
Abstract
Background:
Education can be taken as a key factor in transmission of a value tradition in healthcare. In professional and educational contexts, transmission of values appears to be a kind of guarantee for an occupational group’s professional identity, awareness and ethical integrity. Given the positives of such transmission of value traditions, one can also pay attention to conflicts between the professional tradition and individuals who are brought into that tradition.
Objectives:
How does mediation of value tradition in healthcare education appear out of the students’ perspective based on their own narratives?
Research design and participants:
Students’ texts were analysed through a combination of contrastive discourse analysis and sociohistorical description and then evaluated from an ethical perspective. Data were collected from the annual electronic feedback given by students after their clinical practice at a University Hospital.
Ethical considerations:
Organizational approval was received. Information about the voluntary nature of participation was a part of the feedback tool.
Findings:
The analysis points to the fact that there is a definite theme in the students’ experiences that both the previous research has neglected and that stands in conflict with the current tradition of healthcare education in Finland. That theme can be summarized in the experience of ‘losing one’s identity’, and it is expressed in a request to experience of ‘losing one’s identity’ and it is expressed in a request to have a right to ‘use one’s own name’ also as a healthcare professional.
Discussion and conclusion:
Being addressed by one’s name is to make the person directly involved and responsible, realizing that that person’s perspective is of importance to the way the world is. We argue that this theme (my name) is of ethical importance and could have empowering potentiality when used in an ethically sound way.
An ethical analysis of nursing students’ right to use their name
Introduction and preliminary research question
It has become increasingly common to emphasize the importance of qualitatively performed work in many occupational categories or groups. They can be explicitly expressed in formulated regulations, regulations and occupational rules. In short, certain ethical principles and rules that a professional group collectively believe should characterize the work efforts. They can also be expressed more implicitly in the form of a vocational tradition. The Swedish ethicist Göran Lantz emphasizes, for example, that a vocational profession collects and organizes ethical experiences conveyed through formal education as well as practical models from one professional generation to the next. 1
The starting point – whether explicit or implicit – is both normative and informative in its nature: a professional working person in a specific profession should engage in and relate to his professional activity in a specific way. Transmission of a value-based tradition serves as a kind of guarantee for a professional occupational group’s identity, awareness and ethical integrity.
In the actual transmission of values within a tradition, two poles meet, to state it very simplistically. On one hand, there is the very element of tradition, which is essentially given in the encounter with a given professional tradition. Entering a given internship or practice is not to begin in a vacuum that you can individually dictate. Rather, it is the tradition’s inseparable base for values and its historical appeal that gives the contours of what happens in a practice.
However, there is another side of this coin, namely, the individual or individuals who, in terms of their own life experiences, expectations, dreams, ethical intuitions and ideals, encounter a given professional tradition. The personal-self meets the professional self on its way to a professional identity. 2 The encounter between personal-self and professional self happens continuously, for example, in professional situations when new students start their studies and are introduced to the professional tradition they have chosen to start studying.
Both the explicit and the implicit norms, expectations and professional ideals are constantly included in both studies and in periods in a clinical learning environment 3 included in the studies, as in healthcare studies.
In this article, we focus on this kind of meeting between a professional tradition and individuals encountering the tradition. More specifically, we are interested in paying attention to how this encounter appears from the point of view of healthcare students, who not yet have been incorporated into the specific value tradition, that is, from the perspective that encounters with power and authority. Transmission of a value tradition can, of course, be expressed in different ways. Two possibilities appear immediately: either the conceptualization is formulated so that the power and control dimension is emphasized or it is formulated with greater emphasis on the formability and variability of tradition. Whatever perspective is more emphasized, the balance of these possibilities is of interest.
The occupational tradition we use as the starting point of this study is the healthcare tradition in Finland, as expressed in a certain context, namely, in some aspects of nursing education. The exchange of values that takes place in this care education is part of the transformation of novices into professional nurses and thus a very interesting context to study for this purpose. Especially, the views of these novices and their encounter with the authoritative tradition are of great interest in this article.
To properly focus on it, we have chosen not to focus on nursing education as such, but only on a very specific part of the education, namely, its time spent in clinical learning environment and the students’ experiences of these. Clinical placements are considered an important mean in the students’ journey in becoming a professional nurse. 2 These mandatory periods constitute a large part of the studies, as at least 60 ECTS must be done in clinical practice both in primary and specialist care, as clinical practice. 4 An average student in nursing spend much more hours in clinical environments than in classroom during their education. 3,5
Since clinical learning environment in nursing education appears to be the most suitable intersection of the transmission of value tradition in a practical setting within nursing education, we have chosen to take our starting point here. The preliminary research question that this article deals with can be formulated as follows: How does mediation of value tradition in health education appear out of the students’ perspective, based on their own experiences? The question is far too wide and not specific enough, but before we specify it, we need to say something about both the material and the methods we utilize in this endeavour. The initial research question is sufficiently specific for both material and methods to be presented.
Materials, methods and detailed research assignment
Our study is based on empirical materials made available in connection with practical training periods performed at a University Hospital. The various University clinics have approximately 3000 healthcare students per year, who all do their mandatory supervised clinical practice. Since teaching and supervision is a central part of the university hospital’s task, it is important to develop this part of the University Hospitals field of work. To develop the learning environment of clinical practice, the University hospital has used the same electronic feedback tool Questback for the last 10 years. The Questback feedback tool starts with a letter that informs the students that it is voluntary to give feedback and that feedback is given anonymously.
The letter also informs the students that the feedback is used for development of clinical practice at the Hospital and for research purposes. It is considered that giving feedback after reading the letter means that the student also gives permission to use the feedback for research purposes.
This Questback measuring instrument is a survey-based tool with a total of 51 questions. In addition to the survey, there is an opportunity to give response in an open question. This open question reads, ‘What else would you like to tell me about your completed clinical period of practice?’ The open answers are ‘unused’, so far, no research has been conducted, at the University Hospital, based on these open answers.
This article focuses primarily on the answers formulated within this open question. We deliberately choose this entrance to underline the students’ perspective and how the meeting with the healthcare’s value tradition is shaping those who meet this tradition. The fixed questions in the survey part, based on our initial theoretical input, are seen as the perspective of the current tradition. We know from a previous study that healthcare students did not criticize the codification of ethics based on the current, established tradition when studied utilized by surveys. 6 We also know from another study that nursing students experience ethically difficult situations during their time in clinical learning environment. 7 We also know from others studies that about one-fifth of healthcare students review the supervision during clinical practice as a failure 8 and a lot of studies stating that negative experiences in clinical learning environment interfere with learning outcomes from the education in general. 9 –12 But none of these studies explored the possibility of using the students’ negative experiences as potential critic in lack of empowerment or as potential sources for engagement in unjustified value transmissions within the healthcare tradition.
The material for this article is based on the answers from 2012. The material consists of 1357 texts written by students at the end of a practical placement at the University Hospital, which means that c. 67% of students that year took advantage of the opportunity to communicate their experiences outside the survey questions. The texts are of different lengths, ranging from a few words to a page’s (A4) investigations. The texts are written in a specific situation of students who do a work, the supervised hospital practice, which is evaluated by someone else.
Methodically, the analysis is primarily inspired by a discourse analysis Malin Wreder implemented in her study on care of older people in Sweden. 13 The analysis is made initially in four steps: (1) identification of the characters in which the texts are centred around, (2) identification of previous research as statements dealing with the same characters, (3) description of the discourses that appears by locating so-called “nodal points” and “floating significants” in how the whole is constructed by different elements and (4) analysis of how the discourses that occur either include or exclude different effects. 14
This way of carrying out discourse analysis leaves us empty-handed in two regards. The first is the actual context in which these texts are included. Because transmission of a value tradition of care is the focus of this article, we need to add an aspect that relates to the social–historical context, in this case, the relevant social imaginary of the value tradition within the nursing profession. 15,16 The second aspect concerns the explicit power-critical and empowering perspective that is central to our study. We choose to deal with these shortcomings by making a specification of point 2 in Wreder’s analysis model, namely, that we primarily care about and seek discourse-bearing themes in the texts that previous research has not considered or totally missed, that is, themes that have not previously been noted in scholarly discussions on challenges to be addressed in the nursing tradition or the needs to adjust or renegotiate the “authoritative weight” of the tradition.
Now, we can pinpoint our issue into a more distinct research task making both the power-critical and sociohistorical perspective become fully visible. The task is divided into three interlinked questions: What kinds of the discourses appear in the healthcare students’ open texts, in relation to different value-based topics found in the metre questionnaire part? Is there in previous research gaps or deficiencies which have de-visualized central and ethically relevant experiences that the students express after the supervised clinical practice? Is it possible to find support for the students experiences in the sociohistorical context (vocational culture, value tradition) or can these experiences be perceived as elements for a power-critical and empowering perspective that can challenge the given value tradition in healthcare education and practice?
To handle our research assignment, the analysis of the concrete material has been done as follows. First, all 1357 texts of the students were read carefully (1), and the texts containing some characters, nodal points and floating significants about value-based themes were identified (2). 14,15 The result gave 350 texts of this kind. Thereafter, a literature search was made based on the students' central discourses (3). The student nodes’ nodal points then constituted the keywords in the further search (4). Methodically, one could talk about contrast analysis, where student-discourses are the starting point. If we identify such themes, the following step is to reflect these against the social–historical context (5). Finally, we evaluate and discuss the result we get through this analysis in order to deal with the normative aspect we consciously sought for.
Concrete analysis and results
Students’ discourses – I was met as a person
The texts are generally well written. The shortest consists of a few words and the longest is one side (A4). The longer texts are stories with an introduction, an event or events and then an ending. All longer texts treat negative experiences, in one way or the other, but there are also some short texts treating negative experiences
All texts that contained characters (words and sentences) that concerned a value-based theme, such as the value base of care, treating students, equality and individuality were highlighted. At the next stage, each statement was read carefully to detect common signs, nodal points and fluctuating significances. At this point, it is already possible to spot some outlines of what is included in the discourses and what is left outside. Texts in which similar discourses and characters were detected were arranged in groups, after which each coded group was read separately. Central signs in student discourses were the department’s good atmosphere, ‘I was met as a person and was taken seriously’. In a poor practical placement environment, no supervision is given, and in this context, students discuss a lot about how to be treated as students. These signs are seen in most of the student discourses. The characters ‘me’, ‘mine’ and ‘like a person’ often appeared. The right to their own identity and to be treated as an individual, and not just as a student in the crowd, are central content in student texts.
The largest student discourse therefore circles around the unit’s working environment. Frequent recurring signs here are bullying, equality and being part of the team. Students make demands, want to get responses to their actions and want responsibility. The negative experiences are built around characters as staff lie, ridicule and scream at students. Probations of humiliation, and fear of being humiliated, occur at regular intervals.
The nodal points and interrelationships of the student discourse are presented in Figure 1. In Figure 1, the symbols show how closely each students’ discourses are. There are many arrows between the different symbols, that is, a discourse affects the following. One and the same student can participate in multiple discourses in his text. Green symbols belong to the good experience, while grey and red represent the bad experience. The blue, ‘meet as a person’ and ‘treat others’, exist both in the good and in the bad experiences. ‘Use my name’ is a red discourse, which may also occur in an otherwise good environment, but where students are addressed by the word student and not by their own names. The hierarchy discourse is always a negative discourse. The sign appeared both as part of another discourse, but also as a separate discourse. The words ‘hierarchy’, ‘proudly’ and ‘astonishment’ are included in the smallest discourse, and are also important nodal points, as they give a special meaning to the discourses they are part of. ‘Hierarchy’ the character describes something old-fashioned, ‘despite this’ is a negative experience turned into a positive, and the ‘amazement’ is always something positive, as in a positive surprise that you are treated well, which, of course, says something about the expectations the students had.

Students discourses – I was met like a person.
Scholar’s discourses – solutions and tools
Once the characters and nodal points in the student texts had been identified, a new research search was made with the themes presented by students in their texts. Since the students’ discourses were so many, it was not possible to make systematic article searches for all discourse groups within the framework of this work. Instead, the search identified scholarly key articles for the most central discourses. These were sought for on following criteria: Search terms used were practice placement*, nursing student* in combination with key moments from the different discourses. For example, individual * and valued * can be mentioned. The search had the limits that the articles should be in their entirety in digital form and be written in English. The articles should also be available for free. The search was done both through different search bases and manually. The search began in search databases CINAHL, EBSCO and Google Scholar. Most of these searches gave a few hits, usually between 5 and 30 items, but there were also discourses that did not get a single hit or just 1. Since the headlines do not always tell exactly what the content of the article is, all of them are read in the next stage. After the abstract reading, the articles that addressed the research area were chosen. Read the articles of the selected articles to find new articles and possible other literature.
The original search based on the mentioned criteria gave us a total of 26 academic, scholarly articles. Later, five more articles were found.
One and the same article can deal with both the students’ negative and positive experiences during the clinical placement. Researchers often start from the negative and go against the positive ones. Several of the researchers are looking for tools that students and teachers could use to relieve the effects of negative experiences.
All researchers agree that practice is an important part of the studies. Sandvik’s Finnish–Swedish research group states that ‘clinical studies are important for preparing the student for the professional career role’. 17 One article takes the point even further stating, “The clinical component of the undergraduate nursing degree is viewed by many as the most central element of nursing curricula”. 18 The practical part is thus seen as the most central part of the whole Nursing Education Study Plan. All articles read for our study, written by teachers in nursing education, have the same fundamental attitude. At the same time, as many also pay attention to is that the clinical practice section is often the most expensive section of nursing education. 18 This may be one reason why the teachers discuss the negative experiences more than the positive ones. Earlier research has also shown that negative experiences are one of the reasons why students interrupt their studies (“exit”). 10
Figure 2 presents the discourse’s different nodal points, as well as their mutual relationships. Each symbol represents a discourse identified in the articles. Central to these discourses is to find solutions and tools that could make it easier for students during the practice. The researchers are aware that bullying and invisibility occur, and attempts are made to make students visible, by giving students knowledge, voice and inviting them to participate. In this figure of discourse, there are only a few dashes between discourses, which is because research discourses are usually ‘loose’, that is to say, each research team discusses its research and only one theme or project at a time.
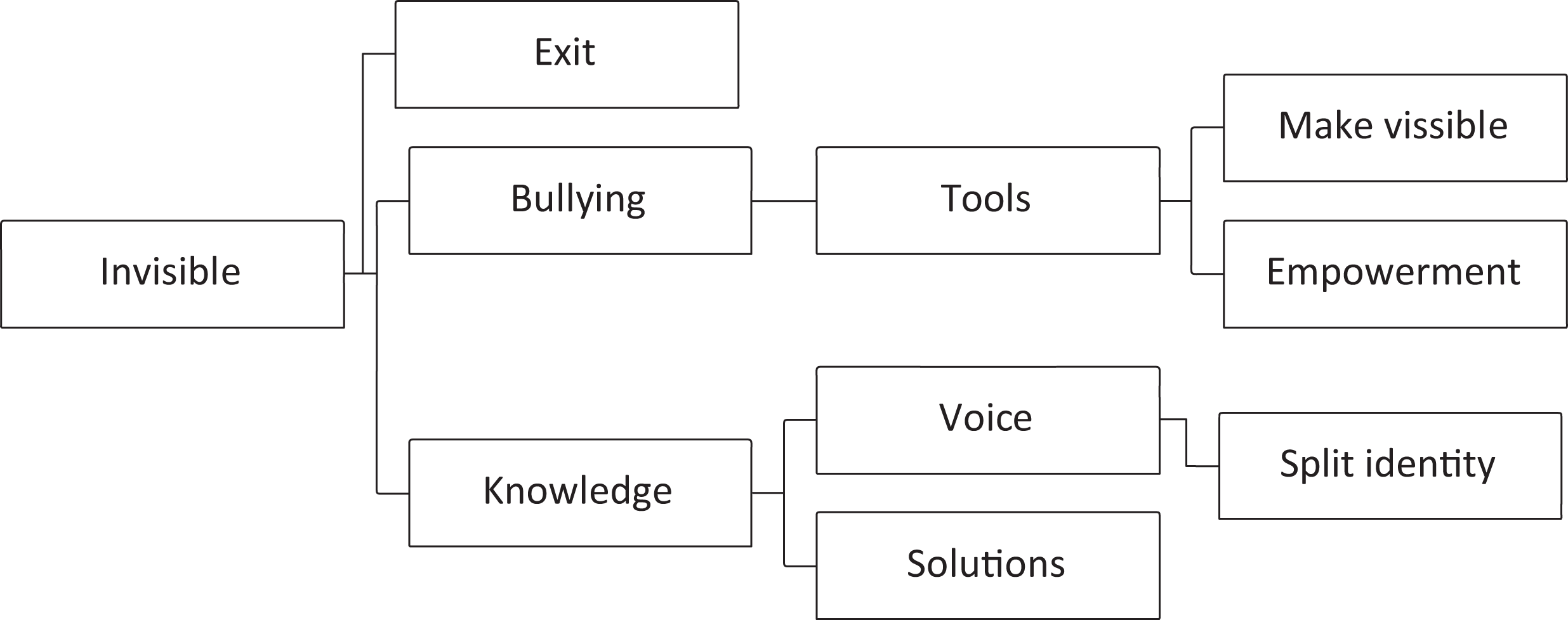
Scholars discourses – tools and solutions.
Today’s students can enter their nursing studies with many personal identities, as this student says, ‘I work, I’m a mum, I run a household, you know, there are more things in life than just my study’. 19 But today’s researchers don’t discuss this personal-self, it is only a small discourse which has only one weak link to the other discourses. 2,11,20 –23
Looking at the whole picture in the scholarly discourse, one can note the following results: it is divided into successful and failed supervisory experiences. A key nodal point in the successful experience is to evaluate students as students and as individuals. Another central node point is belonging to a team. As part of the team you will be heard and seen, you have a voice and are given the opportunity to participate. However, when turning to unsuccessful experiences, it is noteworthy how similar the bad experiences are, regardless of where they happen. Nodal points seen here are an invisible student, bullying and risk of exit. The scholars discourse show a pattern of offering different tools, such as providing different kinds of knowledge and efforts in giving students a voice of their own. Empowerment in the form of co-acting and visualization are also important themes in the scholar’s discourse. 24,25
Results
Approaching the both discourses from a contrastive angle, asking what is included or excluded in the respective discourses, our material show that students and scholars include and exclude different topics or themes in the discourses. At this point, it is important to look into whether there is power-critical potential in the difference that occurs and whether it can be considered ethically justifiable.
In a good atmosphere, students are supervised by everyone, patients are at the centre of work and the hierarchy does not interfere with the work. In the bad practice experience, the hierarchy is clearly visible at work, unequality is clearly marked between different staff groups, and students feel completely invisible and experience threats of reprisals. Both these findings are of interest on a general level of studying ethics in healthcare education. As pointed out by Chris Gastmans, the real contextual space for ethical experiences do not occur in a vacuum, and they take place in an institutional setting: “the position of power(lessness) between doctors and nurses, the working relationship within the team and the hospital, the relationship between nurses and hospital directors, etc. These contextual factors influence greatly the questions asked (or not), the problems signalled (or not), the solutions proposed (or not)”.
26
Students assume that they are entitled to supervision and see it both as an ethical and a legal problem when they feel they do not get it. Students have a very strong desire to be ‘myself with my own personality’ and with ‘my own name’ in an equal relationship during hospital practice.
Students’ discourses concern issues dealt and felt within the clinical placement and exclude almost anything outside of this world. If one puts the figures with the students’ and scholar’s discourses next to each other, one very soon notices that the students’ discourse figure completely lacks the nodal point of knowledge. No student requests additional knowledge in his or her texts. Requesting more or supplementary theoretical knowledge during the supervised hospital practice is a non-existent discourse in the student world in this research.
The scholar’s course addresses the challenges that emerge with developing tools for the students so that they can handle their problems during the supervised practice. In these tools, the desire for more knowledge is brought to light, to make students visible and to give them a voice. What is completely excluded is what the students discuss the most, identity as a right. The right to be addressed with your own name is completely absent.
Exactly here, at this point, we find the locus we in this study set as a goal to search for. It appears with the experience of losing one’s identity and that one is forced to ‘adopt’ a new identity during the supervised clinical practice. It is in this locus that the students make moral demands on their practical experiences which the scholar’s discourse does not answer at all. It is a moral demand rising from the contextual setting of power relations within the place of the practice.
Interestingly, most of the negative experiences of clinical practice, nodal point’s hierarchy, downgrading and invisibility can be summarized relatively easily in the students’ desire for identity as a right, almost explicitly expressed in the desire for the right to be called with their own name. The question of right to name is thus the question that becomes a partial result of our study. The following questions will thus be discussed further: (1) how is the right to name addressed in the sociohistorical context and (2) is this desire for the right to one’s own name ethically justifiable as a stance of combined empowerment and power-criticism?
The sociohistorical context
On the discovery that the request for identity as an ethical request, as a right to be addressed by one’s own name, it is worth looking at the sociohistorical context of healthcare education. Already a brief insight into that context points out an interesting contrast to the issue in our study.
The oldest Hospital of today’s University hospital started a school for nurses in 1889. 27 The School had a strong connection to the tradition of Florence Nightingale. In 1904, a head nurse was employed at the hospital and she was also a director of the nursing school. This head nurse had been educated at a Florence Nightingale School in Great-Britain. Nightingale School’s principles were strongly influencing the education and practice at the old Hospital, and of today’s University Hospital, but also nursing education overall in our country.
According to Sioban Nelson, the inheritance of Nightingale is very distinct. In the Nightingale School, the first and most important is always the well-being of the patient. A good nurse was a virtuous woman who knows her place and is obedient without questioning her superiors. You are formed and transformed into a good nurse through a combination of theoretical and practical education including supervision along with the goal of transforming your character. 28
In the textbook that was used at the early nursing education in our country, Textbook for Nurses (1912), there is an interesting chapter entitled ‘Conditions for prospective nurses. ‘In this chapter, one may find that the main reason to apply for a nursing education should be a burning desire to help those suffering. The central message is on the nurse’s task is love to our suffering neighbour. 29 A good nurse should also be able to follow orders and develop her mind to better fit this profession. It is also suggested that you should not apply to this profession if you have difficulties to comply with rules. A general feature of this textbook is that the individual nurses are part of a nursing community, which is located within hospitals, nationally and internationally. One is not trained to “I am the nurse”, but to “I belong to the community of nurses”. This is so central that the chapter ends with the call: one for all and all for one. 30
For Nightingale, the nursing profession was a religiously motivated vocation and calling. 31 Within the Nightingale School’s tradition, the calling had a central role all the way up till the 1950s. 32,33 The religious undertones of the vocation in this tradition are clear and, according to Åsa Andersson, return to the roots found in Martin Luther’s view of the calling and the woman’s place at work and home in the 16th century. 34 A central aspect of the Lutheran vocation is its focus on serving your neighbour. The purpose of the work is only to serve the weak. In this sense, one should also be prepared to sacrifice one’s own good for the sake of others. 35 It is a distinct form of love that sharply diminishes the subject of action for the benefit of the addressee, a thought which, in the tradition of theology, goes under the concept of “agape” – the love of self-giving. 36
The interesting question therefore is how the issue of naming is to be understood in the context of this tradition of vocational thinking. Among the nurses who preceded the Nightingale tradition, both names and name changes are discussed. Urs Heim argues that the monasteries and diaconate institutions have had different approaches regarding the name. Originally, the new novice in the monastery was always given a new first name at the entrance to the monastery, as a sign that a new stage of life had begun. One appealed to each other with a ‘You’ and the monastery name. Nuns in hospitals were addressed with ‘Sister’ and surname. The deacons kept their civic first names, and one could use ‘you’ with each other as you got to know each other better. Heim writes that in today’s monasteries, a nun is allowed to keep her name if she so wishes and that addressing each other’s with ‘you’ have increased within the monasteries just like in the rest of society. 37 A Finnish Diakonia Centre, founded in 1867, 38 used the same name praxis as Heim describes. One is addressed with the word “Sister” and the person’s first name.
Florence Nightingale herself discussed the issue of naming. Sorvettula emphasizes that Nightingale pointed out that a new nurse should be addressed with her department’s name, for example, ‘sister George’, and eventually the name of the department would completely replace the nurse’s name. Nightingale gives an example; a new nurse is appealed to as ‘department George’s Sister’, then ‘Sister George’ and finally addressing the nurse only with the department’s name ‘George’. She loses her own name and she becomes the department. 39
In England, some departments still have personal names and no numbers as it is in Finland. Eva Lückes expresses the ideology of namelessness and service very concrete in 1898 in the book General Nursing: ‘The noblest service comes from nameless hands’. 40 Lückes looks at the nurse as a servant who works best when she is nameless. She clearly follows Miss Nightingale’s thinking. This tradition was not only something that the teachers in the education maintained. If you go to the contemporary Finnish journal of those days, “Epione”, the healthcare workers own magazine, one will also find similar examples of how healthcare practitioners discuss the use of names. 41
Discussion and ethical reasoning
The short tour into this sociohistorical context gives a clear picture of the value tradition conveyed in health education and its clinical practice. For a younger generation of healthcare students, this tradition of communication is expressed as a conflict in our primary material. One can discuss this conflict as an issue of different generations. From the perspective of generational research, it can be noted that for the younger generations, there is a larger space between the professional and the personal-self. The personal aspects, ‘personal me’ as Saarikoski writs, cannot be completely excluded when joining a professional role. 2,42,43 According to this research, a conflict between one’s own values and one’s working values gives a high risk of work-related stress and burnout. There is an interesting study, given the purpose in this study that highlights the core issue. Rognstad et al. conducted a study of Norwegian health students’ values and attitudes in care. An interesting tension appeared. On one hand, the students want to help others and they are keen on doing it. On the other hand, their world of experience is at the same time characterized by a strong need for positive response and of being able to develop themselves. If they do not get a positive response, this directly affects the actual effort. If the feedback fails, the students do not feel themselves valued and recognized, and therefore, the work effort declines: They only do the most necessary tasks, but do not get involved personally or take their healthcare responsibility seriously. 44
Seeing this conflict as a generational question reveals for some insights, but it does not allow for going into depth on the conflict between the personal and the professional. The generation perspective points to differences in evaluative horizons and what is taken as granted, but the conflict we reported in our analysis is not about the students’ right to own personal values, but the right to own identity and equal treatment. The healthcare students in our material do not question the value tradition of care per se, but some forms of expression for it. They want to care and help, but they do not understand why this necessarily implies the invisibility of them as individuals, the ‘personal me’. They raise severe questions on the pure functionality as a basic model in the health-care’s socio-cultural tradition. This idea of pure functionality is against all that the core values in nursing is all about, its ‘intersubjective, dialogic character’, as called upon by Chris Gastmans. 45
To get a more nuanced reasoning on the specific conflict, we are using a fundamental distinction put forward by Lawrence Blum between ‘role’ and ‘vocation’ in terms of understanding a career role. 46 The idea is simply that if you have a specific occupation, you also have the professional responsibility that this position entails. Everyone who has such a role is faced with similar expectations and duties. The actual purpose of the distinction is to point out that a person’s relation to his or her career may be external in the sense that the occupational role of the expectations and duties does not need to be more closely related to the person who enters an occupational role. A career role thus becomes easily functionally oriented – and impersonal. The concept of “vocation” comes closer to what the students in our material are looking for, namely, that a professional ethic should also be able to include the personal. Blum argues that vocation is characterized by the person being able to identify him- or herself with the values, norms, ideals and traditions that in a deeper sense carry the distinct occupational image. The characteristic of understanding something like a vocal culture is, according to Blum, that there is a given interaction between the values, norms, ideals and traditions within an occupational setting, on one hand, and the individual’s personal ethical values and sensitivity, on the other hand, an interaction that drives a person in a vocation to personally (and voluntarily) identify him- or herself with the ethical ideal of the profession (“role ideals”). 47
An important emphasis in this idea of interaction between the individual professional and the occupational context is a two-way street: what a person in a vocal culture perceives as ethical requirements in the profession and how the response to these is articulated in turn depends on the personal ethical values and the personal sensibility, integrity, judgement and so on. 48 Blum’s reasoning points epistemologically toward “personal knowledge” in the tradition of Polanyi, a form of knowledge that “mediates between tradition and subjectivity”, 49 and ethically toward utilizing virtue ethics within professional ethics. 50
The central emphasis of Blum is the interaction between the traditional and the personal in the idea of the vocation. It in turn requires that the personal must be able to ‘talk with’ or ‘identify with’ the professional, thus creating a ‘professional conscience’. 51 However, unlike the Nightingale School’s emphasis on the total subordination of the personality under the professional tradition and its teleology, Blum’s emphasis on interaction provides a clear space for the personality to contribute to and critically evaluate the expression and practice of the professional tradition. A transmission of values that only repeats past-term expressions and praxis does not meet the standard of justified interaction. One cannot, thus, create a conceptual space for ‘a living, dynamic tradition’. Rather, the result is an agency that does not seek response but only subordination.
In this light, it is highly reasonable to perceive the students’ demands to be treated equally in the clinical practice of care as a requirement, in which a central aspect of the personal – one’s own name – is not made invisible, as a legitimate criticism of power. We cannot see that a desire to not be structurally and systematically invisible would jeopardize the core values of the healthcare of tradition or the diligence of vocational skills in any way. On the contrary, the ideal of functional anonymity refuses to call out a vocation for a person, if the only action needed is from nameless hands. Our suggestion is also in line with studies revealing that students perform better when they can feel ‘belongingness’, that is, when they are recognized as part of the healthcare team. 3,9,52
Upon that, the ideal of pure functionality has a moral dilemma that needs to be addressed. Criticism of the pure functionality can easily be formulated based on Kant’s ethical reasoning, and especially from his formulation of the so-called ‘Human dignity principle’ which states, among other aspects, that a human can never be used solely as a means but must be understood as an end in itself. 53,54 At the same time, there is reason to note the explicit wording that a person should never be used solely as a means. Such an emphasis opens for another important nuance, maybe the most important one. The emphasis underlines that humans are always familiar with different kinds of dependencies, structures, hierarchies and power relations, but in these contexts one should think of a limit in which a person is never completely determined in functional terms. These power structures are the real context for ethical practice. A person who is fully defined in terms of functionality, how legitimate such use of human capacities may be (i.e. as labour of a company, as lover or a loved one regarding another’s intimate needs or as healthcare provider in a hospital), is an extinct, utilized and reified person. It is a person who is completely open to any kind of misuse of power, even if it’s done in the name of care, good or love.
No one can live his or her life without occasionally use another person as a mean, but Kant’s ethical principle reminds us that we can not only relate in that way to other people if we want to respect the morality built into the notion of human autonomy. After all, the only demand worth both respecting and striving for is a positive evaluation of human autonomy, since autonomy is a basic condition for a person to be voluntarily involved (in a tradition) or in care or love (in a relationship).
Rather, the argument can be stated in a different way. Being addressed by one’s name is to make the person directly involved and responsible, realizing that that person’s perspective is of importance to the way the world is. A pregnant expression of ethically sound nuance of being named as stated by the famous writer Tove Jansson. In Tales from the Moominvalley (1962), 55 more specifically, in the first story “The Spring Tune”, Jansson tells of how the little creep Teety-woo gets his name. Before he got his name, he was a restless little creep. When he got his name from Snufkin everything gets a meaning, Teety-woo say Now I’m a person, and everything that happening means something. Because it doesn’t only happen, it happens to me, Teety-woo. And Teety-woo may think this or think that about it, as the case may be – if you understand what I mean?
Conclusion
In the healthcare students’ experiences of clinical learning environments, there are elements that have empowering potential and should be utilized in rehabilitation of certain practices within both healthcare education and practices within clinical learning environments. In our view, the right to be addressed with one’s own name is ethically justifiable and does not jeopardize the core values of the healthcare of tradition or the diligence of vocational skills in any way. Rather, the healthcare tradition’s tacit invitation for a person to be a pure function of care is risking the personal involvement in care acting.
Limitations of the study
The empirical material is limited to a specific clinical learning environment and the sample is only from 1 year. In order to recognize a more solid pattern within this environment, a longitudinal study would be needed. The conclusion is also applicable only to healthcare educations with strong connections to the lived reality of the tradition of Florence Nightingale. Whether our findings also are applicable in other healthcare value traditions in other countries are to be seen in future studies.
Research ethical concerns
Principles of research ethics were observed throughout the study. According to Finnish law, this type of research does not need approval from an official research ethics committee. 56 The permission to use the material is granted by the Hospital District, and it was received in December 2013. Our ethics committees deals with research permissions regarding patient research (Finnish law). That’s why the Hospital District gives permissions for “non patient research.”
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.