
Abstract
Background:
When healthcare personnel take part in military operations in combat zones, they experience ethical problems related to dual loyalties, that is, when they find themselves torn between expectations of doing caring and military tasks, respectively.
Aim:
This article aims to describe how Swedish healthcare personnel reason concerning everyday ethical problems related to dual loyalties between care and military tasks when undertaking healthcare in combat zones.
Design:
Abductive qualitative design.
Participants and research context:
Individual interviews with 15 registered nurses and physicians assigned for a military operation in Mali.
Ethical considerations:
The participants signed up voluntarily, and requirements for informed consent and confidentiality were met. The research was approved by the Regional Ethics Review Board in Gothenburg (D no. 816-14; 24 November 2014).
Findings:
Three main categories emerged: reasons for not undertaking combat duties, reasons for undertaking combat duties and restricted loyalty to military duties, and 14 subcategories. Reasons for not undertaking combat duties were that it was not in their role, not according to ethical codes or humanitarian law or a breach towards patients. Reasons for undertaking combat duties were that humanitarian law does not apply or has to be treated pragmatically or that it is a case of force protection. Shortage of resources and competence were reasons for both doing and not doing military tasks. Under some circumstances, they could imagine undertaking military tasks: when under threat, if unseen or if not needed for healthcare duties.
Discussion/conclusion:
These discrepant views suggest a lack of a common view on what is ethically acceptable or not, and therefore we suggest further normative discussion on how these everyday ethical problems should be interpreted in the light of humanitarian law and ethical codes of healthcare personnel and following this, further training in ethical reflection before going on military operations.
Keywords
Introduction
When registered nurses (RNs) and physicians (MD) (henceforth licensed medical personnel (LMP)) undertake healthcare in a military combat zone, they are exposed to various ethical problems, for example, having to prioritise scarce resources, being obliged to choose between caring for enemies and allies, being caught between military and medical duties and causing a conflict involving dual loyalties. 1 –7 In earlier research on ethical problems in military medicine, the focus has been on exploring severe types of ethical problems when healthcare personnel take part in clearly unlawful actions, for example, assisting in torture-like situations intimidating patients, or intentionally inflicting pain on a person for the purpose of obtaining information. 8 –11 This branch of research has mainly been focused on the role of physicians.
However, the ethical problems focused in this study are more everyday ethical problems where the guiding laws and regulations might not give clear advice or instruction as to what to do. This study also includes nurses’ perspectives. The everyday ethical problems in this study have to do with dual loyalties, that is, choosing between providing medical care and performing military actions that per se may be lawful and beneficial for the military mission. 1,12 –14 This problem has also been observed in other studies, but we have found further examples illustrated by the following typical situations: (a) that LMPs gathered information they claimed to be intelligence when providing care for citizens of the host nation; (b) that LMPs performed guard duties in the Tactical Operations Centre i,15 at the military camp and at the main gate, that is, the entrance to the camp; and (c) that LMPs also filled vacancies and became temporary healthcare personnel, that is, primarily combatants and secondarily healthcare personnel.
In these cases, LMPs might have breached the ethical rules and principles that should have guided their actions. General ethical rules and codes are, for RNs, the International Council of Nurses (ICN) Code of Ethics for Nurses 16 and, for MDs, the World Medical Association (WMA) International Codes of Medical Ethics. 17 Both professions must comply with the codified ethical rules in national healthcare legislation (in this case Sweden). 18 Besides these ethical rules, humanitarian law also applies in combat zones. 19 When LMPs are exclusively assigned to healthcare duties, they must be equipped with a Red Cross ID, issued by the International Committee of the Red Cross, and wear a Red Cross armlet according to humanitarian law. 20 –22 This emblem signifies being a non-combatant, that is, not taking part in hostile actions and only using weapons for self-protection and for the protection of patients. Every country’s LMPs implement healthcare, and some, like Swedish LMPs, are uniformed and armed since they are member of military units and may look like combatants. 23 In employment by the armed forces, LMPs receive preparatory and military training before rotation to combat zones. The military preparation, a basic military training course, aims to convey practical and theoretical knowledge to increase understanding about the military organisation and to develop basic military skills. They also train combat techniques, even though they are non-combatants. Discipline, the importance of good military spirit and the ability to work in groups characterise these preparations. Also included is specific training aimed at imparting knowledge and understanding of problem-solving in combat zone contexts, that is, of how to supply the required nursing and medical skills in a specific combat zone. 24
As it is documented that LMPs can side both with the medical and the military in cases of dual loyalty, it is important to know their respective reasons for doing so. Both to understand how they view their role in the military and to be able to assess to what extent the reasons provided are legitimate given ethical codes and rules that are supposed to guide their operation. Now, there is a knowledge gap on how LMPs reason when they face the types of everyday ethical situations listed above.
Aim
This study aims to describe how Swedish LMPs reason about everyday ethical problems stemming from dual loyalties when providing healthcare in combat zones.
Method
Design
A qualitative content analysis 25 has been used to elucidate the arguments used by LMPs relating to dual loyalties.
Setting
A semi-structured interview topic guide was developed 25,26 containing four vignettes presenting situations 1–4 (see Appendix 1). The purpose with using vignettes was to encourage the participants to reflect on ethical problems by presenting them with a potential situation they might encounter. 27 This guide was tested on participants belonging to a Swedish unit during a training session at the Armed Forces Centre for Defence Medicine in Gothenburg, late 2014. The participants were preparing for a peace enforcement UN operation (Chapter VII mandate) in a combat zone during 2015.
After the training session, the interview topic guide was modified based on the participants’ comments during the session. All the participants at the training session were orally invited to partake in individual interviews. Later on, the participants received an e-mail and were asked to confirm whether they would participate, and the ones who wanted to participate were interviewed.
The inclusion criteria required all participants to be LMPs and to have been stationed with the Swedish Armed Forces in a combat zone within the past 3 years.
Participants recruited for this study are presented in Table 1.
Demographic table.
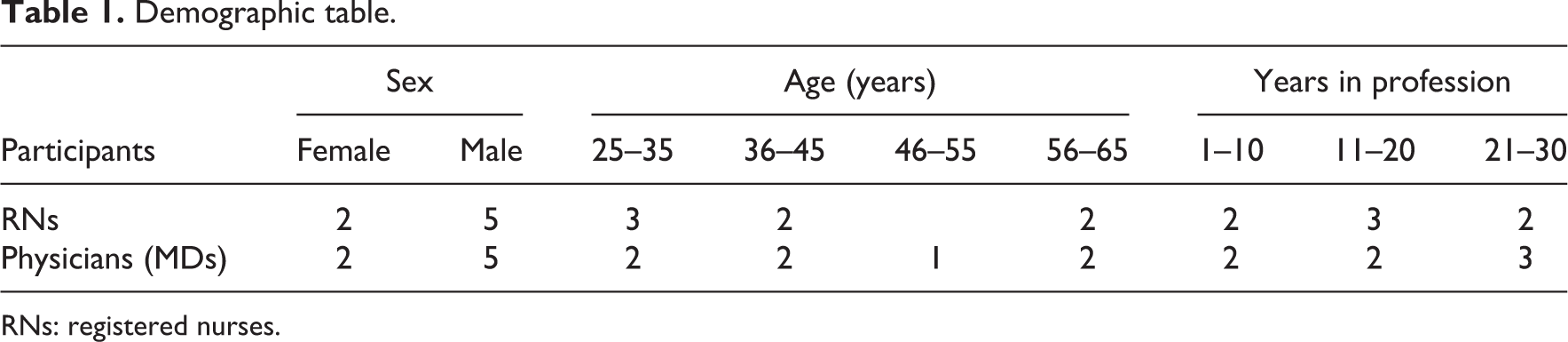
RNs: registered nurses.
Data collection
Using semi-structured individual interviews, LMPs were presented with the four vignettes and asked how they would reason about them. LMPs received the interview topic guide with the everyday ethical problems by e-mail before the interviews and also at the time of the interviews. The interviews were carried out at various places chosen by the participants. Before the interviews started, a short presentation took place and the interviews started with ‘small-talk’. 25 The interviews lasted between 35 and 90 min. They were digitally recorded and then transcribed verbatim by the first author. The first author translated the quotations in the results.
Data analysis
Example of the analytic process
The analysis began with the team reading the transcribed interviews over and over again. The first and last authors organised the data into manageable units of meaning, that is, sentences which described how the participants reasoned. Then a scheme was devised for the meaning units according to which they were coded. After reading the codes again, the codes were classified into subcategories and categories.
The team decided to let categories and subcategories be on a descriptive and manifest level to see the general patterns of how LMPs reasoned and related to dual loyalties. 25
Ethical considerations
This project applied for and gained the approval of the Regional Ethics Review Board in Gothenburg (D no. 816-14; 2014-11-24) since the research involved humans and sensitive questions were asked. 28,29 Informed consent was obtained. 25 Before the interviews, LMPs were informed about the aim and methods of the study, how the principle of confidentiality was to be upheld and how the concept of confidentiality would be applied to the data in this study. The LMPs were then reassured that they had the right to withdraw from the interviews at any time without providing reasons.
Findings
Three categories and 11 subcategories emerged from the data material (see Table 2).
Result table.

Reasons for not undertaking combat duties
Lacking military competence
When LMPs argued they would not do combat duties, that is, duties normally assigned to trained soldiers, one reason was that their specific competence was to implement healthcare by caring for patients. They claimed that they lacked military competence.
As LMPs are being exclusively assigned as healthcare personnel, they claimed they were not trained for combat duties. If LMPs were required to do combat duties, they would inform the military chiefs that they lacked the necessary competence. Combat duties may be of different kinds, but are defined as performing security tasks such as monitoring,
15
at a special command post for military operations. Normally, this command post consists of trained officers and is highly technical with a computer system for maintaining communications with soldiers and military chiefs inside and outside the camp. Therefore, one member of the healthcare staff argued, I would probably say no (to the chief) because I feel I do not really have the competence…to do it (serve in the Tactical Operations Centre) and I would tell him that I am not trained to do this and it’s not my job. (Interview 11)
When carrying out this particular combat duty, LMPs might also receive information requiring special competence which healthcare personnel normally lack, which would complicate things even further. They felt unsure about being able to handle experiences related to this service: ‘…but what shall I do with the information I receive? What will I be facing? I know it can be nasty stuff…it’s hard in my profession and I prefer to avoid this…since I find it a little scary…’, and ‘I’m not at all sure I can handle it and therefore I do not want to be exposed to that…’ (Interview 9)
Against the ethos of the care-giving role
According to participants, as LMPs they were employed in a care-giving role, which meant that their primary role was to carry out nursing and medical duties and to do military duties would go against the ethos of this role.
Sometimes, when they were being asked to undertake duties they meant were combat duties, LMPs referred to their ethical ethos of having a duty to benefit patients and not to hurt anyone: My duty on this operation was to be a nurse and to care for injured patients, and I did not want to be the one to hurt others. (Interview 9) LMPs are not supposed to be used as liaison officers in order to rig information…it would be like a sort of espionage under false colours – no…(Interview 10) If the locals find out that Swedish RNs and MDs are some kind of liaison officers, then we would put the patients in a precarious situation. (Interview 8)
Following the letter and intention of humanitarian law
LMPs argued that they should follow humanitarian law to the letter to live up to the intentions of this law.
First, LMPs argued that they had to follow humanitarian law as it applies in combat zones. According to humanitarian law, LMPs should not be involved in combat duties, as non-combatants and exclusively assigned as healthcare personnel. LMPs who carried out duties against the intentions of humanitarian law felt that they were acting against their healthcare assignment: I haven’t thought much about the ethics but this thing with the Red Cross armlet…if you are wearing it you shouldn’t end up in combat situations like that…as personnel with a Red Cross designation not should be doing guard duties and stuff like that…(Interview 9) It is not possible to use the Red Cross armlet now and then during the same mission. Either, one wears it during the entire mission, or does not wear it at all. (Interview 2) We follow the rules. One can always wonder if the enemy respects the rules, or if the Red Cross ID is a protection, but carrying an armlet means that you follow the regulations. (Interview 13)
Should prioritise healthcare and not military duties
Healthcare professionals adamantly rejected the idea that shortages of personnel to carry out combat duties could be used as a motivation for asking LMPs to fill in vacancies and undertake combat duties: No, vacancies are no reason to force licensed medical personnel with Red Cross assignation to assist with combat duties. (Interview 10)
Reasons for undertaking combat duties
Humanitarian law is not relevant
One reason for LMPs to undertake combat duties was that they did not find humanitarian law to be relevant in these kinds of operations. It could be about not taking humanitarian law seriously as when one participant said, We were equipped with the Red Cross ID, and so we were supposed to wear the armlet and so on, but it just fell off, and then no one was particularly eager to wear it…(Interview 7) But humanitarian law did not apply here…because then that would have meant it was a conflict between different nations, but this is a civil war which means us ending up in a gray zone…(Interview 7) I have no legal problem with humanitarian law…I don’t think you should turn your back on the law…but, at some point the system begins to sag a little and then, what is the most important? Keeping to the principles of humanitarian law or having a functioning monitoring centre? (Interview 2)
Having a military role and military competence
LMPs claimed that everyone in the troop could also contribute by undertaking military duties if they were qualified for them. If they had qualifications for military duties, and if they had been employed only as temporary (i.e. being primarily soldiers, and medical personnel when needed) medical personnel, LMPs would have carried out combat duties voluntarily. In such circumstances, this would have been natural. They explained that they felt part of the unit, dressed like the other soldiers, were equipped with weapons and had weapons training: Yes, well I would not have any worries about asking questions while I take care of patients and bandage them…or verify what happened around here…I have no problem at all with doing that. (Interview 12) I believe there’s a passage in humanitarian law, that if someone has to be body searched and it happens to be a woman, then if at all possible you have to find a woman soldier to do it, and if there’s no woman soldier available then you can ask a doctor to do it since he is supposed to be able to feel women up without kind of having the wrong attitude…I’m kind of sure that there is a passage about that there (in humanitarian law)…(Interview 10)
Doing one’s share
It was important for LMPs to participate in the military duties, they stated, since it would have been hard for them to motivate not taking part when they had no urgent healthcare duties. They wanted to show that they were happy to be able to shoulder their share of the duties: It was difficult to justify towards the other soldiers…when we were in combat zones, we made sure we shared guard duties when we were out on patrols and our colleague sat in the tower of the camp and did guard duty so…well, if it was right or wrong, I don’t know, but that’s how we solved it. (Interview 7) No problem at all, I’d jump for joy and rush into the monitoring centre and serve there…on a chair in a comfortable place with a cup of coffee in my hand…absolutely, no problem what-so-ever. (Interview 12) You can’t just be black or white because then you can’t work anymore. (Interview 2) Some of the RNs and MDs did guard duty at night and they didn’t wear the Red Cross armlet and nor were the vehicles marked with the Red Cross. They did guard duty every night…and they had to do it, otherwise it would not have been possible to carry out all the military duties. (Interview 12)
Contribute to force protection
LMPs saw carrying out duties that are actually combat duties as force protection, for example, preventive measures to mitigate hostile actions, for the sake of civilians. Force protection may also be seen as defensive actions. Thus, when LMPs described themselves as undertaking combat duties, they claimed, Serving in the monitoring centre or standing guard are defensive actions…I would not say no to doing that just for the sake of this principle (humanitarian law)…(Interview 12)
Restricted loyalty to military duties
Under specific conditions described below, LMPs would perform duties that are combat duties.
Undertaking combat duties when under threat
When LMPs were on patrol with soldiers in the villages and were giving healthcare to civilians, they received information, which they claimed to be intelligence. This information was passed on to an officer in charge if the patrol was under threat. Furthermore, LMPs also claimed that they undertook other combat duties, such as guard duties, when under threat. The reasons LMPs provided for accepting combat duties are exemplified by the following statement: The proper answer is that…I will not tell you. But, if there are obvious threats to our units…I would tell the military chief…But yes, basically I would not do it…But practically, it’s pretty easy to end up in an awkward situation, in an ethical dilemma. (Interview 11)
Undertaking combat duties if unseen
There were other occasions too when LMPs might undertake combat duties, especially if it was not obvious to civilians who they were when they were carrying out these combat duties: If no one sees me serving there (in the TOC), wearing a Red Cross armlet…I would do it…I’m obviously not very trained at it but I can respond to the messages…I probably know foreign languages better than they do (the soldiers), and no one outside can see that it’s me. (Interview 10) Standing at the main gate…well, then it’s obvious who I am, I’m visible, and that may harm the confidence people have towards the Swedish troops so…that’s obvious and therefore not possible. (Interview 3)
Undertaking combat duties if not needed for healthcare duties
The primary duty of LMPs was to provide healthcare for their own troop, if possible the allies and any injured civilians. If their services as LMPs were not needed, they might accept duties that they were not primarily employed for: Healthcare duty is always more prioritised than serving in the monitoring centre…I may assist there if it is necessary, but it’s not my number one priority job…(Interview 2)
Discussion
The results show that when LMPs are integrated into a military system in combat zones, two seemingly different value systems are combined, the healthcare and the military. This is shown when LMPs are reasoning around undertaking combat duties or not, if they are having the having competence or not for undertaking these duties, how they view humanitarian law, LMPs prioritising of resources and undertaking military duties when being under threat and when not being visible.
When LMPs referred to their competence, they had different perceptions of having the competence. Some of the LMPs claimed that they lacked the military competence, since they were primarily healthcare personnel and not trained in combat duties. They also claimed it was not in their role to undertake combat duties. The LMPs said that combat duties are normally undertaken by trained soldiers. For example, monitoring systems are not systems that automatically are understood by healthcare personnel, and that therefore technical skills or technical competence for these monitoring systems are often required. In this, their reasoning concerned practical skills and qualifications rather than reflecting around their ethical codes or their caring role. During preparation before rotating to a combat zone, ethics and ethical problems were discussed, but LMPs did not refer explicitly to their own ethical codes. It seems as if the practical skills involved in executing combat duties, that is, the competence per se, were of greater importance or at least more in the forefront of their thinking than ethical values and norms.
However, when claiming they had the competence in undertaking combat duties, LMPs did refer to a sense of justice, claiming that they belonged to a military unit and therefore should undertake military duties. The reasons then were that LMPs wanted to contribute through military duties, even if these duties were combat duties. Furthermore, LMPs were told during training that ‘everyone is a soldier’. Some of them may have interpreted this as allowing them to assist the soldiers with different tasks, even if that would have been combat duties. Besides, they found it hard to justify non-participation to their fellow soldiers, for example, if they refused duties such as standing guard at the entrance to the camp. But some of the LMPs are likely to be trained and have military competence and therefore competent to undertake combat duties, but may not have been aware that the duties can be combat duties and as such incompatible with the ‘healthcare’ mission (such as undertaking body search).
When LMPs are wearing the distinctive emblem, which designates they are exclusively assigned to caring duties, they should refrain from undertaking duties referred to as combat duties according to humanitarian law. 20 –22 However, today most armed conflicts are non-international, and a significant part of humanitarian law, that is, the Four Geneva Conventions from 1949 and the First Additional Protocol, 30,31 applies only in international armed conflicts. When Sweden partakes with a military unit in combat zones, the Second Additional Protocol may apply, 32 including Article 3 common to all four Geneva Conventions. 33 On the other hand, humanitarian law, which is closely related to human rights, is today included in what we refer to as customary law 19 and applies in non-international armed conflicts. In international armed conflicts, ‘combatant’ is defined as soldiers participating in the fighting squad 19 (Rule 3), and LMPs are clearly excluded from participating in such a squad. But in these non-international conflicts, in which Swedish LMPs participate, ‘combatant’ is not clearly defined. 34
Therefore, when LMPs were claiming that humanitarian law did not apply, they were referring to that they partook in non-international operations, where humanitarian law is not explicit about how to define ‘combatant’. The Swedish LMPs may not even have been aware of that the duties they partook in can be combat duties and then considered to be forbidden. Being uniformed and armed, belonging to a military unit and may appear as combatants, 23 the Swedish LMPs may even have viewed themselves as combat soldiers. Some of the armed conflicts Sweden has partaken in recently (Afghanistan and Mali) have been under a UN Chapter VII mandate, that is, peace enforcement conflicts, where the Second Additional Protocol and the common Article 3 applied. But when Sweden partook with soldiers outside the coastline of Somalia, the operation was governed by the Human Rights and Military Operation Rules (SOP) only.
However, customary law does explicitly condemn that LMPs partake in ‘hostile acts, outside their humanitarian function’. 19 An example of ‘hostile act’ may be ‘violation of neutrality’ and ‘act harmful against enemy’, 19 but customary law is not explicit if ‘hostile acts’ could be interpreted as being the duties which some LMPs take part in here. Normally, duties such as standing guard and gathering intelligence are combat duties and referred to as duties undertaken by combatant soldiers. 1 Since customary law is not clear, or explicitly forbid LMPs undertaking the duties referred to here, and do not clearly define combatants, 34 they may have reasons for diminishing the significance of humanitarian law and therefore have a pragmatic view on the law.
On these operations, there are sometimes shortages of LMPs, and even vacancies resulting in shortage of LMPs, resulting in that they have time for healthcare duties only. Even though they had time left and were not needed in healthcare all the time, some of the LMPs claimed that there were no reasons to undertake military duties, or combat duties, since it would have been a wrong priority of resources. However, in these situations, when not needed in their healthcare duties, some LMPs found it hard to motivate non-participation of military duties. They felt a pressure to undertake military duties, even if the duties were combat duties, which is seen in earlier research. 34 –38 But LMPs also referred to justice that it was fair to the peers if they also undertook other duties when not needed in the healthcare duties. If LMPs would not have contributed and undertaken these combat duties, the military tasks would not have been solved, LMPs reasoned. At the same time, even if it is understandable that it might be difficult to refuse doing such duties to enable their fellow soldiers to rest and recover, it might imply that the LMPs are tired and less focused when having to perform life-saving interventions. Further reasons for undertaking combat duties could be that LMPs also wanted to show that they were as much soldiers as anybody else and that they were not afraid of undertaking duties that were not caring duties. It has been voiced that LMPs can experience not being taken seriously as important parts of the unit, or at least as less important parts.
LMPs were sometimes willing to undertake combat duties if they remained unseen from external observers, such as serving in the monitoring centre. When serving there, only their own unit could observe that LMPs had a Red Cross armlet. For visitors at the military camp, LMPs would have been invisible. On the other hand, if LMPs would have been standing guard in the entrance to the military camp, it would have been visible for everyone who passed the entrance that LMPs were guarding. The rationale behind this would be that when wearing a Red Cross armlet it is obvious who they are and what function they have in the unit. 33 From an ethical perspective, this is a problematic reasoning, since there is a risk in undermining the confidence in Swedish LMPs if it is discovered that they act as potential combatants and thereby seemingly make exceptions to humanitarian law when it suits them. Consequently, that could have been risky for the whole Swedish LMP unit and also damage the trust for the Swedish Armed Forces.
LMPs are always obliged to prioritise caring for the patients and uphold a relationship built on trust and honesty in all contexts. This is extra important in combat zones where they represent what might be seen as a hostile military force. But there are circumstances when it is possible to interpret that LMPs are entitled to violate their obligations towards their patients. When a patient poses a risk, in armed conflicts or in peacetime, LMPs may use violence, according to the ethical codes for MDs in times of war. 39 In combat zones, the threats may be experienced as constant, and therefore LMPs may think they could use violence towards enemy forces or illegitimate warriors. Therefore, LMPs stated that under certain conditions, such as being under threat, they might undertake duties that were normally executed by combat soldiers, such as participating in a fighting squad.
In previous research, employment as healthcare personnel in the military is described as creating dual loyalties between healthcare duties and military requirements. 1,11,14,37,40 One may expect that their primary obligation should be towards their ethical codes, 17,41 that is, to put the patient first, care for the injured and reduce suffering, while at the same time being a part of a military organisation means being expected to facilitate and support killing. 42 In extreme situations, healthcare personnel were ordered to participate in torture which demand dual loyalties, 43,44 which is clearly against humanitarian law, ethical codes and human rights 45 (Article 5). However, in the everyday ethical situations described in our studies, some LMPs willingly undertook the military duties required from them. 14 Group pressure or group identification and loyalty rather than formal requirements seem to constitute the explanation for this behavior. 46 This is in line with some earlier research, for example, Gross 36 who wrote that healthcare personnel sometimes had to put their own ethics aside and carry out combat duties. Rubenstein 47 contested this however, claiming that humanitarian law and human rights laws and ethical codes 16,17,31,39,45,48 should guide healthcare personnel in all decisions. Kottow 7 argued somewhat sceptically that times have changed and that healthcare ethics in recent years seem to have become estranged from honouring principles like ‘do no harm’.
Reasons for dual loyalty may be that LMPs did not receive enough training and guidance to identify situations where dual loyalties violated human rights, and also where they risked setting their own ethics aside. Education in ethical codes and humanitarian law may be a powerful tool for reflection and resilience when faced with everyday ethical problems and may serve to prepare healthcare personnel and also their military chiefs and all the other soldiers in the unit. Integrating ethics and humanitarian law in training in the military context may also empower healthcare personnel to be more aware of what kinds of military duties they may and may not perform, if any. 49
It is apparent that the existing humanitarian law and customary law as well as ethical codes do not explicitly advise health professionals how to evaluate humanitarian contra military claims, especially when it comes to more everyday ethical problems. Nor do they give explicit advice on how to determine when the protection of patients’ human rights requires health personnel to put state interests aside.
Even if humanitarian law has been revised and become more adjusted to our times when most armed conflicts are non-international, that is, customary law, 19,34 it is perhaps once again time for a new, updated humanitarian law to be complemented with regulations concerning the kinds of everyday ethical problems we have found. 50 If not a revision, then a suggestion may perhaps be to identify the exceptions to this law where LMPs tend to experience dual loyalties, which is seen in this study. Another suggestion may be to tighten up the ethical codes and stipulate precisely which military duties healthcare personnel may perform when employed in the military despite being exclusively assigned to healthcare.
Although healthcare personnel do not perform military duties that could be interpreted as hostile, there are reasons to be explicit about which military duties their own ethics and humanitarian law allow them to undertake. Military organisations tend to be explicit, but here it seems as if LMPs choose to undertake military duties.
One suggestion for further research is to investigate how military chiefs view their LMPs executing combat duties and how they view the ethical problems discussed here. Since LMPs have only fragmentary knowledge of humanitarian law, another area of research is to investigate how military chiefs are educated in humanitarian law and the relationship between their training and knowledge and the training and knowledge of subordinates. A third area of research is whether there are parallel situations of dual loyalties in civilian healthcare which can help shed light over dual loyalties in military healthcare and vice versa.
Conclusion
The study shows that LMPs reason differently in relation to potential dual loyalty situations. Some provide reason from abstaining doing military tasks referring to competence, role, humanitarian law and ethical codes and lack of resources. However, others provide reasons for doing military tasks with or without restrictions, referring to views on humanitarian law, competence, lack of resources or demands or aspects in the situation. To some extent, the LMPs seem to be ignorant about to what extent humanitarian law applies, but there is also lack of explicit guidance in relation to these situations and some room for interpretation in humanitarian law. Even if the duality in LMPs is understandable, it is problematic that they do interpret their obligations in the combat zone differently, and there is reason to further explore how a more consistent approach could be achieved, for examples by further training and reflection on ethical issues before rotation to combat zone.
Methodological considerations
Credibility was supported by the first and third authors being involved in the analysis process of data and using quotations from participants, and also by ensuring that the findings represent the data analysed. 51 Dependability was supported using the same topic guide and interview questions with all the participants. Confirmability was supported by all authors being involved in the process of reading the condensed codes and naming the categories. 51 Confidence in the interviewer (first author) and third author was established before the interviews, since they met the participants during the education session. The first author has served in the same context as some of the healthcare personnel, although she was stationed as a military chaplain since she is a priest in the Lutheran Church of Sweden. Due to this, it was important to emphasise to interviewees that this was an interview for a study and not a pastoral counselling, and to maintain reflexivity. The results may be transferable in other care situations where dual loyalty is experienced. 52 If any the participant had so wished, the interview would have been terminated without any questions being asked. This did not happen however.
Footnotes
Authors' note
The authors' current affiliations are: Kristina Lundberg: School of Health and Welfare, Jönköping University, Sweden. Sofia Kjellström: Jönköping Academy for Improvement of Health and Welfare, School of Health and Welfare, Jönköping University, Sweden. Lars Sandman: Department of medicine and health, Linköping University, Sweden.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by the Faculty of Caring Science, Work Life and Social Welfare, University of Borås, Borås, Sweden.
Note
Appendix 1
The four ethical problems were as follows: You are out on patrol, and arrive in a village where suspected enemy forces have passed. Of course your commanding chief wants you to see if there is any need of care and at the same time try to find out things about who has been in the village and what they did there. How would you act? Why are you doing that? How come you think like this? Why do you think so? When you thought of this, how did you think? Do you see this as an ethical problem and why in that case? (What is the ethical problem?) Have you been involved in similar cases? Your military chief tells you to serve in the Tactical Operations Centre (TOC) and relieve the guards there because they need to rest and for the moment you do not have any patients. (Sometimes the Senior Medical Officer (SMO) is in the TOC, but here we meant the guard duties.) How would you do? Why are you doing that? How come you think like this? Why do you think so? When you thought of this, how did you think? Do you see this as an ethical problem and why in that case? (What is the ethical problem?) Have you been involved in similar cases? It is calm at the camp, all appear to be well and there is an exercise going on outside the camp where many of the soldiers partake. Your military chief thinks you can go to the main gate and be part of the guard. How do you act? Why are you acting like that? How come you think like this? Why do you think so? When you thought of this, how did you think? Do you see this as an ethical problem and in that case why? (What is the ethical problem?) Have you been involved in similar cases? You have arrived in combat zone when you are told that there are many vacancies among the soldiers. It would be more convenient for the Armed forces if you were temporary healthcare providers, that is, being primarily combatants and if necessary, secondarily, being in your healthcare role. How would you do? Why are you doing that? How is it that you think like this? Why do you think so? When you thought of this, how did you think? Do you see this as an ethical problem and why in that case? (What is the ethical problem?) Have you been involved in similar cases?