
Abstract
Background:
In the past two decades, interest in the concept of ethical climate and in its research has increased in healthcare. Ethical climate is viewed as a type of organizational work climate, and defined as the shared perception of ethically correct behavior, and how ethical issues should be handled in the organization. Ethical climate as an important element of nursing environment has been the focus of several studies. However, scoping reviews of ethical climate research in nursing have not been conducted to guide further research in this area.
Objective:
The purpose of this scoping review is to describe and analyze studies focusing on ethical climate in nursing environment to elicit an overall picture of the research in this field.
Methods:
A scoping review methodology guided by Arksey and O’Malley and Levac et al. was used. Studies were identified by conducting electronic searches on PubMed/MEDLINE, CINAHL, Web of Science Core Collection, PsycINFO, and Scopus and Philosophers’ Index databases. Of 1051 citations, 56 articles matched the inclusion criteria.
Ethical considerations:
This study was conducted according to good scientific guidelines.
Findings:
Ethical climate is a topical research area which has been explored with different methods and outcomes, in different environments, and has mainly been perceived positively. The focus of the studies was on finding associations between ethical climate and work-related factors such as job satisfaction, moral distress, and turnover intentions. Methodologically, research was rather homogeneous using quantitative, descriptive, and correlative research designs.
Conclusion:
Novel perspectives and more diverse methodological approaches paying attentions to issues affecting generalizability of the findings could expand our knowledge in this area.
Introduction
Ethical climate is viewed as a type of organizational work climate reflecting organizational practices, procedures, and policies with moral consequences. 1,2 Victor and Cullen 1 defined ethical climate as “the shared perceptions of what is ethically correct behaviour and how ethical issues should be handled” (p. 52) within organizations. They introduced their ethical climate theory (ECT) in the late 1980s. ECT serves as a descriptive map of ethical decision-making and actions within an organization based on philosophical and sociological theories. More specifically, they used a theoretical perspective to describe different ethical climate types appearing in organizations. 1 In their initial work, they classified ethical climates into five types: caring, independence, law and code, rules, and instrumental. 3 A few years later, Olson 4 defined ethical climate as nurses’ perceptions of how ethical issues are handled in their work environment, and that it refers to “individual perceptions of the organization that influence attitudes and behaviour and serve as a frame of reference for employee behavior” (p. 90).
In the past two decades a growing interest in the concept of ethical climate and its research within healthcare has emerged, especially in nursing environments, where nurses as the largest professional group 5 practice and encounter a variety of ethical issues in their daily work. 6 It has been argued that ethical climate influences nurses’ wellbeing at work and the quality of patient care nurses provide, making it a significant factor in nursing environment. 7 Therefore, an overview of the ethical climate research in nursing would be useful to those interested in the topic, since there is no aggregate knowledge base concerning the focus areas, main findings, and methodologies and quality of the studies examining ethical climate. The purpose of this scoping review is to describe and analyze studies focusing on ethical climate in nursing environment to elicit an overall picture of the research in this field. The study estimates the extent and scope of the available research aiming to provide knowledge for managers, administration, policy makers, and researchers. This knowledge is a valuable resource for informing systematic reviews, and it can be used to guide future research and to reduce duplication of effort.
Methodology
This scoping review was conducted to provide an estimation of the breadth and scope of the available research literature and to provide knowledge for further research. 8 A scoping review methodology guided by Arksey and O’Malley 9 and Levac et al. 8 was used. Scoping reviews can be undertaken to examine the extent, range, and nature of research activity by mapping all relevant research literature, for example, to determine the value of undertaking a full systematic review. 8 Scoping reviews differ from systematic reviews as they do not attempt to synthesize evidence from different studies and they do not typically assess the quality of evidence provided by the included studies. 9 Arksey and O’Malley’s 9 methodological framework outlines a five-stage approach for conducting scoping reviews as outlined below.
Stage 1
For identifying the research questions, a series of questions related to the study objectives was first developed. After becoming familiar with the literature, the following research questions were identified to guide the review: What are the main foci and main findings of the studies? What are the methodological choices used in the studies and how is the validity addressed? How are limitations and research ethics addressed in the studies? What are the implications and suggestions for further research in the studies?
Stage 2
For identifying relevant studies, six electronic databases were searched: PubMed/MEDLINE, CINAHL, Web of Science Core Collection, PsycINFO, and Scopus and Philosophers’ Index. Using the Boolean operators, (non-MeSH) search terms ethical AND (climate* OR environment*) AND (nurse* OR nursing) limited to title and abstract were used. No time limitation was set. The search yielded 1051 citations after duplicates had been removed. The search was run in March 2016.
Stage 3
Study selection started by defining inclusion and exclusion criteria. The inclusion criteria were as follows: (1) studies in peer-reviewed scientific journals, (2) examining ethical climate in nursing environment, and (3) having nurses as participants to provide full or partial data. Studies were excluded when (1) English translation was not available or (2) research was conducted from the patients’ perspective. Furthermore, theoretical scientific and unscientific articles, letters, book reviews, commentaries, editorials, and unpublished papers were excluded.
Two authors (J.K. and O.N.) concurrently and independently applied the inclusion and exclusion criteria to all citations and identified those meeting the research objective. In case the relevance of a citation was vague, the full study was obtained and reviewed and discussed until consensus was reached. After the initial selection of applicable citations, full-texts of all selected citations (n = 89) were obtained. J.K. and O.N. then independently reviewed these full-texts to finalize the list of those that would be included in the review. The disagreements on inclusion/exclusion of studies were resolved by discussion. As a result, 56 studies were included in the review, which are marked with “*” in the reference list (Figure 1). As this was a scoping study, quality assessment of the included studies was not performed using any specific tools to determine whether particular studies provide robust or generalizable findings.
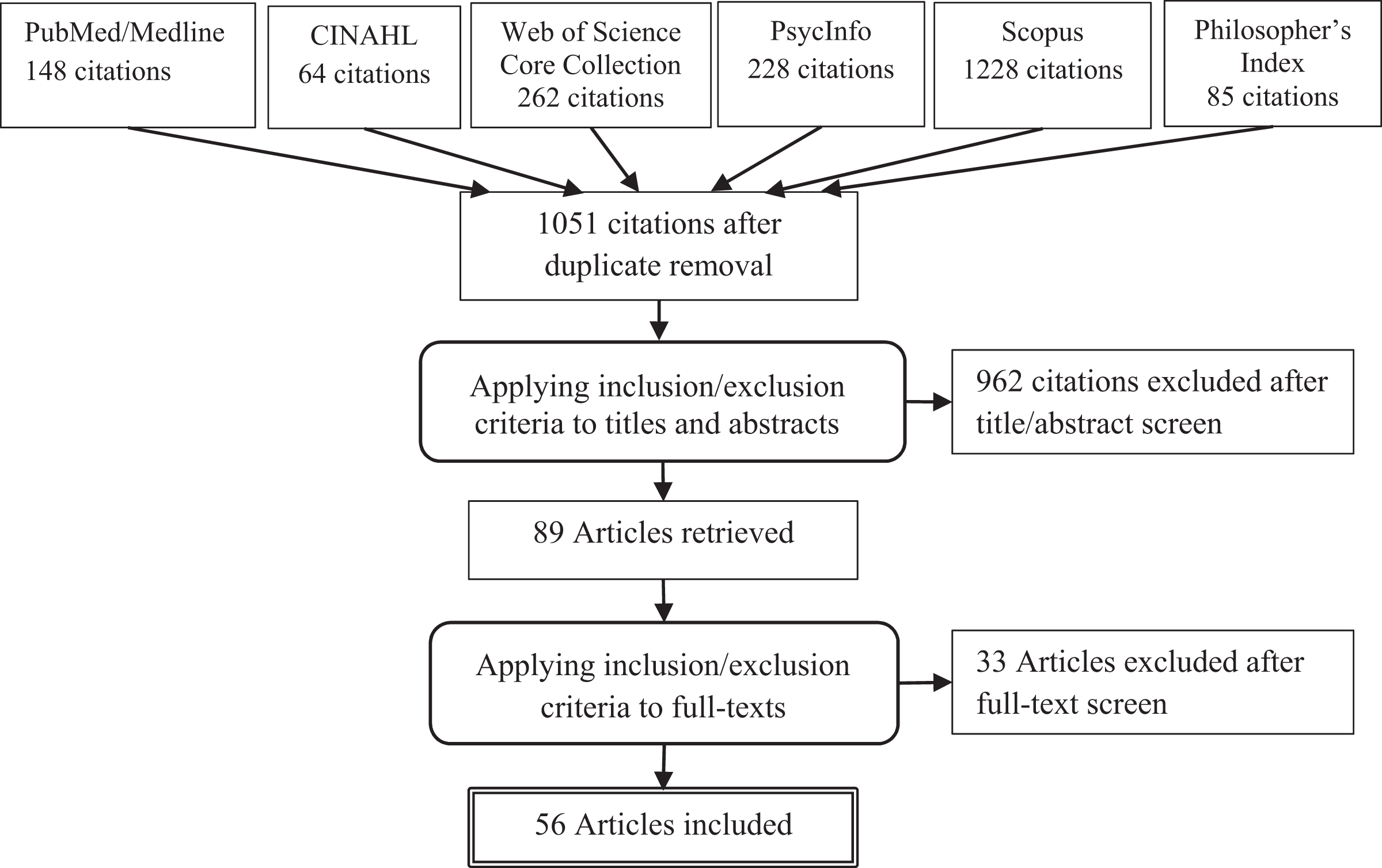
Flow chart of the study selection procedure.
Stage 4
For charting the data, the authors first determined which variables to extract in order to answer the research questions, thereafter developing the data-charting form consisting of descriptive study characteristics: author, year, country, aim of the study, study design, sampling, data collection, data analysis, main foci, main findings, setting/context, research ethics, limitations, further research, and implications/recommendations. J.K. and O.N. independently charted the data using the original terms and phrases and subsequently discussed divergences.
Stage 5
Collating, summarizing, and reporting the results were carried out in accordance with the research questions. Quantitative and qualitative analyses were used to describe study characteristics.
Results
General description of the studies
From 1997, the annual number of publications remained fairly steady until 2007. From 2008 onward, the number of publications has started clearly to increase reaching the highest number in 2015 (Figure 2).
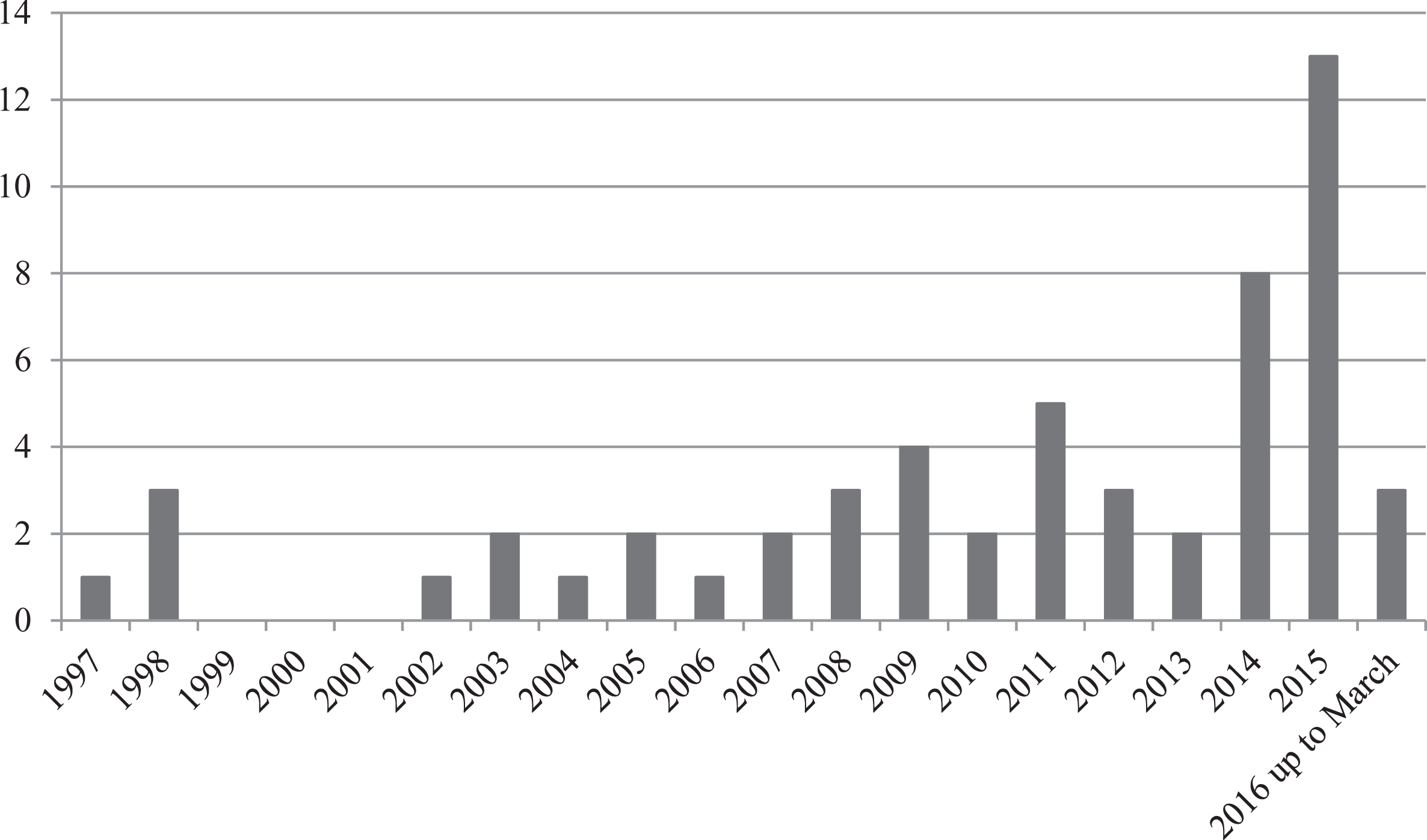
Publication years of the studies.
Studies of ethical climate (n = 56) represent 17 different countries of origin. The United States has been the most productive in number of publications (n = 20; 36%). In other countries, the number of publications has varied from just one up to seven (2%–13%).
In terms of nursing cultures, the Western nursing tradition has been the most prominent comprising 42 (75%) studies from the United States, Canada, Australia, New Zealand, Finland, Sweden, Spain, Italy, Belgium, the Netherlands, and Bosnia and Herzegovina. The Middle Eastern countries of Iran, Turkey, Israel, and Egypt had produced 11 (20%) publications, and the Far Eastern countries of Taiwan and South Korea had produced 3 (6%) studies (Figure 3).

Country of origin of the studies.
Journals
The studies were published in 25 different peer-reviewed scientific journals. A total of 21 (38%) studies were published in Nursing Ethics journal. The number of studies in the other journals varied from one (2%) to three (5%). Most journals originated from the United States (n = 12; 21%) or United Kingdom (n = 7; 13%). Other journals were from Iran (n = 2; 4%), and Canada, India, and Sweden one journal (2%) from each. Nevertheless, the majority of the journals had an international scope thus being open to authors and readership internationally. The majority of the studies (n = 51; 91%) were published in nursing journals with impact factors ranging from 0.25 to 3.561.
Main foci of the studies
Most of the studies approached ethical climate from the nurse’s individual perspective by focusing on its association or effects with job satisfaction, 10 –21 turnover intentions, 10,14,15,17,22 –25 moral distress, 20,26 –36 moral sensitivity, 30 ethical behav/ior, 37 occupational commitment, 15 self-assessed professional competence, 14,15 qualities of empowered nurse, 14 and withdrawal behaviors. 38
Some studies approached ethical climate from the organizational perspective by studying its associations or effects with organizational commitment, 10,16,18,22,39 perceived organizational support, 10,21 organizational distributive justice, 38 and organizational citizenship behaviors. 40
The focus of interest has also been on ethical climate and its associations or effects with work-related factors such as collaboration, 32 teamwork, 41 quality improvement leadership, 41 medical error experience, 23 professional practice environment, 42 and practice environment. 14
Some of the studies paid attention to patient’s perspective by studying associations or effects between ethical climate and appropriateness of care, 28 satisfaction with quality of care, 32 individualized care, 42 and patients’ outcomes. 43
The development of an instrument Hospital Ethical Climate Survey (HECS) was the focus of one study 44 and evaluation of its psychometric properties was the focus of four studies. 44 –47 Some of the studies evaluated healthcare organizations’ ethical climate in a one-site setting 48 –53 or compared ethical climate in different working environments. 18,54 –56 Furthermore, two studies examined ethical climate by utilizing theoretical models 21,34 and promoting ethical climate was the focus area of two studies. 57,58
Some of the studies noted the ethical climate, but the main foci were on another subject such as moral habitability, 59 ethical practice, 60 students’ incivility behaviors, 61 decision-making in cases of physical restraint, 62 organizational ethics, 63 quality aspects of empirical studies, 64 and ethical conflicts. 65
Main findings of the studies
Overall perception of the ethical climate of care providers’ practice environments has mainly been positive. 15,23,31,33,45 However, the participants perceived ethical climate differently across the organizations 45,54 –56 and several different types of ethical climates, as described by Victor and Cullen 3 were recognized, such as professionalism, rules, caring, independence, instrumental, 50 and law and code 55 ethical climates. Ethical climate was positively associated with job satisfaction, 10,12,17,20 professional competence, 15 individualized care, 42 organizational support, 10 organizational commitment, 10 satisfaction with quality of care, 32 ability to manage disagreements, 43 opinions about work, 43 work effectiveness, 43 and physicians’ and nurses’ collaboration. 32 Ethical climate was negatively associated with turnover intentions 10,15,24 and moral distress. 20,27 –33,35,36 However, Schluter et al. 25 concluded that the evidence to support the claim that poor ethical climate is associated with nurse turnover was lacking at the time.
Participants’ demographic characteristics, except age, 45 did not correlate with ethical climate. 19,56 However, nurses perceived ethical climate more negatively than physicians. 28,32,48
Different types of ethical climates 3 showed varying associations with other variables. First, participants were more satisfied with their job when they reported their hospital having a caring, 11,13,16,18,19 rules, 11,13,16,18 or independence 11,16,19 ethical climates. Instrumental ethical climate negatively influenced job satisfaction 16 and positively correlated with intent-to-leave. 21 Second, organizational commitment increased as the participants reported their hospital having caring, rules, independence, 39 or law and code 21 ethical climates, while the instrumental climate type decreased organizational commitment. 16 Third, moral distress was positively associated with the climate types of rules. 26 However, Rathert et al. 34 did not find similar results in their study. Fourth, ethical behaviors were positively associated with independence ethical climate, 37 and organizational citizenship behaviors positively associated with caring, law and code, and rules ethical climates and negatively with instrumental ethical climate. 40 Finally, nurses who perceived the patient dimension of ethical climate more positively, as described by Olson, 44 were less likely to make medical errors. 23
Ethical climate could be enhanced by ethics education, 58 by meeting needs as well as by receiving and giving support and information within the care team. 57 Likewise, working as a team with a standard for behavior promoted a positive ethical climate. 57
Methodological choices of the studies
Research design
The majority (n = 44; 79%) of the studies were quantitative, six (11%) studies were qualitative, 51,57,59 –62 and two (4%) studies 35,36 used both quantitative and qualitative designs (Tables 1 and 2). Of all studies, four (7%) were literature reviews 25,29,63,64 and four (7%) instrument validations. 44 –47 The majority of the studies used descriptive and correlation research designs (Supplementary file 1).
Validity and reliability assessments in quantitative studies.

CFAe: CFA reported in an earlier study; x: reported; xe: reported in an earlier study.
Validity and reliability assessments in qualitative studies.

Settings
Most studies were conducted in hospital settings (n = 44; 79%). Some studies used a multi-site setting comprising different clinical areas. Single-site settings included acute care (n = 9), intensive care (n = 4), medical-surgical (n = 2), geriatric (n = 2), and pediatric (n = 2) units. Other settings were nursing home (n = 3), managed care (n = 1), nursing school (n = 1), and combined hospital and community care (n = 1).
Sampling
The participants were mainly nurses. The total number of nurses in quantitative studies was 11,565, the sample sizes ranging from 36 to 1826 nurses. In qualitative studies, the total number of nurses was 48, and the sample sizes ranging from 7 to 21. Other participant groups were physicians (n = 172), 28,32,43,48 patients (n = 109), 43 nurse aids (n = 38), 48 nurse administrators (n = 32), 16 nurse educators (n = 11), 61 and combinations of nurses and social workers (n = 1215), 6 and nurses, allied health, and medical workers (n = 104). 49 In the latter two combined sample groups, the number of each participant group was not specified. One qualitative study reported no number of participants. 59
Non-probability sampling methods predominated including convenience sampling (n = 17; 30%), purposive sampling (n = 9; 16%), stratified sampling (n = 1; 2%), quota sampling (n = 1; 2%), and theoretical sampling (n = 1; 2%). Probability random sampling was used in five (11%) studies.
Data collection methods
In the quantitative studies, the most used instrument to measure ethical climate was Hospital Ethical Climate Survey/HECS. 44 The original instrument was applied in 20 (43%) and an adapted version in two (4%) studies. Another frequently used instrument was Ethical Climate Questionnaire/ECQ. 1 The original version was used in 14 (30%) and adapted version in 2 (4%) studies. The Ethics Environment Questionnaire (EEQ) 66 was used in four (9%) studies and its adapted version in one (2%) study. The Integrity Audit Ethical Conflict Questionnaire-Critical Care Version (ECNQ-CVV) 65 was used in two (4%) studies and the Ethical Conflict Questionnaire-Critical Care Version (ECNQ-CVV) 65 in one (2%) study.
Other instruments used in ethical climate measurement focused on various organizational factors (i.e. organizational culture, support or commitment, and practice environment or behavior), job satisfaction, nurse turnover, and moral distress. Quality and safety of care, nurse competence, individualized care, nurse empowerment, communication, and collaboration were measured as well.
Qualitative studies applied various interview techniques: focus group (n = 3), individual in-depth (n = 1), semi-structured (n = 1), or critical incident interviews (n = 1). One study used open-ended qualitative questions. 35 Data in literature reviews were retrieved from relevant databases. The number of reviewed studies ranged from 9 to 56. Response rate was indicated in 21 (46%) of quantitative studies. The response rates ranged from 21.4% to 100%.
Data analysis
All studies applied analysis methods appropriate to the research design: statistical in quantitative research data (n = 46), several analysis methods applicable to qualitative research data (n = 8), and content analysis in literature reviews (n = 4).
Validity and reliability assessment
In quantitative studies, construct and structural validity were assessed using factor analysis. Exploratory factor analysis (EFA) was carried out in 6 (13%) and confirmatory factor analysis (CFA) in 20 (43%) of quantitative studies. In 10 cases, the researchers relied on CFA conducted in their previous studies. Content validity was assessed in 13 (28%) studies, of which experts were used in 8, and complemented with content validity index (CVI) in 2 studies. Six studies did not mention the content validity assessment method. Face validity was assessed in 11 (24%) studies.
Internal consistency reliability using Cronbach’s coefficient alpha was used in 43 (93%) studies, one study referring to a previous study. Stability using test–retest was estimated in seven (15%) studies. Power analysis was reported in 13 (28%), and piloting in 9 (20%) studies. Description of instrument translation procedure was found in 18 (39%) studies, three authors (1%) referring to translations in previous studies (Table 1).
In studies using qualitative approach (n = 8), researcher validation confirmability and research process documentation were described in six (75%) studies. Reflexivity and transferability were described in three (38%) studies. Credibility by an outsider validation and participant validation were mentioned in two (25%) studies, and data saturation in one (13%) study. An independent interpretation of transcripts and codes was carried out by multidisciplinary experts to validate the findings in one (13%) study (Table 2).
In the literature reviews, 25,29,63,64 the data retrievals and data analysis processes were well described. Data assessments were carried out by two or three researchers or the research group.
Limitations
Major limitations of the studies dealt with (1) sampling referring to small sample sizes or biased samples in terms of gender or participant group, (2) low response rates, (3) limited scope of the studies referring to single location studies, and the (4) generalizability of the findings. Lack of cause–effect estimation in descriptive research designs was also recognized as a weakness. Attention was paid to social desirability bias. The problems related to common measurement bias, self-reported data, and on-line data collection were also mentioned. A total of 11 (20%) studies provided no discussion of the limitations (Supplementary file 2).
Research ethics
Approval to conduct the study was obtained from different authorities depending on focus of the study. Ethical approval was obtained from ethics committee of the university (n = 21; 36%), ethical review board of the participating hospital/s (n = 16; 29%), and from regional or national authorities (n = 9; 16%). Additional permissions were obtained from directors of department or head nurses, or from professional unions and nursing colleges. Approval was waived in literature reviews (n = 4; 7%). Seven (13%) studies provided no information.
Ethical considerations were provided in a separate article section or included within appropriate other sections in the majority of studies (n = 48; 86%). Written or oral information of the purpose and research procedure of the study, confidentiality, and anonymity were reported in most studies. Completing a questionnaire was a common way to ensure consent to participate. In some studies, a signed informed consent had been asked. Voluntary participation and right to withdraw were also addressed. Four (7%) studies provided no information of research ethics, and for the nature of literature reviews (n = 4), particular discussion of ethics was not relevant.
Implications and suggestions for further research
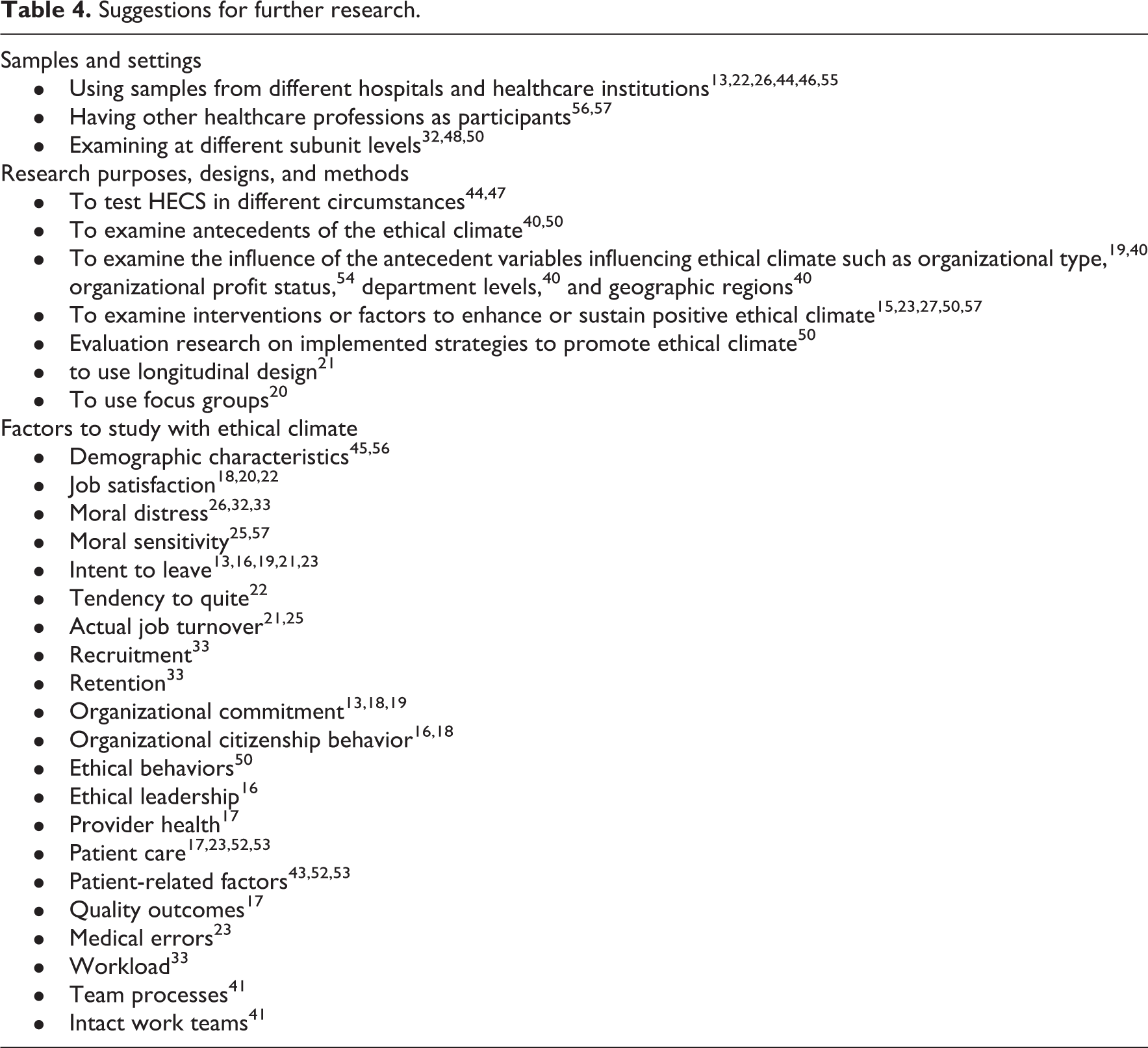
Most commonly, practical implications of the studies were directed to hospitals, administrators, and nursing managers and also to nurses and other healthcare providers as well as for researchers. Only a few implications were directed to education and health policy (Table 3). Suggestions for further research concerned samples and settings, also research purposes, designs and methods, and factors with possible associations with ethical climate (Table 4).
Implications of the studies.

Suggestions for further research.
Discussion
The purpose of this scoping review was to describe and analyze studies focusing on ethical climate in nursing environment to elicit an overall picture of the research in this field. The study estimated the extent and scope of the available research and was aimed to provide knowledge for managers, nurse educators, administration, policy makers, and researchers especially planning further research.
Publication years of the studies revealed that ethical climate is a topical research area. Increasing number of articles has been published in recent years. Why the interest in this field has increased could be manifold. Healthcare environment has become more complex; new sophisticated targeted treatments, including high-priced therapies, 67 technology, 68 the need for prioritization, 69 limited resources, 6 and medicalization, 70 evoke a wide range of ethical issues. Thus, ethical climate has become an important factor in the healthcare environment for it has a significant impact on healthcare workers’ ethical decision-making and ethical behavior. Nurturing ethical behavior and values is, therefore, important in work communities to provide quality care.
Most of the studies were conducted in the United States. Most likely this could be explained by the overall volume of nursing research and resources compared with other countries. However, this gives a picture of ethical climate in American healthcare system and should be interpreted as such. Not only North America and Europe but also countries from Middle East and Far East had contributed to the research on ethical climate in nursing environments. This is welcome, but it seems there are no big differences in how nurses perceive ethical climate among different nursing cultures. This might be due to core nursing values such as respect, dignity, equity, and equality guiding nurses worldwide. Nursing is an ethically charged practice, so the importance of core nursing values as a fundamental guidance for nursing is well known.
Over half of the studies focused on studying the associations or effects of the ethical climate with nurses’ job satisfaction, moral distress, and turnover intentions. It might be a good time to consider expanding the research scope, as the basis of the nurses’ descriptions of the ethical environment is generally perceived positively, but specifically poor environment increases nurses’ moral distress and leads them to change their jobs and profession. In particular, what antecedent factors create good or bad ethical climates? Shifting the research perspective away from nursing and healthcare professionals to look at health policies, healthcare structures, values, and management might be a valuable perspective for future research on ethical climate. Nevertheless, it might also be relevant, if there is enough evidence, to conduct meta-analysis or to create more theoretical models on the relationships between ethical climate and nurses’ moral distress and turnover intentions to get a more comprehensive picture and powerful evidence on these factors affecting each other.
It seems that especially ethical climate types of caring (concern in the organization is the good of all employees and them caring for each other), 3 rules (where it is expected that employees strictly follow company’s procedures and rules), 3 independence (the employees’ personal ethics are important and they are expected to follow their own personal moral and ethical beliefs), 3 and law and code (where people are expected to follow strictly legal and professional standards and consider whether a decision violates any law) 3 are the ones having positive influences on work-related outcomes, whereas the instrumental (situation, where people protect their own interests above all else and are expected to do anything, regardless of the consequences, to further the company’s interests) 3 is having negative outcomes. Especially when dealing with the issues of nurse shortage and turnover, the appearance and the impact of these different climate types should be recognized. Focusing future research on the strategies and interventions that organizations could use to move away from instrumental ethical culture toward ethical cultures that emphasize caring, rules, and independence would be useful.
From a methodological viewpoint, quantitative, descriptive, and correlative research designs predominate ethical climate research. As a fairly new area of interest, this may be understandable and justified. However, academics in the field 71 have pointed out that nursing research should move forward to more sophisticated research designs, which would bring about, for example, causal relationships, which in turn would help nurses to tackle issues which might have adverse effects on nursing care. The potential of descriptive correlational studies to provide strong evidence is limited. 71 This point was emphasized also in the discussion of limitations in some studies of this review. 10,11,32,34,41
Although several sampling methods were used, non-probability sampling methods were common. Non-probability sampling is rarely representative, hence care should be taken that the sampling procedure is strict enough to maximize representativeness. 71 However, the use of non-probability sampling may be the most practical and also a justified method since ethical climate studies seem to be carried out in environments, such as a single hospital or a particular care unit in which the purpose of the study is to detect the ethical climate of this particular context rendering probability sampling unpractical. In their study, Suhonen et al. 47,64 have provided detailed description of sampling in ethical climate research in nursing.
Study limitations concentrated on small sampling sizes, low response rates, narrow scope of single studies, and as the result of these, on low generalizability of findings in quantitative studies. Only limited use of power analysis to estimate a proper sample size was evident. These limitations are related not only to studies of ethical climate but seem to be kind of a norm in many areas of nursing research. These limitations should be addressed more strictly in future studies because they compromise the overall validity of the studies. The lack of cause–effect estimation as a limitation suggests a limited use of sophisticated statistical analyses. Although the number of intervention and implementation studies has increased, a significant part of nursing research still uses descriptive research designs. Social desirability bias as a limitation has also been recognized particularly in ethics research.
HECS by Olson 44 is the only instrument developed particularly for healthcare context and for nurses 44 which may explain its frequent use. It measures ethical climate in relation to other professional groups, organization, and patients in healthcare, whereas another frequently used instrument ECQ by Victor and Cullen 3 focuses on different types of ethical climates, thus measuring the ethical climate from quite a different perspective. Juxtaposing two or multiple instruments might provide deeper knowledge of perceptions of different perspectives of ethical climates and their mutual relationships. Measurement of ethical climate was combined with measurement of various work-related factors in nursing practice environment but only to detect relationships between the measured variables rather than estimating predictive factors or consequential effects. Insufficient attention paid to the impact of variables affecting ethical climate but left unmeasured was a concern of several authors. 11,16,17,26,40,45,48
Discussion about validity and reliability varied considerably between the studies. On time continuum, it seems that description of instrument translation procedure and use of power analysis have increased to some extent during the recent years. Performing exploratory or confirmatory factor analyses and Cronbach’s coefficient alpha have remained frequent and constant throughout the years. There seems to be a slight overall tendency showing that studies published in recent years have started to pay more attention to validity and reliability assessment of measurement. Rigorous assessment of validity and reliability of the measurement is of paramount importance to the overall validity of the study and quality of research. 71 Development projects in nursing care environments are worth the effort only if they are based on high-quality research evidence. Application of research findings in practice whether focusing on patient care or nurses’ work environment is sustainable and ethically justified only if it is based on quality research in terms of accurate measurement.
The extent of ethical consideration varied greatly between articles, which is understandable given the different clinical contexts under study. However, due to the applied research designs, in most studies addressing conventional ethical considerations was sufficient.
Most of the implications were addressed to the hospitals, administrators, and nurse managers. Many authors recommended that all these facets should support strategies and conduct interventions to enhance ethical climates, for example, by providing ethical education for employees. This is understandable as there seems to be an agreement that ethical climate can be changed with new leadership and with modified organizational practices. 6,72 The same issue is also indicated in the suggestions for further research, the most suggesting to examine interventions or factors to enhance or sustain positive ethical climates. However, these implications and suggestions concerning intervention studies have not been addressed significantly even in the most recent research. This review might help to draw attention to these. More research is needed on these issues.
Strengths and limitations
Sourcing from several relevant databases and the systematic process to retrieve and analyze the literature by two researchers are strengths of this review. Setting no time limits to publications which allowed retrieval of a large number of studies is also a strength. Including only studies written in the English language could be considered a limitation, but it might also be justified referring to English as “lingua franca” of modern science. 73 Nevertheless, the impact of cultural diversity may suffer through this limitation. Furthermore, it should be acknowledged that the data analysis process of this review followed Arksey and O’Malley’s method. Their method has also been criticized for not to providing detailed methodological description for concerned process, 8 and by thus making it challenging to follow both for authors and readers.
Conclusion
Ethical climate has been explored in different environments with different methods and outcomes, but it has been perceived mainly positively. Mainly the focus of the studies was on finding associations between ethical climate and work-related factors. The strongest empirical evidence was in linking the ethical climate with nurses’ job satisfaction, moral distress, and turnover intentions.
Methodologically, more attention should be paid to issues which strongly affect the generalizability of the findings. In this respect, also the systematic use of power analysis in estimating required sample sizes is justified depending on the sampling method. Moving forward to more sophisticated research designs such as cause–effect estimation would provide knowledge for targeted development projects in areas which need improvement. Simultaneous use of different instruments would provide a deeper understanding of elements forming ethical climate and how these factors relate to each other. Different qualitative approaches, such as ethnography, critical theory, or case studies, would provide new, deeper knowledge of experiences related to ethical climate which could contribute to the development of new instruments to measure ethical climates in healthcare and nursing contexts.
Future ethical climate research is recommended to shift perspective to look at health policies, healthcare structures, values, and management. Importantly, research on the factors contributing to good or bad ethical climates, and strategies and interventions that healthcare organizations could use to change the ethical climate or enhance and sustain positive ethical climates is needed. Furthermore, it should be considered whether there is enough evidence to conduct meta-analysis or create theoretical models on the relationships between ethical climate and factors that have been found to be associated with ethical climate.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.