
Abstract
Background:
While sustainability is a key concept in many different domains today, it has not yet been sufficiently emphasized in the healthcare sector. Earlier research shows that ethical values and evidence-based care models create sustainability in care practice.
Objective:
The aim of this study was to gain further understanding of the ethical values central to the realization of sustainability in care and to create an ethical practice model whereby these basic values can be made perceptible and active in care practice.
Research design:
Part of the ongoing “Ethical Sustainable Caring Cultures” research project, a hermeneutical application research design was employed in this study.
Participants:
Dialogues were used, where scientific researchers and co-researchers were given the opportunity to reflect on ethical values in relation to sustainability in care.
Findings:
An ethical practice model with ethos as its core was created from the results of the dialogues. In the model, ethos is encircled by the ethical values central to sustainability: dignity, responsibility, respect, invitation, and vows.
Discussion:
The model can be used as a starting point for ethical conversations that support carers’ reflections on the ethical issues seen in day-to-day care work and the work community, allowing ethical values to become visible throughout the entire care culture.
Conclusion:
It is intended as a tool whereby carers can more deeply understand an organization’s common basic values and what they entail in regard to sustainability in care.
Introduction
The concept of sustainability is not new, and it has a rather long history and it has evolved over time. Originally, sustainability was used to describe the connection between human and the environment. The concept of sustainability was brought to the fore with the release of the Brundtland Report (also known as “Our Common Future”), published by the United Nations’ World Commission on Environment and Development. In the report, sustainability was defined as a fundamental process conducive to the realization of long-term yet non-compromising human development. Sustainability as a concept was described in economic, social, and environmental dimensions. 1 Världsmedborgaren 2 claims that the sustainability concept should be expanded, and it is not enough with these three dimensions. Världsmedborgaren supposes that sustainability in addition to economic, social, and environmental dimensions also have an ethical dimension. Världsmedborgaren 2 emphasizes that sustainability is a struggle against ethical erosion.
Sustainability has been explored in many disciplines and become an integral part of many different domains and fields, for example, sociology, ecology, and economics. In 2009, the European Union presented its strategy on sustainability and included public health as a key theme. 3 Still, Schroeder et al. 4 maintain that in the field of healthcare, sustainability as a concept has not yet been sufficiently studied. In current healthcare research, the importance of taking care of the environment 5 while also maintaining a balanced economy 6 –9 is emphasized as being essential for the realization of sustainability in healthcare. Sustainability in healthcare is generated by creating and implementing evidence-based care models that are enduring, embraced by an organization’s entire staff and work as indicators of healthcare. 6,7,9 –13 In line with Världsmedborgaren’s thinking, Crow et al. 10 found that ethics is the foundation for sustainability in healthcare. They highlight the ethical values respect and dignity as the starting point for sustainability. Salmela et al. 13 also underline respectful and dignified care and emphasize that in order for care to be sustainable it should be evidence-based, financially viable, and safe for patients.
Several researchers underscore that sustainability in care is realized through good leadership 9 –12 and a well-educated and engaged staff. 5,10,11 Some researchers maintain that that which is sustainable is expressed and made perceptible in an organization through staff’s thoughts, habits, and routines. 5,9,12,14 This is supported by Porter-O’Grady and Malloch’s 5 findings that sustainability is linked to the care culture. According to Salmela et al., 13 sustainable care cultures should be constructed from contextual, professional, and cultural prerequisites, thus ensuring that the core and art of caring is maintained through good traditions as well as care staff’s ethical and professional competence.
Our review of earlier research shows that the foundation for sustainability in healthcare is based on the clear articulation of ethical values and the implementation of evidence-based care models in practice. This motivates continued research into those values central to sustainability in healthcare and the creation of an evidence-based model for ethically sustainable care. In this study, we particularly highlighted an ethical dimension on sustainability in care because earlier research on such does not to any significant extent exist.
Aim
The aim of this study was to unfold ethical values in the field of the ethical dimension of sustainability and to create an ethical practice model (EPM) for enabling ethically sustainable care.
Research design and method
This study is part of an ongoing research project, Ethical Sustainable Caring Cultures, at a hospital in western Finland. The study has a hermeneutical application research design that is participatory-oriented, which allows the opportunity to unite clinical practice and caring theory and thereby evolve or change the current clinical practice. 15 Hermeneutical application research design has its roots in Gadamer’s 16 philosophical hermeneutics. The starting point or preunderstanding lies in a common picture of caring reality, a common view of knowledge and common values or ethos. In accordance with the principles of hermeneutical application research, the participants in this study consisted of scientific researchers and co-researchers from clinical practice. We used reflective dialogues through which the participants were given the opportunity to reflect on ethical values and good care. By opening up for reflection through dialogues and discussions, a common understanding can be reached and new innovational thinking can occur. Our use of an application research approach anchors any eventual change in clinical practice and also contributes new knowledge to the scientific theory. 15,17 The hermeneutical application research was implemented in three phases: articulating of the preunderstanding by a description of common ontological and contextual assumptions, putting the preunderstanding at stake through reflective dialogues, and bringing the new understanding to light in order to gain a common understanding.
During the first phase, the ontological assumption was formulated as: ethics are rooted in the thought that caring pertains to safeguarding the human being’s dignity and the sanctity of life. The contextual assumption was derived from a summation of the participating care organization’s administrative and official documents as well as a review of Caring Science research, where the research focus lay on ethical values. We found that the variables dignity, respect, responsibility, traditions, and good habits (among others) were the foundations for the realization of sustainable care. We also sought contextual information through an electronic questionnaire, answered by staff (n = 120) at eight selected hospital units (32% response rate). The questionnaire not only provided us with an empirical view of carers’ thoughts on the ethical values they considered important but also revealed that they desired more time and opportunities to be able to reflect on their ethical thoughts and actions in clinical practice.
During the second phase, we invited staff from the selected hospital units to participate in reflective dialogues. This allowed us, the scientific researchers, an opportunity to, together with the co-researchers, reflect on ethical values and how such can be made perceptible and active in care. A total of 21 carers from psychiatric, medical, surgical contexts and the context of service units (radiology, laboratory) elected to participate in the dialogues. Three participant dialogue groups (with seven participants in each group) were formed and four researchers with theoretical knowledge in the field of Caring Science led the groups. The groups each met once a month, six times for 2 h per time. Each time, the dialogue centered on one of the ethical values that emerged during the first phase of the research. Prior to each dialogue, the participants were given a written presentation, based on theoretical knowledge, of the actual ethical value being discussed, allowing participants opportunities for personal reflection. During the dialogues, the participants reflected together on how theoretical knowledge can be expressed in clinical practice.
During the third phase, we sought new understanding and consensus about ethical values that enables sustainable care. First, the participants’ reflections were written down while the dialogues were taking place. Then, after each dialogue was finished, the scientific researcher participating in the actual dialogue summarized and formulated the group’s common understanding. These were subsequently collected and used to create an EPM. The EPM was thereafter further modified during a conclusory dialogue between the scientific researchers and co-researchers.
Ethical considerations
The study follows the guidelines for good scientific praxis as described by the Finnish Advisory Board on Research Integrity 2012 18 and the ethical principles delineated in the Declaration of Helsinki 2002. 19 Consent for the study was obtained from the participating care organization’s upper management. In the cover letter containing information about the study and explaining the purpose of the group dialogues, participants were guaranteed anonymity. Participation in the study was voluntary and written informed consent was sought prior to participation.
Findings
An EPM
The dialogues resulted in an EPM (Figure 1). The EPM is derived from the researchers and co-researchers’ common understanding of the ethical values that enables sustainable care, as well as how these can become perceptible and implemented in care.
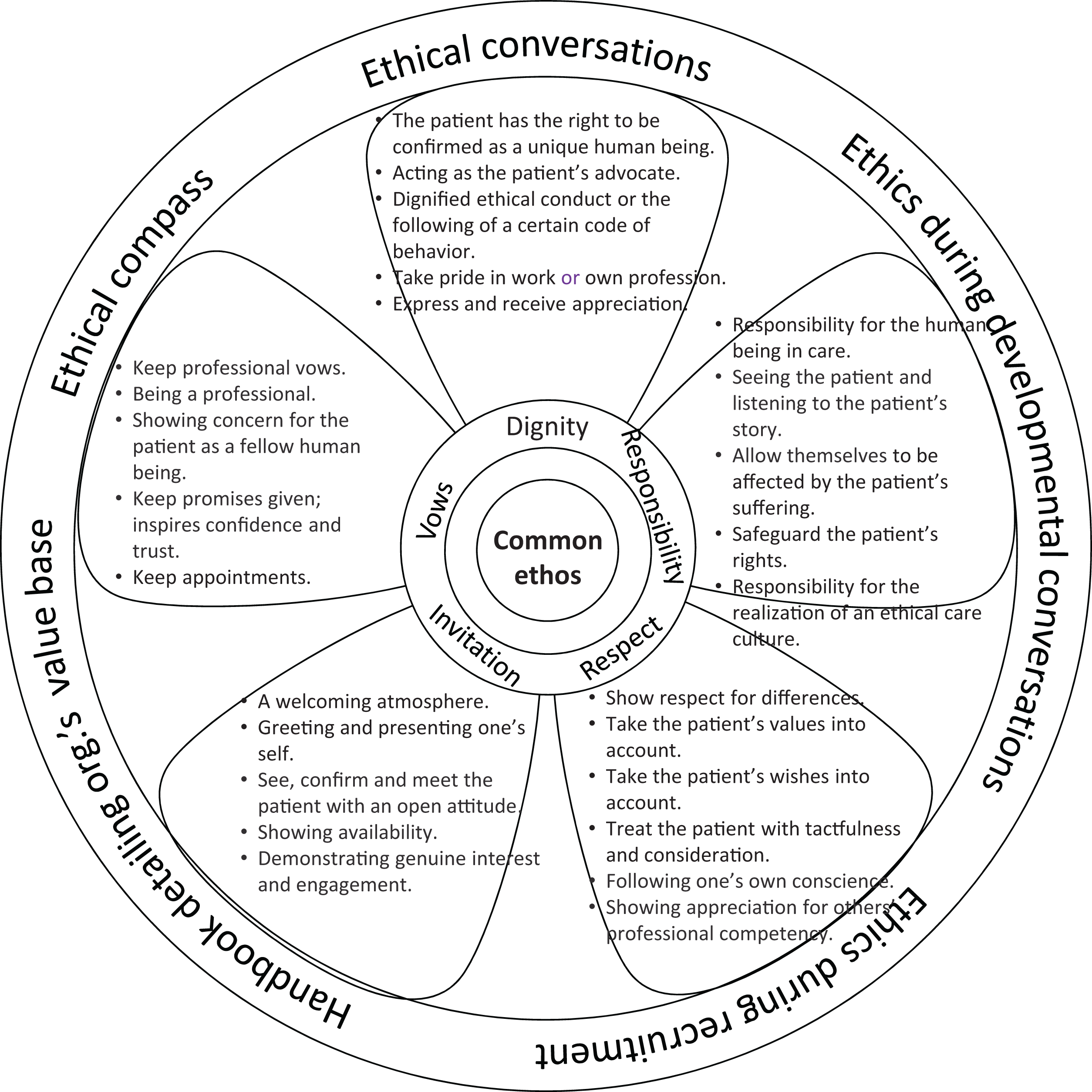
Ethical practice model (EPM) for sustainability in care.
The text in the innermost circle of the EPM is the core of the model: the common ethos. The ethos of care is the ontological value base for sustainability in care, that is, the fundamental value base for care. The text in the middle circle, which encircles the common ethos, reveals the five ethical values considered central to sustainability in care: dignity, responsibility, respect, invitation, and vows. The text in the outermost circle shows the tangible tools and new habits that an organization can employ to create sustainability in care.
Of the ethical values, dignity, respect, and responsibility emerged during the first phase of the study while invitation and vows were revealed during second phase. In the text below, we further illustrate these with examples of how the participants perceived these in clinical practice.
Dignity
Dignity was maintained when carers had a clear view of their mission, which is working for the patient’s best. This mission entails focusing on the primary task of “being there” for a patient, assuming that the patient has the right to be confirmed as a unique human being and acting as the patient’s advocate. When carers “are there” for a patient, the patient feels important and noticed and dignity is maintained. Conversely, carers not being there can seriously violate a patient’s dignity.
Believing and taking the patient seriously also maintains dignity, and not doing so can cause the patient to feel a sense of powerlessness or despair. Dignity is furthermore maintained through carers’ dignified ethical conduct or the following of a certain code of behavior. This can entail greeting a patient, introducing one’s self, using polite terms such as “thank you” or “excuse me” and acting in socially polite manner. Carers’ dignity is also maintained when they take pride in work or own profession. Dignity also becomes perceptible when carers express and receive appreciation and through joy and humor create a positive work atmosphere.
Responsibility
Responsibility was perceived as an all-encompassing responsibility for the human being in care. Carers bear the responsibility of safeguarding that which is good for the patient, seeing the patient and listening to the patient’s story. Carers’ responsibility for individual patients is highlighted when they allow themselves to be affected by the patient’s suffering. In the moment that carers dare meet and allow themselves to be affected by a patient’s gaze, they must decide whether to bear the responsibility for care or not. Accordingly, responsibility also entails having the courage to safeguard the patient’s rights and to take the patient’s side. While carers bear personal responsibility, responsibility cannot be limited to individual carers; it is collective and collegial and encompasses a common duty to cooperate and help other staff members, even for example between units. The responsibility for the realization of an ethical care culture entails that individual carers assume responsibility for acting as ethical role models for others and working for the realization of the care culture and the common mission, that is, the patient’s best.
Respect
Respect for each and every human being in daily care work was considered to be important and entailed showing respect for differences. Differences enrich a care culture and should be utilized, noticed, and valued. Respect becomes perceptible when carers take the patient’s values into account, take the patient’s wishes into account, and treat the patient with tactfulness and consideration. Respect also entails acting in accordance with and following one’s own conscience and showing appreciation for others’ professional competency. Respect for others’ knowledge also increases work motivation and improves workplace satisfaction.
Invitation
Invitation was described as the ability to receive or meet others in a welcoming manner, that is, the creation of a welcoming atmosphere. By greeting and presenting one’s self, carers show that they see, confirm, and meet the patient with an open attitude. Invitation also entails showing availability as carers. A further important aspect is demonstrating genuine interest and engagement in the patient’s situation.
Vows
Vows were described as the importance of keeping the ethical vow that one, as a professional carer, has taken. Carers keep professional vows in clinical practice by being a professional and showing concern for the patient as a fellow human being. It was considered very important that carers keep promises given to a patient, which inspires confidence and trust. It was furthermore considered important that carers uphold the agreements or arrangements made as part of one’s working duties, that is, keep appointments.
As mentioned previously, the outermost circle of the EPM reveals the tangible tools and new habits that an organization needs to implement in order to create sustainable care. In our project, the tangible tools and new habits include regular ethical conversations among carers, reflections on ethics and ethical competency during regular carer and nurse leader developmental conversations, reflections on ethics and ethical competency during the recruitment of new staff, a handbook detailing the care organization’s value base, and an “ethical compass” that is used to steer activities and delineate the tangible, contextual ethical vows relevant to the organization’s various units. The incorporation of these tools and habits in the organization allows everyone to experience that the central ethical values in care practice are perceptible and active in the organization’s care culture. 10 –12
Discussion
This article shows that sustainability in care from an ethical dimension is generated by creating and implementing evidence-based care models. 6,7,9 –13 Sustainable care is also supported by clear articulation of ethical values. Ethical values constitute the core of sustainability, and sustainability is a struggle against ethical erosion. 2,10 Sustainability is also clearly linked to the care culture. If sustainability in care is to be developed and maintained, it is necessary that the entire care culture should embrace the same ethical values. The leader and caregivers strive together in creating a caring culture. 13 A prerequisite for sustainable care is good leadership and well-educated and dedicated carers.
We assumed that sustainability has an ethical dimension 14 and therefore sought the ethical values central to sustainable care in an attempt to construct an EPM for enabling ethically sustainable care. From our findings, we created a practice model that can be used as a tool, independent of context, to help make the central ethical values necessary for sustainable care both perceptible and active. However, a challenge is whether healthcare professionals acquire these models, and whether these models really provide a basis for care. A challenge of implementing our ethical model (EPM) is that it only will be a new set of empty values if it is not used in practice. This means that the basic idea of a sustainable care is demolished. To ensure that our model will be used in practice, it has been important that carers have actively participated in the creation of the model, along with the involvement of management. 10 –12 A decisive factor is that the organization and management support the implementation of new models. 12 Furthermore, the model is also based on research and the knowledge contributed by scientific researchers, which according to Gloppen et al. 7 makes the model evidence-based and thus also sustainable in time of change and economic turbulence.
According to Eriksson, 20 the core of a care culture is its ethos, that is, its fundamental value base. In a care organization, all staff should be cognizant of and familiar with this ethos if the organization’s values are to be maintained and realized. A condition for this is that staff continuously highlight and discuss ethical values, which strengthens their ethical attitudes and competency. 2,21 Through such continuous “rediscovering” of ethical values, a culture is given a new life. 20 Our use of a hermeneutic application research approach and our inclusion of co-researchers from clinical practice ensured that the EPM created through this study included the ethical values seen in the care culture studied here.
We found that if sustainability in care is to be developed and maintained in an organization, it is necessary that the organization’s entire care culture should embrace the same ethical values, which was also seen in studies by Porter-O’Grady and Malloch. 5 A care culture is based on cultural elements such as traditions, rituals, and basic values. 20 Our results showed that sustainability in care can be strengthened by introducing meaningful habits and routines into an organization. 5,9,12 Rytterström et al. 14 describe habits and routines as being pragmatic and meaningful when they support good care. Still, habits and routines can become barriers to sustainable care, if carers in an organization interpret them as actions to be merely repeated or uncritically embraced and if carers do not tailor them to suit the specific needs of each unique patient. It is therefore important that carers continuously reflect on and evaluate existing routines and continuously implement sustainable habits and routines that emanate from actual research and theoretical care models. The ethical values inherent in a culture are not merely limited to patient care but are also continuously seen and expressed in an organization’s work community: in the ever-changing meeting between co-workers, new employees, medical residents, and students.
We also found that dignity and respect are central ethical values in sustainable care, which is in line with Crow et al.’s 10 research. In earlier research, nurse leaders and other carers have been considered personally responsible for the realization of good and sustainable care. 9 –12 Yet we found that the responsibility for such lies with an organization’s entire staff and as such is consequently a collective and collegial responsibility that should be embraced throughout the entire care culture, a finding also supported by Salmela et al. 13 This study moreover provided new understanding of the central ethical values invitation and vows.
Methodological reflections
The incorporation of the tools and habits delineated in our findings allows everyone in an organization to experience that the central ethical values in care practice are perceptible and active in said organization’s care culture. During the dialogues part of our study, providing participants with information prior to group discussions allowed the participants the opportunity to personally reflect on the subject matter before engaging with the group. Still, the research design demanded comprehensive knowledge and input from the study researchers and co-researchers over a sustained period of time. During dialogues, the scientific researchers needed to express themselves clearly, listen actively to both what was said and unsaid and ask inquiring questions that advanced the dialogue. All participants needed to be open and prepared to share their experiences and queries. Both scientific researchers and clinical co-researchers needed to be given sufficient opportunity to fully express themselves. Also, in that the dialogues took place over a 6-month period, some fluctuation was seen in regard to the number of participants participating in each dialogue. We do not, however, consider this to have affected the results: three core groups of 5–7 participants per group participated in each dialogue, the dialogues took place on numerous occasions, and a sufficient number of participants were present each time. Furthermore, all those participating in the study were given the opportunity to influence both the content and formation of the EPM during a conclusory meeting.
To facilitate an evaluation of the dialogues from an application research perspective, a questionnaire consisting of both open-ended and close-ended questions was distributed to all participants 1 week after the final dialogue took place. With the questionnaire, we sought to capture whether or not the dialogues contributed to new understanding of the research subject and whether any eventual new understanding also contributed to a change in the clinical co-researchers perceptions of how they should “be” or act as carers. The clinical co-researchers expressed that their participation had affected their ethical thinking and their ethical sensitivity had increased. We found that they engaged in new actions after reflection, seen as new habits in daily working life. Through the application research design, basic values could be perceptible and active in care practice, that is, scientific theory became visible, which is a methodological strength.
Conclusion
The aim of this study was to gain further understanding of the ethical values central to the realization of sustainability in care and create an EPM whereby these basic values can be made perceptible and active in care practice. Through an application research design that included dialogues between Caring Science researchers and clinical co-researchers, dignity, respect, responsibility, invitation, and vows emerged as the ethical values central to sustainability in care. The EPM created during this study was intended to be used as a tool to help carers better understand an organization’s common value base and what such means for sustainability in care. The EPM can also be used to oppose the ethical erosion that Världsmedborgaren warns about.
Footnotes
Acknowledgements
We thank all who participated in this study. L. Nyholm has contributed to design and writing the final version to be published. S.S. has contributed to design and revising the article critically. L. Nyström has contributed to conception, drafted the article, and analyzed qualitative data. C.K. has contributed to design, conception, and drafted the article.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Principles of research ethics were strictly observed throughout the study. Consent for the study was obtained from the participating care organization’s upper management.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vaasa Central Hospital District has allocated EVO funding for this study.