
Abstract
Background:
Palliative care is acknowledged as an appropriate approach to support older people in nursing homes. Ethical issues arise from many aspects of palliative care provision in nursing homes; however, they have not been investigated in this context.
Aim:
To explore the ethical issues associated with palliative care in nursing homes in the United Kingdom.
Design:
Exploratory, sequential, mixed-methods design.
Methods:
Semi-structured interviews with 13 registered nurses and 10 healthcare assistants (HCAs) working in 13 nursing homes in the United Kingdom were used to explore ethical issues in palliative care. The ‘Ethical Issues in Palliative Care for Nursing Homes’ instrument was used to measure the frequency and level of distress arising from ethical issues through a cross-sectional survey with 69 registered nurses and 129 healthcare assistants. Data collection occurred between December 2014 and November 2015.
Ethical considerations:
Ethical approval was granted by Queen’s University’s School of Nursing and Midwifery Research Ethics Committee and governance sought from each nursing home’s manager.
Findings:
The interviews revealed three themes: ethical issues in practice; relational issues; and organisational issues. No significant differences between registered nurses and healthcare assistants were evident, confirming the patterns emerging from the interviews. Relational issues, primarily issues with residents and families, occurred most frequently and caused greater distress.
Conclusion:
The shared environment is key in the experience of ethical issues; therefore, multidisciplinary education is needed for ethical decision making in palliative care. Addressing staff knowledge and service organisation may reduce ethical issues locally and provide a benchmark for global change.
Introduction
The population of older adults is increasing more rapidly than the total population on a global scale, with most significant increases evident in Europe. 1 Within the United Kingdom, 40% of the population aged 65 and over have a chronic illness, and this increases to 69% in the population aged 85 and over. 2 More older people are living and dying in nursing homes. Between 2006 and 2008, just 12.1% of people died in nursing homes, 3 compared with 20% in 2015. 4 The trend of an ageing population is one that will continue and, due to the increased prevalence of chronic illness and complex comorbidities, result in increased pressure on resources in nursing homes. 5
Generalist palliative care is acknowledged as an appropriate approach to support older people in nursing homes, with referral to external specialist palliative care when appropriate.
6,7
Palliative care is defined as, an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual.
8
Aim
This research aimed to provide a comprehensive understanding of the care provider’s experiences of ethical issues during palliative care provision within nursing homes in the United Kingdom.
Methods
Design
A two-phase, exploratory, sequential, mixed-methods design based on the taxonomy of Creswell and Plano Clark 12 was identified as the most appropriate design to fully address the research aim. Insufficient prior research was available to justify an explanatory design; therefore, it would be inappropriate to conduct the quantitative research first. In addition, the information gained from the qualitative exploration was used to shape the quantitative survey, and therefore the two methods could not run in parallel. The first phase focused on RN and HCA experiences of ethical issues and the second phase focused on understanding the frequency and level of distress reported by RNs and HCAs associated with these issues across Northern Ireland. Data collection for Phases 1 and 2 occurred between December 2014 and November 2015 (Figure 1).
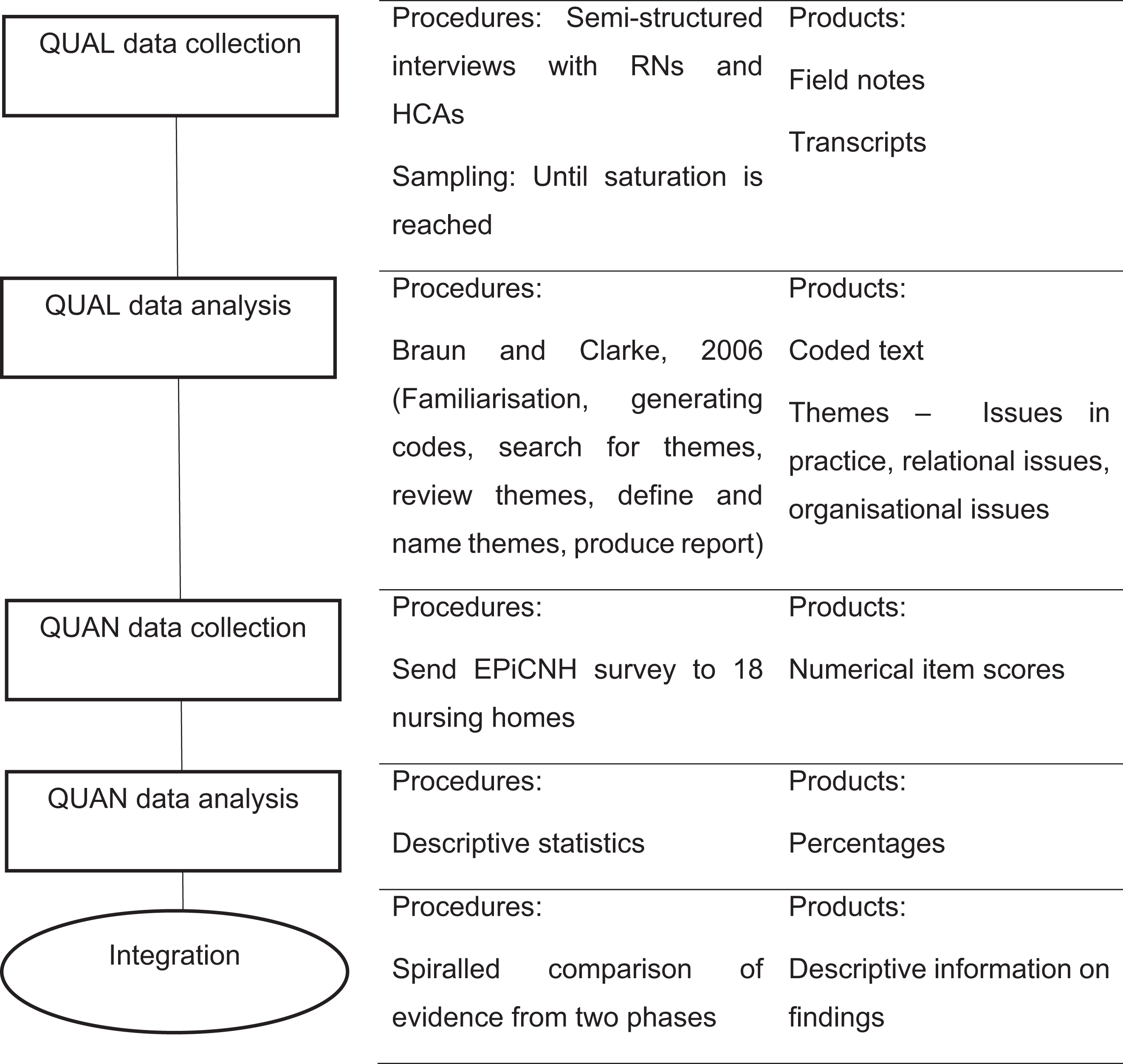
Research design.
Participants
In Phase 1, semi-structured interviews were undertaken with the purposive sample of RNs and HCAs from 13 nursing homes across Northern Ireland who accepted an invitation to participate. Staff were recruited through the provision of an information pack and oral presentation about the study by the researcher. If they were willing to participate, they completed the consent form and the researcher contacted them directly using the provided contact information. Participants were recruited until saturation was reached and no new themes were emerging from the dataset, which was anticipated to be approximately 12 interviews based on the research literature. 13
In Phase 2, a cross-sectional survey was conducted with all RNs and HCAs employed in 18 nursing homes across Northern Ireland who were working on the day of data collection. Based on feedback from Phase 1, the researcher recruited in person at the nursing homes at arranged times, and staff were invited to participate. In the United Kingdom, no data were available to indicate the total number of RNs and HCAs employed in nursing homes, and therefore a power calculation was not possible. To allow for an exploratory factor analysis (EFA) which was conducted as part of the larger study, Costello and Osbourne 14 recommend a sample size of 200. To ensure safe staffing levels, the Regulation and Quality Improvement Authority 15 recommend a ratio of 35% RNs to 65% HCAs; therefore, 70 RNs and 130 HCAs were considered the desired sample size. A convenience sample of 23 nursing homes was approached and 18 responded positively to an invitation to partake. The total number of RNs and HCAs employed per home ranged from 9 to 100 (mean = 33.2, standard deviation (SD) = 24.4).
In both phases, the inclusion criteria were as follows: currently employed in the nursing home as an RN or HCA; over 18 years old; and could provide informed consent.
Data collection
In Phase 1, qualitative, audio-recorded, semi-structured interviews using the critical incident technique 16 were used to ascertain the key ethical issues surrounding palliative care provision within the nursing home setting. An interview guide was developed based on a previous study 17 and pilot tested prior to use. Each participant undertook one interview. Individual interviews were held in a private room within the nursing home and lasted for 11–67 min (median = 30 min).
In Phase 2, a cross-sectional survey was used to assess the frequency and level of distress experienced by RNs and HCAs associated with ethical issues during palliative care provision in the nursing home. The survey was undertaken within the nursing home in which they were employed, located across Northern Ireland. Participants completed the surveys during their shift and returned them to the collection point on the same day.
The ‘Ethical Issues in Palliative Care for Nursing Homes’ (EPiCNH) 18 was used to collect data. The survey was developed through a literature review, interviews with key stakeholders to develop items, face validity testing with an expert panel and pilot testing with the population of interest. The scale consisted of 26 items, scored on two subscales: the Frequency Scale and the Distress Scale (further details on the psychometric properties of the instrument have been previously published 18 ). Participants were asked to rate each item from 0 to 4, with a score of 0 indicating that the item did not occur frequently or cause any level of distress, and a score of 4 indicating high frequency or distress.
Analysis of data
Phase 1 data were stored and managed through NVivo 10 software. And 10% of the audio recordings and transcripts were independently reviewed and analysed by the research team to ensure transcript accuracy and to increase credibility of the interpretation. Interviews were transcribed verbatim and analysed concurrently through thematic analysis. 19 This included a six-step process of familiarisation, generating codes, searching for themes, reviewing themes, defining and naming themes and producing a report.
Survey data (anonymised) were entered and managed using IBM SPSS Statistics v22. Ten percent were checked for transcription errors by a member of the research team (D.M.). Descriptive statistics were used in Phase 2 to summarise what was revealed through the survey and highlight which themes were most prevalent. T-tests were conducted to look for similarities and differences between RNs and HCAs in terms of both frequency and distress.
Validity and reliability
Lincoln and Guba’s 20 framework for trustworthiness and rigour was used to assess credibility. Member checking was conducted to confirm credibility, a thick description was used to improve transferability, dependability was assessed by external audits and reflexivity through a reflexive journal allowed for confirmability of findings. Each team member independently analysed the transcripts, then discussed and agreed codes to confirm inter-rater reliability.
Integration
Following the guidance of Creswell and Plano Clark, 12 integration was undertaken through data transformation and a spiralled comparison within the discussion. The data from Phase 1 were integrated with the literature review and informed the development of the survey instrument utilised in Phase 2. Phase 1 categories linked to items in the survey which allowed the items to be ranked in terms of frequency of occurrence and level of distress associated with the theme. Results were presented in a spiralled comparison, which means that data from Phases 1 and 2 are integrated and then described concurrently.
Ethical considerations
Ethical approval was granted by Queen’s University’s School of Nursing and Midwifery Research Ethics Committee (02.DPreshaw.08.15.M7.V4). All participants were supplied with a participant information sheet which discussed confidentiality, anonymity, disclosure of sensitive information and participant welfare. Written informed consent was obtained prior to participation in the interviews, whereas consent was implied based on the return of the survey. Governance was sought from the manager of each nursing home.
Results
Participant profile
Table 1 portrays the demographic characteristics of the sample who completed the survey, including their work designation, age, gender, education and number of years spent within the nursing home.
Demographic characteristics of participants.

RN: registered nurse; HCA: healthcare assistants; NVQ: National Vocational Qualification; RGN: registered general nurse.
Main findings
The interviews revealed three themes related to ethical issues reported by healthcare providers during palliative care provision: ‘Ethical issues in practice’, ‘Relational ethical issues’ and ‘Organisational ethical issues’. Data from the two phases have been presented in a spiralled comparison (Table 2).
Tabular summary of integration.

SD: standard deviation; PEG: percutaneous endoscopic gastrostomy; HCAs: healthcare assistants; GP: general practitioner.
a Highest scoring items.
Ethical issues in practice
Ethical issues in practice were found when participants experienced conflict between what they felt was right and what was their duty of care. This included respecting human rights, conflicting bioethical principles (autonomy, beneficence, non-maleficence and justice) and nursing ethical principles (fairness, respect of dignity and truthfulness, issues with autonomy due to a lack of advance care planning, and the use of futile or aggressive treatment). The quotes below demonstrate the challenges in being truthful, and conflicting ethical principles of resident autonomy and beneficence: I’m a nurse so I shouldn’t lie to my resident…but sometimes it’s very difficult. (Participant O, RN, p. 4) you do feel you’re going against their wish but at the same time, you need to get washed…or you need to eat, you’re only trying to encourage something for your own good…but you do feel uncomfortable doing it. (Participant L, HCA, p. 5)
Relational ethics
Relational issues focused on the conflicts within the relationships of staff, families and residents including attentiveness to resident care needs, responsiveness to criticism and demands from families and care partners, and concerns about the competence of colleagues. The following quotes demonstrate specific examples of conflict with families over the best interests of the resident and concerns over the compassion of a colleague: I had a family and the mother’s 91, she has dementia and they insisted she was taken off her night sedation with the result of the woman didn’t sleep and was up all night shouting. (Participant B, RN, p. 8) I think her [the nurse’s] manner was sharp and maybe not as sympathetic as she should have been. (Participant A, RN, p. 12)
Organisational ethics
Organisational issues were a consequence of the structure and quality of services available within the nursing home and included distributive justice (resource allocation and quality of services), the organisation of services, particularly the coordination with, and responsiveness of, locum general practitioners (GPs), and staff wellbeing. The quotes below demonstrate the personal struggle with lack of time to get to know the residents, and the quality of services to ensure residents feel like a person and not a number: Sitting with someone and having a chat goes a long way…you just don’t have that time since coming here. (Participant M, RN, p. 5) I don’t believe somebody should feel like a number on a door and to me…that’s the way people are. (Participant L, HCA, p. 7)
Integration of datasets
The data from Phases 1 and 2 were integrated and presented in a spiralled comparison to draw out three key findings. First, relational ethical issues are most distressing to healthcare providers when providing palliative care. Elements include attentiveness, responsibility, competence and responsiveness, and how these can conflict during daily palliative care provision. Examples of this finding include the following: interactions between RNs and HCAs and the families of patients receiving palliative care resulted in frequent ethical issues and a high level of distress; resistance from residents during care provision was very distressing for most healthcare providers; and poor communication between staff was both frequent and distressing. Second, staff training in palliative care is still lacking, but desired by healthcare providers to improve experiences of palliative care provision and reduce ethical issues. Finally, communication to facilitate shared decision making between families and the multidisciplinary team is essential to improve palliative care and reduce ethical issues.
Discussion
The aim of this research was to provide a comprehensive understanding of care providers’ experiences of ethical issues during palliative care provision within nursing homes. The interviews revealed three main themes in which ethical issues could be categorised: ethical issues in practice, relational issues and organisational issues. The EPiCNH survey identified relational ethical issues to be the most frequently occurring, and the most distressing, ethical issues reported by RNs and HCAs. No significant differences between the RN and HCA survey data were evident in both the Frequency Scale and the Distress Scale, which confirmed the patterns emerging from the qualitative interviews. Synthesising the findings from Phases 1 and 2 revealed that the theme of relational issues, primarily issues with residents and with families, was most likely to occur frequently and cause higher levels of distress.
Interpretation of main findings
Decision making to ensure fair and ethical treatment, balancing autonomy, justice, non-maleficence and effective communication to support beneficent care were the most frequently raised issues in practice, highlighting the need to address these areas directly through improved training. Managing the challenging behaviour and negative symptoms, particularly in terms of resisting care, was a clear example of the struggle between balancing justice and non-maleficence. It is also supported by previous studies, for example, Gjerberg et al. 21 found RNs and auxiliary nurses to report ethical dilemmas due to demanding residents who ended up with more resources and breaches in patient autonomy. The conflicting ethical principles of beneficence and autonomy were commonly cited throughout the literature, 22 –24 for example, disagreements between nurses and patients were reported when the best patient outcomes were limited by the patient’s wishes. This research has added to the knowledge base by demonstrating how communication challenges can lead to ethical issues irrespective of the capacity of the resident.
Relational issues were found to be the most frequent and most distressing, setting apart palliative care ethical issues from ethical issues experienced during everyday nursing care. This research added to the evidence base by demonstrating how a lack of family understanding can lead to unrealistic demands within palliative care; however, while openness with the family is important, the resident must remain central to the decision-making process. The influence of family distress on care may suggest a need to include families actively in decision-making processes from the beginning of the care journey. Interacting with family members was found to be a concern for RNs and HCAs in both this study and many previous studies including those by Enes and de Vries, 25 Schaffer 26 and Gjerberg et al. 27 These studies found meeting relative’s needs, interacting with families, communicating about death and disagreements over treatment to be the major ethical issues. Lopez et al. 28,29 identified nurses as feeling ‘in the middle’ of the decision-making processes and ambiguous in terms of their specific role as they wished to create a plan that was acceptable to the GP, the family and the patient. Trying to satisfy everyone within the decision-making process was identified by nurses as a concern in this study; however, HCAs previously reported getting on with the job instead of involving themselves in decision making. 30
Lack of staff and problems with GP involvement were highlighted as the main organisational ethical issues, indicating a need to increase resources and improve coordination of GP care within nursing homes. Many issues involving the GP were reported within the literature. Dreyer et al. 31 found that homes with only one GP visit per week also had limited coordination of care, and Enes and de Vries 25 found lack of GP knowledge of symptom control to be an ethical issue. Involving GPs in nursing home care proved challenging for participants both in this study and in Schaffer’s 26 study, where difficulty contacting GPs was one of the most frequently occurring ethical problems. While restraint was commonly found as an ethical issue throughout the literature, 11 it was not identified by participants in this research. This could be caused by a lack of understanding of restraint and how it may conflict with a person’s right to freedom, or it could be a result of better management and use of restraint.
Strengths and limitations
The main strengths of this research include the rigorous pilot testing of the interview schedule and the survey instrument prior to use; team collaboration throughout the analysis process and the practical element of a mixed-methods approach which resulted in clear and direct messages for service improvement. Limitations have also been recognised. This study was only conducted in one part of the United Kingdom, limiting its wider application. The challenges of researching ethical issues which have previously been poorly defined, and the recognition that nursing homes who are willing to participate in research may be systematically different to those who are unwilling to participate in research may limit the applicability of findings across all nursing homes.
What this study adds
The key implications for policy include the need for inclusion of ethical decision making within palliative care education and support for the United Kingdom Clinical Ethics Network’s (UKCEN) argument 32 that it is time for formal recognition of clinical ethical committees, with the services of such committees made available to nursing homes. This recommendation has global implications for palliative care provision, linking to the World Health Organization’s (WHO) 33 acknowledgement of the need for training and debate on the ethical aspects of a range of issues for those receiving palliative care.
The overwhelming similarities between RNs and HCAs highlight the importance of the shared environment in the experience of ethical issues. The key implications for practice include the need for multidisciplinary training and support for RNs and HCAs who are struggling to build strong networks with residents, families or colleagues, and a means of incentivising training in palliative care to help overcome common ethical issues. Training staff to take account of patient and family values and incorporate this into decision making has been recognised by the WHO 33 as a means of addressing important ethical issues. Distribution of knowledge in ethical decision making in palliative care may be achieved by support of local knowledge transfer projects which are less expensive to run and accessible remotely, for example, Project Extension for Community Health Outcomes (ECHO). ECHO is an evidence-based telementoring intervention that connects primary care providers with expert teams of specialist providers via regularly scheduled videoconference. 34 In addition, the implementation of strategies to strengthen and organise services, access and referral systems that are fully integrated across healthcare delivery would address many sources of ethical issues raised in this research.
Future research may consider exploring how to develop a multidisciplinary approach to palliative care education and ethical decision making, why training in palliative care is unattended and evaluating patterns of usage to search for methods of improving attendance. In addition, researchers should seek to understand the family’s perspective when engaging with nursing homes, including the development of family-friendly strategies to increase the likelihood of families engaging in care decisions.
Conclusion
This research has identified the ethical issues reported by RNs and HCAs during palliative care provision in the nursing home. Relational ethical issues were most distressing to healthcare providers when providing palliative care, in particular, poor staff communication and its impact on the quality of care for residents. The shared environment is key in the experience of ethical issues; therefore, multidisciplinary education, with managerial support, is needed for ethical decision making in palliative care. Addressing staff knowledge links to global policies on training in ethical debate for palliative care and may be achieved by transferring knowledge and specialist skills through mechanisms such as Project ECHO. Integration of nursing home services with specialist palliative care services should be a priority for research and policymaking nationally and internationally, due to its impact on ethical issues and quality of care provision.
Supplemental material
Supplementary_File - Ethical issues experienced during palliative care provision in nursing homes
Supplementary_File for Ethical issues experienced during palliative care provision in nursing homes by Deborah HL Muldrew (née Preshaw), Dorry McLaughlin and Kevin Brazil in Nursing Ethics
Footnotes
Acknowledgements
D.H.L.M., D.M. and K.B. made substantial contributions to the design of the work, the acquisition, analysis and interpretation of data, revised the manuscript and approved the final version to be published.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by a student scholarship from Queen’s University, Belfast.
Supplemental material
Additional information relating to the project can be accessed by contacting the corresponding author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.