
Abstract
Background:
Nurses are confronted daily with ethical issues while providing patient care. Hospital ethical climates can affect nurses’ job satisfaction, organizational commitment, retention, and physician collaboration.
Purpose:
At a metropolitan academic medical center, we examined nurses’ perceptions of the ethical climate and relationships among ethical climate factors and nurse characteristics.
Design/participants:
We used a descriptive correlational design and nurses (N = 475) completed Olson’s Hospital Ethical Climate Survey. Data were analyzed using STATA.
Ethical considerations:
Approvals by the Nursing Research Council and Institutional Review Board were obtained; participants’ rights were protected.
Results:
Nurses reported an ethical climate total mean score of 3.22 ± 0.65 that varied across factors; significant differences were found for ethical climate scores by nurses’ age, race, and specialty area.
Conclusion:
These findings contribute to what is known about ethical climate and nurses’ characteristics and provides the foundation to develop strategies to improve the ethical climate in work settings.
Keywords
Introduction
Nurses are confronted with ethical issues on a daily basis while providing patient care in today’s changing healthcare environment. The number and complexity of ethical questions in healthcare are rising and affect not only the healthcare professional but also the quality of care provided to the consumer as well. 1,2 It has also become increasingly evident that ethical climate of an organization can influence clinical decision making.
Ethical work climate, a concept first introduced by Victor and Cullen, 2 refers to employees’ perceptions of ethical events, ethical practices, and ethical procedures within an organization. Similarly, in the patient-care settings, Olson 3 described that nurses experience ethical climate as “the individuals’ perceptions of organizational conditions and practices influencing the way difficult patient-care problems having ethical implications are discussed and decided in their work setting (p. 348).” Research has shown that healthcare providers’ perceptions of the ethical climate in their institutions affect their organizational commitment (characterized by strong beliefs in the organization and a desire to do one’s best for the organization, wanting to stay connected to the organization), 4 job satisfaction, 5 –8 turnover intention, 9 and collaboration with physicians. 10 However, few researchers have examined the association of ethical climate and nurse characteristics; conflicting results are reported. 10,11 Most of these studies of ethical climate were conducted outside the United States with healthcare providers employed in general hospitals. 5,7,8,11
Therefore, the purpose of this study was to examine nurses’ perceptions of the ethical climate at a large metropolitan academic medical center in the United States and examine relationships between ethical climate and nurse characteristics. Our research questions were (a) what are nurses’ perceptions of the overall hospital ethical climate, (b) what are nurses’ perceptions of the hospital ethical climate related to five factors (peers, patients, managers, hospital, and physicians), and (c) what are the differences in ethical climate perceptions (overall and the five factors) by nurse characteristics group (gender, age, race/ethnic background, level of nursing education, years employed at current institution, and specialty area)? Better understanding of nurses’ perceived ethical climates will provide foundational information to develop strategies to facilitate the best ethical climate which could contribute to improved nurses’ organizational commitment, retention, and physician collaboration, ultimately leading to improved quality patient care.
Background
Building on organizational and economic theories, Victor and Cullen 2 developed the Ethical Climate Theory (ECT) and conceptualized ethical climates as “general and pervasive characteristics of organizations, affecting a broad range of decisions (p. 101).” Ethical climate is a type of work climate that reflects the organization’s procedures, policies, and practices around moral issues. Ethical climate is defined as the “perception of what constitutes right behavior, and thus becomes a psychological mechanism through which ethical issues are managed. The ethical climate influences one’s decision making as well as subsequent behavior in response to ethical dilemmas (p. 177).” 12 Individuals’ ethical climate perceptions have demonstrated powerful influences, both positive and negative, on organizational outcomes including organizational commitment, job satisfaction, psychological well-being, and dysfunctional behavior. 12
To examine an organization’s ethical climate, individuals’ perceptions of the ethical climate can be measured. Instruments measuring ethical climate have been developed for business and industrial settings as well as for healthcare settings. In the business setting, Victor and Cullen 12 measured ethical climate in terms of five ethical climate dimensions: caring (benevolence, what is best for others), professionalism (concerned with laws and codes), rules (concerned with organizational rules, policies, and procedure), independence (individuals follow their own personal and moral beliefs), and instrumental (egoistic, primary goals is for personal benefits). Although Victor and Cullen’s instrument was developed in business settings, researchers such as Filipova 13,14 and Tsai and Huang 8 used this instrument in healthcare settings, such as hospitals and nursing homes.
Building on Victor and Cullen’s work, Olson 3 designed an instrument to measure nurses’ perceptions of ethical climate in healthcare settings. She measured ethical climate in terms of nurses’ perceptions of organizational practices and the relationships that nurses have in their work setting with peers, patients, managers, hospital, and physicians. Olson 3 purported that how nurses perceived the ethical climate impacted their attitudes about ethical issues, the role they take when ethical questions and problems arise, and their ethical decision making. Olson 3 argues that a positive ethical climate is needed to support professional nursing practice. Thus, by measuring the ethical climate, investigators can better understand nurses’ perceptions of the organizational practices and relationships they have in their work setting with peers, patients, managers, hospital, and physicians.
As predicted by Victor and Cullen, 2,12 associations between one’s ethical climate perceptions and organization outcomes, such as organizational commitment, and job satisfaction have been demonstrated with healthcare providers. For example, researchers identified positive correlations between nurses’ perceptions of ethical climate and organizational commitment, and inverse relationships between ethical climate and turnover intention. That is, Borhani et al. 4 found that the more positive the perceived ethical climate, the higher Iranian nurses’ organizational commitment; Tsai and Huang 8 reported the same relationship in their study of nurses in Taiwan. While Ulrich et al. 6 and Hart 9 measured a similar variable to organizational commitment—intention to stay—and found that a positive ethical climate was a strong predictor of US nurses’ decisions to remain in their current position. Likewise, nurses who perceived a more negative ethical climate were more likely to have left or considered leaving their current position. 10
Investigators have reported positive correlations between healthcare providers’ perceptions of ethical climate and job satisfaction in general hospitals in the United States, 6 Taiwan, 8 and Israel. 7 Similar results have also been reported for nurses employed in a teaching hospital in Iran. 5
Additionally, associations have been reported between nurses’ perceptions of their ethical climate and collaboration with physicians. Hamric and Blackhall 15 explored the perspectives and experiences of nurses and physicians working in intensive care settings. They reported a positive correlation between ethical climate and team collaboration.
Conflicting results have been reported regarding the relationship between nurse characteristics and ethical climate. In a sample of 374 nurses employed in acute care settings in Canada, Pauly et al. 10 reported no significant associations between nurses’ perceptions of ethical climate and their gender, age, years of experience, education, and employment status. In contrast, Bahcecik and Ozturk, 11 with 276 nurses in Turkey, found a significant positive relationship between ethical climate and nurses’ age, years of experience, and work setting. That is, younger nurses perceived a more positive ethical climate than older nurses; less experienced nurses (1–5 years) perceived a more positive ethical climate than more experienced nurses (6–23 years); and nurses in pediatric and intensive care unit (ICU) settings perceived a more positive ethical climate than nurses in other settings. Goldman and Tabak 7 examined relationships among nurses’ gender, years of experience (seniority), and ethical climate and found a significant positive correlation only between nurses’ seniority and perceptions of ethical climate. However, these perceptions were of the ideal not actual ethical climate.
In summary, these results suggest that nurses’ perceptions of ethical climates are related to the nurses’ organizational commitment, job satisfaction, turnover intention, and physician collaboration. Because of these relationships, ethical climate is an important consideration for organizations. Thus, learning more about an institution’s ethical climate is essential as a preliminary step needed before developing interventions aimed at improving ethical climate to in turn improve these outcomes.
Methods
Design and study population
We used a cross-sectional study to address the study purpose. 16 Our target population was registered nurses (RNs) providing direct patient care at a large academic medical center in the metropolitan Midwest.
Instruments
Olson’s Hospital Ethical Climate Survey (HECS) including a demographic questionnaire was used to measure nurses’ perceptions of the ethical climate and nurses’ characteristics. The HECS is a 26-item instrument that measures nurses’ perceptions of ethical climate and the relationships nurses have in their work setting with the following factors: peers, patients, managers, hospital, and physicians. Response options are on a five-point scale (1 = not true, 2 = rarely true, 3 = sometimes true, 4 = usually true, and 5 = always true). Total possible factor sub-scale scores are: peers (20), patients (20), managers (30), hospital (30), and physicians (30). Example items for each factor are: my peers listen to my concerns about patient care, patients know what to expect from their care, my manager is someone I respect, hospital policies help me with difficult patient-care issues/problems, and nurses and physicians respect one another. The higher the HECS score, the more positive the perceptions of ethical climate of the organization. Olson 3 reported Cronbach’s alphas of 0.91 for the 26-item instrument (total score) with sub-scale scores ranging from 0.68 to 0.92. For this study, internal consistency Cronbach’s alpha for the total score was 0.87 with sub-scale scores ranging from 0.81 to 0.87.
Nurses completed a demographic survey. Demographic characteristics included the following: gender, age, race/ethnic background, level of nursing education, years employed at current institution, and specialty area.
Procedure and ethical considerations
This study received approval by the Nursing Research Council and the Institutional Review Board. All RNs providing direct inpatient care at a large academic medical center in the metropolitan Midwest were invited to participate in the study. Nurses were assured participation was completely voluntary, anonymous, and that information would be stored in a password protected electronic format.
Nurses were sent a link to the electronic survey, which included a cover letter inviting participation. To encourage participation, the nurse ethicists visited the patient-care areas two to three times a week (with a candy basket) and sent weekly reminder emails over a period of 1 month.
Data analysis
For this observational study, descriptive statistics were produced for all study variables. Summaries included mean ± standard deviation (SD) for continuous variables, such as the HECS factors sub-scales, and frequency with percentage for categorical variables. Cronbach’s alpha was used to assess the internal consistency (reliability) of the five-factor sub-scales. In order to compare the differences in each sub-scale between and among groups, a Student’s t-test or one-way analysis of variance (ANOVA) was used after examining normality and homogeneity of variances for these sub-scales. If the data of scales were not normally distributed or assumptions of homogeneity of variances were violated, then the non-parametric alternative Wilcoxon rank-sum test or Kruskal–Wallis test was appropriately used. In addition, Bonferroni’s post hoc test following a one-way ANOVA or Dunn’s test following a Kruskal–Wallis test was used for multiple comparisons with Bonferroni’s correction. For less than 5% missing data, a factor sub-scale score was calculated if nurses answered at least half of the items in a multi-item sub-scale (or half plus one in the case of sub-scales with an odd number of items) to derive a sub-scale score for nearly all nurses’ across the five factors. Data were analyzed using STATA/SE 13.1 (StataCorp, College Station, TX).
Results
Sample
Of the 1274 RNs providing direct care to patients invited to participate in the study, 493 (38.7%) responded. We excluded nurses in advanced practice, leadership, and outpatient roles. Of the 493 respondents, 18 were removed from the data analysis due to answering less than half of the items for each scale, leaving 475 respondents for analysis.
As shown in Table 1, the majority of nurse participants were female, 50 years of age or older, and White. Most had a minimum of a bachelor’s degree in nursing (BSN), were employed at their current institution for 5 years or less, and worked on adult critical care, followed by neonatal and medical surgical units.
Nurse characteristics.
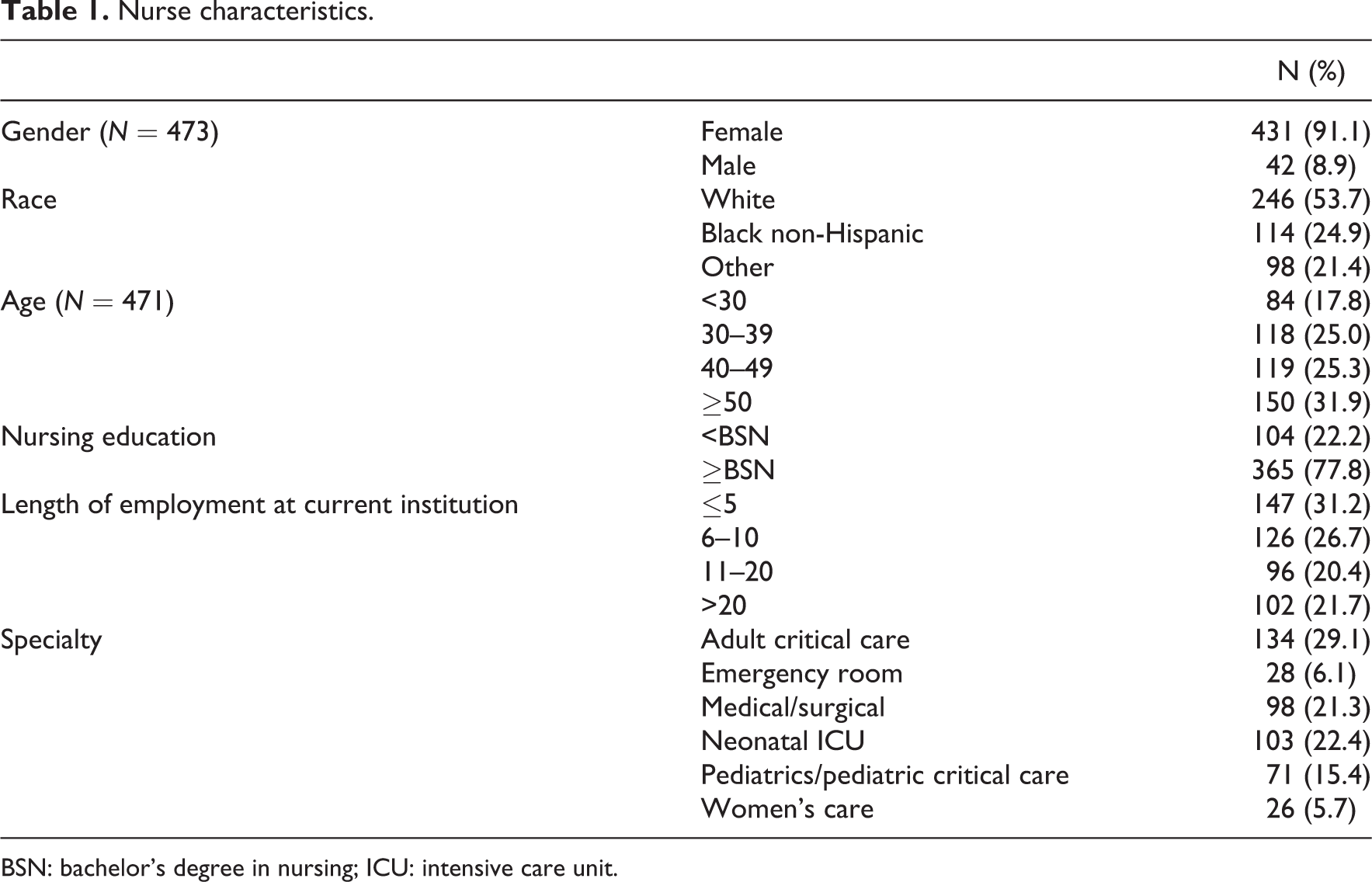
BSN: bachelor’s degree in nursing; ICU: intensive care unit.
HECS scores
Nurses’ HECS total mean score was 3.22 ± 0.65, with a range of factor sub-scale mean scores from 2.93 to 3.94. Nurses’ peer and patient mean sub-scale scores were the highest while manager, hospital, and physicians scored among the lowest. Cronbach’s alpha coefficients of manager, hospital, and physician were respectively greater than 0.83, suggesting that the items of these scales have relatively high internal consistency. HECS total mean scores and the five sub-scales mean scores including SDs, Cronbach’s alpha, and rank order are shown in Table 2.
Nurses’ HECS total and factor sub-scale scores.

SD: standard deviation.
Nurse characteristics and HECS score
Nurse characteristics by HECS scale mean scores are shown in Table 3; total mean scores are reported below. There were significant differences among nurses’ HECS scales mean scores by nurse characteristics including differences in HECS total mean score by age. That is, nurses less than 30 years of age reported higher total mean scores (M = 3.55 ± 0.52) compared with nurses in the other age categories (M = 3.08 to 3.24), p < 0.0001 by Dunn’s pairwise comparison. A similar pattern was shown in nurses’ HECS factor sub-scale mean scores for peers, patients, managers, hospital, and physicians.
Nurse Characteristics by HECS total and factor sub-scale scores.
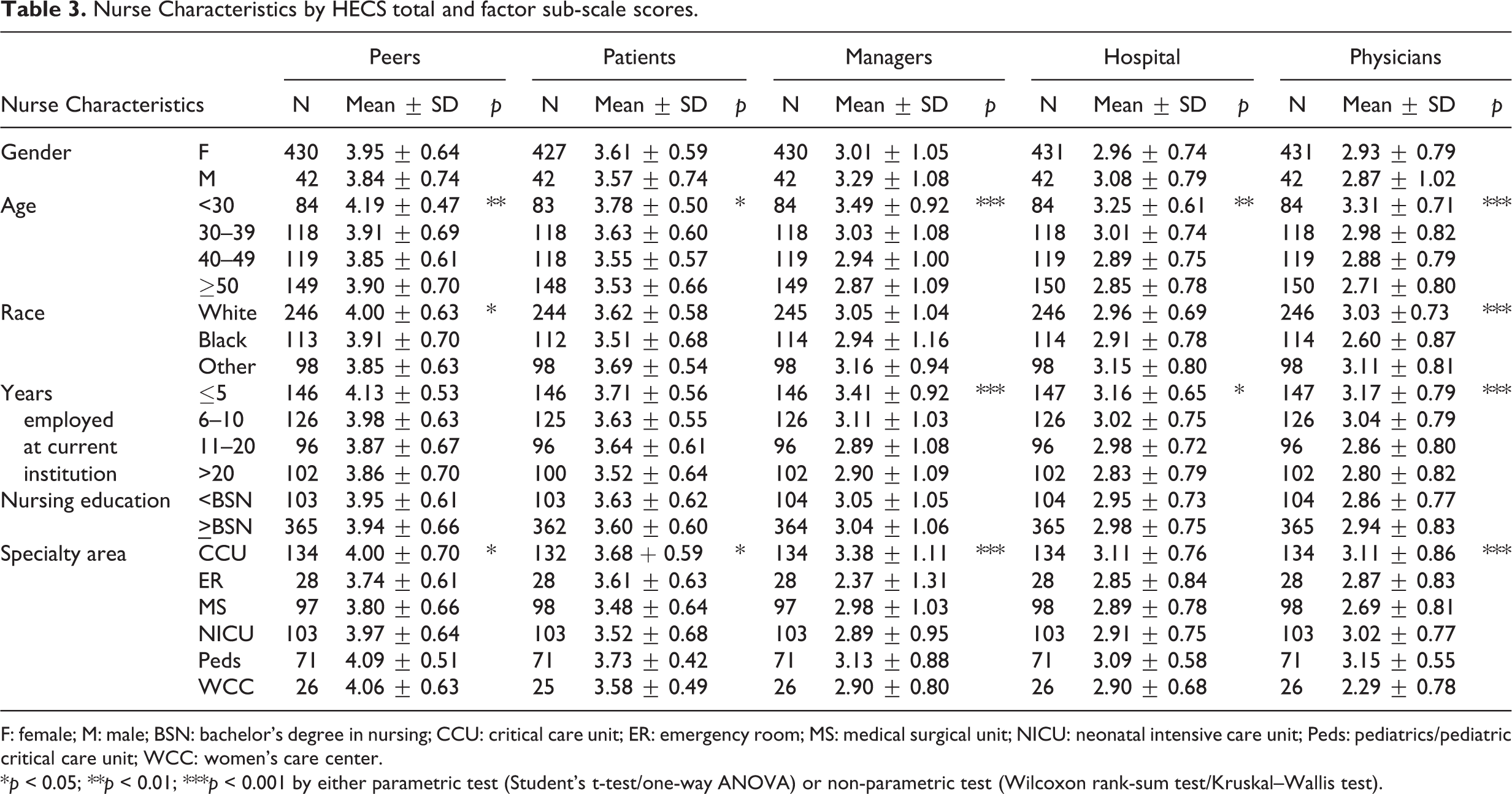
F: female; M: male; BSN: bachelor’s degree in nursing; CCU: critical care unit; ER: emergency room; MS: medical surgical unit; NICU: neonatal intensive care unit; Peds: pediatrics/pediatric critical care unit; WCC: women’s care center.
*p < 0.05; **p < 0.01; ***p < 0.001 by either parametric test (Student’s t-test/one-way ANOVA) or non-parametric test (Wilcoxon rank-sum test/Kruskal–Wallis test).
Significant differences among nurses by race were also present for HECS total mean scores and two of the five sub-scale mean scores (peers and physicians). Nurses who reported themselves as other (did not select White or Black non-Hispanic) had the highest total mean scores (M = 3.33 ± 0.65), while nurses reported as Black non-Hispanic had the lowest total mean scores (M = 3.09 ± 0.70), p = 0.036 by Bonferroni’s multiple comparison test.
Additionally, differences by specialty were present. Nurses in adult critical care settings had the highest total mean scores (M = 3.39 ± 0.69) followed by nurses in pediatrics and pediatric intensive care, (M = 3.37 ± 0.45), neonatal (M = 3.19 ± 0.64), medical/surgical (M = 3.09 ± 0.66), women’s care (M = 3.04 ± 0.56), and emergency room settings (M = 2.99 ± 0.72). The total mean score of nurses in adult critical care settings was significantly higher than nurses in neonatal and medical/surgical groups (p ≤ 0.0001 by Dunn’s pairwise comparison). Likewise, there were differences by nurses’ specialty and their HECS scale mean scores for peers, patients, managers, and physicians (Table 3).
Discussion
The purpose of this study was to examine nurses’ perceptions of the ethical climate at a large metropolitan academic medical center. Our research questions were as follows: (a) what are nurses’ perceptions of the overall hospital ethical climate, (b) what are nurses’ perceptions of the hospital ethical climate related to five factors (peers, patients, managers, hospital, and physicians), and (c) what are the differences in ethical climate perceptions (overall and the five factors) by nurse characteristics group (gender, age, race/ethnic background, level of nursing education, years employed at current institution, and specialty area)? We had two major findings: (a) nurses reported perceptions of a moderately positive ethical climate that varied across factors and (b) differences were found between perceptions of ethical climate and nurses’ age, race, and specialty area.
Based on total HECS scores, nurses at our institution reported somewhat higher than neutral perceptions of the ethical climate. These findings are consistent with results reported by Pauly et al., 10 Sauerland et al., 17,18 and Ulrich et al. 6 Olson 3 argues that a positive ethical climate is needed to support professional nursing practice. Our moderately positive scores suggest potential for improvement of the ethical climate in our institution to better support nursing practice.
Out of the five factors, nurses ranked their perceptions of their relationships with peers and patients the highest, followed by managers, hospital, and physicians. Pauly 10 reported a similar rank order: peers, patients, managers, physicians, and hospital. However, Pauly reported higher mean scores for all five factors. Taken together, these findings suggest that nurses perceived more positive relationships with peers and patients influencing the role they take when ethical questions/problems arise, and with their ethical decision making. Findings further suggest that to support professional nursing practice, future interventions should be targeted toward the improvement of organizational practices and nurses’ relationships particularly with managers, the hospital, and physicians. Furthermore, findings support the notion that ethical climate can and does vary across organizations and should be measured so organizations can identify their strengths and target improvement efforts toward areas of lower scores.
Our finding that nurses’ perceptions of hospital ethical climate significantly differed by age is consistent with Bahcecik and Ozturk’s 11 study in which younger nurses (<23 years of age) had a more positive perception of their ethical climate environment. These findings suggest that nurses’ age can influence their perception of the organizational ethical climate. Younger nurses may have more positive perceptions of ethical climate because their experiences with ethical problems and ethical decision making were more limited than those of older nurses. Conversely, experienced nurses’ greater insight and knowledge about a preferable ethical climate could have negatively affected their perceptions. Furthermore, these older nurses could have a cumulative effect of negative experiences over time also affecting their perceptions. Further research is needed to evaluate these differences.
In our study, we found a significant difference by race for nurses’ perceptions of ethical climate, particularly with the factor sub-scales of peers and physicians. This difference was likely found in our study because of the larger sample of Black non-Hispanic nurses (25%) who completed the survey. This percentage of Black respondents differs greatly from recently reported percentages of Black nurses in our state (8%) 19 and the United States (12%). 20 While investigators have not previously reported differences in ethical climate by race, Ulrich et al. 6 reported that Black nurses experienced more ethical stress and were three times more likely to leave their position when compared with Caucasian nurses. Our findings could be due, in part, to a limited exposure to differing racial groups among nurses either by design or desire, resulting in a lack of understanding of the others’ life experiences and culture, subsequently influencing their organizational practices and relationships in their work setting with peers, patients, managers, hospital, and physicians. In a literature review of Black role conflict, Robinson 21 concluded that because of racial/ethnic identity, gender, and professional roles, Black nurses experience multiple role expectations, which can expose them to additional role stress as compared to their White colleagues. Thus, it is likely that the ethnic, racial, and cultural experiences of nurses impact their relationships with other healthcare professionals as well as their perceptions of ethical climate of their organization. Black non-Hispanic nurses in our institution reported the lowest HECS total mean scores and two of the five-factor sub-scale mean scores (peers and physicians) suggesting that they too may be experiencing additional role stress. Further research is warranted to investigate the differences in ethical climate scores of nurses of differing races.
Nurses in critical care settings and nurses in pediatrics and pediatric intensive care reported the highest HECS total mean scores. Similar results were found by Bahcecik and Ozturk. 11 In our study, nurses in the emergency room reported the lowest scores. Our findings could be explained in part by the lower patient to nurse ratio and longer patient length of stay in critical care settings, allowing nurses more time with patients and families when ethical issues arise. Furthermore, patient acuity in these settings could lead to stronger collaboration among healthcare providers facilitating resolution of ethical issues. In contrast, the fast pace in the emergency room could limit both nurses’ interactions with the patients and families, and collaboration with other healthcare providers.
Findings from this study provide the foundation to develop strategies, in particular ethics education and institutional support, for handling ethical issues, and to improve organizational practices and relationships that nurses have in their work setting especially with managers, hospital, and physicians. Future research and ethics education are suggested to facilitate a positive ethical climate leading to increased nurses’ organizational commitment, job satisfactions, collaboration with physicians, and decreased turnover intention.
Methodological considerations
Limitations of this study include a low response rate as well as a convenience sample from a single academic medical center in a metropolitan setting. It is likely that our results cannot be generalized to nurses in other organizations. In addition, during analysis, nurses’ HECS total mean and sub-scale scores were pooled from both adult and pediatric nurses. Based on their settings, these nurses’ different perceptions of ethical climate could have skewed the results for these variables. However, many of our findings were consistent with findings from past studies.
Conclusion
Examining nurses’ perceptions of the ethical climate allowed us to identify foundational information regarding nurses’ perceptions of the hospital ethical climate related to five factors (peers, patients, managers, hospital, and physicians) and the relationship between ethical climate and nurse characteristics. In addition, these findings contribute to what is known about ethical climate and nurses’ characteristics in a large metropolitan medical center in the United States. Future research and ethics education are suggested to facilitate a positive ethical climate leading to increased nurses’ organizational commitment, job satisfaction, decreased turnover intention, and collaboration with physicians.
Footnotes
Acknowledgements
This research was supported by Katherine Pakieser-Reed PhD, RN, Executive Director of the Center for Nursing Professional Practice and Research. We gratefully acknowledge her for supporting this research conceptually and financially. In addition, we acknowledge Julie A. Johnson, MPH, RN and Daniel Sulmasy, MD for earlier assistance with this project and Cynthia LaFond, PhD, RN, CCRN-K for her review of the manuscript. We would also like to acknowledge the staff nurses who participated in this research.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.