
Abstract
Background:
Nurses’ service behaviors have critical implications for hospitals. However, few studies had adequate ethical considerations of service behaviors and accounted for how organizational or individual antecedents can induce nurses to engage in service behaviors. In addition, they mainly focused on the one side of role-prescribed or extra-role service behavior.
Objective:
This study aims to explore the chained mediation effect of ethical climate and moral sensitivity on the relationship between organizational ethical leadership and nurses’ service behaviors and to examine the relationship, from a comparative view, of the role-prescribed service behavior and extra-role service behavior.
Methods:
In all, 476 nurses from three tertiary hospitals were investigated with the Ethical Leadership Scale, Ethical Climate Scale, Moral Sensitivity Questionnaire and Service Behavior Questionnaire. Structural equation modeling was adopted to analyze the data. SPSS and Mplus statistical software was used in the data analysis.
Ethical considerations:
Approval was obtained from the Ethics Committee at School of Nursing, Hebei Medical University. Data privacy and confidentiality were maintained and assured by obtaining subjects’ informed consent to participate in the research before data collection.
Results:
The effects of ethical leadership on nurses’ service behaviors are mediated by two variables in turn: ethical climate and nurses’ moral sensitivity. Ethical climate and moral sensitivity partially mediated the relationship between ethical leadership and nurses’ role-prescribed service behavior and fully mediated the relationship between ethical leadership and nurses’ extra-role service behavior.
Conclusion:
Organizational ethical leadership positively affected ethical climate, which positively affected nurses’ moral sensitivity and affected both their role-prescribed service behavior and extra-role service behavior.
Keywords
Introduction
In the face of policy limitations on healthcare institutions and the competitive environment of large hospital expansions, delivering high-quality service is considered a key success factor in the healthcare industry. The pursuit of service excellence is considered an essential strategy. 1 Thus, an increasing number of hospitals seek to offer excellent quality beyond patients’ minimum needs and expectations. 2 Nurses’ service behavior can be considered a patient-centered care 3 and have a crucial influence on service evaluation and long-term success of hospitals. Therefore, nurses’ service behaviors have critical implications for hospitals.
As nurses’ service behavior describes a moral philosophy with core value: considering patients’ wants, needs, and preferences. 4 In our view, service behavior refers to the caring or helpful behavior of nurses directed toward the patients, and it is kind of patient-oriented ethical behavior. However, the ethical consideration of nurses’ service behaviors has been ignored by previous researchers. 5 Moreover, previous studies have been limited in that they have classified the predictors of service behaviors into only two broad categories: individual differences and organizational factors, 6 but few studies have adequately accounted for how organizational or individual antecedents can induce employees to engage in service behaviors; 7 especially in nursing practice, how the organizational factors affect nurses’ psychological processes to implement service behaviors have not been previously discussed. In addition, even though previous research on customer service behaviors have dealt with two types of employee behaviors, such as role-prescribed and extra-role behaviors, 6,8,9 researchers mainly focused on the one side of role-prescribed or extra-role service behavior (ESB) in their research models. 6
Given these gaps in the literature, this study aims to explain the ways in which organizational ethical leadership (EL) and ethical climate (EC) can influence nurses’ service behavior by moral sensitivity and examine the relationship from a comparative view of the role-prescribed service behavior (RSB) and ESB.
Background
In service research, RSB refers to expected employee behaviors in serving the firm’s customers that may derive from implicit norms in the workplace or from explicit obligations as specified in company documents. 10 ESB refers to discretionary behaviors of contact employees in serving customers that extend beyond formal role requirements. 9 Since this study was done in the context of healthcare environments, the operationalized RSBs were the extent to which nurses understand the patient’s needs and desires and can therefore help or provide solutions for patients. And the operational definition of ESB was the extent to which nurses’ non-compulsive, helpful, and constructive behaviors involving serving and helping patients. Both RSB and ESB are discretionary behaviors with a strong flavor of patient-centeredness that involve helping patients with work-related problems; these behaviors are especially critical for the success of hospital. 10,11
Along with the changes in the nurse–patient relationship and the shortage of nurses in China, nurses who have been under great work stress for a long time develop moral numbness toward clinical ethical dilemmas. Awareness of the ethical issues of clinical settings is the first of four components involved in making an ethical decision and taking an ethical action. 12,13 Without recognizing the ethical aspects of a situation, it is impossible to solve any ethical problem because without the initial recognition, no problem exists. 14 According to Lützén et al., 15 moral sensitivity is defined as an “attention to the ethical values involved in a conflict-laden situation and a self-awareness of one’s own role and responsibility in a situation.” Development of moral sensitivity creates an attitude and ethical response in nurses and enables providing ethical care and service for patients, 16 and this development leads to ethical decision-making that favors the patients. 13 In this sense, moral sensitivity is the source of nursing ethics, and it is also the prerequisite for nurses’ service behaviors.
There is a paucity of research in examining the factors of nurses’ work environment and its association with nurses’ service behavior. Current literature suggests that the way nurses perceive their work environment can affect their recognizing ethical issues and their ethical decision-making. 17 EC has earlier been defined as “the shared perceptions of what ethically correct behavior is and how ethical issues should be handled.” 18,19 In nursing, EC has been described as the nurses’ perceptions of handling ethical issues in their work setting. 20 EC not only affects which issues organizational members consider to be ethics-related but also determines the ethical standards that members use to understand, weigh, and resolve such issues. 21 Silén et al. 22 concluded that a positive EC can be characterized by the ability to meet the needs of patients and relatives, to get and give support and information within the working group, and to have a code of conduct in the workplace. In research by VanSandt et al., 23 the results proved that the ethical work climate is a major factor of a person’s ethical awareness.
According to Social Learning Theory, EL is defined as “the demonstration of normatively appropriate conduct through personal actions and interpersonal relationships and the promotion of such conduct to followers through two-way communication, reinforcement, and decision-making.” 24 In other words, ethical leaders influence the ethical behavior of followers by setting and observing high ethical standards and the use of reward and punishment. 24,25 For example, nurses in their everyday work demonstrate a commitment to ethical practice and can act as ethical role models for others. Nurse managers such as matrons, supervisors, and head nurses are responsible for influencing their employees and for acting as mediators between organizational and professional values. 26 Essentially, ethical leaders help create an organizational climate in which doing the right thing is expected and valued through role modeling appropriate behavior. According to Shin, 27 EL is one factor that has been identified as an antecedent of EC.
The purpose of the study
The aforementioned literature indicates the apparent complexity of the relations between EL and nurses’ service behavior. The purpose of this study is to develop and test the research models that investigate the effects of EL, EC, and nurses’ moral sensitivity to service behaviors. It was hypothesized that EL would influence nurses’ service behavior through a chained mediation model; that is, EL impacts nurses’ service behavior first through EC and then through nurses’ moral sensitivity. Moreover, the effects on RSB and ESB were tested.
Methods
Participants and data collection
This study employed random and convenience sampling. In June 2017, questionnaires were administered to 600 Chinese nurses from three tertiary hospitals (500+ beds each) in Hebei Province. A total of 476 survey forms were returned completed, corresponding to 79.3% of the total number of nurses. The overall sample was overwhelmingly female (95.8%), was young (94.5% under the age of 40 years), and had received collegiate education (97.7% had a bachelor’s degree or above). Table 1 contains the data describing these samples.
Demographic characteristics.

These nurses first read and signed a consent form indicating that their participation was voluntary and guaranteeing the anonymity of their individual responses. After signing and returning the consent form, each nurse was presented with the survey instrument. The instrument included several demographic questions. The participants were instructed to read the statements carefully and to respond to the associated questions.
Ethical considerations
Approval was obtained from the Ethics Committee at School of Nursing, Hebei Medical University. Data privacy and confidentiality were maintained and assured by obtaining subjects’ informed consent to participate in the research before data collection. All participants were informed of their right to withdraw from the survey at any time.
Measures
All the measures were prepared in Chinese. However, the scales of EL, EC, and moral sensitivity were cited in English articles, and they were subsequently translated into Chinese by the third author (Z.G.). For avoiding distortion in the translation, the scales were translated back to English by two professionals independently and compared with the original English version of the paper. No significant differences in language were identified.
Ethical leadership
Brown et al. 24 developed a 10-item instrument to measure EL. The 10 items were rated on a 5-point scale (5 = strongly agree; 1 = strongly disagree). For example, “My superior listens to what followers have to say” and “My superior makes fair and balanced decisions.” High scores imply higher EL. Cronbach’s α for EL was 0.933.
Ethical climate
According to Abou’s 28 research, Ethical Climate Questionnaire (ECQ) developed by Victor and Cullen was used to measure nurses’ perceptions of EC in their work settings. 19 It consisted of 24 items including five dimensions: instrumental, caring, independence, law and professional codes, and rules. Responses were measured on a 5-point Likert-type scale ranging from 1 = strongly disagree to 5 = strongly agree. Sample items were “Our major concern is always what is best for the other person” and “In this hospital, the law or ethical code of their profession is the major consideration.” A higher mean of EC reflected a higher level of nurses’ perception of it. In this study, the scale’s α reliability was 0.766. The Cronbach’s α for sub-dimension of instrumental, caring, independence, law and professional codes, and rules were 0.675, 0.818, 0.744, 0.801, and 0.667, respectively.
Moral sensitivity
The Moral Sensitivity Questionnaire (MSQ) was developed by Lützén et al. for the purpose of measuring moral sensitivity in healthcare practice. 15 The MSQ we used consisted of three dimensions: moral burden, moral strength, and moral responsibility. The MSQ is a Likert-type measurement instrument consisting of a total of nine items. Score 1 expressed high sensitivity with “total disagreement,” and score 5 expressed low sensitivity with “total agreement.” An example item is “I find it very hard to cope with my emotions when meeting with patients who are suffering.” The internal reliability result for this measure was 0.776, and the Cronbach’s α for moral burden, moral strength, and moral responsibility were 0.638, 0.682, and 0.765, respectively.
Service behavior
Nurses’ service behavior was measured using the eight items developed by Chen. 29 As presented in Appendix 1, the service behavior scale consists of two dimensions: RSB and ESB. Eight items are rated on a 5-point Likert-type scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicate a higher degree of service behavior. In this study, the scale’s α reliability for RSB, ESB, and overall service behavior were 0.867, 0.848, and 0.840, respectively.
Data analysis
SPSS and Mplus statistical software were used in data analysis. The descriptive statistics (means and standard deviation) and the correlation analysis of all the variables were utilized in the evaluation of the data. Mplus was used to estimate the models’ fit in this sample.
Results
Descriptive statistics
Descriptive statistics and correlations for control variables, EL, EC, moral sensitivity (MS), RSB, and ESB were provided in Table 2. RSB showed a positive correlation with EL, EC, and MS, with the highest correlation being with MS and the lowest correlation was with EC. ESB also showed a positive correlation with EL, EC, and MS, with the highest correlation being with MS and the lowest correlation was with EL.
Descriptive statistics.
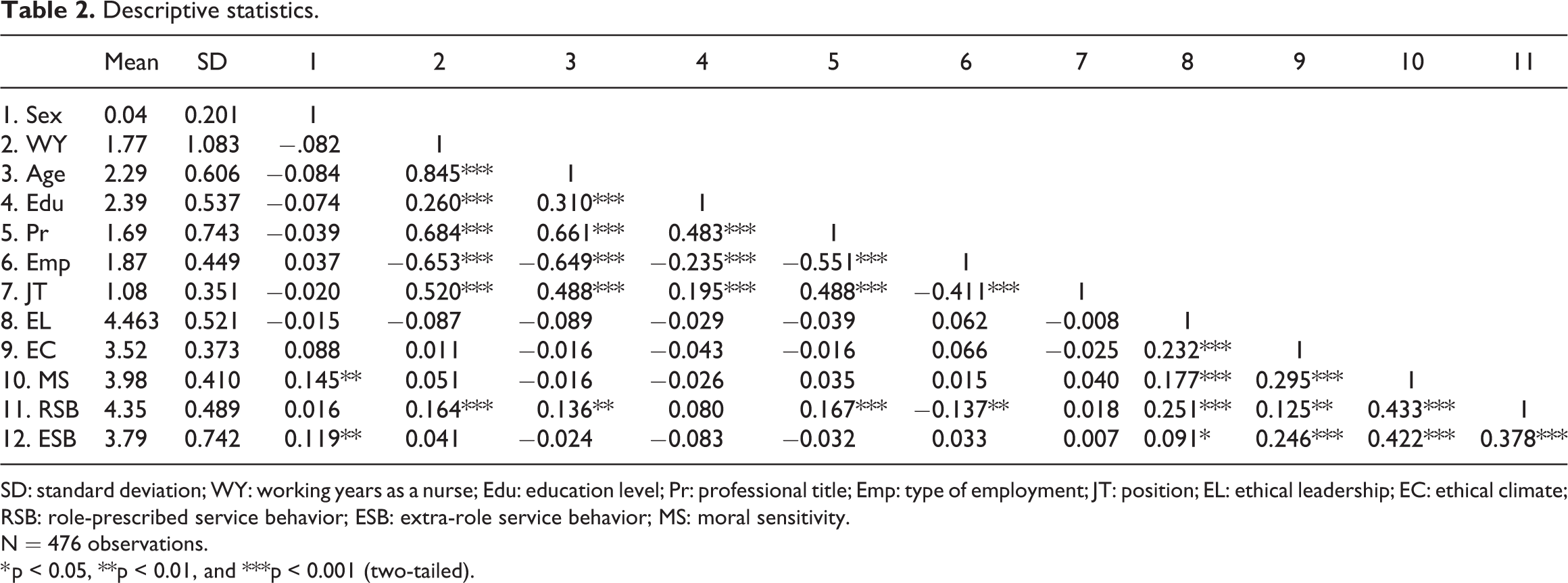
SD: standard deviation; WY: working years as a nurse; Edu: education level; Pr: professional title; Emp: type of employment; JT: position; EL: ethical leadership; EC: ethical climate; RSB: role-prescribed service behavior; ESB: extra-role service behavior; MS: moral sensitivity.
N = 476 observations.
* p < 0.05, **p < 0.01, and ***p < 0.001 (two-tailed).
Direct effects of ethical leadership on ethical climate, moral sensitivity, role-prescribed service behavior and extra-role service behavior
Structural equation modeling (SEM) examined the direct effects of EL (controlling for sex, WY, Age, Edu, Pr, Emp, and JT) on EC, MS, RSB, and ESB and provided an adequate fit to the data: root mean square error approximation (RMSEA) = 0.053 (95% confidence interval (CI) = 0.043, 0.063), close-fit test p = 0.305, comparative fit index (CFI) = 0.953, Tucker–Lewis index (TLI) = 0.926, and standardized root mean square residual (SRMR) = 0.040. The results showed that with the exception of ESB (β = 0.108, 95% CI = −0.042, 0.250), EL significantly influenced EC, MS, and RSB (Table 3). That is, there was a significant direct effect between EL and RSB, but not between EL and ESB. Furthermore, 87.2% of the variance in EC, 84.4% of the variance in MS, 81.9% of the variance in RSB, and 71.7% of the variance in ESB were accounted for in this model.
Direct effects models for EL predicting EC, MS, and RSB.

LL: lower limit of 95% CI; UL: upper limit of 95% CI; EL: ethical leadership; EC: ethical climate; RSB: role-prescribed service behavior; ESB: extra-role service behavior; MS: moral sensitivity. *p < 0.05, **p < 0.01, ***p < 0.001.
Chained mediation models between ethical leadership and role-prescribed service behavior
Pathway estimates and 95% CIs for the mediation models (controlling for sex, WY, Age, Edu, Pr, Emp, and JT) including RSB were provided in Table 4. EL was associated significantly with EC, MS, and RSB. EC was associated significantly with MS, with the exception of RSB. MS was associated significantly with RSB. A single-mediator effect was found between EL and RSB through MS (β = 0.047, p < 0.05), while the other single-mediator effect between EL and RSB through EC was not significant (β = −0.013, p > 0.05). There was a significant chained mediation effect from EL through EC and then MS to RSB (β = 0.023, p < 0.001). The total effect between EL and RSB was significant (β = 0.253, p < 0.001) and was mainly composed of direct effect, in which indirect effects only accounted for approximately 22.5%. Therefore, organizational EC and nurses’ moral sensitivity partially mediated the relationship between EL and nurses’ RSB. Figure 1 shows the chained mediation models between EL and RSB with resulting path coefficients.
Chained mediation models of EL, EC, MS, and RSB.

EL: ethical leadership; EC: ethical climate; RSB: role-prescribed service behavior; ESB: extra-role service behavior; MS: moral sensitivity; CI: confidence interval. *p < 0.05, **p < 0.01,***p < 0.001 (two tailed).
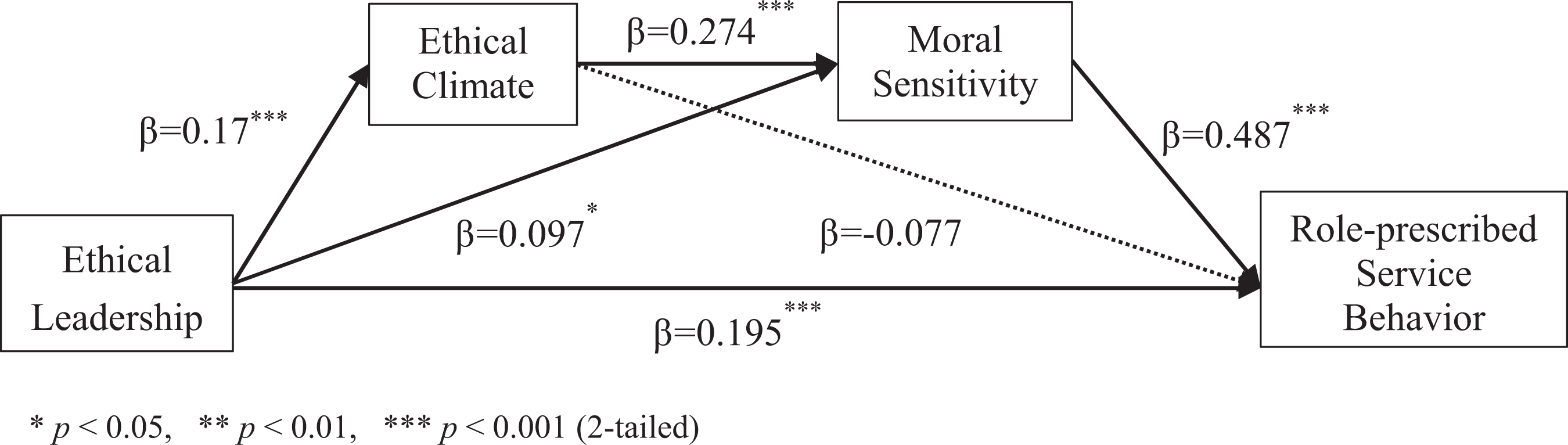
Chained mediation model from ethical leadership to role-prescribed service behavior.
Chained mediation models between ethical leadership and extra-role service behavior
Pathway estimates and 95% CIs for the mediation models (controlling for sex, WY, Age, Edu, Pr, Emp, and JT) including ESB were provided in Table 5. EL was associated significantly with EC and MS, with the exception of ESB. EC was associated significantly with MS and ESB. MS was associated significantly with ESB. The single-mediator effects between EL and ESB through both MS (β = 0.048, p < 0.05) and EC (β = 0.029, p < 0.1) were positively significant. There was a significant chained mediation effect from EL through EC and then MS to ESB (β = 0.023, p < 0.01). Moreover, EC and MS fully mediated the independent-to-dependent variable relation (Taylor et al., 2008). The total effect between EL and ESB was marginally significant (β = 0.106, p < 0.1) and was mainly composed of indirect effects, in which direct effects only accounted for approximately 5.7%. Figure 2 shows the chained mediation models between EL and ESB with resulting path coefficients.
Chained mediation models of EL, EC, MS, and ESB.

EL: ethical leadership; EC: ethical climate; RSB: role-prescribed service behavior; ESB: extra-role service behavior; MS: moral sensitivity. +p < 0.1, *p < 0.05, **p < 0.01. ***p < 0.001 (two tailed).

Chained mediation model from ethical leadership to extra-role service behavior.
Discussion
Our study significantly contributes to nurses’ service management literature by investigating the impact of organizational EL on the two types of nurses’ service behaviors, incorporating the mediating mechanisms of organizational EC and nurses’ moral sensitivity in a single parsimonious framework. As we predicted, there were significant correlations between EC and nurses’ RSB, ESB, and overall service behavior. Therefore, we proved that when the leaders are ethical, they are more likely to create a circumstance in which doing the right thing is expected and valued. 24 Ethical circumstances include the nurses’ consciousness of ethical problems and desires to maintain high moral standards. 30 When nurses work in an EC, they are more inclined to be sensitive to ethical issues in various situations and then implement RSB and ESB. The findings of this study have several theoretical implications.
First, this study is one of very few attempts to investigate relationships among organizational EL, EC, nurses’ moral sensitivity, and service behaviors. Our findings respond to the calls and paints a more detailed picture of how organizational or individual antecedents induce employees to engage in service behaviors. 31 As such, this study provides useful insights on the moral psychological mechanism of organizational environment affecting nurses’ service behaviors. Reinforcing the contention in the literature that the link between organizational management practices and employee service behaviors may be better explained by mediating variables, 32 our results highlight the significance of organizational EC and nurses’ moral sensitivity as mediators in the relationship between organizational EL and nurses’ service behaviors.
Second, this study has examined the relationship from a comparative view of the RSB and ESB. An SEM analysis supported the relationship between EL and service behaviors. However, there was a significant direct link between organizational EL and nurses’ RSB, but not between organizational EL and nurses’ ESB. The total effect between EL and RSB was mainly composed of direct effect. However, the total effect between EL and ESB was mainly composed of indirect effect. Organizational EC and nurses’ moral sensitivity fully mediated the relationship between EL and nurses’ ESB. Thus, if healthcare institutions want to increase the nurses’ ESB, they should pay more attention to training ethical leaders to cultivate an EC, and then, they can increase nurses’ moral sensitivity to provide nursing care that goes beyond existing role expectations and formal job descriptions.
Third, this study contributes to nurse ethics research by integrating service behavior into the ethical decision-making model. Moral sensitivity was the first step in ethical decision-making and ethical behavior was the last. As nurses’ service behaviors are the caring or helpful behaviors of nurses directed toward patients, they are kind of patient-oriented ethical behaviors. Social desirability is the tendency of individuals to deny socially undesirable traits and behaviors and to admit to socially desirable ones; 33 in existing studies, there were few empirical studies of ethical behavior due to its social desirability. The introduction of nurses’ service behavior as a specific ethical behavior into the field of ethical decision-making research will reduce the sensitive nature of ethics research effectively, and it will expand the theoretical domain of nurse ethics and service behavior theory and enrich the research results of ethical decision-making.
A major limitation of this study is that all variables were measured via self-report with survey methodology leaving open the chance for common method variance to influence the results. We acknowledge that the use of self-report measures is a potential limitation of the study. Nevertheless, we note that the most valid source for information about an individual’s moral sensitivity is the individual him- or herself. Social desirability bias is a problem that must be solved in the self-report survey; 34 especially in ethics research, researchers need to be particularly sensitive to the potential effects of a social desirability response bias. 35 To overcome this weakness, it is clear that multiple indices (e.g. physiological, physiological indexes) should be used to indicate more reliable information about the moral sensitivity levels of participants in the future. In addition, the sample was confined to one region of China, which may limit the generalization of the findings to other Chinese-speaking areas. As previous study demonstrated that employees who live in collectivistic societies are more likely to define extra-role behaviors as part of their expected job behaviors compared with employees who live in individualistic societies. 36 Chinese nurses are more likely to possess collectivistic cultural values than those nurses who are from the West, which may yield systematic biases in their responses to the surveys used in the research. 9 Further national and international research could contribute to a greater understanding of the effects of EL, EC, and nurses’ moral sensitivity to their service behaviors.
Conclusion and implications
In conclusion, organizational EL positively affected EC, which positively affected nurses’ moral sensitivity and affected both their RSB and ESB. However, the mediating effects were different; organizational EC and nurses’ moral sensitivity partially mediated the relationship between EL and nurses’ RSB but fully mediated the relationship between EL and nurses’ ESB.
Based on these findings, this study provides some implications for hospital administrators and nursing managers: First, select and educate ethical leaders to foster an EC and increasing moral sensitivity of nurses. Second, pay more attention to cultivate EC, and then, the nurses will be promoted to be more sensitive to the clinical issues and provide more patient-centered service behaviors. Third, as kind of patient-oriented ethical behaviors, nurses’ service behaviors, both role-prescribed and ESBs, are encouraged.
Footnotes
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Social Science Foundation of China (15CGL075), Shandong Social Science Planning Fund Program (18DGLJ02), and the Scientific Research Foundation of Beijing Information Science & Technology University (1835002). We are grateful to the hospitals and their employees who participated in this study.