
Abstract
Background:
Moral distress and workplace bullying are important issues in the nursing workplace that appear to affect nurse’s burnout.
Aim:
To investigate the relationship between moral distress and burnout in Iranian nurses, as mediated by their perceptions of workplace bullying.
Ethical considerations:
The research was approved by the committee of ethics in research of the Urmia University of Medical Sciences.
Method:
This is a correlation study using a cross-sectional design with anonymous questionnaires as study instruments (i.e. Moral Distress Scale-Revised, Maslach Burnout Inventory and The Negative Acts Questionnaire-Revised). Data were collected from 278 nurses from five teaching hospitals in Urmia, the capital of Western Azerbaijan, northwest of Iran. Structural equation modeling and bootstrapping procedures were employed to recognize the mediating role of their perceptions of workplace bullying.
Results:
The mean score of moral distress, burnout, and the Negative Acts Questionnaire-Revised Scale among the participants were 91.02 ± 35.26, 79.9 ± 18.27, and 45.4 ± 15.39, respectively. The results confirmed our hypothesized model. All the latent variables of study were significantly correlated in the predicted directions. The moral distress and bullying were significant predictors of burnout. Perception of bullying partially mediated the relationship between moral distress and burnout. The mediating role of the bullying suggests that moral distress increases burnout, directly and indirectly.
Conclusion:
Nursing administrators should be conscious of the role of moral distress and bullying in the nursing workplace in increasing burnout.
Introduction
Iranian nurses, as nurses of a developing country, face many challenges in their work when performing their obligations. These challenges are generally due to nursing shortages, job dissatisfaction, low salaries, and poor social position of nurses. 1 These challenges reduce quality of nursing care through increasing their workload and hence result in wrong actions. Wrong actions can lead to moral distress of nurses. 2 On the other hand, nurses mostly make ethical decisions in their workplace, while they may not be fully aware of it. Many situations including, illness, aging, suffering, and death of vulnerable patients are among other situations in which the nurse must make his or her own decision about moral action. 3 Nurse advocacy role and responsibilities to patients, families, society, and colleagues, as well as background restrictions, further increase the likelihood that nurses will experience moral distress. 4 moral distress is defined as the psychological disequilibrium and negative sense experienced when the nurse makes a moral decision but does not implement it or do the right thing because of hierarchical limitations. 5 A clear example to explain distinctions between moral distress and emotional distress is given by McCarthy and Deady: 6 “while restraining patient, a psychiatric nurses may experience emotional distress but she is likely to become morally distressed only if she believes that restraining the patient is morally a wrong action.” The literature shows that moral distress causes many physical and emotional problems in nursing such as anger, guilt, helplessness, stress, burnout, job dissatisfaction, negative changes in self-image, and spirituality and leaving nursing. 7 –10
Burnout is one of the major problems hindering all health systems and a known syndrome among health sector staff. 11,12 The syndrome is formed in response to work-related chronic mental pressures. Burnout complications include physical complaints, sleep problems, depression, social dysfunction, resignation, repeated absences, reduced energy and work efficiency, reduced job satisfaction, and reduction in the quality of patient care and services. 13 Burnout is considered a major risk factor for leaving a job. 14 Some studies proposed that there is a positive correlation between burnout and moral distress. 10,15,16 Johnson-Coyle et al. 17 suggest that the most detrimental result of moral distress is in fact burnout.
Workplace bullying, often known as “horizontal/lateral violence” in the nursing literature, has recently gained global attention. 18 The concept of workplace bullying was introduced by a Swedish psychologist, Heinz Leymann, in early 1980 and later became known as bullying in England. The synonyms in the nursing literature include “verbal abuse” (also known as “reviling or verbal bullying”) and “workplace aggression.” 19 Bullying differs from the usual workplace conflicts. It occurs more frequently, lasts longer, and a victim is unable to defend oneself or stop the negative activity, as the victim is weaker than the bully. 19 Bullying behaviors in a workplace occur in different forms, and they can be extremely well hidden and difficult to recognize. Bullying behaviors include threats and damage to professional status, such as the use of rude phrases, constant criticism, humiliation, intimidation, and false accusations. 20 The isolation of people through some acts, such as deprivation of information, refusing to answer telephone calls and e-mails, and ignoring the victim, are types of bullying behaviors. Moreover, the professional status of an individual exposed to bullying may become unstable due to negative activities, such as the assignment of trivial tasks that are often below their actual abilities. 21 The literature reported a few reasons for bullying, including organizational changes, workplace reconstruction, and organization downsize. 22 The pressure on nurses due to increased workload and improved cost-effectiveness also provide a foundation for bullying behaviors. 23 In all, 1%–5% of the workforce in the Scandinavian countries has experienced bullying, which mostly occurs among colleagues at the same organizational levels. 24 The figures for the United States and England are much higher (10%–38%), as most managers and supervisors bully. 25 In Korea, 15%–23% of nurses are believed to be victims of bullying. 26 The literature showed only two studies 27,28 in Iran on the frequency of workplace bullying of nurses; these studies, however, are not sufficient for clarifying the different aspects of this concept. Esfahani et al. have stated that only 31% of the participants in their research experienced bullying at work. They collected their research data from nurses working in private hospitals. 27 Golparvar and Rafizadeh 28 found that there is a significant relationship between bullying with psychological well-being and spiritual well-being among Iranian nurses. Both studies had insufficient sample size and used no standard tool for measuring the concept of bullying.
Workplace bullying is highly destructive physically, mentally, socially, and functionally. The workgroup members that witness bullying experience stress and psychological problems such as anxiety, depression, and suicidal thoughts. 29 A total of 10% of nurses reported thoughts of suicide due to workplace bullying. 30 Bullying victims also reported physical symptoms such as lightheadedness, abdominal pain, back pain, and insomnia. They also have higher body mass indexes and are more prone to chronic diseases. 31 These people are absent from work due to their disease more often, as 2% of absences are due to workplace bullying. 32
There is a direct and casual relationship between bullying and burnout. 33,34 The results of many studies indicate that bullied nurses presented significantly higher levels of burnout. 35 –37 Symptoms of burnout (emotional exhaustion and depersonalization) were higher and more frequent among nurses who reported to have been bullied. 38,39
Although moral distress and workplace bullying have been well studied separately, no one to the best of our knowledge has studied the possible relationship between them. Here, we wish to explore the hypothesis that moral distress is associated with workplace bullying. In addition, according to the literature, moral distress is recognized to be associated with different aspects of an organization (e.g. ethical climate, job satisfaction, organizational commitment, and organizational citizenship behaviors). 40,41 Therefore, the role of workplace bullying on the moral distress–burnout relationship is expected in our hypothesis. Indeed, nurses who perceive moral distress and feel to be victim of bullying might report burnout.
The framework of this study is influenced primarily by the existing theoretical models in organizational psychology and nursing research that suggest work characteristics affect nurses’ outcomes. 42,43 Rochefort and Clarke 42 state that work environment as a set of concrete or abstract features of an organization, related to both the structures and processes in that organization that are perceived by nurses as either facilitating or constraining their professional practice. A desirable workplace empowers nurses to practice to the full scope of their knowledge, competencies, and skills in patient care. In such an environment, nurses are more satisfied, suffer from less burnout, and provide higher quality of care. 44
The literature shows that moral distress in the nurses’ work environment causes stress. 45,46 On the other hand, stressful working environments have long been assumed to create conditions that may lead to the development of workplace bullying. 47 Therefore, in this study, we hypothesized that moral distress caused workplace bullying in the workplace and tested this hypothesis.
Thus, stemming from theory and the reviewed literature, we hypothesized that: (1) the nurses’ moral distress would affect their burnout; (2) the nurses’ moral distress would affect their perception of workplace bullying; (3) the nurses’ workplace bullying would affect their burnout; and (4) the perception of workplace bullying by the nurses would cause mediating effects on the relationship between their moral distress and burnout (Figure 1).
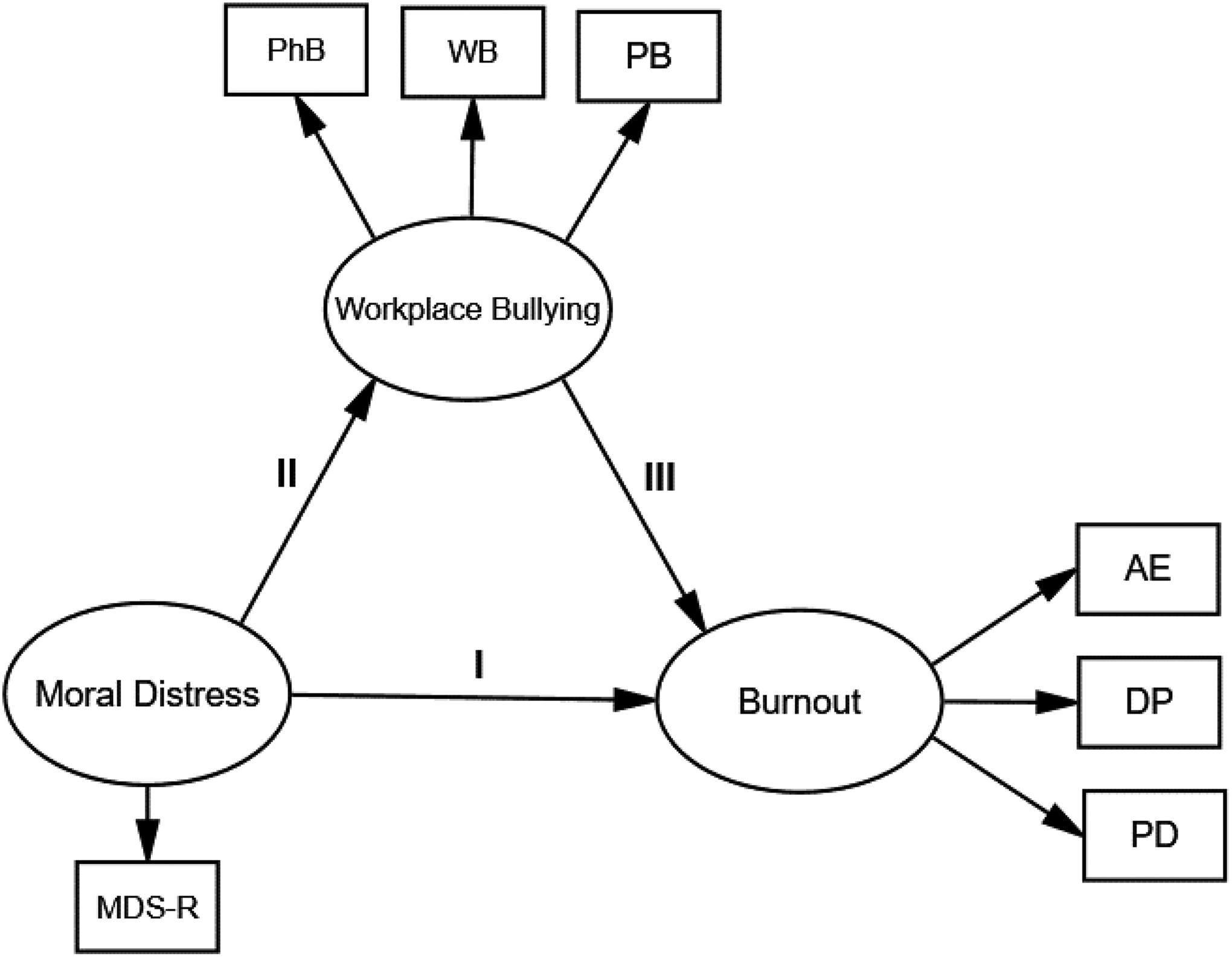
The hypothesized model.
The main purpose of this research was to examine the direct and indirect effects of variables on burnout among Iranian nurses. To the best of our knowledge, this is the first research that aimed to examine the associations between moral distress, workplace bullying, and burnout among Iranian nurses. Particularly, moral distress would positively predict bullying and workplace bullying would positively predict burnout in these nurses. A perception of workplace bullying would mediate the relationship between the moral distress and the nurses’ burnout.
Methods
Aims
The objective of this study was to study the relationship between a group of Iranian nurses’ moral distress and their burnout, as mediated by their perceptions of workplace bullying.
Study design
This is a correlational study with a cross-sectional design.
Setting, data collection, and sample
This study was conducted in Urmia, the capital of Western Azerbaijan, northwest of Iran. The nurses were randomly selected from five teaching hospitals in the city, and only those with at least 1 year of experience were included. Nurses working in private hospitals, part-time nurses, and those working in clinics were not included. Based on earlier studies, sample size was calculated as 325 with respect to the possible attrition of 20% of the participants. The sample was heterogeneous and included nurses in a variety of roles, age groups, and levels of education and seniority. This was done to have an illustrative sample of the entire target population. Two interviewers on different shifts in different wards distributed the questionnaires. The questionnaires were administered at the end of the shift when nurses were living in the hospital. The questionnaires were administered anonymously and the participants were assured that their responses were confidential. A cover letter was attached to the questionnaires explaining the research objectives. It was likely that those who experienced bullying would be more likely to participate in the study. Therefore, the term “bullying” was not included in the questionnaire, and the participants only become familiar with this term at the end of the questionnaire (Question 23). This prevented possible biases. A certain place was reserved in each hospital to allow the participants to fill the questionnaire in a quiet environment. In this case, the research assistants could answer the possible questions of participants. The entire procedure lasted approximately 30 min. Of the 325 questionnaires, 26 were filled out incompletely and 10 questionnaires were not filled out. Eleven nurses refused to cooperate in the research. A final total of 278 questionnaires were analyzed (response rate: 85.5%).
Ethical considerations
The research was approved by the committee of ethics in research of the Urmia University of Medical Sciences (ir.rec.umsu.1395.26). Furthermore, all scales in this study were used with permission from their respective designer. All the participants were included willingly and provided written consent. The participants were assured of the confidentiality of their information. Finally, it was explained to them that they were not required to write their names on the questionnaires.
Measurements
Moral distress
In this study, we utilized Moral Distress Scale-Revised 48 to measure the perception of moral distress among participants. The MDS-R contains 21 items. It measures an individual’s perceptions to a situation based on (1) intensity of moral distress ranging from 0 (none) to 4 (great extent) and (2) frequency of the encountered situation ranging from 0 (never) to 4 (very frequently). The data are then computed into a composite score of actual moral distress using a 2-way procedure. First, the frequency score and the intensity score are multiplied for each of the items. The score for every item can range from 0 to 16. Second, the total score for each scale is obtained by adding up the scores of all items (frequency multiplied by intensity), which can be between 0 and 336. Higher scores indicate higher moral distress. Hamric et al. 48 determined the reliability of the questionnaire using Cronbach’s alpha coefficient of 0.89. Soleimani et al. 49 translated the scale to Farsi (after obtaining permission from the inventor of the scale) and then confirmed the face, content, and construct validity of this scale in a sample of Iranian nurses. In our study, Cronbach’s alpha for frequency and intensity of moral distress was found to be 0.91 and 0.89, respectively.
Burnout
This research used the Maslach Burnout Inventory (MBI) 50 to measure burnout. MBI contains 22 questions and is based on the Likert-type scale. The inventory measured emotional exhaustion, depersonalization, and lack of personal fulfillment within a professional activity framework. The responses are based on a severity scale in the range of never (0) to very much (6). Maslach et al. 51 reported the internal validity for the three aspects of emotional exhaustion, depersonalization, and lack of personal fulfillment as 0.90, 0.79, and 0.71, respectively. A study in Iran measured emotional exhaustion, depersonalization, and lack of personal fulfillment as α = 0.84, α = 0.81, and α = 0.74, respectively. 52 In this study, Cronbach’s alpha for the questionnaire was 0.84.
Workplace bullying
The Negative Acts Questionnaire Revised (NAQ-R) 18 questionnaire was used to measure workplace bullying. The NAQ-R measures victims’ perceptions of workplace bullying in a 6-month period. It has 22 questions and consists of three subsections measuring physical, work, and personal bullying acts. 18 The participants are asked how many times they had experienced 1 of the 22 questions in the questionnaire. The responses include never, now and then, every month, every week, and every day. Two methods are used for scoring the questionnaire. In the first method, the questions whose responses are never, now and then, and monthly are scored as 0. The questions whose responses are every week and every day are scored as 1. If a participant’s total score is equal to or greater than 2, they have been subjected to bullying according to the scientific definition of bullying. In the second method, any response is scored 1 (never) to 5 (every day), and the total scores indicate the total score of the questionnaire. The higher the score, the more the individual has become a victim of bullying. The validity and reliability of the NAQ-R questionnaire was reported by the tool’s creator. Cronbach’s Alpha for reliability was 0.89. 18 Sá and Fleming 39 obtained a high internal consistency for the questionnaire (Cronbach’s Alpha: 0.87). Before starting the data gathering, the NAQ-R questionnaire was first translated and then validated. To guarantee the questionnaire’s validity, two professors fluent in English, one active in the field of psychology and the other in the field of management, translated the questionnaire individually. A Persian version was prepared after comparing the two translated versions. In the next step, one professor fluent in English who was not aware of the contents of the primary questionnaire made a reversed translation (i.e. from Persian into English). Finally, after comparing the two versions, no report was received from the respondents concerning the conception of the questions. To determine content validity, we made use of the opinions of 11 individuals specialized in this field and the board members of the Faculty of Nursing and Midwifery of Urmia. In this study, Cronbach’s alpha of the questionnaire was 0.91.
Data analysis
The data were analyzed in SPSS and AMOS Ver. 23. The demographic characteristics of the participants, bullying prevalence, burnout level, and moral distress were analyzed proportionally using frequency, percentage, mean, and standard deviation (SD). the relationships between moral distress, burnout, and workplace bullying were determined using Pearson’s correlations. The two-step modeling procedure of Anderson and Gerbing 53 was used to detect the mediation effect. The first step tested whether the measurement model was suitable, by assessing the degree to which all the latent variable structures fit the model. If all the latent variables were well represented by the indicators, then we confirmed the structure of the model in the second step. Therefore, the measurement model provided the convergent validity and differential validity, whereas the constructed model provided the predictive validity. Chi-square values, the comparative fit index (CFI), the root mean square error of approximation (RMSEA), and the standardized root mean residual (SRMR) were used to evaluate the model fit. A nonsignificant chi-square value indicates a good fit between the model and the data. The general cutoffs to accept a model included a CFI equal to or greater than 0.95, an RMSEA equal to or smaller than 0.05, and an SRMR smaller than 0.08 (the path coefficients were accepted as significant at the 0.05 level). 54
Results
Demographic characteristics of participants
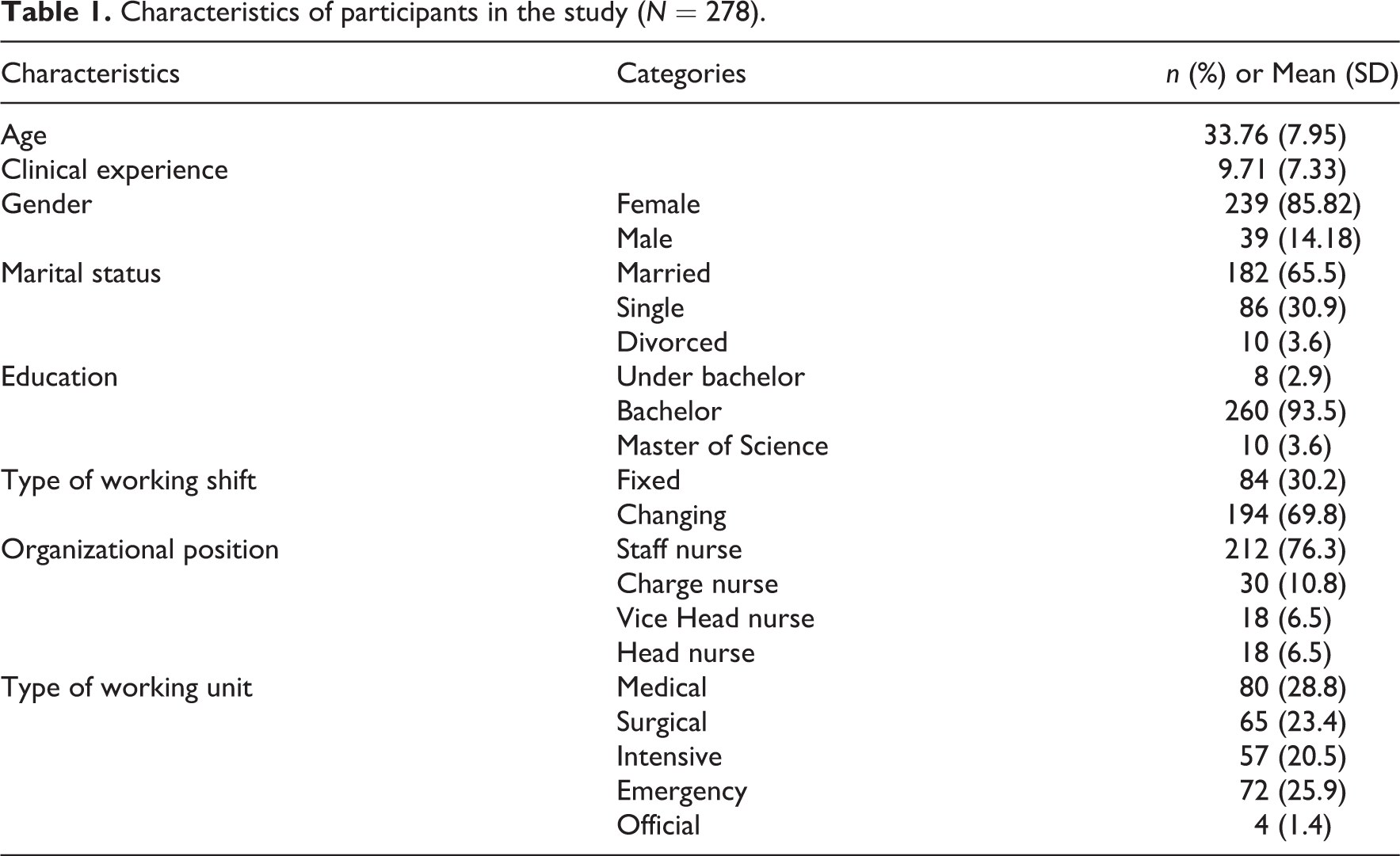
The mean age of the participants was 33.76 ± 7.95 years. The average clinical experience of the nurses was 9.71 ± 7.33 years. A total of 239 of the participants were females (85.82%). Most nurses were married (65.5%) and had BS degrees (93.5%). Most participants had rotating working shifts (69.8%). The majority of nurses who filled out the questionnaires were staff nurses (76.3%; Table 1).
Characteristics of participants in the study (N = 278).
Moral distress, workplace bullying, and burnout among participants
The mean score of MDS-R was 91.02 ± 35.26 in the participants indicating that the level of moral distress in Iranian nurses is low. The most frequent item was (carry out the physician’s orders for what I consider to be unnecessary tests and treatments) and the least (follow the family’s wishes for the patient’s care when I do not agree with them, but do so because of fears of a lawsuit), with the mean scores being 2.65 ± 1.20 and 1.11 ± 0.9, respectively. The highest intensity also pertained to the item (I have witnessed that the quality of care is reduced due to poor team communication) and the lowest to item (increase the dose of sedatives/opiates for an unconscious patient that I believe could hasten the patient’s death), with the mean scores being 2.11 ± 1.12 and 1.71 ± 1.02, respectively.
The mean of the total score for MBI in participants was 79.9 ± 18.27. The mean of emotional exhaustion, depersonalization, and lack of personal fulfillment subscales were 35.55 ± 10.73, 21.78 ± 5.99, and 22.56 ± 7.84, respectively. According to the opinion of Maslach et al., 51 the level of all three subscales in this research is high.
The mean score of the NAQ-R scale among the participants was 45.4 ± 15.39. The mean of Questions 4 (pressure not to claim something you are entitled to) and 22 (unmanageable workload) among the participants exceeded that of other questions (2.62 ± 1.32), which indicates the frequency of these two negative acts among the participants. The negative act described in Question 1(someone withholding information that affects your performance) had the minimum prevalence among the participants (1.5 ± 0.78).
Correlations among the main variables
As the correlations are shown in Table 2, all the variables were significantly correlated in the predicted directions. The correlation among the moral distress, burnout, and the workplace bullying was significant in all dimensions.
Correlations among main variables of study.

MDS-R: Moral Distress Scale-Revised; PhB: physical burnout; WB: work bullying; PB: personal bullying; AE: affective exhaustion; DP: depersonalization; PD: personal deficit.
**p < 0.01.
*p < 0.05.
Measurement model
Three latent variables, moral distress, bullying, and burnout and six observed variables were studied. The measurement model showed a good fit as follows: χ2 = 64.4 (22, 299), p = 0.009, RMSEA = 0.06, SRMR = 0.04, and CFI = 0.96. Furthermore, all the factor loadings for the indicators on the latent variables were significant (p < 0.001), indicating that all the latent variables were well represented by their indicators.
Structural model
The direct standardized path coefficient from the independent variable (moral distress) to the dependent variable (burnout) was significant in the absence of mediators, β = 0.62, p < 0.001. The results found that the total effect of moral distress on burnout decreased when the mediator (bullying) was included in the model (β = 0.51, p < 0.001). A partially mediated model with mediator and a direct path from moral distress to burnout exhibited a good fit to the data: χ2 = 64.4 (22, 299), p = 0.009, RMSEA = 0.06, SRMR = 0.04, and CFI = 0.96 (Figure 2). Moreover, testing of the parameter estimates showed that the path coefficients from moral distress to burnout, from moral distress to bullying and from bullying to burnout were all significant. As the bootstrap method yields the most accurate confidence intervals for indirect effects, 55 so we took advantage of the bootstrap estimation procedure 56 (with a specified bootstrap sample of 5000) to test the significance of the mediation effects of bullying on the relationship between moral distress and burnout. Taken together, all the hypothesized direct effects among latent variables (depicted in Figure 2.) were significant. Notably, the indirect effect of moral distress on burnout via the perception of workplace bullying was similarly significant (Table 3).
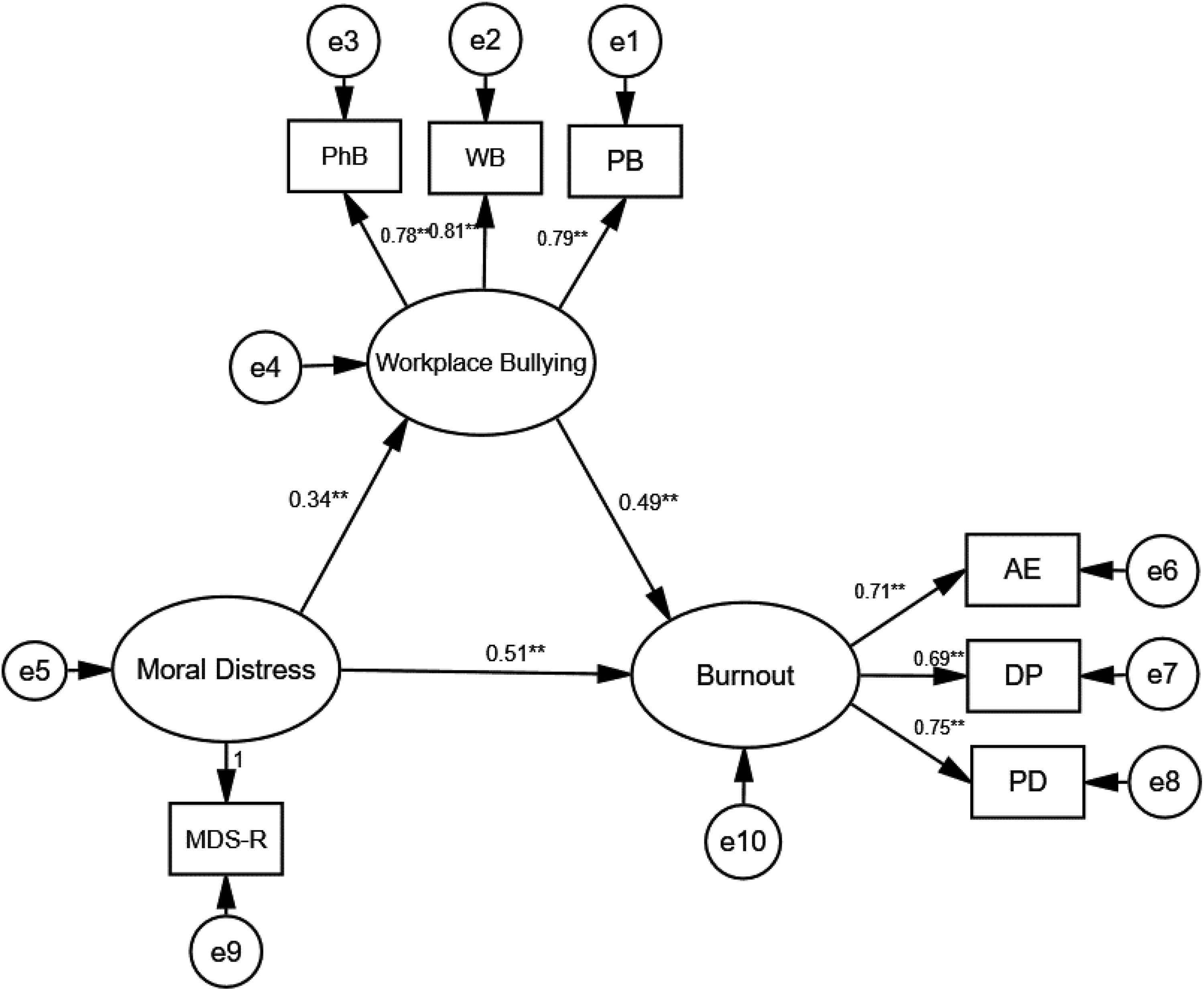
The final structural model (n = 278).
Direct and indirect effects and 95% confidence intervals for the final model.

CI: confidence interval.
* Empirical 95% confidence interval does not overlap with zero.
Reversed model
To elaborate more on the relationships and the hypothesized directions among study latent variables and to determine the casual relationships between latent variables, we also tested the reverse model (see Figure 3). To construct the reverse model, the paths between latent variables were assumed reverse. The results showed that all path coefficients between latent variables were insignificant. The fit indices of the reverse model (χ2 = 91.6 df = 22, RMSEA = 0.13; SRMR = 0.11; and CFI = 0.88) are unsatisfactory. Therefore, the reverse model is not acceptable. This finding showed that the direction of the assumed paths in the “hypothesized model” is correct, and the reverse paths between the main variables of the study are not correct. For example, moral distress is a predictor of workplace bullying, while workplace bullying is not a predictor of workplace bullying.

The reversed model (n = 278).
Discussion
In this study, the mean score of moral distress in nurses was low, which is consistent with the results of some earlier studies. 48,57 Our results are in contrast with some that showed high levels of moral distress among nurses. 58,59 The results of Soleimani et al. 60 similarly showed low levels of moral distress in Iranian nurses. In this study, low moral distress can be attributed to work environments (wards). Due to the fact that the intensive care unit (ICU) nurses had little share in our study sample, it is possible that the nurses sampled in our research engage with fewer ethical problems compared with those who work in the ICU, which may clarify why they demonstrated lower levels of moral distress.
The burnout level among the nurses was high, which is consistent with the findings of other studies in Iran. 61,62 Thus, it is necessary to use policies for lessening burnout.
The prevalence of workplace bullying in this study was 46% (i.e. approximately half of the nurses are victims of workplace bullying). The prevalence of bullying is higher than one of the only earlier studies in this field that was also conducted in Iran, 27 in which one-third of the nurses were recognized as workplace bullying victims. This score is neither as low as the Scandinavian countries nor as high as that in Turkey. 30 It has the highest similarity with the prevalence in the studies of Quine 21 and Kurtis et al. 63 in Britain and Australia, respectively. Generally, such prevalence is much higher than that in other professions. 64 The reason for the high prevalence of bullying among nurses is the nature of the profession, which is very stressful. A high-volume workload in this profession is also a contributing factor. 65 In Iran, as a developing country, some problems such as nurse and hospital shortage lead to hospitals being crowded, as is evident by the bed occupancy rate of over 80% in many hospitals, and the lack of timely payments for overtime and bonuses increase the stress of nurses and intensifies clashes among them.
As stated in the “Introduction”, the main purpose of this study was to investigate the relationship between moral distress, workplace bullying, and burnout of Iranian nurses. This study extended preceding research concerning moral distress, bullying, and burnout. Specifically, we contended that the nurses’ moral distress is associated with their perceived workplace bullying, which would have an effect on burnout. In the interpretation of this finding, it should be noted that the existence of moral distress in the workplace of nurses increases their stress. This stress, in turn, provides conditions for the onset of workplace bullying. As for the relationship between moral distress and job burnout, it is possible that moral distress could lead to internal constraints such as uncertainty, lack of self-confidence, fear, worry, and other situations that predispose to burnout. 66
Similar to previous studies, the results of this research support the idea that a perception of workplace bullying can increase burnout of nurses. Indeed, when bullying happens, nurses working in unfriendly and stressful organizational climates are normally inclined to consider it as deliberate and damaging, to perceive the importance of the event, and to feel a victim and at risk of burnout. 67 Therefore, people perceiving a bullying and stressful organizational climate are more likely to report job burnout. 68
Notably, the perceived workplace bullying partially mediated the relationship between the nurses’ moral distress and their burnout. Thus, nurses with a high level of moral distress might perceive more bullying which causes a high level of burnout. This has not been shown in prior studies. The mediating role of bullying should provide new insights to reduce the job burnout in nurses. Indeed, bullying is a factor that can be addressed 69 (e.g. supporting victims of bullying, teaching the nurses about workplace nurses, developing policies to address workplace bullying, and celebrating positive and bully-free work environments) to decrease burnout. The present findings showed that only focusing on workplace bullying to address burnout is not sufficient, and nursing managers should pay particular attention to reducing the moral distress of nurses. Recently, several approaches to reducing moral distress have been published 70 –72 that can be applied by nursing managers (e.g. American Association of Critical Care Nurses 4 A’s 73 ).
Research limitations and recommendations for future studies
As the study was conducted in the state hospitals of Urmia in Western Azerbaijan, cautions should be exercised in generalization of the results for other nurses. Future studies should be conducted using a larger sample size and in a broader geographic area. Our study design also prevented us from making causal inferences about latent variables. A longitudinal design could better explain the causal relationships between the study variables. Another limitation is that this study, which is based on self-report data, is vulnerable to common method biases. 74 Hence, ensuring respondent confidentiality and counterbalancing the questionnaire items were employed to minimize the bias. The other research limitation was data collection through paper questionnaires. Some nurses might have been unable to express their real opinion of the hospital environment while being with their colleagues. Therefore, it is recommended that future studies use an electronic method (sending e-mail) to allow nurses to fill out questionnaires in an environment other than wards. As the NAQ-R is a general questionnaire for many professions, it cannot cover all aspects of the bullying phenomenon in nursing.
Conclusion
This study shed light on the relationships between nurses’ moral distress, their perception of workplace bullying, and their burnout. Our results suggest that the perception of workplace bullying might be influenced by a nurse’s moral distress. Therefore, managers might reduce burnout not only by decreasing workplace bullying but also by paying attention to individuals’ moral distress.
Footnotes
Acknowledgements
The authors appreciate all the nurses who participated in this study.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Research Department of Urmia University of Medical Science financed this research [Grant No. 1395.26].