
Abstract
Background:
The nature of children’s cancer comes with lots of ethical issues. Nurses are encouraged to adhere to ethical codes in their practice.
Objectives:
This study aimed to compare the perspectives of nurses and mothers of children with cancer regarding the adherence of nurses to ethical codes.
Research design:
In this descriptive-comparative study, a researcher-made questionnaire was used to assess the amount of adherence to Iranian nurses’ code of ethics in perspectives of pediatric oncology nurses and mothers. As a convention, the total scores were categorized as optimal, average, and low adherence.
Participants and context:
A total of 200 mothers and 60 nurses in pediatric oncology wards of five major hospitals in Tehran, Iran, participated in 2016.
Ethical considerations:
Organizational approval by the university and informed consent were ensured before conducting the research. The principles of voluntariness, confidentiality, and anonymity were respected during the research process.
Findings:
Results showed the mean score of the adherence to ethical codes by nurses, as per the nurses is 86.71 (12.57) and as per the mothers is 78.67 (16.09). The highest frequency for “Low adherence” and “Optimal adherence” to code of ethics by nurses were “Respect for individual autonomy and decision-making” (mothers, 72% and nurses, 70%) and “Commitment to confidentiality” (mothers, 64% and nurses, 74%), respectively. This revealed a significant difference between the responses of the nurses and the mothers (p = 0.001).
Discussion:
The results support the other studies in Iran about the difference between the perspectives of patients and nurses about adherence of nurses to ethical codes.
Conclusion:
Integration of family-centered and conventional care in addition to more attention to the education of professional ethical principles could be helpful to improve the ethical performance of nurses in oncology pediatric wards.
Introduction
Cancer is one of the most challenging diseases during childhood. In addition to physical and psychological suffering of child, families may improve many psychological health problems, such as anxiety and depression. 1 The nature of cancer comes with certain sensitivity, and it brings lots of ethical issues. 2 This becomes even more complex, when it is related to pediatric population. 3 Issues such as informed consent pertaining to begin or continuation of a treatment, decision-making with respect to the care policy at the end of life stage, matters related to pain and suffering, upholding integrity with children and families, as well as giving bad news, are among the ethical topics in the field of pediatric oncology, with which care professionals are often faced. 4,5
Having an ethical and spiritual approach is one of the requirements of disciplines that provide services for humans. Nursing is one of the professions for which ethics is an essential part for an optimal performance. 6 Nursing is an independent discipline, the mission of which is to provide healthcare, treatment, and rehabilitation services at the highest possible standard to protect and promote the health of a community and the individuals within. A way to evaluate ethics in is to define the acceptable ethical behaviors in particular situations in the form of ethical codes. 7 The development of ethical codes tailored to culture and religion of a society is the best strategy to improve the quality of nursing services expected by the people concerned. For the last decades, developing ethical guidelines are considered a major priority in healthcare in Iran. It is believed that Iranian nurses adhere to ethical principles according to their religious belief system, or rely on some international ethical declarations. This might cause a lack of unity in their practice. To outline standards of ethical professional practice in different levels, ethical codes for nursing were developed in this regard, aiming to provide a working framework and an Islamic-based ethical decision-making and practice guide for nursing. 8 In 2010, a group of experts submitted the “Iranian nursing code of ethics” with 12 values, and 71 ethical guidelines to the Supreme Council of the Ministry of Health and Medical Education. This declaration was formulated after a broad review of literature on code of ethics of international nursing organizations, such as the International Council of Nurses, analyzing the data throughout a 6-month period, and adopting them to the social, cultural, and religious context of the country. The experts evaluated the codes through four focused-group discussions including 40 clinical nurses; and the final draft was developed following some disorderly surveys to achieve more consensus between professional associations. 9,10 The “Iranian nursing code of ethics” received the final approval for application at the second meeting of this Council on 4 March 2011. Since then, it is included in the main curriculum’s outlines of nursing programs and some sporadic in-service training workshops have been provided for nurses to get familiar with the codes or to specify them in their own field of practice. Although the legal audit for nursing errors in Iran is integrated with a general system of audit for all medical and healthcare providers, under supervision of the Ministry of Health and Medical Education, the guidelines derived from the code of ethics for nurses are congruent with the related regulation, makes it possible to audit ethical performance of nurses. 10,11
Since the announcement of the decrement, researchers have conducted various studies regarding the adherence to nursing code of ethics. Most of these studies evaluate the perspective of nurses or nursing students in this regard. 10,12 The studies that compare adult patients’ and nurses’ perspectives show that there are differences of point of views between the two groups about the ethical performance of nurses. 8,13 –15 Some reasons have been mentioned in the related literature, such as less assigned priority to the topic of ethics in nursing programs or a dominance of task-oriented approach in nursing practice in Iran. Despite many generalities of these results, applicable for all fields of nursing, more clear conclusion in the field of pediatric oncology nursing needs specific studies. According to our knowledge, no study has been done on perspectives of families of children with cancer about nursing adherence to ethical codes and to compare them with the point of views of nurses. It is important to know any disagreement to provide promoting interventions. Fathers are the legal guardian and responsible of decision-making for minors in the country, but most of the diagnostic/treatment practices are done in a context that both parents are involved. In addition, for cultural reasons, mothers are the main care providers of children and only ones who can stay with them in hospital. Because of the nature of the disease and its treatment, multiple and lengthful nurse–mother encounters happen, which increase the possibility of more challenging relationships and occurrence of ethical-related issues. Mothers are therefore better judges on nurses’ adherence to ethical codes. Their point of view and its comparison with what nurses understand of their actual performance offer a clear picture of the state of ethics in the fields of pediatric oncology. The disagreements will show the specific fields of ethical issues of nurses, which need to be improved, and noticed by educators and managers in pediatric oncology nursing fields. The results would be helpful for other countries, which have similar cultural context.
Purposes
The overall purpose of the study was to compare the perspectives of mothers and nurses about adherence to professional ethical codes in Iran by nurses in the care of children with cancer. The research questions were as follows: What is the perspective of mothers of children with cancer on nurses’ adherence to the professional ethical codes in children’s oncology wards? What is the perspective of nurses on their adherence to professional ethical codes in the children’s oncology wards? Is there any association between demographic characteristics of nurses and mothers of children with cancer and their perspective on a nurses’ adherence to the ethical codes in children’s oncology wards?
Materials and methods
Study setting
This descriptive-comparative study was carried out in the oncology wards in five educational publicly funded specialized hospitals in Tehran, the capital of Iran. Four of the hospitals involved were specialized centers for children and one was a general hospital with a children’s oncology ward. These centers are the reference of many cities in northern, central, and western parts of Iran due to their position in the capital. The study population concerned mothers of children with cancer and nurses employed in oncology wards of these five hospitals.
Participants
All nurses working in children’s oncology wards, and 200 mothers who met with the inclusion criteria were selected. Inclusion criteria of the mothers were, being at least 18 years old, having their child admitted for at least 24 h, having a definite cancer diagnosis for that child, being mentally capable of answering questions, and not suffering from severe anxiety or depression according to themselves (any recent hospitalization for mental problems was asked to exclude the conditions in mothers that can affect their emotions and judge).
Data collection
Convenience quota sampling for the mothers was done within 6 months and according to the average of children admitted to the hospitals involved. The researcher referred in succession on odd or even days on different shifts to the research environments; and collected information. A number of 40 was chose for each hospital based on a relatively equal number of beds. The nurses of the pediatric oncology wards of studied hospitals were selected with census method in the same interval. All nurses of all shifts completed the self-report questionnaires in their work break. The researcher was present at all times during the completion of the questionnaires. The mothers completed their relevant questionnaires with assistance of the researcher while sitting near the bed of the child she was taking care of.
For the data collection, two different questionnaires in Persian were designed for the separate study groups. Each questionnaire had two parts: (1) demographic information and (2) questions associated with ethical codes. The second part of the questionnaire contained 28 items in 8 of 12 ethical values, mentioned in Iranian nurses’ ethical codes, includes “Respect for child and his family” (five items), “Patient (child and family) education” (three items), “Respecting the autonomy and decision-making” (four items), “Commitment to Integrity” (two items), “Commitment to justice” (two items), “Commitment to Confidentiality” (two items), “Conscientiousness” (four items), and “Improving the quality of care” (six items), by scoring as per the Likert scale for choices: never (0), rarely (1), sometimes (2), often (3), and always (4). The 12 ethical values include. 16 The other four values have more concerned with the ethical practice in the fields of research, education, and professional development.
The minimum total scale score was zero and the maximum score was 112. In analyzing the findings, responses of “never,” “rarely,” or “sometimes” were classified as “low adherence,” the response of “often” as “average adherence” and response of “always” was rated as “optimal adherence.” This means that the total score of less than or equal to 56 qualifies as “ low adherence” to the code of professional ethics by the nurses involved, score 57–84 as “average adherence” and a score of 85–112 as “optimal adherence.” This categorizing was conducted to compare the perspectives of participants about the adherence of nurses in oncology pediatric wards to ethical codes.
To determine the face validity and content validity, the questionnaires were given for evaluation to 10 faculty members, experts in the field of nursing ethics, and pediatric nursing of the following universities: Shahid Beheshti University of Medical Sciences, Iran University of Medical Sciences, and Tehran University of Medical Sciences.
After adopting on items of the questionnaire based on content experts and target group’s recommendations, a panel of 15 nursing experts in the fields of oncology and ethics was invited to verify the content validity of questionnaire. The Content Validity Index (CVI) was computed for each item on the scale (I-CVI) as well as for the overall scale (S-CVI). For each item the I-CVI was computed as the number of experts giving a rating of either 3 or 4, divided by the number of experts. The items that had I-CVIs of 0.78 or higher were retained. The S-CVI was computed using the averaging method (S-CVI/Ave). The degree of relevance for the entire questionnaire was S-CVI = 0.90.
In order to determine the internal consistency reliability of the questionnaires, Cronbach’s alpha coefficient was calculated, which obtained 0.93 for the questionnaire related to the mothers, and 0.92 for the questionnaire related the nurses. In order to evaluate the stability reliability of the instrument, test–retest method was used. To conduct the research, the questionnaire was handed out to 10 mothers of children with cancer who were hospitalized and to 10 nurses working in the pediatric oncology wards of the hospitals involved in a preliminary study. After collecting the data in two phases (a 2-week interval), the interclass correlation coefficient (ICC) of 0.95 for mothers and 0.98 for nurses was obtained.
Data analysis
The collected data were analyzed using the SPSS statistical software (v 17). Descriptive statistics, included frequency, percentage, mean, and standard deviation were used to describe the demographic information and the perspectives of the participants. In addition, t-test and Mann–Whitney were used to describe the differences between two groups in their mean of overall scores and each item of the questionnaire, respectively. In addition, Pearson’s correlation coefficient and Spearman coefficient were used to assess the correlation between the mean of overall scores of the questionnaire in each group with their own demographic characteristics. To compare the means of scores for the questionnaire in multiple groups of each demographic characteristic, the one-way analysis of variance (ANOVA) was used.
Ethical considerations
In the process of sampling, in order to ensure adherence to the research ethics, such as a clarification about the purpose of the study, their right to choose to participate or cancel their participation, reassuring them about the confidentiality of the personal data accumulated and refraining from publishing names or other personal details in the questionnaire and reports, procedures were monitored by The Ethics Committee of Shahid Beheshti University of Medical Sciences in the relevant stages of this study (IR.SBMU.PHNM.1395.400).
Findings
Participants
Nurses
All nurses were working in pediatric oncology wards for over 6 months at the five hospitals involved, had a bachelor’s degree and higher, and willingly participated in the study. Thus, 60 nurses with inclusion criteria participated in the study. All nurses were females (100%), among which the majority were married (53.3%), in the age group under 30 (41.7%), had bachelor’s degree in nursing (91.7), with an experience of less than 6 years (53.3%). Of these, only 14 them (23.3%) passed the professional ethics courses when they were in-service training (Table 1). This short-time non-endorsed courses had been held in one center to help nurses achieving their necessary annual job-improvement scores.
Demographic characteristics of mothers and nurses.
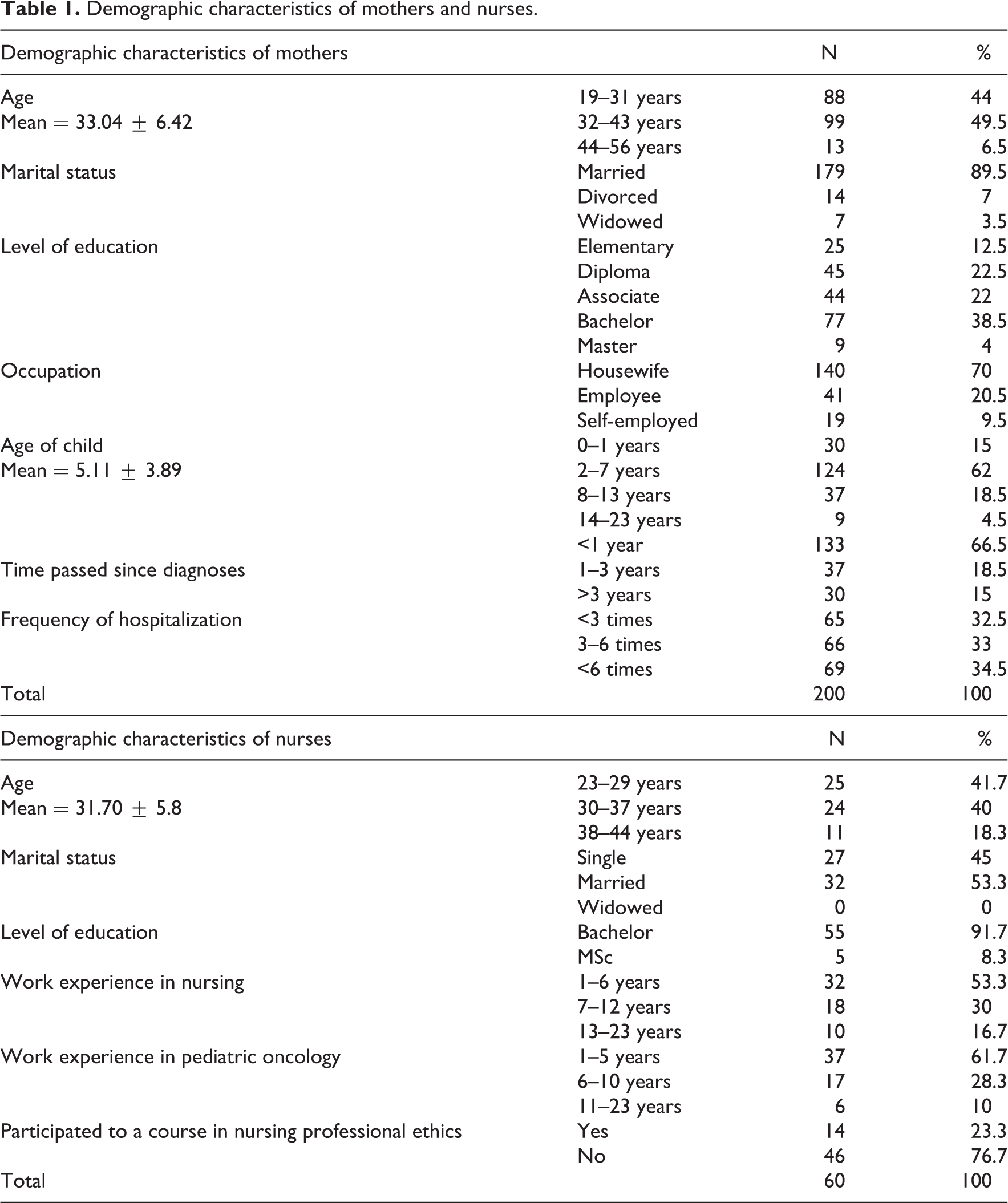
Mothers
In all, 200 mothers were enrolled in the study. The majority (89.5%) of them were married, 49.5% were in the age group of 32–43 years old, 38.5% had a bachelor’s degree, and 70% were housewives. The majority (62%) of their children were in the age group of 2–7 years old with the elapsed time since the diagnosis less than 1 year (66.5%), while parts of the children (34.5%) were hospitalized more than 6 times (Table 1).
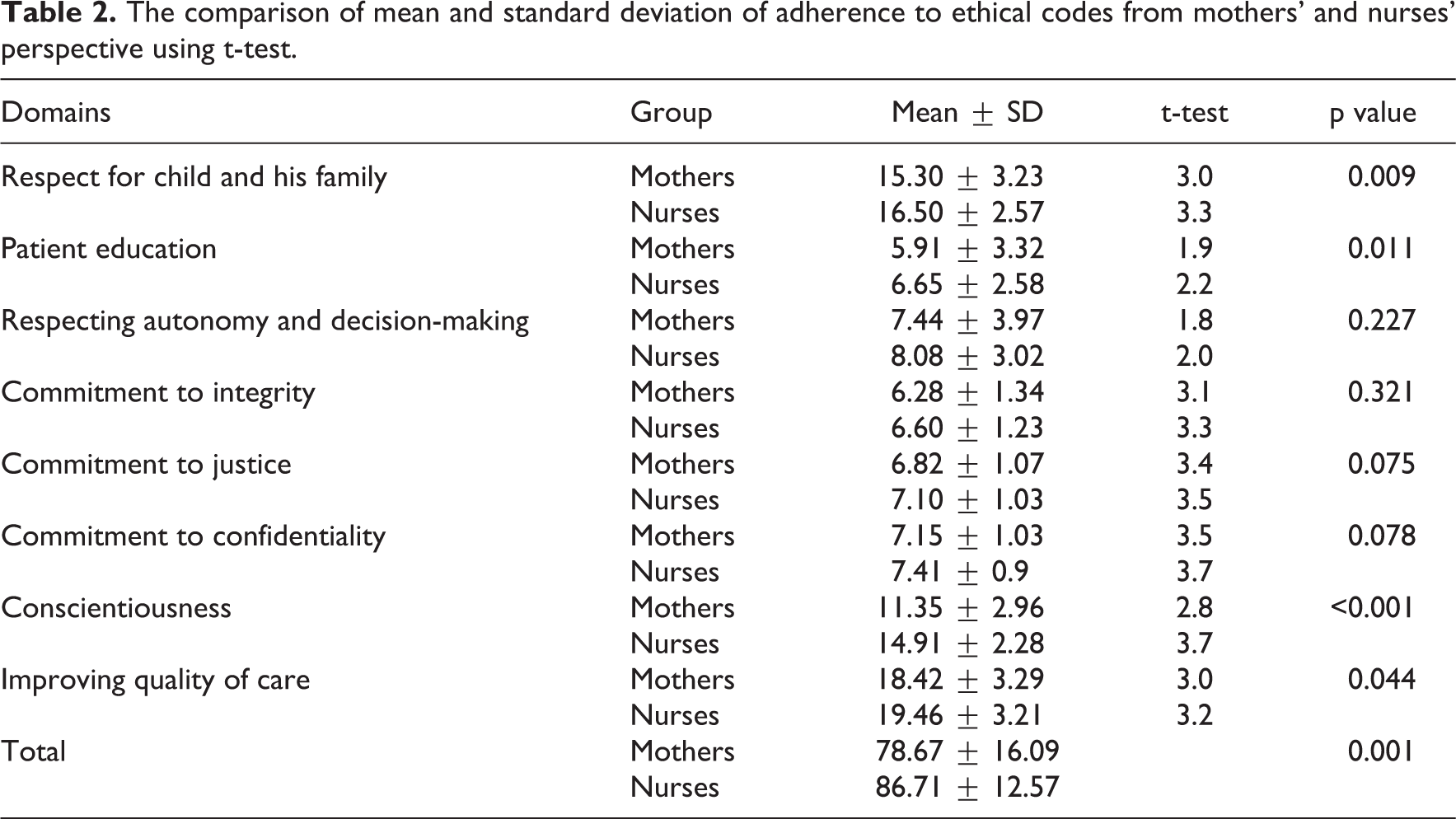
Distribution frequency of adherence to ethical codes by nurses as per the perspective of the mothers and the nurses and comparing the average in each domain as per the perspective of the mothers and the nurses are given in Table 2. According to statistics, the mean score of the adherence to ethical codes by nurses, as per the nurses is 86.71 (12.57) and as per the mothers is 78.67 (16.09). The independent t-test results show that there is a significant difference between the two groups (p < 0.001). In addition, independent t-test showed that there is a significant difference in these two groups in terms of “Respect for child and family,” “Patient education,” “Conscientiousness,” and “Improving the quality of care.” This means that from the perspective of the mothers, nurses’ adherence to ethical codes in these areas was less than what the nurses themselves think about their performance.
The comparison of mean and standard deviation of adherence to ethical codes from mothers’ and nurses’ perspective using t-test.
In the evaluation given by both groups, the highest frequency for “Low adherence” to the codes of ethics by nurses was in the area of “Respecting autonomy and decision-making” (mothers, 72% and nurses, 70%) (Chart 1). The highest frequency for “Optimal adherence” in the view of both groups was within the scope of “Commitment to confidentiality” (mothers, 64% and nurses, 74%) (Chart 2). In addition, frequency for average adherence of nurses to professional ethical codes in each of the domains studied from the perspective of mothers and nurses is shown in Chart 3.
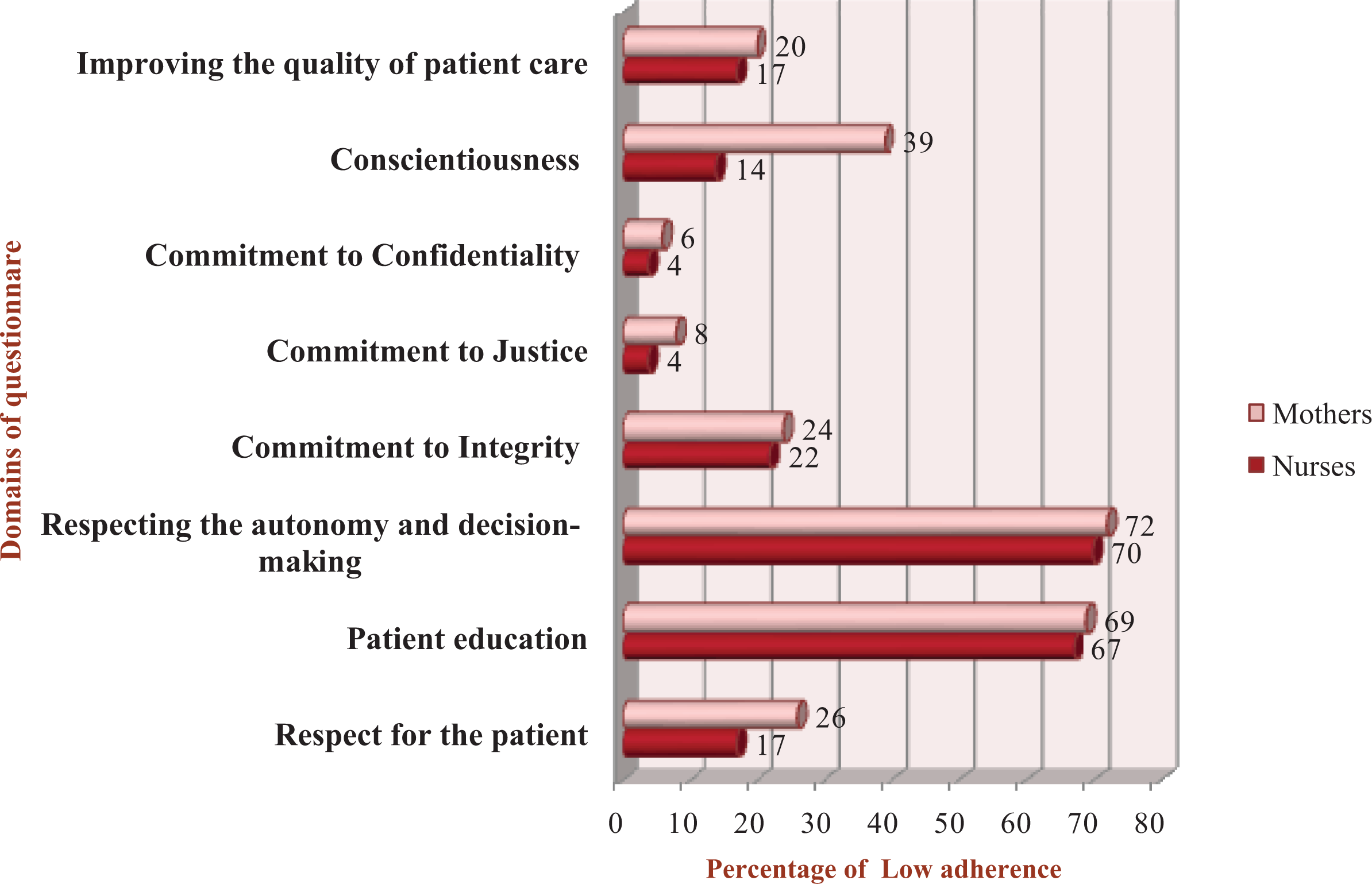
Frequency of adherence of nurses to professional ethical codes in each of the domains studied from the perspective of mothers and nurses (low adherence).
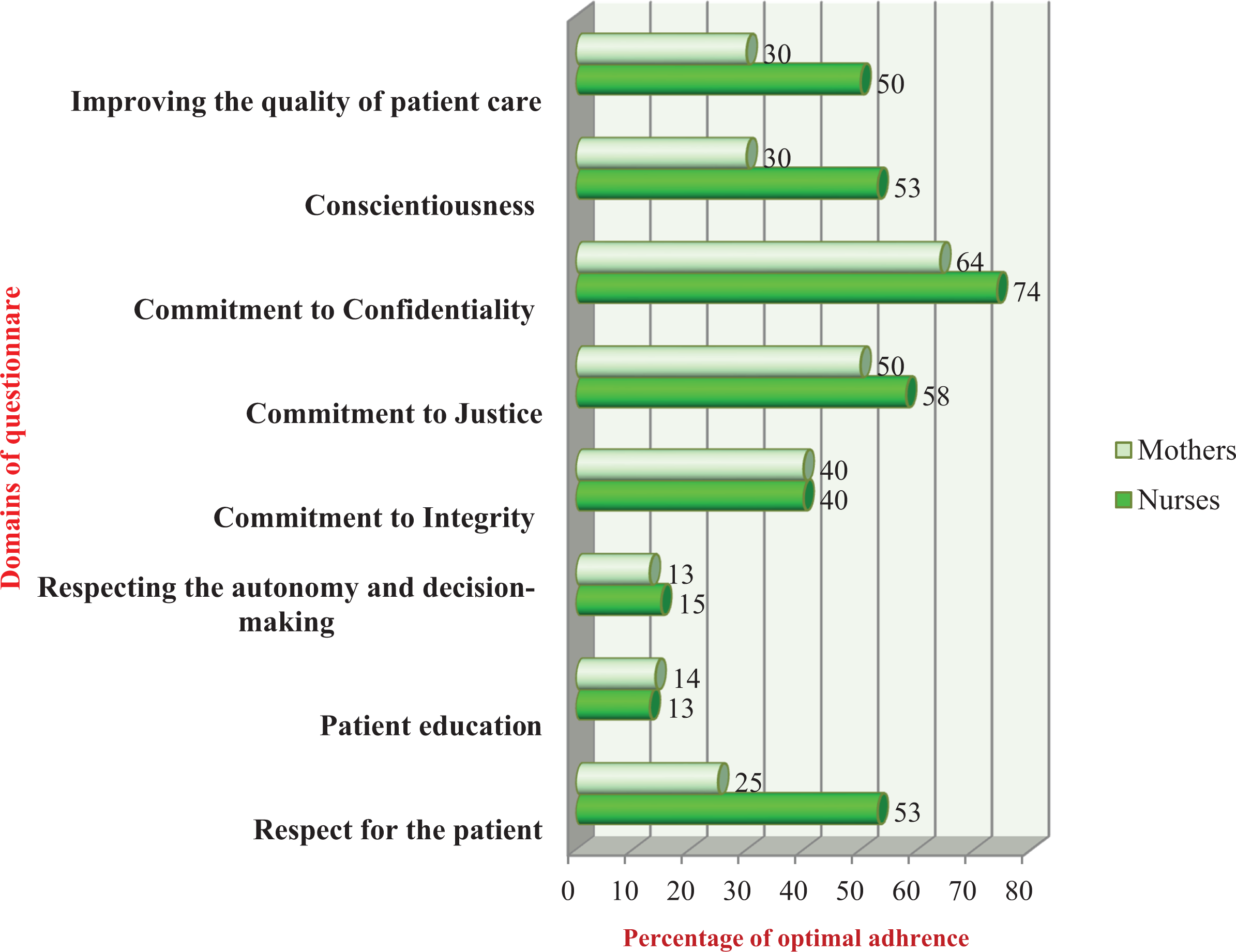
Frequency of adherence of nurses to professional ethical codes in each of the domains studied from the perspective of mothers and nurses (optimal adherence).

Frequency of adherence of nurses to professional ethical codes in each of the domains studied from the perspective of mothers and nurses (average adherence).
Pearson’s correlation coefficient showed that there is a significant relationship between the age of children with cancer (r = 0.59), frequency of hospitalization (r = 0.59), and the time elapsed since diagnosis (r = 0.78) with the perspective of mothers about adherence to ethical codes by nurses (p < 0.001). An increase in each of the above variables led to the outperformance of nurses better in adherence to ethical codes from the perspective of the mothers. t-Test showed a significantly difference between two groups of nurses with and without the experience of passing a professional ethics course in their mean of overall score to the questionnaire (100.78 ± 8.18 vs 86.7 ± 9.86, p < 0.001), showing the course has led to more overall score in the questionnaire of the study.
Discussion
The results showed that adherence to ethical codes by nurses was at an optimal level in the perspective of nurses, and at an average level in the perspective of the mothers. These results are consistent with most of previous research conducted in Iran, where the patients’ point of view on adherence to ethical codes by nurses was different from that of the nurses’ perspective, 17,18 while in some studies, the patients as well as nurses considered the adherence to ethical codes by nurses at an optimal level. 12,14 On the other hand, all the studies were conducted on adherence of ethical codes by nurses taking care of adult patients. The nature of care for children, especially in pediatric oncology ward, needs different considerations. A qualitative study on nursing students investigating adherence to privacy by nurses in pediatric wards indicates that this ethical behavior is not observed properly by nurses when dealing with children. 19 Other studies concerning perspective about nursing care in the pediatric wards suggests that the mothers are not satisfied with the services offered, of which some are mentioned in the ethical codes of nurses in Iran. For example, in the study of Aslanabadi and Shahbazi (2014), there was a ranking of low adherence to the “Provision of information by nurses” and “Providing time to talk to mothers.” Both items are mentioned in the questionnaire of this study, in the areas of “Patient education” and “Respect for child and his family,” and confirms the results of the study. 20 The results of other studies in the field of mothers’ perspective on the care provided to their children, show items like “Nurses’ communication with parents” and “Provision of information” have low scores for adherence to. Maximum scores were related to “The clinical nursing services.” 21,22 Duly observing of the ethical standards in nursing and nursing care by the nurses leads to improved quality of clinical practice and healthcare, and thus the efficiency of nursing. At a first glance, practicing of nursing can be considered as clinical and separate from ethics, while ethics and clinical practice should not be separated. 13 However, many studies suggest that nurses often focus on the technical aspects of their profession about which, patients were mostly satisfied. High satisfaction in this aspect can be due to the controlling and monitoring of the managers, the high priority of technical care, and the excellent skills of the nurses in this domain. 23 On the other hand, the still-current dominant medical paternalism in the healthcare system of Iran prohibits proper interaction and information giving between staff and patients. According to Taleghani et al., 24 mothers in pediatric oncology wards require more than anything that they have a relationship with the nurses of their children, who is based on sympathy and full support. They need their educational needs to be met with information relevant to the disease and treatment process, comprehensive, and humanistic understanding to alleviate the suffering of children. They feel that nurses put an emphasis on their technical-professional work and allocate little time to such care. This negatively affects the humane and ethical aspects of nursing care in pediatric oncology wards. 24 Ethical issues always are considered as integrated with religious beliefs in Iran. As an assumption, all nurses should follow ethical rules recommended by Islam in their practice. The subjects of nursing ethics and ethical codes are mentioned as a mix of religious rules in ethics in the general program of bachelor nursing. These have been resulted in a lack of general knowledge about the professional ethics in nursing in Iran. It has been only quiet a short time since attention has been paid to the education and execution of professional ethical topics in nursing schools and practice settings. Some specified congresses and in-service courses have been planned for nurses, which may not sufficiently increase the professional ethical knowledge of nurses or improve their practice. In addition to the above and according to studies, fatigue and lack of time, resulted from workload, lead to a negative attitude and emotional stress on nursing staff and thus, emotional and physical isolation and negligence of the emotional rights and needs of patients. 13,22,25 To put it more clearly, when the workload is high and the nurses are pressed for time, the nurses do the duties that they can be held accountable for.
In this study, “Patient education” and “Respecting autonomy and decision making” had the least optimal level in the perspective of the nurses as well as the mothers, which supports the results of other studies in the domain of parental consent to provide information and parent education of children with cancer and giving the right to make decisions. 26,27 It seems that most nurses believe that authorizing families of children with cancer in matters related to health and nursing interventions may result in irrational decisions of these families. 28,29 However, one of the ethical duties of the care team is to increase the efficiency and to facilitate patients and their families to participate in caring plans. Providing the family of the children with the right to make decisions inspires them, give them a feeling of being part of the medical team. This feeling is the essence of family-centered care. 30 One study done in Sweden shows that most of the ethical issues in the care of children with cancer are related to decision-making about treatments and beginning palliative care, challenges according to different perspectives between medical staff and families of children with cancer. 25 In similar studies, also lack of time, inadequate personnel and lack of preparation, and experience of nurses to provide relevant information about the disease and giving the right of autonomy and decision-making to the families are the major factors in the shortcoming of nurses in this domain. 31,32
The findings of this study showed that the performance of nurses in the area of “Respect for child and his family” is at an average level in the perspective of mothers, and at an optimal level in the perspective of nurses. The nature of working in a pediatric ward brings a sense of being compassionate and relatively caring for patients. However, indicators of respect for the patient are attention to the mental aspect, emotional states, and sympathizing with the patient and his family 23 mentioned in the items of the questionnaire. In this study, the item “the nurses listen carefully to the opinions, feelings and sufferings of children and families” accounts for the lowest score and is consistent with the results of other studies. 20,22 In a survey conducted by the American Nurses Association, the nurses’ perspective was that there are barriers to ethical practice in their work environment interfering with the decent and compassionate care. 33 According to them, insufficient number of nursing staff, high workload, lack of time, and financial and institutional constraints were the major obstacles in observing the professional ethics. Other studies also suggest that nurses stress the need for effective management styles for nursing in Iran. 13,22,34,35
The results indicated that the highest difference in the mean scores in the two groups of mothers and nurses is related to “Conscientiousness.” The mothers stated that the performance is low in this regard, while the nurses themselves believe to have an optimal performance. There is a significant difference regarding each of these four items comparing the scores of nurses and mothers. Supporting children and families when performing invasive procedures, empowerment of families, prioritizing the needs of family care and addressing the problems of families and children formed the theme of the items in this area. These findings are consistent with similar studies, where parents of children with cancer say that the care needs of themselves and their child was not a priority for nurses and that nurses prioritized to fulfill the technical tasks and implementing the treatment commands for the children. 22,24,36,37 It seems that despite the emphasis on the concepts of family-centered care and atraumatic care in the children’s nursing care, the needs of various aspects of children and parents and the reduction of their physical suffering are still ignored for various reasons. Task-based nurses, patriarchal perspective prevailing in healthcare environments while ignoring the whole family and children when providing care are among the factors which are mentioned along with other management factors such as lack of time and education as the underlying cause of the shortcomings. 14,27,38 This difference also comes out in the score of nurses and mothers in the area of “Improving the quality of patient care.” In this context, there is a significant difference in facilitation of empowering parents in the care of their child. This was consistent with the findings of other studies in this area, where parents expressed the opinion that nurses make no attempts to make them independent in the care of the child. 27 There are several reasons explaining this difference of opinion between patient and nurse, so it has been recommended to conduct profound and extensive research to explain the causes of the differences in the perspective of patients and nurses about professional performance criteria.
The results showed that the expression “the nurse respects the children’s religious beliefs and his family” accounts for the highest score belonging to the area of respect for the patient. This finding is consistent with that of other studies on the adult population. 13,39 High levels of religiosity of the population and managers planning in hospitals, to provide religious services due to the governmental support, such as allocating prayer rooms for mothers, and having conditions of prayers in congregation, are among the reasons that make mothers and nurses expect a high level of such performance for nurses.
The results of this study are consistent with another study that showed parents of children in the educational hospitals in Tehran are satisfied with nurses’ commitment in confidentiality and consider it at an optimal level. 40 This value also had good scores in other studies on some different population by age and the type of disease in Iran; so, it should have a cultural reason. Confidentiality is one of the main concepts of the traditional medicine of Iran, very emphasized by Avicenna, so that it has a probability that nurses have a lot of cultural encounter with this ethical principle.
The relationship between demographic characteristics with the perspective of mothers pertaining to the adherence of nurses to the ethical codes shows that the mothers of children with a higher frequency of hospitalization and those with a longer elapse of time since the diagnosis reported a better score. It seems that the mothers gain more satisfaction from ethical practice of nurses during hospitalization by adjusting their expectations, and by recognizing the role and status of each healthcare team member in the clinical environment. 15 However, another study on the perspectives of mothers with the nursing care, age of mother, hospitalizations, and the time elapsed since the disease showed no significant relationship with their scoring. 20 Further research is needed in this regard.
In addition, the findings indicated that the majority of nurses (76.7%) were unfamiliar with the codes of professional ethics and have not taken any course in this case. This percentage is very high, considering that passing such courses shows a significant positive relationship with the perceived level of adherence to the ethical codes. The findings support the results of other studies that prove the improvement of the ethical performance of nurses by passing “in-service” courses and familiarity with the professional codes of ethics of nurses. 11,14,22,41
Although the study was conducted at five big hospitals in Tehran mothers, the sample size was small, which reduces the generalizability of the findings. Therefore, it is recommended to conduct further studies with larger sample sizes. It is also recommended to measure the actual performance of nurses in adherence to ethical codes in children’s oncology wards using other methods than self-reporting.
Conclusion
This study showed that adherence to ethical codes by nurses in pediatric oncology wards is significantly different between the perspectives of mothers and nurses, while the average of the scores for the questionnaire is lower in the point of view of the mothers compared to the nurses. The findings are denotative for the managers and nursing staff so that it is essential to have a strategic plan to improve adherence to ethical codes to reduce the difference between the two perspectives. In-service courses need to be provided in all type of settings to emphasize practical aspects of using ethical codes. It is needed to regularly evaluate the real performance of nurses in ethical issues to discover fields that need to be improved. In addition, it is necessary to make the patients familiar with the professional roles of nurses to avoid underestimation of ethical performance of nurses because of confusion about real roles of nurses with those that is regarded to the whole system of healthcare.
Footnotes
Acknowledgements
This article was extracted from the thesis written by first author derived from her MSc thesis in pediatric nursing approved by the Research Vice-chancellor of Shahid Beheshti University of Medical Sciences (95/4/26-66000899). The authors wish to acknowledge Catharina Huberta Schouten for critical editing of English grammar and syntax of the manuscript. The researchers are grateful to mothers of hospitalized children and nurses of the oncology department of studied hospitals.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.