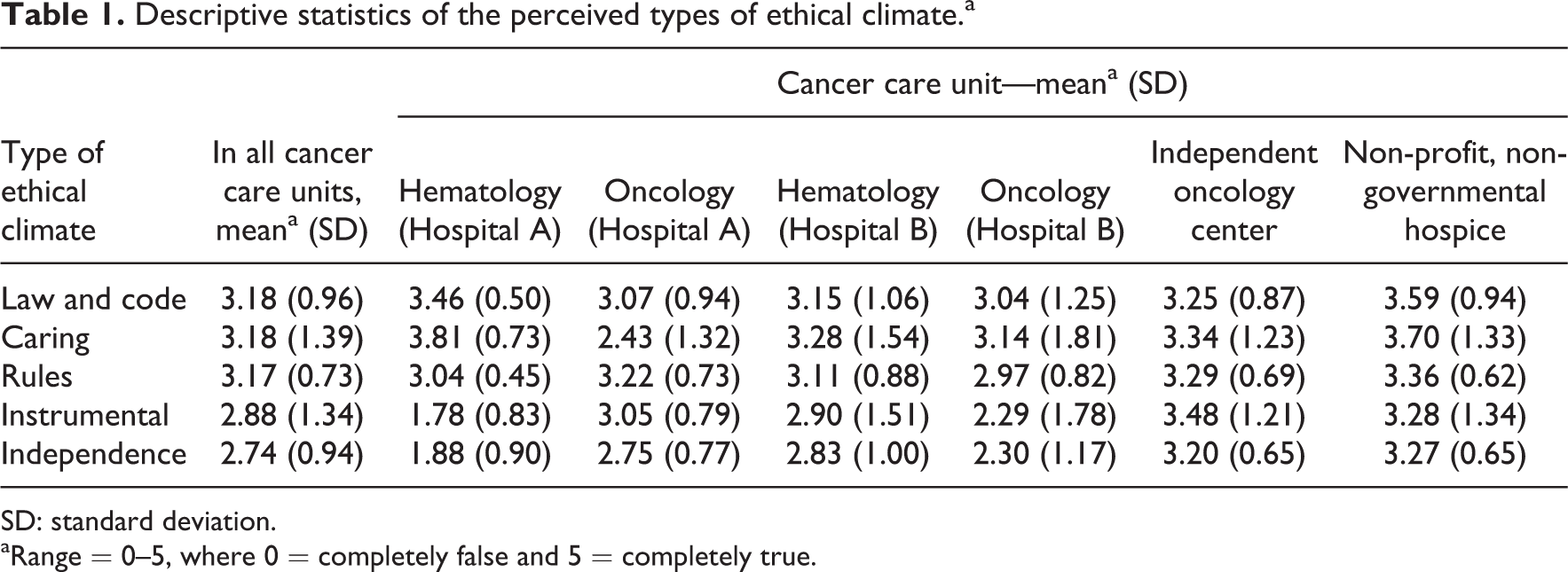
SD: standard deviation.
aRange = 0–5, where 0 = completely false and 5 = completely true.
Participants’ characteristics and the types of perceived ethical climate.
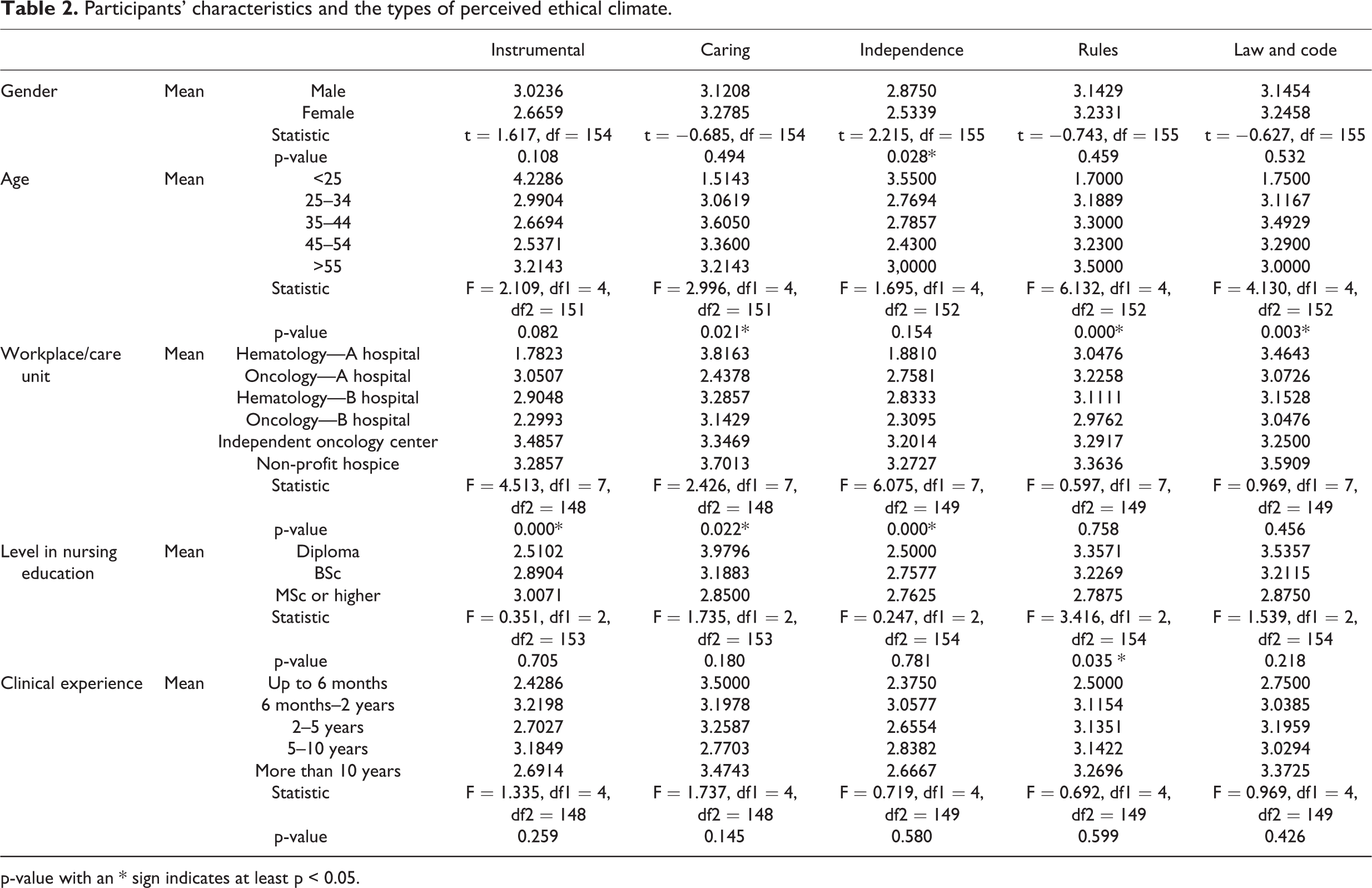
p-value with an * sign indicates at least p < 0.05.
The respondents as a whole identified the presence of law and code ethical climate (M = 3.18, SD = 0.96) and the caring ethical climate (M = 3.18, SD = 1.39), indicating two prevailing types in these units. Rules ethical climate was also rated high in nurses’ perception (M = 3.17, SD = 0.73), while independence ethical climate had the lowest mean (M = 2.74, SD = 0.94). MANOVA analysis showed a significant overall difference between the cancer care units on the mean values of ethical climate types (Pillai’s F(35, 735) = 4.17, p < 0.01, partial η2 = 0.17). Further analysis using ANOVA for each type of ethical climate showed statistically significant differences in the mean values between different cancer care units for the instrumental ethical climate (F(7148) = 4.51, p < 0.01), the caring ethical climate (F(7148) = 4.42, p < 0.05), and the independence ethical climate (F(7149) = 4.43, p < 0.01). Post hoc tests in combination with the ECQ means of these types per unit showed that differences existed between particular units. For example, the hematology unit of hospital A presents a statistically significant lower mean value in the instrumental ethical climate and the independence ethical climate than the oncology unit of the same hospital (hospital A). However, the hematology unit of hospital A presents a statistically significant higher mean value in the caring ethical climate than the oncology unit of the same hospital. With regard to the instrumental ethical climate, the hematology of hospital A presents also a statistically significant lower mean than the independent oncology center and the non-profit hospice, whereas with regard to the independence ethical climate, the hematology of hospital A presents statistically significant lower means than all the remaining units. The oncology unit of hospital B presents statistically significant lower mean in the instrumental ethical climate and in the independence ethical climate than the independent oncology center. However, no statistically significant differences were found between different cancer care units, with regard to the rules ethical climate (F(7149) = 0.6; p > 0.05) and the law and code ethical climate (F(7149) = 0.97; p > 0.05).
Post hoc tests regarding the rules ethical climate in relation to the level of nursing education revealed that those nurses holding a BSc degree present statistically significant higher means than those nurses holding an MSc or a higher degree (e.g. a PhD). No other significant differences have been found for the other types of ethical climate, regarding the educational level of participants. With regard to the categories of age, statistically significant differences have been found only for the caring, the rules, and the law and code ethical climates. Specifically, those nurses with age less than 25 years present statistically significant lower mean value for the caring ethical climate than those with age from 35 to 54 years. In addition, the younger nurses (age < 25 years) present statistically significant lower mean value for the rules ethical climate than all other participants and statistically significant lower mean values for the law and code ethical climate than instrumental ethical climate and the independence ethical climate, than those with age from 25 to 54 years. The analysis using independent sample t-test showed statistically significant differences in the mean values between males and females only for the independence ethical climate, whereas males present statistically significant higher means than females. No significant differences have been found for the other types of ethical climate regarding the gender. However, it was out of the purpose of this study to explore or discuss further these differences.
Nurses’ reported missed nursing care
The overall reported mean value of missed nursing care was M = 2.51 (SD = 0.90). The mean value and SDs of all elements of care reported as missed are presented in Table 2, while further discussion of this part of the results is out of the purpose of this article and reported elsewhere. 26
The relation of the types of ethical climate with missed nursing care
This study revealed significant correlations between certain types of ethical climate as perceived by the nurses and the self-reported overall level of missed nursing care. The perception of nurses of overall missed nursing care was positively related to the instrumental ethical climate (r = 0.612) and independence ethical climate (r = 0.461). This means that when nurses perceive the ethical climate in their units, as one that focus on egoistic tendencies and personal morality, they also perceive that more nursing care activities are missed in these units. However, the overall reported level of missed nursing care was negatively related to the caring ethical climate (r = −0.695), the rules ethical climate (r = −0.367), and the law and code ethical climate (r = −0.487). Therefore, when nurses perceived that the ethical climate in their units is characterized by benevolent and utilitarian ideals, or guided by the compliance and respect of ethical principles, rules, laws, standards and codes of conduct, they also reported less care omissions occurring in their units.
Since significant differences have been found with regard to certain types of ethical climate, between different care units, the relationships between ethical climates and missed nursing care have been further explored, after controlling for the care units. To achieve this, linear regression models have been fitted, with missed nursing care as the dependent variable, the continuous variables of ethical climate types (instrumental, caring, independence, rules, and law and code) as the independent variables, and by controlling for care unit as the categorical variable. The independent oncology center has been chosen as a reference baseline for the categorical variable because it has the highest number of participants. The results from this analysis indicate that missed nursing care is positively related to the instrumental (b = 0.337, p < 0.05) and the independence (b = 0.324, p < 0.05) ethical climates and negatively related to the caring (b = −0.314, p < 0.05), the rules (b = −0.365, p < 0.05), and the law and code (b = −0.327, p < 0.05) ethical climates. On average, the positive relationship of missed nursing care with the instrumental ethical climate found to be significantly higher in oncology of hospital A (b = 0.586, p < 0.05), in hematology of hospital B (b = 0.674, p < 0.05), and in oncology of hospital B (b = 0.566, p < 0.05) than the independent oncology center. With regard to the positive relationship of missed nursing care with the independence ethical climate, on average, this was significantly higher in the oncology of hospital A (b = 0.632, p < 0.05) and the oncology of hospital B (b = 0.555; p < 0.05) than the independent oncology center. However, the negative relationship of missed nursing care with the caring ethical climate was on average significantly higher in hematology of hospital B (b = 0.607, p < 0.05) than the independent oncology center, whereas the negative relationship of missed nursing care with the rules ethical climate was on average significantly higher in the oncology of hospital A (b = 0.538, p < 0.05) and hematology of hospital B (b = 0.684, p < 0.05) than the independent oncology center. Finally, with regard to the negative relationship of missed nursing care with the law and code ethical climate, on average, it was significantly higher in the oncology of hospital A (b = 0.514, p < 0.05) and hematology hospital B (b = 0.679, p < 0.05) than the independent oncology center (Table 2).
Descriptive statistics of the elements of nursing care reported as missed.a

SD: standard deviation; PRN: pro re nata.
aRange = 1–5, where 1 = never missed and 5 = always missed.
Discussion
Both the law and code ethical climate and the caring ethical climate were the prevailing types in the care units under study, while the rules ethical climate had also a high mean score. This result is unique in the nursing literature, since usually one type of ethical climate predominates in each care setting. In contrast, the prevailing ethical climate identified in most studies, 31,33 –36,38,39 was the law and code ethical climate, in other studies 3,32 was the rules ethical climate, whereas in some cases 29,37 the authors either did not seek to find a dominant ethical climate type or else did not report it. It is possible, that the difficult context of cancer care units, call for a combination of these ethical climate. Thus, it appears that in compliance with rules, codes, and professional standards, the adherence to the units’ rules and procedures, the attention to interpersonal relationships, the concern for others (patients, families, and colleagues), and maximization of good is a highly important necessity in these units. This is consistent with most studies, where the law and code ethical climate appears to be the prevailing type, 31,33 –36,38,39 or other studies that ranked the rules ethical climate very high. 3,32
The higher ranking of caring ethical climate in this study is consistent to some studies 33 where this type appeared higher than independence and instrumental climates, but in contrast to most studies where it ranked in middle of the list 31 –34,38 (thus not having the higher mean) and other studies where it ranked last. 39 Therefore, it seems that the caring ethical climate which is desirable 37 to exist, is more easily identifiable in these settings and this may explain in part the low levels of reported missed care.
In line with other studies, 34,38 independence climate ranked last, showing perhaps that in cancer care units, behavior according to own beliefs and personal morality is not considered as a normal practice. In contrast, in other studies, 31 –33,35,36 the ethical climate with the lowest mean levels was the instrumental. The low ranking of independence ethical climate, together with the high mean levels of the rules ethical climate and the law and code ethical climate, can lead to the assumption that in cancer care units, there are strong hierarchical and bureaucratic structures, which play a big part in nurses’ decisions. Therefore, when nurses need to prioritize care, they should conform to a highly regulated environment and the necessity to adhere to certain rules and procedures. This at one hand may lead to less care omissions, but on the other hand may lead nurses to those elements of care that are highly expected by the local rules and regulations, such as those that are implied by the biomedical model of care (e.g. administration of medicines). The instrumental ethical climate ranked fourth, but very close to independence ethical climate, while in other relevant studies ranked last. 31,32,35,36,43 However, the low rankings of independence and instrumental ethical climate together with the high ranking of caring, the law and code and the rules ethical climate and the revealed correlations, may again explain in part the low levels of reported missed care.
In consistency with previous studies, 15 –17 the reported overall level of missed nursing care in these units was quite low and these results are discussed in some detail elsewhere. 26 Nevertheless, it can be also explained by the types of ethical climate that are prevailing in this setting. As it was revealed from this study when nurses perceived the ethical climate in their unit as one that focuses on egoistic tendencies and personal interest, they also perceive that more nursing care activities are missed. The same exists when they perceive the ethical climate of their unit as one that is guided by personal beliefs, personal morality, and an individual sense of what action is right and what is wrong. However, if all nurses working in a specific unit act in a way that only suits their own interests, it is likely that there would be limited opportunity to decide in a transparent and fair way, what is right, when two different interests are in conflict. For example, when shared norms focus on individual self-interest or the personal sense of what is right and what is wrong as opposed to the good of the entire unit and the general welfare of all relevant stakeholders (patients, significant others, nurses, and other professionals), less collaboration is likely to exist and thereby missed nursing care may increase.
When nurses perceived the ethical climate in their unit as being guided by benevolent and utilitarian ideals (i.e. a focus on maximization of good), then they also reported fewer care omissions. When shared norms focus on the good of the whole unit and all of its stakeholders as opposed to individual self-interest and personal morality, more collaboration is likely to exist that may lead to fewer care omissions. The same exist when the ethical climate was perceived as having a strong focus in compliance with and respect of ethical principles, rules, laws, standards, and codes of conduct. However, certain ethical principles and values that govern nursing practice may have passed with greater universality to specific care units and this may be related to nurses’ decisions regarding missed care. It seems that the cancer care units are influenced by deontological principles and professional rules, and this in turn is related to a reduced level of reported missed care.
Further analysis of the relationships of missed nursing care with the types of ethical climate, after controlling for the care units of this study, have shown these relationships (either positive or negative) to be on average significantly higher in certain units than others. Having this in mind, one can assume that improvements of the ethical climate at the unit level may assist in the prevention of missed nursing care from increasing and that the unit-level nurse managers may have an important role to play toward the achievement of this goal. It is often quite difficult for unit-level managers to have much impact on the hospital’s general work climate, especially when these hospitals are quite large organizations. 29 However, by acknowledging the prevailing types of ethical climate of each care unit and their relationships of these types with the reported level of missed nursing care, unit-nurse managers may be able to reduce the influence of instrumental and independence types of ethical climate or to foster the ethical climate types of caring, law and code, and rules in their units. For example, they may be able to improve the ethical climate in their units by active listening to all unit nurses; by behaving with all of them with respect, equality, and justice; and by showing caring attitudes toward all of them as well as toward the patients of their unit. Additionally, they may facilitate the interpersonal relations and the collaboration among nurses, as to strengthen the team functioning within their care unit. However, one can argue that these improvements can be achieved at the level of the care unit, even if the hospital’s organizational climate is defensive, punitive, or not supportive and this in turn may have an impact on the levels of reported missed nursing care.
Nevertheless, in consistency to the majority of relevant nursing studies, 31 –33,35,36,39,43 nurses identified five types of ethical climate (instrumental, caring, rules, law and code, and independence). In other studies, 3,37 the rules and the law and code types were re-categorized under a single type that was labeled as “rules” 3 and “rules and codes,” 37 correspondingly. However, significant differences were found between different units (even within units of the same hospital), regarding the caring ethical climate, the independence ethical climate, and the instrumental ethical climate. Although further analysis was out of the purpose of this study, this finding may support the theory suggesting a variability of the ethical climate types, at the organization level, the unit level, and even at the job level of analysis. 9,10 Having this in mind, one can assume that it is possible that nurses working in the oncology unit of one particular hospital to perceive the ethical climate in their unit as mainly egoistic, whereas nurses working in the same hospital but in another unit (e.g. hematology) to perceive the ethical climate in their unit as mainly caring. This in turn, may lead to the assumption that nurses working in a particular unit not only face similar ethical challenges in relation to care issues arise in this unit but may also share the same values, norms, habits, and so on according to the type of ethical climate that is prevailing there. Although it is premature to form firm conclusions and the whole idea merits further investigation, if we accept that different ethical climate exist in different units of the same hospital, this may be related to nurses’ decisions when they ration care to patients. Therefore, if improvements in ethical climate are needed in order to decrease missed nursing care, one can assume that these can be achieved even at the unit level. Thus, nurse managers 29 even of each unit may have an important role to play in the promotion of an ethical climate that could increase nurses’ morale and could contribute to quality patient care outcomes. In contrast, no statistically significant differences were found between different units, with regard to rules ethical climate and the law and code ethical climate, and these two types of ethical climate ranked very high. This may additionally support the argument that cancer care units are highly regulated care entities.
Study limitations
The generalizability of the findings, at international level, is limited by the fact that the data were collected only from the cancer units in one country. Therefore, one cannot assume that these units are representative of their entire hospital or the nursing profession as a whole in this or any other country. This study used self-completed tools, and this may have led to self-reported bias. However, the achieved response rate mitigates this limitation to some extent, as the findings reflect the perceptions of nearly all nurses in these settings. However, this study presents consistency with studies worldwide and initiates a research agenda regarding the types of ethical climate in relation to missed nursing care.
Conclusion and implications of practice
This study contributes to our understanding of the unexplored area of the types of ethical climate in adult cancer care settings and the relationship of these types with missed nursing care. Taking into account the findings and the above discussion, one can assume that nurse managers and clinicians should try to reduce the influence of instrumental and independence types of ethical climate in their units, as to prevent missed nursing care from increasing. For example, all relevant stakeholders including managers and clinical nurses could be engaged in joint activities, discussions, workshops, formal and informal meetings, or even training programs in an effort to achieve agreement in strategies that could promote the total welfare of patients, staff, and the society in general and in strategies that could prevent individual interests to guide nurses’ decisions and actions when care is rationed. The focus of these activities could be the creation of a shared climate of group cohesion and of a common understanding that the organization is interested for the total welfare of all stakeholders, in such cases, and not only for the individual interests of each member of staff or of one particular patient group. Moreover, by considering first what is best for everyone and by do not accepting any discriminations (i.e. acting as role models), nurse managers could persuade nurses when they ration nursing care, to focus on the general welfare of all stakeholders with equality and justice and not to give emphasis to individual interests or the personal sense of morality. However, by fostering the ethical climate types of caring, law and code, and rules within their units, nursing administrators, educators, and clinicians can contribute in reducing missed nursing care, especially in this sensitive area of practice. Among others, they need to focus their attention on the education of nurses with regard to ethics in healthcare and ethical theories, as well as the ethical climate where practicing nurses are working. The focus of such an effort could be the way this knowledge can assist in the provision of quality nursing care as well as the prevention of missed nursing care. Exploring the types of ethical climate and missed nursing care on a routine basis may provide useful data to nursing management in order to assess improvements in care over time and could facilitate nurses in their practice toward quality care and fewer care omissions. However, more research is needed at an international level to create more robust evidence that could illuminate the area of ethical climate in relation to missed nursing care, in the area of cancer care, as well as in the general care setting. This study found significant associations among the types of ethical climate and missed nursing care. However, there is a need to establish causal relationships that could further inform nurse leaders and guide their actions.
Footnotes
Acknowledgements
The authors express their gratitude to Professors Beatrice Kalish and John B Cullen for their permission to use the instruments for this study. Additionally, they are grateful to the nurses who participated in the study and Mr Gerry Barrett for the language editing of this manuscript. S.V., E.P., A.C., P.A., and A.M. contributed to study design and S.V., E.P., A.C., P.A., C.E., and A.M. contributed to data collection and analysis, and manuscript preparation.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Cyprus University of Technology.