
Abstract
Background:
People with progressive cancer experience that their bodies change due to disease and/or treatment. The body is integral to the unity of the human being, a unity that must be perceived as whole if dignity shall be experienced. Relatives are in touch with the suffering bodies of their dear ones, physically, socially, mentally, and existentially, and thus the relatives’ experiences of the bodies of their dear ones might yield insight into the concept of dignity.
Aim:
The aim of this study is to explore relatives’ experiences of the patients’ bodily changes from a perspective of dignity.
Research design and method:
A total of 12 relatives from a hospice in Norway were interviewed. Gadamer’s ontological hermeneutics inspired the interpretation.
Ethical considerations:
The principles of voluntariness, confidentiality, withdrawal, and anonymity were respected during the whole research process. The Norwegian Social Science Data Services approved the study.
Results and conclusion:
The conversations about the body were conversations about ambivalent or paradoxical matters that shed light on the concept of dignity. The results show that the relatives got in touch with elements that otherwise would have remained tacit and unspoken, and which gave glimpses of a deeper truth, which might reveal the core of dignity. Furthermore, the relatives’ confirmation of the ambivalence might be understood as a strong ethical obligation to treat the other with dignity. The confirmation may also reveal the relatives’ unselfish love of the other, which can be understood as the core of ethics and ethos. Finally, the results reveal the relatives’ limited insight into their dear ones’ bodily changes, and we discuss the challenges of truly seeing the other. Body knowledge and the relationship between body and dignity as phenomena cannot be ignored and needs more attention and articulation in clinical nursing practice and in nursing research.
Introduction
The body is the center of human experience. It is in continuous dialogue with the world and represents the patient’s access to the world and to other people. 1 People with progressive cancer experience that their bodies change due to disease and/or treatment. These changes affect physical, psychological, social, and existential dimensions of life. 2,3
The bodily changes do affect not only the patients but also their relatives. Several studies 4 –6 show that relatives worry and have a difficult time when their dear ones experience severe cancer disease. Relatives have higher levels of anxiety and lower quality of life throughout the period of illness and also after the patients’ death. They have to handle both their own worries and take care of the one who has become ill. 4 –6 This may be detrimental to the relatives’ own health and social functioning.
The concept of dignity is important in the healthcare context, and influences the caregiver’s view of humanity and the quality of care. There has been great effort trying to clarify and enhance the understanding of dignity within nursing and caring research. 7 –10 For Kant, dignity is an absolute inner value all human beings possess. 11 Edlund, 12 Edlund et al., 13 and Eriksson et al. 14 refer to it as absolute dignity. Absolute dignity is a value that belongs to every human being simply by virtue of being human and cannot be taken away. 12 –14 Relative dignity is influenced by the culture and society that the human being is a part of and can be transformed, torn, and rebuilt. 12 –14
Edlund 12 and Edlund et al. 13 describe the body as bearer of this relative dignity. People experience dignity when they perform actions that are in accordance with the culture’s and body’s rules and norms of dignity. However, the body is also a source of violation. It holds feelings of independency and freedom, limitations, and dependency. The body also generates feelings of pride and shame, vulnerability, violation, strength, and powerlessness. It is an important part in the unity of the human being, a unity that must be whole if dignity shall be experienced. 12,13
Merleau-Ponty 15 states that peoples’ understanding of the world is based on the body’s understanding of its surroundings or situations. Any perception of a thing involves perception of the own body. The body is something we have and something we are. We exist as both body and consciousness, but the two do not exist as separate units. Merleau-Ponty 15 says that self and world are not one but neither are they completely separate. There is an intertwining between self and world, a reversibility that means that there is a folding of the self into world and world into the self. He describes this as that to touch is also to be touched, to see is likewise to be visible. To engage in the world in a sensory way means that we participate in it, are part of it, and flesh signifies this participation or intertwining. 15,16
The relatives are in touch with the sick bodies of their dear ones physically, socially, existentially, and/or mentally. Since the literature review reveals that the body influences dignity, 12,13 knowledge about the relatives’ experiences of their dear ones’ bodies might yield knowledge of what the body represents, symbolizes, and means from the perspective of dignity. Thus, this knowledge might give insight into the concept of dignity.
Research studies have explored relatives’ experiences of dignity in relation to death, but few studies 17 have examined what relatives consider to promote dignity in a palliative phase. Despite the importance of body from a perspective of dignity, we also found sparse research on the relationship between dignity and body as phenomena from the perspective of caregivers. The research we found was from the perspective of patients. 12,13,18 This study is part of a project where we try to understand more about body and dignity in a cancer context. Another study in this project, a semantic analysis where we seek to explore and understand different dimensions of the body, is in process.
Aim
The aim of this study is to explore the relatives’ experiences of the patients’ bodily changes from a perspective of dignity.
Research questions
What are the relatives’ experiences of the patients’ bodily changes? How do these experiences give insight into the phenomenon of dignity in a bodily perspective?
Methodology
The study has a hermeneutic approach based on Gadamer’s 19 ontological hermeneutics. Gadamer 19 has not developed a method of interpretation but describes how pre-understanding and data can merge into a fusion of horizons where a new understanding appears. This might happen through slow, lingering reading where the text is one of the horizons and the other is the researcher who reads the text. The intention is to seek the truth that lies behind immediate reality.
Setting, sample, and method of data collection
In order to gain insight into the relatives’ experiences of dignity, qualitative research interviews were used to collect data.
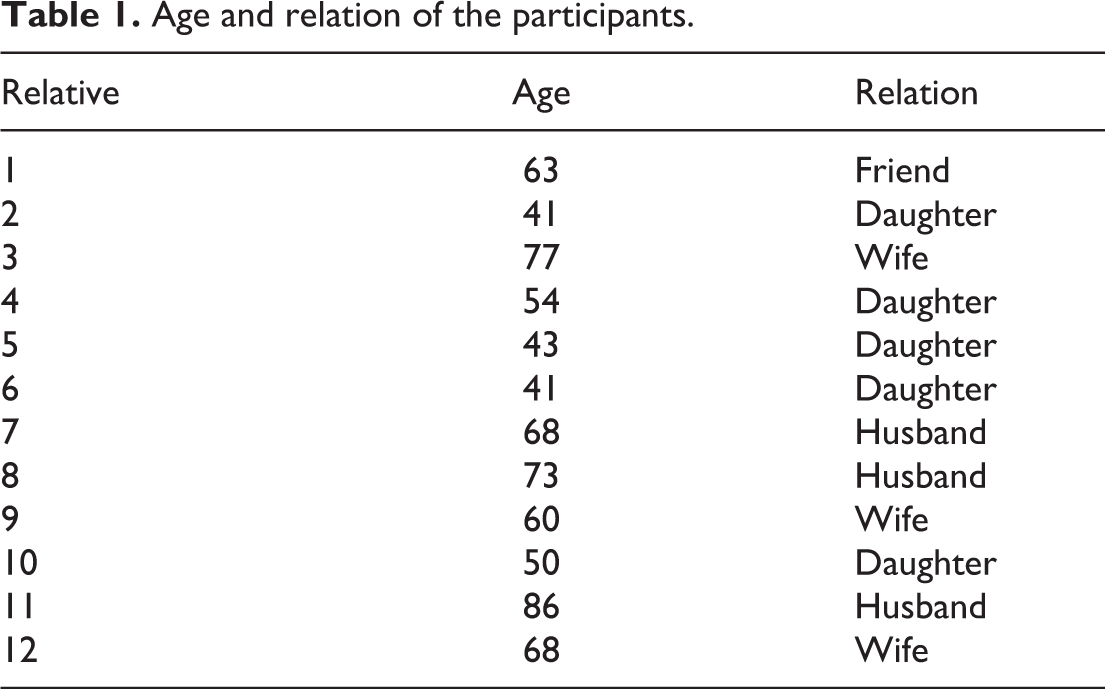
A total of 12 relatives (Table 1), 3 men and 9 women, aged 41–86 years, from a hospice in Norway, participated in the study, 10 from a hospice day care unit and 2 from a hospice inpatient unit. The relatives were the one the patients felt closest to; spouses, grown-up children, and friends. All participants spoke and understood Norwegian and were mentally aware of time and location. The period of data collection lasted from April to June 2015. One of the head nurses in the unit performed the inclusion of informants.
Age and relation of the participants.
An interview guide based on the purpose of the study and the theoretical perspective was composed. The interviews were taped and transcribed by the first author (V.B.L.). They lasted between 45 to 75 min. The transcribed interviews and the tape recordings constituted the materials for interpretation. Interviews were read of all in the research group, and the themes were agreed in discussion.
Interpretation
One may ask whether it is problematic to use a hermeneutic design while Merleau-Ponty, 1,15 who is important for understanding the body in this study, represents a phenomenological tradition. Even if it may seem contradictory, we have chosen to use both of them because Gadamer’s hermeneutic philosophy is used on a methodological level in order to understand the text, and Merleau-Ponty’s philosophy is used on another level to get a deeper understanding of the substance of the body.
Within the Gadamerian approach, our pre-understanding is essential for the understanding of meanings of texts. We discovered, during the interpretation process, that the pre-understanding was too strong and a barrier to what the text was telling us. Thus, it was difficult to formulate questions to pose to the text and to allow the text to speak, as Gadamer 19 describes it. However, we experienced that Gadamer’s 19 philosophy of play 20 helped us to creativity and engagement for the text to reveal meaning while we tried to transform his descriptions of the movement of the play into our attitude of interpretation. Gadamer describes the play as a constant movement backward and forward where the movement takes precedence over the consciousness. The movement has no goal that brings it to an end, rather it renews itself in constant repetition and brings into light what is otherwise hidden and withdrawn, and thus the play is a transformation of the truth. 19,20 We intended to have the same attitude during the interpretation process so that we openly could listen to what the text could tell us and not be captured by our pre-understanding.
Even if Gadamer has not outlined a method of interpretation, studies 21,22 have operationalized his hermeneutic philosophy to aid interpretation. We have been inspired by the four steps in Koskinen and Lindström’s 22 hermeneutic reading. The hermeneutic process started with a first reading of the interviews in their particularity and otherness. The next step was to separate larger textual units that touched and evoked wonder and extract them from the text. By lingering reading patterns of meaning units were uncovered, which through further interpretation gave new understanding.
Ethical considerations
One of the head nurses in the hospice informed the research participants about the purpose of the study and obtained written consent from the informants before the research study started. The informants were informed of the principles of voluntariness of participation, the duty of confidentiality and anonymity, and the possibility of withdrawal from participation without giving any reasons. The relatives were at a vulnerable stage in their life and this raised special ethical demands for the researcher to be sensitive and protect the relatives’ dignity throughout the research process. The Norwegian Social Science Data Services (NSD), reference number 42503, approved the project.
Results
The relatives told stories about the consequences cancer disease had for the bodies and lives of their dear ones, and what these bodily changes meant for the relatives. The relatives were concerned not only about changes to their dear ones’ physical bodies but also about the mental and existential changes. In this sense, the body is extensive and involves the whole human being and their life and not only the physical corpus.
Five themes emerged from the hermeneutic interpretation: Fear of being devoured and the struggle to hold on; A stranger—not the one I knew, but the same, nevertheless; The longing for what there was and the wish to lift up what there is; A gnawing uneasiness—the need to understand and to be invited; The vulnerable and decaying body appeals to responsibility and loyalty.
Fear of being devoured and the struggle to hold on
Relatives said that they had to stay on the outside of their loved ones’ lives because they feared that the tiredness of the patients would paralyze them. The patient’s tiredness was quite extensive and devastating and greatly affected the relatives. They struggled to keep going and felt like equilibrists who had to balance on a knife’s edge and not take the wrong steps and fall. It was tough to be the patient’s crutch, someone said. Others described their life as an earthquake, a “roof slide” and as hanging on by their fingertips. One woman said: “I cannot go down because then I’d give up, and I can’t do that. I hope it’s enough” (9).
One relative became irritated, angry, and provoked by the tiredness and unwillingness of the patient to fight and defy the fatigue. The muscles and hence life have to be triggered, she said: I don’t know why I get angry. It is an unreasonable demand; I know. He gets up in the morning, eats his breakfast and brings his coffee into the living room. Then he lies down on the sofa because he is tired. I can tell him to get up and exercise, go for a little walk, bend and stretch his legs. I feel that he doesn’t try enough. (3)
A stranger−not the one I knew, but the same, nevertheless
The relatives not only talked about the physical changes of the body but they were just as concerned with the body’s psychological, existential, and social changes. A woman described the difficulties of living in a marriage with a person who was totally changed mentally. She felt she did not know him anymore. He had become a stranger that she did not belong to anymore. Their relationship was totally changed. Being together, doing activities that provided good experiences, was important to the relationship between the relatives and their dear ones. The relatives described feelings of loneliness when this was no longer possible because of the patients’ illness.
The relatives experienced the changes in personality as more difficult to deal with than the physical changes of the body. It was hard to witness the patients in another reality and not remembering anything. The relatives were particularly concerned with the patients’ eyes which they described as having an empty gaze, as being uninhabited, absent, and alien because of the consequences of the severe cancer disease and its treatment: Her eyes are like big windows. Her drugged and gazing eyes make her look like she is absent. Not absent, but I can see when she is not with us and has to be brought back to reality. She is a bit empty and scared at the same time. (1) It is depressing to see a human being so sick and helpless. He has shrunk and there is no chance of recovery. (6) It is hard to see him just fade away. He has become extremely reduced physically. (12)
One might ask whether the patients’ bodily changes did not at all affect the relatives or whether this statement has to do with a commitment to treat their dear ones with absolute dignity. The expression “He is my husband, no matter what” (9), might imply that.
A husband also said that the illness and thus the bodily changes had made their relationship closer. He was grateful that he had this experience because he had not felt this emotionally involved in any circumstances earlier in life. He felt that the disease had brought them closer together.
The longing for what there was and the wish to lift up what there is
Relatives found it difficult to see the great negative influence the changed bodies had on the patients’ self-images. They looked back on the past and on the patient’s body as it was when he or she was healthy. They talked about how they missed the time when their loved ones had not yet become ill. Relatives’ desires to look back on how the patient was before, remembering how beautiful and vigorous he or she was, might bring back some of the pride and dignity and thus give the relatives strength and power in a difficult time.
A daughter said with pride that her father was so handsome before he got sick and that he had changed as a consequence of the cancer disease: I have a nice picture of him when he was young and in the army. He was such a handsome man, very attractive. My father has always been very good looking. I was very proud of him when I was a little girl. He had dark thick hair. There is not much left of it now…I prefer to think about him the way he looked earlier, before he got sick. (4)
A gnawing uneasiness—the need to understand and to be invited
The relatives described how the sick body sent signals that were more or less easy to understand. The signals were of a physical, mental, or existential character. The relatives described how demanding it might be to see the blurred body and interpret the signals that worried them. It was of great importance to the relatives to understand the patients’ situation and they described how difficult it was to live with a gnawing uneasiness most of the time: I think he has more pain than we have ever been told and understood. It was a shock to us when he told us that he was in a lot of pain. I would have liked to know…(5)
Some relatives were also especially concerned with how much time the patient had left and when he was going to die: I do not know how much time he has left and I do not want to know the exact date for his death. But at the same time I wonder; does he have one year left, half a year…? Can we go away for a holiday? What will the summer be like? Many people have told me that there will be signs when death is approaching, but I do not know what signs I am looking for. (10) I do not see her that often and therefore I am a bit behind and I do not know how her situation is just now. (2) I feel I have to pull out of her how she feels. Everything is good, she says. And then I suddenly discover that she is in pain. (2)
At the same time, the relatives reflected on reasons why some patients did not want to let them in. To be able to carry their bodies with dignity might involve having a private room in themselves where they could be on their own, one daughter said. This might be important to some people.
The vulnerable and decaying body appeals to responsibility and loyalty
The fight to be invited in and the great need for understanding describe the responsibility the relatives felt for their loved ones. The severity of the illness became very clear through the decaying body. It made them worried and anxious and they used all their effort to grasp what was going on.
The relatives described the responsibility in different ways. One relative described being a relative as work, work that was neither hard nor heavy. It was a privilege to live close to the patient and follow his struggle and suffering. However, later in the conversation she also said how exhausted and concerned she was and wondered whether she had enough strength to bear the pain. Another relative said that he would not be without these experiences. They had made him a more compassionate and better human being. He had earlier not been very emotionally involved in situations, but that was different now. He was happy that he had become so emotionally engaged and dependent on his spouse who was sick. He said that if you have a commitment to something or someone you also come to depend on the person or business that is your responsibility.
The vulnerable and decaying bodies also demanded loyalty from the relatives. One cannot pull a drowning man up and then leave him alone, one spouse said. Another relative expressed disgust and contempt for her father’s unhealthy body. He lived a life that was so fundamentally different from her own healthy life. She felt that many of his bodily problems were self-inflicted and nothing she wanted to deal with: My parent has lived an unhealthy life. This has been demanding because it is so fundamentally different from myself. I like to exercise, I do not smoke, I eat healthy food and I take care of my body. (4)
Interpretative discussion
The stories about the sick body were stories about how the relatives experienced being relatives. The relatives described what the patients’ body did and did not express, how this affected them, which consequences it had for their relationship, and which actions this induced.
In order to get a deeper insight into dignity in a bodily perspective, the relatives’ stories have been in a continuing dialogue with the researchers’ pre-understanding and the theoretical perspective of the study. Through this dialectical movement back and forth, we asked ourselves what does the bodily in the stories tell us and what does it mean in addition to being the concrete observable body.
The stories revealed a coexistence of opposing and conflicting feelings and experiences. The relatives described these demanding or ambivalent feelings about the other’s bodies, what this meant to them, and how they acknowledged or confirmed this ambivalence. The meaning and confirmation of this ambivalence, but also the need and the challenges the relatives expressed to understand their dear ones’ blurred body, became important to understand in relation to dignity. Thus, through an overall interpretation and dialogue with the text, four themes emerged: The demanding feelings that the body causes—a threat to dignity; The meaning of ambivalence and how this discloses aspects of truth; Confirmation of ambivalence—act of will to promote dignity; The challenges of seeing in order to understand the other’s body.
The demanding feelings that the body causes—a threat to dignity
The relatives tell about how their dear ones’ bodies bring forth feelings of anger, sorrow, sadness, discouragement, provocation, irritation, and how the sick bodies are described as strangers. They also tell how the sick bodies are demanding, annoying, and cause exhausting tensions. To endure the situation, the relatives keep themselves as much as they can on the outside of the patients’ lives.
These negative feelings and experiences of their dear ones’ bodies are in great contrast to Edlund’s statement of the body as bearer of the external relative dignity. 12,13 They are also in contrast to values such as pride, nobility, position, value, respect, grandiosity, and authority, which are some of the results in Edlund’s 12 semantic analysis of dignity. 13
At first glance, the descriptions of contrasts are contrasts between the sick and the healthy body due to the understanding of the concept of dignity in a bodily perspective, and the healthy body is the bearer of dignity. However, the healthy body is something more than just the external, apparently perfect, body that one might observe if one tries to understand the body according to Merleau-Ponty’s 15 philosophy of flesh. Merleau-Ponty 15 describes the intertwining between the body and the world as a fold where the elements fold back upon themselves.
The intertwining or the reversibility means that the body and the world are mutually dependent on each other and in a continuous dialogue. 15 That might raise the question of whether it is appropriate to distinguish between relative and absolute dignity according to the assumption that the body is bearer of dignity in the way Edlund 12 and Edlund et al. 13 claim. Maybe, it is more fruitful to understand dignity as a unity in a bodily perspective or as a value inherent to the human being 11 and not divide it into internal and external dimensions of the concept.
The meaning of ambivalence and how this discloses aspects of truth
Despite several stories about how the dear ones have changed physically, mentally, socially, and existentially, it seems as a paradox arise in all the interviews as the informants state that the patients are the same despite the bodily changes.
The paradoxes reveal an ambivalence between the relatives’ experiences and feelings and the fact that their dear ones are the same or possibly an ambivalence between what they feel and what they think they ought to feel. What the ambivalence concerns might vary from person to person, but Werkander Harstäde et al. 23 refer to Lögstrup who claims that there is an ambiguity in shame and that shame is connected with awkwardness and implies a sensitivity to boundaries that should not be crossed. One might ask whether the ambivalence may represent some of this ambiguity in shame described by Lögstrup in his work.
However, the ambivalence discloses a complexity or intertwining between contraries. The characteristics of intertwining are that something twists together and creates something new. Merleau-Ponty 15 describes that the intertwining of body and the world form a reality that is more real than the individual’s visibility. The results showed that encouraging the relatives to tell their stories from a bodily perspective might have helped them to get in contact with matters that otherwise would have remained silent and unspoken.
Confirmation of ambivalence—act of will to promote dignity
The unanimous confirmation that the patients were the same might also be understood as an act of will. The relatives had decided that their dear ones were not changed despite the several stories they told about great bodily changes. The act of will may be the power of control that minds have over their feelings. This mental control might be relatively strong in terms of the strong feelings that the participants described quite thoroughly in the interviews.
The confirmation might also be viewed as a strong ethical commitment by the relatives to not let their loved ones down. The patients’ sick bodies appeal to strong ethical obligations to be treated with dignity. The confirmation might also be grounded in the substance of love that is fundamental to being. 24 Agape love is the unconditional and unselfish love toward the other and is the core of ethics and ethos. 24,25 This love may become the duty to act in a caring manner and hold the other’s otherness with respect and dignity. Lévinas 26 also describes the ethical obligation of seeing the other’s body. He claims that the relationship to the face is immediately ethical. The relationship to the other is asymmetrical and selfless. To take ethical responsibility is to respond to the other’s appeal to be cared for.
Even if Merleau-Ponty has not formulated an ethics, it is natural to ask whether the philosophy of flesh and reversibility can be understood as ethics. Aarø 27 claims that Merleau-Ponty’s description of reversibility forms a basis for an ethics of being. He refers to an example of a painter where the painter’s interaction with the world of perception constitutes a perspective that enjoins the painter to be responsible for that perspective in communication with other individuals, and responsibility is the meaning of ethics according to Levinas. 26,28
There are also many bodily tensions or struggles in the interviews. The relatives describe their fight and effort to keep themselves going as quite exhausting and demanding strong acts of will. The relatives do not only fight for themselves but also fight for their dear ones and use a lot of strength trying to persuade the patients not to give up. However, the act of will to not allow their dear ones to let go might also evoke feelings in the patients of not having personal freedom, which again may threaten the patients’ dignity. The tensions and fights describe bodies that are not in a state of equilibrium, but in a state of imbalance, which is the opposite of the Latin meaning of dignity as equality and credibility. 14 Gadamer 29 also describes the constant movement of bodies between the loss of equilibrium and the search for a new point of stability and thereby health. According to him, we need this balance for our lived environment and for the feeling of being at home in the world.
The challenges of seeing in order to understand the other’s body
The relatives are very touched by the vulnerability and suffering of their dear ones due to the bodily changes. However, even though the relatives told several stories about how their dear ones’ bodies changed as a consequence of living with severe cancer disease, the interviews did not reveal much of what the bodily changes might mean to, and feel like, for the patients.
Merleau-Ponty 15 describes challenges concerning seeing. He says that even though we might trust that what we see corresponds with what the other sees, no person fully experiences the same as another person. The world that we see is the world as it is for us and what we see is outside the other’s body. We may therefore wonder if it is just as much their own suffering the relatives are telling us about as the suffering of the patients. García-Rueda et al. 30 confirm this and imply that much of the knowledge of the experiences of living with advanced-stage cancer are based on reports from caregivers and the perceptions of professionals, and that these reports are not so much about the concerns of the sufferer but rather provide the perspectives of others.
However, Merleau-Ponty 15 argues that even though we all have our private world, we are still in the world “floating in Being with another life” (p. 144). Through perception, there is a folding of self into the world and vice versa that mean that we touch and we are touched, we see, and we become visible. 15 This may imply that the relatives perceived more than they were able to express with words during the interviews. To make this perception meaningful, maybe, relatives need alternative ways of communication that might bring forth what is speechless.
Methodological considerations
The sample of this study consisted of 12 relatives from a hospice day care unit and a hospice inpatient unit, the relative the patient described as being the closest. No sons participated in the study. Maybe the results had been different if it was not a purposive sample, but a sample with more specific criteria. We also found Merleau-Ponty’s philosophy of great value for opening new dimensions of the body.
Conclusion and recommendation
The intention of this study has been to explore the relatives’ experiences of the patients’ bodily changes and how these experiences give insight into the phenomenon of dignity. The relatives describe sorrow, frustration, and anger evoked by the patients’ bodily changes. They feel that their dear ones have become strangers. The relatives are worried about being consumed by the difficult situation and have to use all their strength to keep going.
The conversations about the body are conversations about ambivalence or paradoxical and silent matters that might hold a deeper truth than the one immediately discovered. This deeper truth might reveal the core of dignity. Confirmation of the ambivalent or rather paradoxical body is grounded in the fundamental love for being and in an act of responsibility, both important bricks in the concept of dignity. Furthermore, the complexity of the body may make the division between absolute and relative dignity inapplicable when understanding dignity in a bodily perspective.
The study reveals that body knowledge cannot be ignored. The relatives’ understanding and experiences of the world are rooted in the body and what the body symbolizes, means, and expresses. This knowledge needs more attention and articulation in clinical nursing practice and among the nursing leadership, while this study reveals that knowledge about the meaning of the body is important in nursing care. Inviting the relatives and the patients to talk about bodily matters should be just as common as inviting them to talk about other basic needs.
Further research is also required in order to explore more about the relationship between body and dignity as phenomena, including the perspectives of patients and nurses, while it has got little attention in nursing research today. The literature review confirms that there is sparse research about the importance of body. Understanding of the body revealed in this study might be a starting point and the first brick in developing a theory about bodily dignity.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.