
Abstract
Background:
Managing HIV treatment is a complex multi-dimensional task because of a combination of factors such as stigma and discrimination of some populations who frequently get infected with HIV. In addition, patient-provider encounters have become increasingly multicultural, making effective communication and provision of ethically sound care a challenge.
Purpose:
This article explores ethical issues that health service providers in the United States and Botswana encountered in their interaction with patients in HIV care.
Research design:
A descriptive qualitative design was used to collect data from health service providers and patients using focused group discussions. This article is based on responses from health service providers only.
Participants and context:
This article is based on 11 focused group discussions with a total sample of 71 service providers in seven US sites and one Botswana site.
Ethical considerations:
Ethical review boards at all the study sites reviewed the study protocol and approved it. Ethical review boards of the study’s coordinating centers, Rutgers University and the University of California at San Francisco, also approved it. The study participants provided a written informed consent to participate.
Findings:
HIV service providers encountered ethical challenges in all the four Beauchamp and Childress’ biomedical ethics of respect for patients’ autonomy, beneficence, justice, and nonmaleficence.
Discussion:
The finding that HIV service providers encounter ethical challenges in their interaction with patients is supported by prior studies. The ethical challenges are particularly prominent in multicultural care and resource-constrained care environments.
Conclusion:
Provision of HIV care is fraught with ethical challenges that tend to pose different issues depending on a given care environment. It is important that strong partnerships are developed among key stakeholders in HIV care. In addition, health service providers need to be provided with resources so they can provide quality and ethically sound care.
Keywords
Introduction
The advent of antiretroviral therapy has had a dramatic positive impact on HIV-related morbidity and mortality worldwide, improving the quality of life for people living with HIV and increasing their life expectancy. 1 –3 The positive impact of antiretroviral therapy is a function of the efficacy of treatment that depends on a number of factors including early diagnosis, early initiation of treatment, retention in care and adherence to recommended treatment, and a lifestyle that supports treatment adherence. 3 In an increasingly multicultural communities of our present times, managing HIV treatment and ensuring that it is efficacious bring about a patient-provider encounter characterized by diverse cultural, ethnic, racial, and religious backgrounds that frequently compromise effective communication and good patient-provider relationships, bringing to surface questions about whether or not healthcare providers practice in an ethically responsible manner. 4
In addition to the diversity in the background of both patients and HIV service providers, management of HIV itself is a complex multi-dimensional and highly dynamic task because of a combination of factors such as stigma and discrimination of some populations who frequently get infected with HIV, the need to protect confidentiality of those infected while at the same time protecting those who are at risk of being infected, criminalization of failure to disclose a positive HIV between sexual partners in some countries, criminalization of gay and lesbian populations in some countries, and questions about whether preventing HIV infection through antiretroviral therapy is right or wrong. 5 Particularly in low-resourced environments, questions about how best to maximize the use of limited resources as in targeting urban versus rural areas, children versus adults, prevention versus treatment, and antiretroviral medications versus expensive chemo and radiotherapies often arise. 6,7 Consideration of mandatory HIV testing has brought about questions about HIV service providers’ obligations to the individuals under their care versus obligations to the public 5 as well as the value of patients testing and knowing their HIV-positive status when they cannot be assured of a cure. 8 Another issue that makes HIV care challenging is the transmissibility of the HIV virus between patients and healthcare providers. Because of the concerns about protection of both patients and service providers, patients may demand to know the HIV status of their care providers and refuse to be cared for by such providers. In a similar vein, healthcare providers may choose not to take care of HIV-positive patients for fear of getting infected with the virus. 8
Over and above the challenges just highlighted, like any healthcare, HIV care takes place within socio-political, cultural, and economic conditions that may interplay among themselves and with ethical issues to create a unique tone in patient and HIV service provider experiences and interactions. 5 Such conditions may be poverty, displacement of populations, and political climate including allocation of resources for HIV care. For instance, in the Democratic Republic of Congo, lack of food was a barrier to HIV treatment adherence. 9
The term ethics is a branch of the philosophy of science that pivots on issues of rightness or wrongness of acts. 10 Beauchamp and Childress 11 proposed a framework for addressing bioethical issues. The framework is made up of four ethical principles, namely, respect for the decision-making autonomy of clients, beneficence, justice and nonmaleficence. Respect for persons obligates HIV service providers to acknowledge patients’ autonomy, honor their preferences including the right to refuse treatment and respect to the individuals’ right to truthful information. 10 It has been argued that respecting the patients’ autonomy may be more complex than we may believe as it also implies respecting their cultural values and religious identities as well as their choice to give the family more power than the patient in determining the best treatment. 12
Beneficence holds treatment providers responsible for doing good for patients and protecting them against harm and the risk of death. 13 It has been argued that the hallmark of healthcare providers’ duty of beneficence is doing the best they could to enable patients to get the best benefit from treatment or care interventions. 5 Kaposy et al. 5 further noted that beneficence requires that the healthcare providers build trusting relationships with patients and that they are adept at problem solving. Justice requires that treatment be accessible and fairly provided to all who need it without discrimination and that the scarce healthcare resources are equitably distributed. 14 Nonmaleficence cautions treatment providers not to do anything, in action, word, or omission that may subject the patient to harm. Beauchamp and Childress framework will guide the discussion of ethical issues in this article. Although the four principles are frequently discussed as if they are mutually exclusive, they are actually intertwined as for instance, delaying care because of stigma and discrimination to the extent that health problems complicate and become difficult to manage violates the principles of justice, beneficence, and non-maleficence. 14
Ethical issues as used in this article concern patient-provider encounters that put providers in a situation whereby they felt their practice integrity was being or risked being threatened. The threat came about because one or more of the four ethical principles risked or was(were) being violated. If the situation presented the provider with two alternative courses of action with neither of those providing a satisfactory solution, or when trying to fulfill one principle, the others were violated, then the situation was taken to be a dilemma. 13
The salience of ethics in HIV care stems from stigmatization and discrimination of those infected, impingement of care into the person’s private life, and the incurability and communicability of HIV infection. The ethical concerns center on containing the infection in a manner that protects the patient’s right to privacy and autonomy in decision making. Ethical issues cut across dimensions of HIV care such as treatment adherence, human and material resources for care, HIV status disclosure, and communities’ HIV and treatment literacy. Whereas a significant attention has been paid to guidelines for ethical care and the impact of unethical care on patients, 15 only little attention has been given to the challenges that HIV service providers, and nurses in particular, meet in their effort to providing ethically responsible care to persons living with HIV in the United States and Botswana. However, as has been noted, HIV care provision may pose serious ethical challenges for nurses. This study that sought the perspective of both people living with HIV and their service providers about the health literacy of people living with HIV provided a platform for a broad understanding of what goes on in providing antiretroviral treatment including the ethical challenges that service providers encounter.
The focus of the article is limited to exploration of ethical issues that service providers encountered in their interaction with patients receiving HIV services in Botswana and the United States. No known study has considered the ethical issues in HIV care in the United States and Botswana. However, healthcare and nursing in particular have become global, necessitating that practitioners and researchers get familiarized with the life worlds of other cultures and how those compare with what they take as valid knowledge. This is important because practitioners research and practice across the globe and therefore need to be familiarized with care issues across countries. It is hoped that the article will stimulate discussions and research on the areas highlighted as well as facilitate sharing of strategies for addressing similar encounters.
Methods
The data on which this article is based came from a larger data set from a multi-site study exploring health literacy among people living with HIV, prescribers of antiretroviral treatment who could be physicians or nurses, and other non-treatment prescribers taking part in treatment such as pharmacists, counselors, and nurses. 16 Qualitative descriptive design was employed for the study. A qualitative descriptive design studies a phenomenon in its natural state within the context of the research environment. As the design does not commit to any theoretical view of the phenomenon, qualitative descriptive design allowed the researchers to describe health literacy for people living with HIV to the extent that was possible within the parameters of the study. 17
Ethical clearance was obtained from ethical review boards of the relevant authorities at all the eight study sites. As coordinating centers for the study, Rutgers University and the University of California at San Francisco also provided approval for the study. All those who participated in the study provided a written informed consent following a detailed explanation of the study.
A total of 120 people living with HIV and 71 health HIV service providers were purposefully selected to participate in the study. Sampling of the study participants followed a convenience sampling of the study sites providing health services for people living with HIV including antiretroviral therapy. The study had eight sites, seven in the US cities and one in a Botswana city. Clients receiving HIV services from the US sites were multicultural groups made up of locals and immigrant populations while those receiving services from the Botswana site were of a relatively homogeneous cultural background that was, however, quite different from that of those at the US sites. In addition, policy guiding HIV services in Botswana and the United States were quite different with the services in Botswana provided to all citizens free of charge while in the United States, some clients were covered by health insurance while some were paying out of pocket.
Multi-country-multi-site sampling enabled investigation of disparities of health literacy, as well as consistencies and differences of the dimensions of health literacy. The multi-country-multi-site sampling of health service providers was expected to provide insight into the similarities and differences in the ethical challenges that HIV service providers encounter when providing care to clients from diverse cultures. Understanding of such consistencies and differences could assist in advocating for resources to support HIV service providers in different settings and geographical regions and lead to quality and ethically sound care as well as provide opportunities for cross-country exchange of information on practices that work.
A focus group discussion guide aided data collection. Questions that generated data on ethical issues covered service providers’ sharing of HIV and treatment-related information, challenges encountered in communicating such information, and how service providers determined that patients comprehended information shared with them. Examples of questions were “what strategies do you use to educate your patients on HIV” and “what is the impact of your patients’ beliefs and attitudes on educating and counseling them?” In total, 17 and 11 focus group discussions were held with people living with HIV and HIV service providers, respectively. Focus groups were audio-taped and later transcribed verbatim. At the sites where English was not the primary language, transcripts were later translated into English. ATLAS, ti software aided content analysis.
Rigor of the study
Colorafi and Evans 17 outlined measures to ensure rigor in qualitative research and some of those were carried out in this study. An interview guide was used to ensure consistent approach to data collection by different but similarly trained investigators across settings. The study was piloted on samples of participants from the study populations in order to ensure alignment of the design to the research questions. Multiple researchers coded the data and agreed on the codes. Characteristics of the sample have been described in detail so as to allow comparison with other groups. Potential threats to generalizability of the study findings have also been discussed.
This article is based on the responses of service providers only. Service providers were in two categories: those who prescribed antiretroviral treatment were labeled “healthcare providers” in the study, abbreviated HCP. Non-treatment prescribers providing other aspects of direct care were labeled “professional care team members,” abbreviated PCTM. For purposes of this article, HCP and PCTM are collectively referred to as “HIV service providers.” However, verbatim excerpts spell out HCP and PCTM. Responses of HIV service providers considered to be ethical challenges were extracted from the transcribed interviews and grouped into categories according to common threads linking them. Each category was further examined to identify its sub-categories. Identified categories and their sub-categories were examined and compared across the eight sites in the two participating countries.
Findings of the analysis focusing on ethical issues encountered by HIV service providers
Characteristics of the HIV service providers
In all, there were 71 HIV service providers who participated in the study. In total, 59 (83.1%) participants were from the United States while 12 (16.9%) were from Botswana. US participants came from diverse regions of the country and had diverse cultural backgrounds. Eight of the 12 service providers who made up the Botswana sample were physicians who were non-Botswana nationals mainly from other African countries. Service providers were from diverse disciplines, with the majority of them being nurses; they had wide levels of education and age range. Table 1 provides a demographic profile of HIV service providers.
Characteristics of HIV service providers (N = 71).
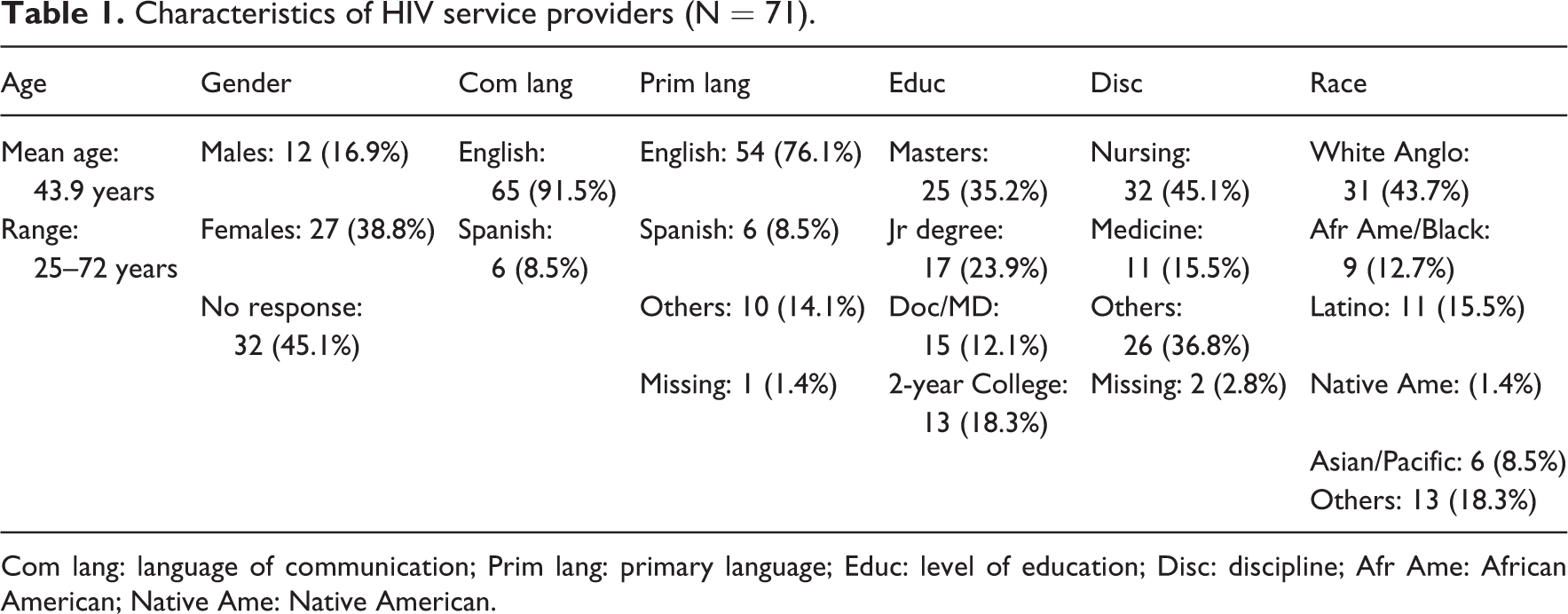
Com lang: language of communication; Prim lang: primary language; Educ: level of education; Disc: discipline; Afr Ame: African American; Native Ame: Native American.
Description of ethical issues encountered
All the four principles of Beauchamp and Childress’ framework for bioethical ethics emerged as concerns for HIV service providers participating in the study. Although ethical issues were reported at all the study sites, contextual variations made some more salient than others. The issues are presented under the principles of respect for patients’ autonomy, beneficence, justice, and nonmaleficence.
Respect for patients’ autonomy
The issue surrounding respect for patients’ autonomy came about when patients and service providers had different expectations about the level of patients’ participation in care. In their effort to respect the patients’ right to self-determination with regard to their preferences about their care and treatment, service providers were often frustrated by the response that they got from patients. Whereas HIV service providers expected patients’ full participation in their treatment plan, some patients looked up to providers to take full responsibility for the treatment. Such patients took a passive stand, only waiting to hear from providers if there was need to change anything. Patients believed that a competent provider should be able to work independently of the patient and should therefore take total control of the treatment plan. On the other hand, service providers felt uncomfortable assuming a paternalistic position because that did not only violate the principle of respect for patients’ autonomy but it also compromised the quality of care as patients’ full participation would have increased the chances of their needs being appropriately addressed. The following excerpt from one interview illustrates how HIV service provider’s effort to respect the patient’s autonomy in decision making conflicted with what the patients expected in the patient-provider interaction: …he was really furious that people were asking for his input. His perspective was: “why would I come all the way here to give you my input? I came here to see experts and I want experts to take care of me…” (HCPs)
Beneficence
Issues surrounding the principle of beneficence were related to the patients’ belief that miracles, home remedies, and religious practices such as prayer could cure HIV. Service providers expected that patients seeking HIV services from the healthcare system had faith in the services provided. However, some of them encountered clients who came forward to seek care and yet strongly believed that their illness could be explained and healed better by their cultural healthcare systems such as home remedies and religious practices. Other patients adamantly denied that they were infected with HIV and believed that home remedies would heal their illnesses. A few had stopped antiretroviral medications in response to advice from their religious leaders.
HIV service providers were therefore frustrated because whereas patients were coming over to treatment centers to seek help, they were not effectively benefiting from the services offered. They were wondering if it was worthwhile to continue providing the services when their efforts were futile. The following sentiment came up in a group discussion: “I have had many African Americans that tell me they do not take the medicine because they’re miraculously healed by God; and I have seen a lot of them die from the disease because of that” (PCTM). At another interview session, one respondent said, “I have a couple of patients who adamantly don’t believe they have HIV…and so I don’t answer to that; I don’t know how to fix that or change that or talk to it” (HCP). As they have obligation to act in the best interest of the patient, HIV service providers were frustrated by their failure to provide the best care that they believed could benefit their patients.
Another situation that challenged HIV service providers’ obligation to act in the best interest of the patient was when politicians interfered with professional autonomy. Although it was reported at only one of the eight study sites, political interference in professionals’ decision making was disturbing as it left providers feeling powerless. A scenario that was provided was a case of a patient who had missed treatment for a considerable number of days. According to the treatment protocol, the patient had to re-start the treatment regimen. However, the patient was not in agreement with his doctor as rather than starting treatment afresh, he or she wanted to pick from where he had stopped and continue with the treatment. Upon failing to convince his or her service provider to let him or her continue with the treatment, the patient approached a top politician who then called the provider and instructed that the patient be given treatment that he or she was demanding. This put the provider in a difficult position because his or her decision was based on evidence-driven protocol that was used for all patients. Whereas the service providers admired the positive political response to the HIV crisis in the country, they felt that some politicians were encroaching on professional autonomy. The following is what one participant said: If one runs out of treatment for 4 days the policy of the government…he should be taught afresh so that you re-start. The person will be saying, “I am sick, so I cannot start afresh”; then he calls the minister, the minister will phone somebody who will phone the chief medical officer…and the chief medical officer will be on your head saying, “give the pills to that one!” So we have the policy and all the political connections. So you ask yourself: “should I follow the policy or the politics that come from up there?” (HCP)
Justice
Questions surrounding the principle of justice came about because of some service providers’ discomfort in treating members of the gay and lesbian population. At one setting, service providers felt treating gay and lesbian population was a moral challenge because their value systems did not accommodate the population’s sexual orientation. Their personal selves were in disagreement with their professional obligation of unbiased treatment of all patients. Even though they did not report any discriminatory treatment of gay and lesbian populations, one believes that they might have been aware that their body language could communicate a message that was contrary to how they were trying to present themselves to patients. For instance, one provider reported that she or he had difficulty finding acceptable words to use in communicating with patients who were gay or lesbian.
Tension resulted as service providers yearned to be integrated providers who would be able to provide care that does not discriminate against patients based on sexual orientation. Another source of tension was that gay and lesbian population feared being discovered in anticipation of being rejected, as they were aware of the stigma related to gay and lesbian people. HIV service providers therefore experienced frustration related to honoring the principle of justice or fair treatment to all patients.
Nonmaleficence
Concerns related to the principle of nonmaleficence were mainly to do with shortage of resources. For instance, one concern was related to the use of interpreters when available service providers could not communicate with patients in the local language. Whereas the use of interpreters was a valued solution in situations where the service provider and client had no common language, the approach had its own dilemmas and frustrations. In some instances, both the service provider and the patient had doubts about the validity of the interpreted communication. One service provider described the use of an interpreter as having “a relationship by proxy” with the client as there was no direct communication between the client and provider. The issue that comes out of this was that, in cases where a professional interpreter was not available, the service provider could not confidently assure the patients that his or her information would be kept confidential as there was the third person who was privileged with the information. This was even more problematic because sometimes there was doubt if information was actually reaching across to the other side. “…you don’t know if the interpreter is saying the right thing. You may say something in a minute and the interpreter takes five minutes and you wonder what the interpreter is saying” (HCP).
Another issue related to the use of interpreters was breach of confidentiality. In some settings, the workplace guidelines did not allow staff and patients’ family members to interpret. However, because service providers did not have the type of personnel that the guidelines recommended, they had to use what they had at hand, therefore violating the guidelines. One service provider stated, “We make do with what we have” relating to using patients’ family members to interpret and by so doing exposing any patient’s confidential information to the interpreting family member. The scenario represents a violation of the principle of nonmaleficence or a risk of harm to the patient as quality of care was potentially compromised and as confidentiality of the patient’s information could not be guaranteed.
At the Botswana site where no guidelines regarding who could or could not interpret existed, no dilemma was reported as staff such as nurses and auxiliary personnel could interpret; as long as one could speak both English and the local language. The only concern was doubt that some interpreters might fail to convey accurate message between the patient (non-English speaking) and the doctor (non-Setswana speaking). However, at the US sites, ethical issue surrounding language interpretation concerned invasion of patients’ privacy if interpreting was done by non-licensed persons who feared that they could be sued for doing what they were not licensed to do.
Resources constraints often involved unavailability of service providers who were competent enough to meet the needs of patients. At one study site, the standard practice had been to discourage pregnant women who tested HIV positive from breastfeeding because of the risk of passing the virus to the unborn baby. However, a new development had been to encourage women who had tested HIV positive to breastfeed. When women demanded clarification on the inconsistent message coming from the same service providers, the latter’s response was that they did not know why the policy had changed and that they were simply passing on the information that they had been given by their superiors. One would therefore argue that service providers were not adequately empowered through training to enable them to meet the demands of HIV care. The principle of beneficence obligates service providers to do good through meeting the healthcare needs of patients; including the need for accurate information that could empower them to make the right decisions. Although service providers may have done well to tell patients the truth about their knowledge deficit regarding the latest policy, one may wonder if that was in the best interest of patients. One option could have been to ask patients to give them some time to find the right information.
The responses of participants reveal that resources constraints, including lack of knowledge, make the work of HIV service providers ethically challenging. This is because as they strive to do what they deem could best benefit patients, they were constrained by the lack of requisite tools.
Discussion
Findings of the study revealed that HIV service providers encountered challenges in all the four ethical principles articulated by Beauchamp and Childress. 11 Prior studies have also pointed out the difficulty that HIV service providers face in their effort to respect patients’ autonomy. In their study conducted among nurses in the Netherlands, participants reported a dilemma related to choosing between respecting patients’ autonomy and providing service that they believed would lead to optimal medical outcomes. 18
Other studies have revealed that religious beliefs have a potential to be both barriers 6 and facilitators 19 –21 in HIV treatment adherence. In a Tanzanian study, patients reported that they had stopped taking HIV treatment after being prayed for and being promised that prayer would heal them, 22 while in a South African study, patients reported to have stopped taking antiretroviral treatment because they were taking traditional medicine. 23 The findings provide evidence that religious beliefs and traditional medicine can present a challenge to western HIV treatment. Similarly, issues surrounding religious beliefs and their relation to treatment adherence in this study challenged HIV service providers’ respect for persons and their preferences as they did not trust that patients’ preferences would lead to positive health outcomes. It can be argued that religious beliefs must be respected because they inform the way patients live their lives including managing their illness and adhering to treatment.
With regard to the incongruence between religious beliefs and western healthcare HIV treatment, there were no differences between Botswana site and the US sites; and although religious beliefs have been reported to act as either barrier to or facilitator of HIV treatment adherence, in this study, religious beliefs only served as a barrier to treatment adherence as patients interrupted western HIV treatment with the belief that prayer would heal them. Political interference in professional autonomy was only reported at the Botswana site. Probably because of the country’s small population size (just over 2 million), there was a high likelihood for patients and political authorities to be socially connected and to reach one another with ease.
The concern about service providers violating the ethical principle of justice in HIV care is not unique to this study. The findings are congruent with those of prior research on HIV-positive gay and lesbian population. The United States National Women’s Law Center 24 reported that gay and lesbian population were often denied HIV care and discriminated and that they often avoided seeking care for fear of being discriminated. Often the denial of care was influenced by healthcare providers’ religious beliefs. 24 In Uganda, a study revealed that many HIV-positive transgender people avoided seeking help from hospitals because they were prejudiced, made fun of, and denied treatment by health providers. 25 This study revealed that recognition and acceptance of gay and lesbian population was at different stages of development across countries. For that reason, it was often a moral challenge for HIV service providers to treat gay and lesbian populations as they felt uncomfortable interacting with them. In the same vein, gay and lesbian populations feared being discovered in anticipation of being rejected. HIV service providers were therefore violating the principle of justice that demands that all people be treated equally such that everybody gets his or her share of the benefits and risks. Because of a challenge in communication with patients with whom they did not have a common language, healthcare providers were concerned about the quality of care they were providing. They felt mistrusted by patients and, as a result, avoided asking some questions that could be culturally labeled to invade patients’ privacy. 26 Some host country laws that made administrative and payment processes burdensome presented a dilemma to healthcare providers who found themselves having to deny care to some immigrants. 26
Resources constraint in this case was lack of healthcare providers who could provide culturally competent care to immigrants as the principle of beneficence dictates. It was however evident that whether or not ethical issues related to language interpretation arose depended on the context. For instance, in the United States, where interpreting was formalized and to some extent regulated, 27 there were concerns about potential lawsuits whereas at the Botswana site there were no concerns about possible litigation.
Whereas at one setting for this study, family members including children served as interpreters, in a study conducted among refugees in Sweden, it was inappropriate for family members, particularly children, to interpret. 28 It is likely that in a sophisticated highly litigating society, questions about who is best to interpret could be an issue while in a less sophisticated and less litigating society in which collective existence is valued over individuality, people will feel obliged to assist others by offering their voluntary interpreting service. The findings challenge healthcare providers to keep on adjusting their approach to providing services to different cultural groups.
In a study conducted in South Africa, doctors who could not directly communicate with patients reported finding it dilemmatic to practice medicine in a way that was contradictory to what they valued as they could not take history from the patient and family because of language barrier. 29 Health service providers found themselves giving preference to patients who would not present language barriers and only attending to others later on. It was reported that the quality of interpretation was poor as often the informal interpreters would only communicate to patients what they believed would make sense to them. The study participants expressed the need for professional interpreting services and provision of language training to foreign doctors. 29 Similarly, in this study, HIV service providers reported that often they doubted what the interpreter was telling the patient. However, Penn and Watermeyer 20 argued that it is unrealistic to expect that interpreters would convey the message in exactly the same way the speaker says as they also bring to the encounter their own values, beliefs and prejudices and even cultural backgrounds which may even add quality to patient-provider encounter. It can therefore be argued that language interpretation is a complex issue that may present an ethical dilemma to the healthcare providers as it raises questions about whether or not one is acting in the best interest of the patient. Concerns about confidentiality in the use of interpreters raised in this study have also been expressed in prior studies. 29,30
An issue about patients who do not want to play an active role in decision making about their own care because they trust that healthcare providers are best placed to address their problems has also been reported in a Netherlands study whereby some patients wanted to be passive and to leave all care activities to nurses. The situation put nurses in a difficult position because whereas they wanted to respect patients’ preferences, they did not believe such preferences were best for the patients’ optimum health outcomes. 18 Because of the increased attention to consumer voice, political interference in professional autonomy has increasingly become a concern. 31 Political interference has also been reported as a source of frustration for health workers in Pakistan where ruling politicians were found to favor some service providers over others. 32
The discomfort in providing HIV care to members of the lesbian and gay population reported in this study has been argued to harm patients as it may bring about serious emotional, physical, and financial consequences for them including unnecessary invasion of privacy and delayed institution of treatment. 24 In a study conducted in Uganda, it was reported that transgender persons avoided seeking HIV services in the public sector for fear of being denied treatment, ridiculed, discriminated, and abused. 25
Implications for research
The finding that religious beliefs often disrupted HIV treatment adherence suggests that more research is needed particularly in service environments represented in the study in order to increase the understanding of the role of religion as a resource or hindrance in antiretroviral therapy. Research on communities’ views on how best to approach ethically sensitive HIV care could provide a guide to developing effective community-professional partnership strategies.
Implications for practice
HIV service providers need to respect patients together with their religious beliefs. However, it is evident that respecting such beliefs is often a complex process as they may be incongruent with the treatment protocol. Representatives of western healthcare and communities’ religious groups need to work closer together to establish a common ground. Such partnerships could enhance mutual understanding and consensus on how to manage the interface between religious beliefs and western healthcare. Previously published work from the same study has revealed that a trusting relationship between patients and HIV service providers is important in the health outcomes for people living with HIV. 16 Treatment adherence counseling needs to explore patients’ beliefs and practices that have the potential to compromise treatment adherence.
HIV service providers need to be assisted to clarify their values so that they can be more able to work with patients with belief systems or sexual orientations different from their own, 33,34 because doing otherwise may compromise justice. They also need effective communication skills training so they can be able to consider the words that they use, the timing of the message, and the context of the issue at hand when interacting with patients.
Healthcare providers have been cautioned to be aware that their ignorance about realities other than the western theories and evidence may cause them to do harm to people of minority cultures. 35 This observation may also apply to service providers’ encounter with religious beliefs in this study that were unsupported by western evidence. As Ong-Flaherty et al. 35 suggested, healthcare providers need to be a little skeptical about the reality that they know and be open to learning about alternative realities. 35
Implications for policy
Health policy actors need to get educated on how religion works in healing so that they can be able to support service providers’ accommodation of patients’ religious beliefs as a “value-added” to treatment adherence and efficacy. Similarly, dialogues of healthcare professionals, politicians, and community members need to be opened up so that the latter can be sensitized on biomedical ethics that govern professional work. Taylor et al. 36 have advocated for dialogues between policy makers and religious leaders that can enhance the two parties’ appreciation of circumstances of people who seek alternative therapies for HIV treatment. An earlier publication from the same data set used for this article has underscored contextualizing and individualizing care as important dimensions of HIV care. 37 The reported differences in how interpreting services are viewed in participating countries sensitizes us to the importance of consideration of the context of care in designing and implementing HIV service delivery policies and in updating such policies as cultural values of communities get modified over time.
The issues surrounding interpreting provide evidence that some structure is needed to protect those who avail their interpreting services out of compassion in situations where language presents a barrier in the communication between patients and HIV service providers. Consultations with community representatives may be necessary in order that flexible structures may be put in place to aid decision making. Dialogues may be more practical than a legal framework, particularly in communities with a strong sense of community or social connectedness and who rely less on written and inflexible rules in responding to the needs of fellow human beings.
Study limitations
As ethical issues were not explicitly addressed in the research questions, this secondary analysis is limited in its ability to explore HIV care ethics in-depth. Participants may have been selective in deciding what information they could volunteer as they did not have to respond to any specific prompt about ethical issues they had encountered. Future studies focusing on qualitative description of ethical issues encountered in HIV service provision are therefore recommended. Owing to its small sample size and convenient sampling, this qualitative design limits the generalizability of the study findings. A study with a more even representation of sites augmented with a quantitative component could make the findings more generalizable.
Conclusion
HIV service providers encountered ethical challenges in all the four biomedical ethics articulated by Beauchamp and Childress. Challenges surrounding the principles of respect for patients’ autonomy, justice, and beneficence were represented by issues relating to the incongruence in the beliefs of health service providers and those of patients with regard to health and healing as well as the expected level of patients’ participation in their own care. In addition, honoring the principles of beneficence and justice became dilemmatic when politicians interfered in decisions that invaded the boundaries of professional autonomy. Challenges surrounding the principle of nonmaleficence were related to the use of interpreters when patients and service providers did not speak a common language for communicating with one another. The use of interpreters could deprive both parties of important information relating to care and could also breach the confidentiality of patients’ information by introducing the third person in the service provider-patient communication.
The findings call for more serious attention to such areas of care as religious beliefs of patients and service provision to marginalized populations such as gay and lesbians through both research and practice. There were only a few differences between the ethical issues reported at the seven US sites and those reported at the Botswana site. The differences in the use of interpreting services sensitize us to the importance of consideration of the context of care in designing and implementing policies in HIV care and in updating such policies as cultural values of communities get modified over time.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the HIV/AIDS nursing Care and Prevention, National Institutes of Health [J32 NR007081] (Portillo); Irwin Belk Distinguished Professorship, University of North Carolina Wilmington; K24DA037034 (Johnson); and the Government of Botswana Human Resources Development Council.