
Abstract
Background:
Using lies, in dementia care, reveals a common practice far beyond the diagnosis and prognosis, extending to the entire care process.
Objectives:
In this article, we report results about the attitude and the behaviour of nurses towards the use of lies to patients with dementia.
Research design:
An epidemiological cross-sectional study was conducted between September 2016 and February 2017 in 12 elderly residential facilities and in the geriatric, psychiatric and neurological wards of six specialised hospitals of Italy’s Campania Region.
Participants:
In all, 106 nurses compiled an attitude questionnaire (A) where the main question was ‘Do you think it is ethically acceptable to use lies to patients with dementia?’, instead 106 nurses compiled a behaviour questionnaire (B), where the main question was ‘Have you ever used lies to patients with dementia?’
Ethical considerations:
Using lies in dementia care, although topic ethically still controversial, reveals a common practice far beyond the diagnosis and prognosis, extending to the entire care process.
Findings:
Only a small percentage of the interviewed nurses stated that they never used lies/that it is never acceptable to use lies (behaviour 10.4% and attitude 12.3%; p = 0.66). The situation in which nurses were more oriented to use lies was ‘to prevent or reduce aggressive behaviors’. Indeed, only the 6.7% in the attitude group and 3.8% in the behaviour group were against using lies. On the contrary, the case in which the nurses were less oriented to use lies was ‘to avoid wasting time giving explanations’, in this situation were against using lies the 51.0% of the behaviour group and the 44.6% of the attitude group.
Conclusion:
Our results, according to other studies, support the hypothesis of a low propensity of nurses to ethical reflection about use of lies. In our country, the implementation of guidelines about a correct use of lie in the relationship between health operators and patients would be desirable.
Introduction
Using lies, in the context of dementia care, reveals a common practice that finds application far beyond the diagnosis and prognosis, extending to the entire support process. This is because with dementia, especially as the disease progresses, the problems related to communication difficulties occur frequently, and truthful communication is unlikely to be established in a stable and continuous way. 1
Authors who favour the use of the lie consider it a useful instrument to attenuate the patient’s pain, to improve his well-being, to ensure he abides by the pharmacological therapies and to reduce his agitation as well as his aggressive and dangerous behaviours. Such authors justify lying because the patient progressively loses the ability to understand and perceive the logic of communication and is thus unable to distinguish between truth and lies. In addition, the authors underline that from the operator’s point of view, using lies simplifies the relationship. 2 –8
Authors against the use of the lie define it as an unethical and immoral communicative modality used to avoid difficult situations to manage the process of daily care. They also emphasise the indispensability of the truth due to respect for the autonomy of the patient and for the basic trust present in the relationship between the patient and his caregiver. 9 –11 This position belongs to British organisations such as the General Medical Council, 12 the Nursing and Midwifery Council 13 and the Alzheimer’s Society. 14
To properly understand the central theme of the debate, we must distinguish between a non-therapeutic lie and a therapeutic lie. The non-therapeutic lie is characterised by an intentional ambiguity. Its end is persuasion and control, and it is used for the benefit of the health operator and not for the benefit of the patient. In contrast, the therapeutic lie is used for the patient’s benefit. It is empathic, person-centred and reflects a desire to negotiate, although it is not always adapted to the patient’s cognitive level. 2,4,15 –18
In the literature, further distinctions of the concept of the lie can also be found: outright lies, subtle lies, 19 little white lies, 20 going along, 20 lies of omission, 20 tricks, 15 environmental manipulations, 21 simulated presence 15 and the use of dolls. 22
Over time, studies have increasingly shown the need to properly define the concept of therapeutic lies 4,23–24 and have contributed to the debate regarding their ethical and moral implications, which has led to guidelines 4,25 and recommendations 26 aimed at including this practice within an ethical framework that takes into account the patient’s vulnerability. 24 For example, recommend the use of lies as the latest in a series of alternative strategies ranging from ‘meeting someone’s needs’ to ‘simulating the need’, ‘distracting’ and the use of a ‘therapeutic lie’. 26 –28
In an effort to resolve the semantic ambiguity implicit in the term ‘therapeutic lie’, Caiazza and James 29 introduced the concept of dementia-orientated reality (DOR), a person-centred communication structured with clear intention based on the patient’s biography that also fits in his timeline. The concept was subsequently reviewed and adapted in Italian. 30
Italy is lagging behind with respect to this issue, and such cultural lag explains the fact that in clinical practice, the lie is used when healthcare providers are not adequately prepared to assess their implications in their relationship with the patient and family members. The single study conducted in Italy by Cimmino et al. 31 explored the views and attitudes of a sample of 74 physicians and psychologists regarding the use of lies in dementia patient care. This study showed that 68.9% of Italian practitioners use lying essentially to deal with risk situations for the safety and well-being of the patients. Then, a cross-cultural study explored such attitudes among a sample of Italian and British doctors. 32
In literature, there are few studies that explored attitudes of nurses about lying in dementia care. 4,17,33 Therefore, in this article, the attitudes and behaviours of nurses towards the use of lies with patients with dementia are evaluated.
Methods
Setting
An epidemiological cross-sectional study was conducted between September 2016 and February 2017 in 12 elderly residential facilities and in the geriatric, psychiatric and neurological wards of six specialised hospitals of Italy’s Campania Region.
Campania Region’s residential facilities (residenze sanitarie assistenziali (RSA)) accommodate dependent older people because of physical and/or mental disability. These people cannot be taken care of at home, but hospital care is not necessary.
Participants
The study’s participants were nurses working in the selected hospitals/residential facilities for the elderly.
To collect data from all or most of the nurses, two expert operators went to each facility two or three times during the shift change. Before questionnaire delivery, a brief meeting was held to explain the meaning of the study.
The questionnaire was filled in anonymously after informed consent had been obtained.
As a nurse could have a different position about lies depending on the degree of dementia, the II and III degrees of the Clinical Dementia Rating (CDR) scale were identified as the target population of patients.
Questionnaires
Two different types of questionnaires were delivered randomly to the nurses. Both questionnaires contained the same questions, but one was submitted that related to attitude (A) and the other related to behaviour (B). For the attitudinal questions, we referred to the attitudes towards lying to people with dementia (ALPD) questionnaire. 34 Then, the attitudinal questions were reformulated to behavioural mode. Before study initiation, the questionnaire was reviewed for content and comprehensiveness by 10 nurses and no changes have been made from the original version.
Therefore, the main question for (A) was ‘Do you think it is ethically acceptable to use lies with patients with dementia?’ For (B), the main question was ‘Have you ever used lies with patients with dementia?’ Then, six different situations in clinical practice were identified as a possible source of lies. These situations were preceded by the following premises: (A) ‘For which of these situations do you consider ethically acceptable to use lies to the patients suffering from dementia?’, which could be answered with a four-point Likert scale: disagree, partially disagree, partially agree and agree; (B) ‘For which of these situations did you happen to use lies to patients suffering from dementia?’, which could be answered with a four-point Likert scale: never, rarely, sometimes and often. Moreover, each question showed between brackets a practical example, with exception of the question no. 5. Listed below are the six different situations: ‘To simplify drug ingestion’ (Nurse: ‘Open your mouth and I’ll give you a candy’); ‘To permit the execution of an invasive procedure’ (surgery, endoscopy and blood tests) (Nurse: ‘Let’s go for a walk’); ‘Not to deny a false statement of the patient’ (the patient asks about his/her deceased mother; Nurse: ‘She will come later’); ‘To alleviate the stress of the patient’ (to a patient with serious illness; Nurse: ‘Don’t worry; tomorrow we will discharge you’); ‘To prevent or reduce aggressive behaviours’; ‘To avoid wasting time giving explanations’ (Patient: ‘Can I have a beer?’ Nurse: ‘Yes, later…’).
The next section contained more theoretical questions, with dichotomous answers, in order to get more comparability between A and B: for (A) ‘Should the use of lies be adapted to the cognitive abilities of the patient?’ (yes/no) and ‘Do you think it would be useful to introduce a discussion between health providers on the use of lies to define more precise rules regarding the behaviour to be implemented towards patients with dementia?’ (yes/no); for (B) ‘Has the use of lies been adapted to the cognitive abilities of the patient?’ (yes/no) and ‘Have you ever spoken with other health providers about a shared mode of the use of lies?’ (no; yes, with other nurses; yes, with the physicians; yes, with the relatives). Finally, there is one question that appears on both questionnaires: ‘Have you ever thought about the possible negative consequences of using lies?’ (yes/no).
The Ethics Committee of the University of Campania ‘Luigi Vanvitelli’ approved this study.
Data analysis
Descriptive analysis was performed on all the variables. Comparison of proportions was performed to compare, in attitude and behaviour, similar variables. A p value <0.05 was considered the level of statistical significance. Analyses were carried out using SPSS Version 11.0 statistic software package.
Results
Of 235 nurses who submitted the questionnaire, 23 refused consent, meaning that the overall response rate was 90%. In total, 212 nurses answered the questionnaire: 106 answered the ‘attitude’ form and 106 answered the ‘behaviour’ form. Of the 212 nurses, 53.4% were women, 72.8% were more than 41 years old and 58.1% had been working for over 10 years. Only 10.8% of the nurses studied were head nurses of the ward (Table 1).
Sociodemographic characteristics of the study population.

The two groups were comparable for these socio-demographic characteristics. The main question of the two questionnaires was aimed at evaluating whether and how often the nurses used lies (behaviour) and whether they think it is acceptable to use lies (attitude). Table 2 shows that in both cases, only a small percentage of the interviewed nurses stated that they had never used lies/that it is never acceptable to use lies (behaviour 12.3% and attitude 10.4%; p = 0.66).
Nurses’ attitude (A) and behaviour (B) about using lies with patients with dementia.

*Comparison of two proportions – results: χ2 = 0.189; 95% CI = –7.4+11.2; p = 0.66.
Starting from the ‘disagree’ and ‘never’ columns of Table 3, the situation in which the nurses were more oriented to use lies was to prevent or reduce aggressive behaviours. Indeed, only 6.7% (A) and 3.8% (B) were against using lies. However, the case in which the nurses were less oriented to use lies was to avoid wasting time giving explanations. In this situation, 51.0% (A) and 44.6% (B) of the respondents were against using lies.
Nurses’ attitudes (A) and behaviour (B) about using lies during patient care.
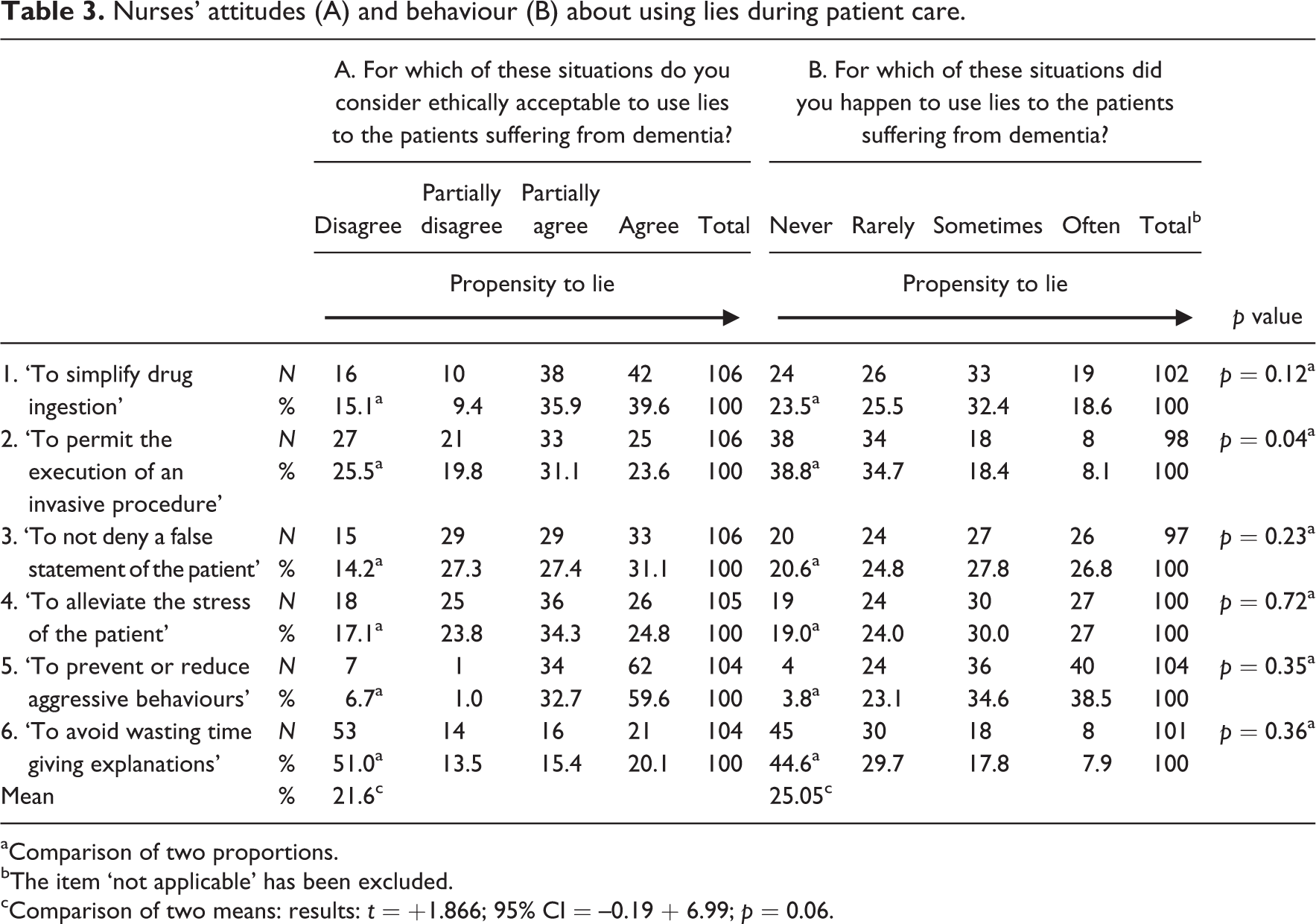

aComparison of two proportions.
bThe item ‘not applicable’ has been excluded.
cComparison of two means: results: t = +1.866; 95% CI = –0.19 + 6.99; p = 0.06.
The majority of nurses believed ‘the use of lies should be adapted (77.1%)/has been adapted (71.8%) to the cognitive abilities of the patient’. The majority of nurses also reported that ‘They thought it was useful to discuss (79.6%)/have discussed (77.1%) about a shared mode of the use of lies’. Finally, 86.7% (A) and 77.9% (B) said ‘They had thought about the potential negative consequences of telling a lie’. In all answers, we observed a consistency between attitudes and behaviours (p > 0.05; Table 4).
Nurses’ opinions about adapting lies to patients’ cognitive abilities, about discussion, about use of lie and about potential negative consequences of lying.

*Comparison of two proportions
Discussion and conclusion
The debate on the use of lying as a communication strategy is still open and highlights the need to further clarify risks and benefits of lying in the contexts of care, in the best interest of the patients with dementia and in order to allow operators to respect ethical principles. Indeed nurses, daily involved in practical patient care, appear more exposed to the ethical and moral implications of using lies.
In our study, the first conducted in Italy on nurses, only 12.3% said that they had never used lies and only 10.4% said that using lies is never acceptable. Therefore, our results are in line with the literature, especially when referring to samples formed of nurses. 4 We found a slightly higher rejection of lies in physicians. 25,31 This discrepancy could be explained by the fact that healthcare providers who most readily supported the use of lies were those professionals providing the most intensive face-to-face care.
Faced with a very high percentage of nurses who lie (87.7%), only 9.4% said they do it often. This finding leads to the assumption that in our sample, using lies is considered a strategy to use in moderation.
As for the typical situations of daily clinical practice, also in our study, the lie appears to be used mainly in the interest of the patient: to relieve stress; not to contradict a false statement and to convince the patient to adhere to drug therapies. All behaviours mentioned are in line with the idea of the therapeutic lie justified on the grounds that one is dealing with a patient who is gradually losing the ability to decide on his own care and adequately assess the risks to his safety. 3–4,6,7,17.25,34 Confirming this is the high percentage of respondents opposed to the use of lies in the case of to avoid giving explanations that waste time, which is a situation where the interest is greater in the provider than in the patient (non-therapeutic lie). Therefore, in accordance with other studies, 4,17,33 in our sample, the lie more ethically accepted and the most used seems to be the one that corresponds to the interest of the patient and not the care provider. Moreover, we would like to comment the question ‘to prevent the patient’s aggressive behavior’. We have supposed this situation in the interest both of the patient and of the nurses and we have considered in the border between therapeutic and non-therapeutic lie. Thus, lying in these situations is a common interest of patient and nurse. Therefore, it is not a coincidence that nurses, in this specific situation, have expressed the greatest agreement on lying (93.3%). The subjects of our sample stated that they believe a lie must be tailored to the cognitive level of the patient and declared that in most cases, they apply this principle in clinical practice. Additionally, not only have they discussed this principle with colleagues, but they think it is useful to do so. Finally, they claimed that they reflect about the potential negative consequences of lying in their daily practice.
Our study is the first that has been conducted for the purposes of comparing and evaluating, through two separate questionnaires, attitudes and behaviour towards the use of lies. There were two initial hypotheses. With the first, we were expecting a higher number of people who use lies and a lower number of subjects who believe they are ethically acceptable. This was based on the fact that it is unacceptable to use lies, but some do it anyway for convenience, to simplify procedures. With the second, we hypothesised that there would be a substantial consistency in the responses to the attitudinal and behavioural questions and consequently, as opposed to the first hypothesis, a lower attitudinal propensity towards ethical reflection on the part of healthcare providers. Our study’s findings support the second hypothesis, as indicated by the high percentage of individuals who failed to express a clear position about the ethical acceptability of lies (based on the prevalence of the answer ‘it depends’).
In Britain, to meet the demand of trained healthcare providers in the use of deceptive practices, guidelines for lies were developed in 2016. 4,28 They were further refined in 2013 25 and changed significantly by the Newcastle group, taking into account features associated with memory and relationship-centred care practices. 35
In our country, it would be desirable to implement guidelines aimed at ensuring the use of lies within an established ethical framework that respects the four common bioethical principles: autonomy, beneficence, non-maleficence and justice. 14 On the basis of this study, it is necessary to reinforce how important it is for healthcare providers to receive adequate training in the use of lies because it increases the awareness of this practice and its ethical implications.
Limitations
Considering the difficulties associated with finding an adequate number of nurses and the fact that we did not do a correct sampling of them, we believe that the modalities of the samples did not bias the results of the study. The comparison between attitudes and behaviours must be interpreted with caution for two reasons: respondents of the two questionnaires belong to different populations and the two four-point Likert scales were not entirely overlapping. Therefore, we preferred to compare only the items to which the respondents answered ‘no’ on both questionnaires. The topics of this study were particularly exposed to an information bias because the respondents could have hidden their use of lies to please the interviewer and because the use of lie is considered a socially reprehensive act, even though the study was anonymous. We assumed that this effect was particularly strong in the last two questions presented in Table 4, when most of the nurses stated they had engaged in discussions with other healthcare providers about a shared mode of the use of lies and that they reflected on the possible negative consequences of a lie.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.