
Abstract
As the aging population, including frail older people, continues to grow in Mainland China, quality of life and end-of-life care for frail older people has attracted much attention. Advance care planning is an effective way to improve end-of-life care for people with advanced diseases, and it is widely used in developed countries; however, it is a new concept in Mainland China. The effects of advance care planning and its acceptability in Mainland China are uncertain because of its culture-sensitive characteristics. The objective of this article is to discuss the serious social issue of caring for frail older people and illustrate the possibility of implementing advance care planning in nursing homes in Mainland China through a review of relevant literature, which will focus on legislation, healthcare system engagement, public engagement, and cultural issues. Recommendations to promote and implement advance care planning include choosing nursing homes as a proper setting, establishing an ethical climate, and enhancing public awareness.
Introduction
The aging population in China is on the rise, and frail older people comprise a large part of that population. As frail individuals are more vulnerable to cognitive impairment and chronic diseases, 1 quality of life (QOL) and end-of-life care (EOLC) for frail older people have gained much attention. The implementation of advance care planning (ACP), which is “a communication process about the goals of care and the means of planning and recording preferences for the care of patients who may lose their capacity to communicate in the future,” 2 addresses the issue of EOLC, 3 including helping patients with an incapacity to make informed consent decisions through a proxy, 4 maintaining patients’ dignity in dying 5 and control over their life, and promoting communication among patients, caregivers, and physicians. 6 ACP has been accepted by the public and healthcare professionals 7 as can be seen by the use of advance directives, which are standardized legal forms that describe treatment and EOLC preferences and the completion rates of living wills. In response to the shortcomings of legislation on advance directives, ACP was developed. 8,9 ACP is a less legal-focused concept with a broader meaning compared with advance directives, as it focuses on the process of communication under the scope of the person-centered care model. 10
ACP has been embedded in healthcare systems in developed countries, including the regions of Hong Kong and Macao; however, it is still a new concept in Mainland China. Thus far, the literature has focused on frail older people, who represent the largest population of those aged 65 and over and the possibility and necessity of implementing ACP in Mainland China.
The prevalence of frail older people in Mainland China
In China, 11%–14.9% of people aged 65 and above and 20%–40% of people aged 80 and above have experienced frailty. 11 The general state of frailty leads to an increased risk of adverse events and, finally, death. The process of EOLC for those with severe frailty takes days, weeks, and sometimes even months. Therefore, EOLC for frail older people is an immense challenge for healthcare providers in Mainland China.
The status of EOLC for frail older people in Mainland China
In Chinese acute care hospitals, the underutilization of EOLC is a very common practice, and services are often not provided according to patients’ preferences. 12 In addition, a long-term care system and a network of community social work is still at the beginning stage in China 13 and thus an EOLC system has yet to be fully realized or created. Older people living at home and in nursing homes have access only to emergency department services and intensive care unit (ICU) admission before death, except for patients and their family members who accept a natural death at home. This phenomenon might contribute to poor-quality EOLC, 12 in which Chinese people often die without sufficient palliative care support.
The connection between ACP and EOLC for frail older people in Mainland China
Frailty is commonly accepted as a condition of weakness with adverse health problems. 14 Furthermore, frail people are also more likely to suffer from a bedridden state before death. 15 Based on these consequences of frailty, the question of whether frail older people want to discuss their EOLC and organize their end-of-life issues before death was explored by Sharp et al., 16 who showed that a majority (61%–91%) of older people wanted the opportunity to discuss their EOLC, but only 2%–29% had discussed some form of EOLC plans with healthcare professionals. The findings from that study raised two important issues: (1) are the services provided to frail older people meeting their real needs and (2) have their EOLC preferences been respected?
Life-sustaining treatments (LSTs) are normally applied at the end stage of life for most patients in China. As frail individuals are more vulnerable to cognitive impairment, chronic diseases, and severe diseases, treatment decisions are often made by the patient’s family and healthcare professionals if the patient has not implemented an ACP, which is painful for those involved. Thus, having an ACP in place before the patient becomes incapacitated makes it easier for those involved to make treatment decisions.
ACP programs are widely available around the world, and China is now ready to accept this new concept, 17 which is why it is important to choose an appropriate group of people, appropriate methods, and an appropriate place to initiate the program in Mainland China.
Implementation of ACP worldwide
The following will discuss four aspects of ACP—legislation, healthcare system engagement, public engagement, and cultural issues—as well as the advantages and disadvantages of its implementation.
Legislation
Today, most countries in North America and Europe, as well as some Asian countries and regions, have legislation on advance directives. 18 In developed countries such as the United States, Australia, and England, advance directives have their own legal status, while in other countries and regions such as Hong Kong, it represents legal persuasion without the status of a legal document. Legislative systems vary considerably according to individual healthcare systems and cultures worldwide; however, the purpose is the same—to protect patients and respect individual rights through law. For example, Taiwan approved the Hospice Palliative Care Act on June 7, 2000, to protect people from unwanted treatments through advance directives; 19 in Hong Kong, advance directives were not legislated but rather were promoted by the Law Reform Commission in 2006 and by the Food and Health Bureau in 2009; and the government of Mainland China has yet to issue a single action on advance directives. The complex process of decision-making on EOLC puzzles many clinical physicians and nurses, which has resulted in a large gap between the legalization and implementation of ACP. In addition, a lack of legislation has hindered healthcare providers’ implementation of ACP, 20 leading to the quality of death index rankings of 71st for Mainland China, 22nd for Hong Kong, and 6th for Taiwan of 80 countries. 21
Healthcare system engagement
Since doctors and nurses know how to communicate with patients and document patients’ wishes and how those wishes should be carried out, an ACP program can be applied at the healthcare system level. Four elements have been proposed by the Respecting Choices program: system design, facilitation of ACP skills education and training, community education and engagement, and quality improvement. 22 The most important place to begin in an ACP program is designing the system. The program designer must develop specific strategies to promote the implementation of ACP in healthcare settings, including documenting advance directives and patients’ preferences in their records. Paper documents are generally used, but computer-based electronic advance directives are becoming popular in some countries, such as the Medical Order of Life-Sustaining Treatment (MOLST) in the United States. 23 Documenting patients’ wishes can guide physicians in making decisions in specific situations and can induce healthcare professionals to cooperate on ACP issues. For example, if a patient does not want resuscitation if hospitalized, doctors and nurses can discuss this wish with the patient and his or her family members, have an informed consent form signed by all relevant parties, and refer the patient to a hospice ward, nursing home, or his or her own home.
Healthcare system engagement is a vital mechanism that provides an environment for healthcare professionals to carry out an ACP program. However, in China, this is one of the major barriers to implementing ACP because healthcare system engagement has not been embedded into the healthcare system.
Public engagement
In business, customers must know about a product before they can assess the quality of similar products. This principle can be used in the healthcare setting as well. If the public knows that they have a right to make decisions on EOLC, they may take action. Educating the public on EOLC issues generally falls to coalitions and non-governmental organizations (NGOs) worldwide. Most coalitions and NGOs have focused their attention on getting the public to complete forms of advance directives, such as Five Wishes in the United States and Choice and Dignity in China (Beijing Living Will Promotion Association, LWPA). 24
Another way to educate the public is through peer education, 25 group discussions, information sheets, and workshops. In the United States, some organizations have established “healthcare decisions” days or weeks to evoke public concern about true QOL and the right of autonomy in the end-of-life period. The LWPA, an NGO, is the only organization in China that has promoted advance directives, primarily through their website where people can sign electronic living wills online. The LWPA is quite active in promoting the concept of living wills through well-known people in China. The organization has also devoted great effort in expanding its influence through its website, WeChat, and charity activities, with an emphasis on the completion rate of living wills. However, because China is in the very early stage of the public being involved with EOLC decision-making, whether people understand the process of making decisions on EOLC or the purpose of advance directives has yet to be addressed.
Cultural considerations
As ACP is a culturally sensitive topic, healthcare professionals need to adapt themselves according to their understanding of cultural and clinical contexts. The following will discuss the cultural aspects of talking about death and truth telling for a better understanding of how to conduct ACP in China.
Talking about death
Death is interpreted differently in different religions. 26 Christians are taught that when they die their soul goes to heaven and is welcomed by God. 27 When Catholics die, they must confront their soul and trust in Jesus. 27 Buddhism believes that “death is not the end of life but the end of the body, as the spirit leaves the body and enters a new body and new life,” 28 and emphasizes the impermanence of lives. The fear of death results from the fear of the unknown and what will happen after death. 26,27
People with a Western cultural background are much more inclined to talk about death than Chinese people because of their exposure to death education in their culture at an early age. 29,30 Furthermore, most Westerners have faith, which helps them cope with death through a positive attitude. Finally, the necessary preparations for death, such as open discussions with family members are encouraged in Western cultures. 29
Chinese people regard death as taboo and believe that talking about death in front of a critically ill patient is bad for the patient’s health and recovery; 29,30 thus, death is simply classified and liberalized by Chinese culture. Confucius said, “Life even unknown, how about after life? Unknown life, how to know death?,” which means that if one does not know about life, one cannot talk about death. 31 Confucius accepted death and the hereafter but believed that people should pay more attention to living in the present and that it was not necessary to talk about unknown things. Confucius gave meaning to death, in that only after people gave meaning to their current life could they think about death. The proverb “Unknown life, how to know death?” has been mistaken by some Chinese people who believe that it means that one should avoid talking about death. The philosophy of death in Confucianism has impacted Chinese people’s thoughts and behaviors, including whether they accept talking about death or do not.
In summary, for those with a Western cultural background, talking about death is a common practice, whereas Chinese people are reluctant to discuss the subject because of their cultural and religious beliefs, which can hinder Chinese healthcare professionals’ assessment of patients’ needs in clinical practice. Thus, attitudes about death in China should be reassessed to educate people on EOLC issues and ACP.
Truth telling
As discussed above, religion, culture, and values shape people’s thoughts and behaviors, as well as their system of faith and practices. In Western countries, the legislative right of autonomy and informed consent takes precedence over social values, morals, religious beliefs, and relationships between people. 32 Therefore, it is the healthcare professionals’ obligation to tell the truth to patients regardless of their illness, whether stable or critical. Patients have the right to know the truth and make their own decisions about treatment. 28 If patients want to discuss their decisions with their doctor and family members, they should be at the center of all those involved, and their right of autonomy should be respected and protected by the law. 28
In Chinese culture, patients are in a vulnerable position regarding their health status, which is often kept from them by family members and healthcare professionals. 30 It is commonly agreed that telling patients the truth about their disease may not be good for their ability to manage it, especially those who have been diagnosed with cancer or a critical illness, in which case telling the truth to these patients is considered not only dehumanizing but also immoral from a cultural perspective in China. 30
Moreover, the Law on Practicing Doctors of the People’s Republic of China emphasizes that doctors must make judgments before they tell the truth and treat patients to avoid harming them. These different viewpoints of truth telling affect healthcare professionals’ practices, which can result in different clinical behaviors. Chinese healthcare providers are more concerned about cultural influences than patients’ rights and are thus less flexible than their peers in Western countries. 30
Ethical issues
Ethics regulations provide standards for healthcare professionals’ behavior in various clinical situations when making decisions and providing reasons for the decisions being made. Ethical issues often arise in ACP communication and the decision-making process because of conflicts and considerations about what are reasonable decisions for a person’s EOLC. These conflicts may occur between healthcare providers and patients, or patients and their family members, or family members and clinicians. Which treatments make sense to a person with an advanced disease? What is considered “quality of life” in EOLC? People have different views on the matter of life and death, as well as appropriate and inappropriate care. To address these differences, the four principles of ethical reasoning include respect for autonomy, beneficence, non-maleficence, and justice. 33 These principles are commonly used to guide healthcare providers in decision-making on treatment according to the clinical context.
Increased sensitivity to the diverse needs of people based on their economic status, education level, social status, culture, religion, and other views regarding EOLC issues is very important in providing care. Healthcare professionals working with families may encounter conflicts in making ethical choices based on different views. In China, many hospitals have an ethics committee to guaranty the safety of research projects or new technology used in the diagnosis and treatment of patients, which provides guidance for doctors and nurses who encounter ethical conflicts regarding EOLC.
The process of decision-making
A meaningful decision results from knowing what is required. Therefore, the process of decision-making is affected by many factors. First, patients need to have the capacity to make decisions. 34 Given that it is very important for patients to have an EOLC plan, the process of ACP requires patients to reflect on their life experiences and values, understand their illness, judge the information provided, and then make a choice.
The capacity of patients’ decision-making may be affected by a number of acute or chronic diseases, such as dementia. Therefore, it is necessary to assess patients’ capacity for decision-making, especially that of older people, and no matter the results, patients should be involved in at least the process of decision-making. Even though patients’ rights are emphasized in informed consent and autonomy in decision-making in Western countries, the process of ACP still involves family members and physicians, 35 which encourages that decisions be made by either the patient alone or with family members. The purpose of engaging family members and doctors in the process of decision-making is to ensure that treatment decisions for EOLC are understood. 29
On the contrary, family members in China generally have the privilege of making treatment decisions for cancer patients or patients with a critical condition because patients typically are the last ones to know about their illness and its treatment. The role of family members in the decision-making process in China is very different from that in Western countries, as the framework for shared decision-making has yet to be executed in the Chinese healthcare system. 30 As ACP is a new concept in China, its implementation should be shaped by Chinese culture; moreover, EOLC should be communicated to Chinese people without offending them, using the proper language in a Chinese cultural context.
Discussion and recommendations
Introducing ACP in nursing homes
As found in two systematic reviews, 36,37 there is a gap between the number of older people who want to discuss their EOLC preferences and those who are actually given the opportunity to do so. Most healthcare providers do not know that there are strategies that can help people initiate a plan for EOLC treatment in Mainland China. 38 When people learn about ACP, they show great interest in the topic. 17,38 Therefore, introducing the concept of ACP and knowing how to implement and embed it into daily work in the healthcare environment is very important. The following are some recommendations for implementing ACP.
First, since promoting ACP in Mainland China is at a very early stage, the best place to begin is choosing the right place and the right population. Nursing homes are appropriate settings for the application of ACP because most nursing home residents have complicated health problems, such as frailty and other disabilities, compared with patients in hospitals. 39 Although nursing home residents may know about EOLC issues and want their treatment preferences to be known, they may not have the ability to express their decisions on or wishes for EOLCtreatment in the future. Considering these factors, ACP is very critical and important in this setting in Mainland China.
Second, ACP communication should begin with relevant conversations about EOLC at the time of admission to a nursing home. 37 Such conversations should involve stakeholders, such as nursing home residents and their family members and healthcare providers and should be on an individual basis or sufficiently customized, as well as culturally sensitive, to reach an agreement on informed consent, respect for personal autonomy, documentation of preferences, and adherence, as much as possible, to the residents’ expressed preferences.
Third, ACP should be discussed between the nursing staff and residents during daily nursing care. In hospital settings, familial relationships are emphasized over an individual’s autonomy, so truth telling and conveying bad news is typically performed between doctors and family members. However, in nursing homes or other community settings, residents can communicate directly with the nursing staff. A previous study by the authors, which developed two paths for the implementation of ACP communication according to the person-centered theory and the family-centered theory, 40 confirmed that nursing home residents preferred to make decisions about their EOLC themselves. The first path, for long-term care facilities, is based on the person-centered theory (see Figure 1 below), in which older people make decisions by themselves, 41,42 while the second path, for acute care settings, is based on the family-centered theory (see Figure 2 below), which is frequently used in Chinese hospitals. 43
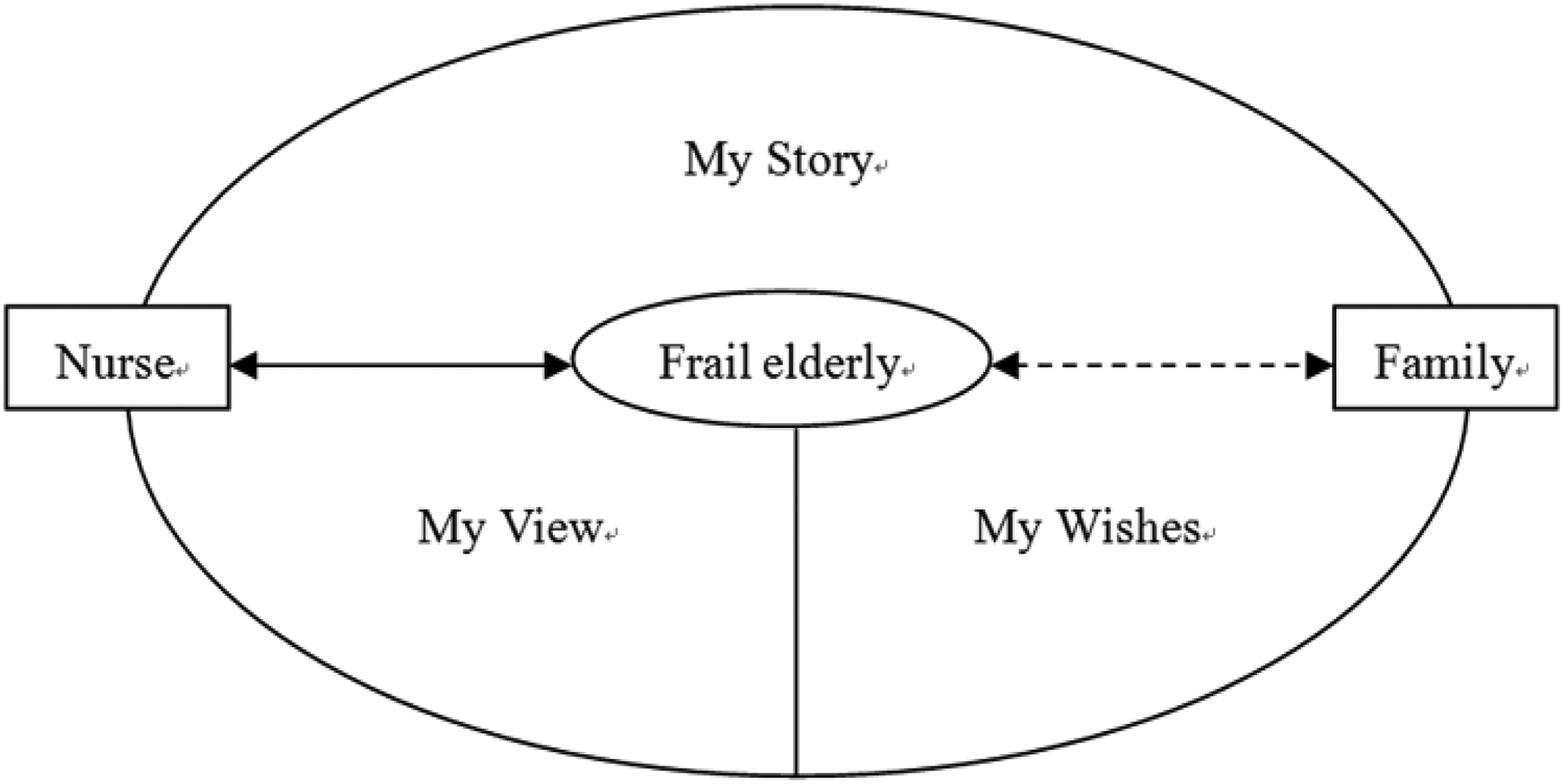
Path for long-term care facilities based on the person-centered theory.
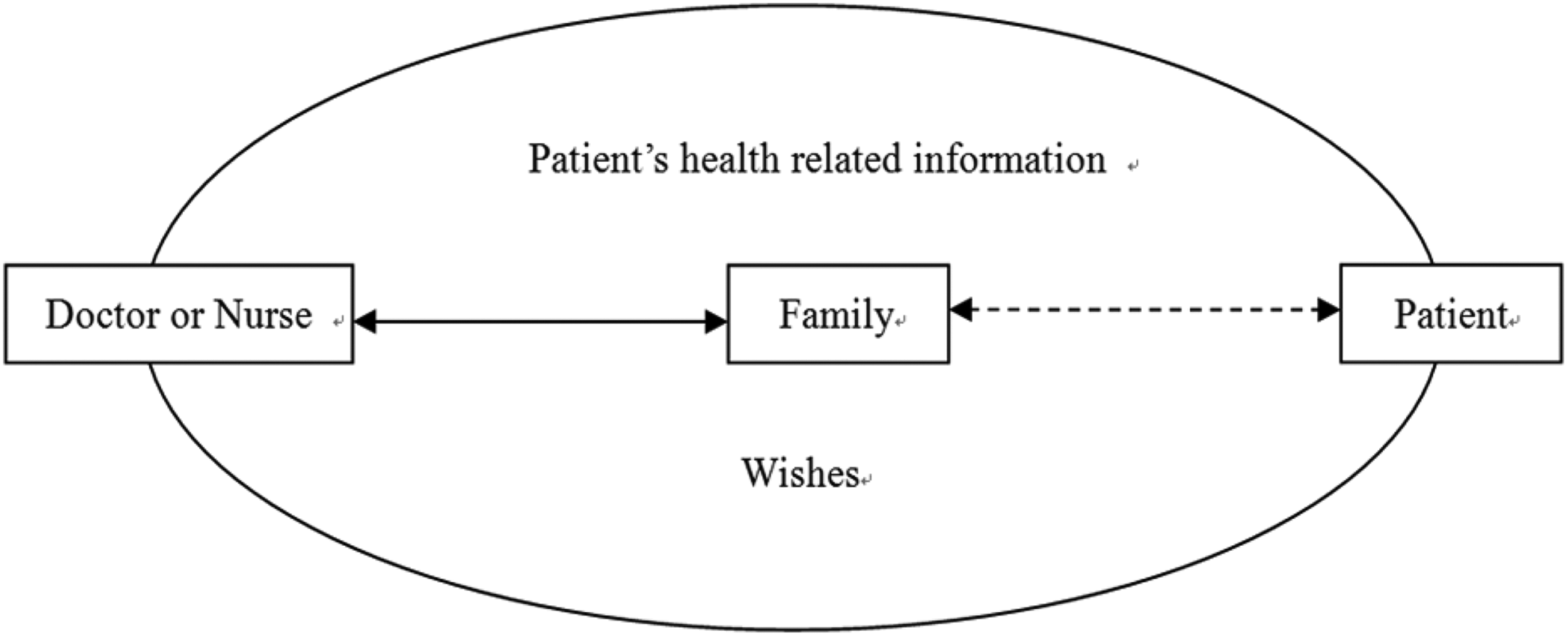
Path for acute care settings based on the family-centered theory.
In Figures 1 and 2, the ACP conversation is initiated by a nurse or a doctor, as shown in the box on the left. The dotted arrow represents the ACP conversation, which may or may not take place. In Figure 1, the structured ACP conversation is comprised of three sections: my story (which focuses on health), my views, and my wishes. In Figure 2, the ACP conversation focuses more on the patient’s health status, prognosis, costs, end-of-life span, and treatment preferences. The first path has been confirmed in the previous study mentioned, while the second path will be explored in the future.
Training healthcare providers
It has been found that if nurses have a very good understanding of ACP, introducing it to residents of nursing homes will be more readily accepted. 44 The aspects of ACP that healthcare providers should be knowledgeable in include the procedures and content of ACP communication, how to conduct an ACP program, ethical considerations when decision-making conflicts arise, and various decision-making models. Knowing how to implement ACP in the proper way and at the appropriate time in nursing homes will increase satisfaction among residents who have considered planning for their EOLC. 45
Enhancing public awareness
Public engagement is very critical in promoting ACP in China. Zheng et al. 12 demonstrated that there is a gap between the strong desire for self-determination and relevant limited knowledge of planning ahead on healthcare issues. However, because most Chinese people have no religious beliefs, 46 there are limited resources from which to receive relevant knowledge on life and death issues. In addition, there is no life and death education at any level of the school curriculum, including the medical school curriculum, in Mainland China. 47 Therefore, promoting life and death education to the public by way of school curricula, seminars, workshops, and websites can enhance public awareness of the issues of living and dying. Moreover, non-profit groups that sponsor research and develop guidelines should provide preference documents to facilitate EOLC discussions. In addition, setting up social activities such as “ACP” days or weeks and designing social logos would also be helpful in promoting ACP in Mainland China.
Establishing ACP regulations
Hong Kong’s ACP regulations offer a very good example for Mainland China to follow. Given that ACP is a new concept in China, establishing ACP regulations at the healthcare system level to guide doctors and nurses’ behavior should be considered before any legislation regarding ACP.
Ethical reflection in ACP implementation
Principles and methods used to make decisions on EOLC
As confirmed by Chan and Pang’s 41 study, patients found that it was easy to start a conversation about their own health situation; therefore, following the principle of informed consent, detailed information about their health status needs to be provided. A question prompt list (QPL), which has been recommended in three studies, is a very useful instrument for advanced cancer patients and their caregivers to guide physicians. 45,48,49 It has been suggested that a QPL based on Chinese culture should be developed for frail older people and their family members to guide them in asking questions about the patient’s health.
Furthermore, regarding decision-making conflicts, doctors and nurses should follow the best interests of their patients. Frail older people often experience long-term chronic diseases that can cause them to think about their EOLC, 37 and decision-making conflicts generally arise from disagreements with their family members. 42 To mitigate these conflicts, a family meeting to discuss decision-making on EOLC is recommended. Family values and personal autonomy should be respected in making a final decision. Healthcare providers must learn how to relate a shared decision-making model that combines familialism and medical paternalism during family meetings to cope with disagreements on EOLC decision-making. 50
Establishing an ethical climate
One study with 1215 participants reported that nurses and social workers felt powerless (32.5%), overwhelmed (34.7%), fatigued (40%), and frustrated (52.8%) when they were confronted with ethical issues. 51 To help nurses and doctors mediate ethical conflicts, an ethics committee should be established in healthcare facilities. The ethics committee should develop guidelines to enable healthcare providers to cope with ethical issues at the beginning stage, update relevant ACP documents, develop a QPL to help patients and their family members ask questions, and control the quality of ACP. Creating a supporting environment for healthcare providers can increase their compliance to implementing ACP.
Conclusion
This article will examine the implementation of ACP in China, beginning with the best place to promote ACP and when and with whom ACP communication should take place. From cultural and social aspects, other recommendations include training healthcare providers, enhancing public awareness, and establishing regulations for ACP. Furthermore, based on Chinese culture, a shared decision-making model should be employed to help frail older people avoid decision-making conflicts and increase QOL. Finally, an established ethical climate can provide strong support for healthcare providers when they are confronted with ethical conflicts. This article will conclude with a discussion on how these recommendations can facilitate the implementation of ACP in China.
Footnotes
Acknowledgements
R.-L.D., Diana T.F. LEE and J.-Z.D. conceptualized the study. L.-L.C. and Z.J.-H. conducted the review and entered the data. R.-L.D. wrote the first draft of the manuscript. Then Diana T.F. LEE and J.-Z.D. provided critical edits, and R.-L.D. revised the manuscript. Finally J.-Z.D. and Diana T.F. LEE approved the manuscript. This article adapted from R.-L.D.’s doctoral thesis which was an original study for the doctor of nursing degree.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant no.: 71663064).