
Abstract
Background:
Promoting patients’ rights is essential for defining the standards of clinical services within a country. Given their responsibilities, nurses can be the primary target for research to investigate the issue of patients’ rights within a healthcare system. As such, assessing the knowledge of nurses about patients’ rights is an essential step toward improving the quality of healthcare in limited resource settings like Sudan.
Objectives:
We aimed to assess the level of knowledge about patients’ rights among the nursing staff at Friendship Teaching Hospital in Sudan.
Methods:
This hospital-based cross-sectional study was carried out at the Friendship Teaching Hospital in Sudan. We surveyed the totality of nurses (95) at the hospital using an amended survey. The data were analyzed in SPSS software using descriptive and inferential statistics.
Ethical consideration:
The study was approved by the Research Unit of Khartoum Ministry of Health and the Hospital administration. All respondents gave verbal consent prior to participating in the study.
Results:
Only 48.4% of the participants knew about the existence of the Sudanese Charter of patients’ rights. Nonetheless, our analysis found that 65.8% of nurses had acceptable level of knowledge (scored more than 75% of the total knowledge score) of patients’ rights, and none of the participant scored less than 50% of the total knowledge score. Finally, we found no statistical association between the knowledge score and demographic data, educational level, whether the participant knows about the existence of the Charter or not and a number of other factors.
Conclusion:
Nurses’ lack of knowledge about the existence of the Sudanese Charter of patients’ rights adopted in 2009 rights confirms the need for further efforts by Ministry of Health to promote the document. Furthermore, further research is needed to investigate the disconnect between nurses’ lack of knowledge about the existence of the charter and their awareness of the rights within the charter as well as the actual implementation of rights.
Introduction
The specifics of patients’ rights vary depending on the social context. Nonetheless, there is a growing global consensus that privacy, confidentiality of medical information, right to treatment refusal, proper information on healthcare services, and acknowledgment of relevant risk of medical procedures are universal patients’ rights. 1 Promoting patients’ rights must be a priority for healthcare policy makers all over the world. Adopting patients’ rights regulations is a quality assurance measure that promotes health ethics and protects patients against discrimination. 2 Moreover, promoting patients’ rights is essential for defining the standards of clinical services within a country. 3
The concept of patients’ rights has been on the rise following the adoption of the United Nations’ Universal Declaration of Human Rights (UDHR) in 1948. 4 Ever since, numerous countries have adopted some version of patients’ rights regulations. 5 In 2009, the Sudanese Federal Ministry of Health, in collaboration with the Sudanese medical council, adopted the Patients’ Charter of Rights as part of the National Health Policy. The charter states that, in addition to the right to basics services provided in healthcare facilities, patients have the right to know the diagnosis, medications’ side effects, considered medical interventions and the names of medical staff, as well as the right to have a translator, information about hospital ombudsman office, and a medical report and even the right to refuse examination and treatment. 6 Many of the components of the charter are consistent with the cultural values in Sudan, especially rights related to privacy and confidentiality.
It is important to note that passing regulations does not always translate into implementation. The World Health Organization cautions that creating patients’ rights regulations, without efforts to raise awareness about the importance of these rights, does not lead to improved quality of healthcare. 7 It follows that several studies have reported violations of basic patients’ rights such as informed consent in countries where patients’ rights Charters were adopted. 8 –10
Success in improving the quality of healthcare through a patients’ rights approach is dependent on both patients’ and healthcare professionals’ knowledge and implementation of rights. 11 Among healthcare professionals, midwives, nurses, and physicians hold the primary responsibility for persevering the rights of patients. 12 A number of scholars argue that—due to the amount of time nurses spend of with patients’—nurses have an even greater responsibility to preserve patients’ rights than other healthcare professionals. 13 Nurses are suited to gain the appropriate knowledge and develop the required awareness to uphold the rights of their patients. 14
Generally, studies have found that healthcare professionals report knowledge and commitment to respecting patients’ rights. Nevertheless, prior research has also shown that there is a gap between the practice of patients’ rights among healthcare professionals, and their perceived knowledge and awareness of such rights. 4,15 Given their position, nurses 16 can be the primary target for research to investigate the issue of patients’ rights within a healthcare system. As such, assessing the knowledge of nurses about patients’ rights is an essential step toward improving the quality of healthcare in limited resource settings like Sudan. Prior research in different countries has shown poor, moderate, or even high levels of knowledge of nurses regarding patients’ rights. For example, a study in India found that nurses exhibited high levels of knowledge of patients’ rights ranging from a mean of 68.5% to 71.43%. 17 Another study in Turkey found that 51% of nurses and midwives did not know about legislation regarding patients’ rights in the country. 12 In West Indies, 37% of nurses had little knowledge about ethical guidelines. 16
Due to lack of data, the extent to which the Sudanese Charter of patients’ rights has been utilized remains unclear. To our knowledge, no previous study has examined healthcare professionals’ knowledge or implementation of patients’ rights in the Sudan. Furthermore, there is no monitoring and evaluation system established by the government to assess whether the existence of the Charter has led to improved healthcare quality in the country. To that end, this study aims to assess the level of knowledge about patients’ rights among the nursing staff at Friendship Teaching Hospital in Sudan. Moreover, the study ultimately aims to contribute to reducing the gap in patients’ rights research in the country.
Methods
Study design and setting
This hospital-based descriptive cross-sectional study was conducted in one of the tertiary hospitals in Khartoum state, Sudan. The hospital delivers services for a considerable portion of the Khartoum’s population with almost 200 beds and a mid-annual admission of 9381 patients. The hospital provides a wide range of services, through healthcare professionals and trainees in the main four clinical departments in addition to Ophthalmology and Dermatology referral clinics, to a diverse population. The study targeted the totality (n = 95) of the nursing staff at the hospital. The staff included full-time nurses, part-time nurses, midwives, and nursing students officially working at the hospital as part of their training.
Data collection
Two experienced investigators collected quantitative data from participants. Out of the total number of nursing staff, 90 agreed to join the study, with a refusal rate of 5.3%. Data were collected using a structured, self-administered questionnaire. The questionnaire followed the structure of the questionnaire used by Sheikhtaheri et al. 18 We created a questionnaire that accurately reflects the rights asserted in the Sudanese Charter of patients’ rights. Ultimately, 16 questions were used to assess the nurses’ knowledge of patients’ rights. Moreover, a new section was added to assess the general information about patients’ rights among the nurses.
Statistical analysis
The data were entered and analyzed by SPSS software version 24. To analyze knowledge levels, the researchers used Likert scale with a range from 5 (completely agree) to 1 (completely disagree). The level of knowledge was categorized as follows: scores less than 50% of the total points (for total questions and for each question) were considered “unacceptable,” between 50% and 75% were considered “relatively acceptable,” and more than 75% were considered “acceptable.”
Wilcoxon rank sum test was used to compare categorical demographic and knowledge, where appropriate. A logistic regression was used to determine relationship between all independent variables (age, sex, education, and experience) and knowledge as dichotomous outcome. The significance level was set to 0.05 for all analyses.
Ethical considerations
The study was approved by the Research Unit of Khartoum Ministry of Health and the Hospital administration. All respondents gave verbal consent prior to participating in the study.
Results
A total of 90 nurses completed the survey. The majority of survey participants were females (80.9%), who received a nursing diploma prior to practicing (71.8%) and had more than 10 years of nursing experience. Further demographic characteristics are depicted in Table 1.
Demographic characteristics of survey participants.

Less than half of the participants (48.4%) knew about the Sudanese Charter of patients’ rights, and of those who did, only 37.7% have read it. However, in terms of the participants’ perception of their level of knowledge about patients’ rights, only 10% thought their knowledge was poor, while the vast majority thought their knowledge was excellent or very good (Figure 1). Most participants (72.1%) stated they never experienced any patients’ rights problems or complaints; nonetheless, workplace was the most common source of knowledge for participants (Figure 2).

Nursing staff perceptions about their level of knowledge (n = 90).
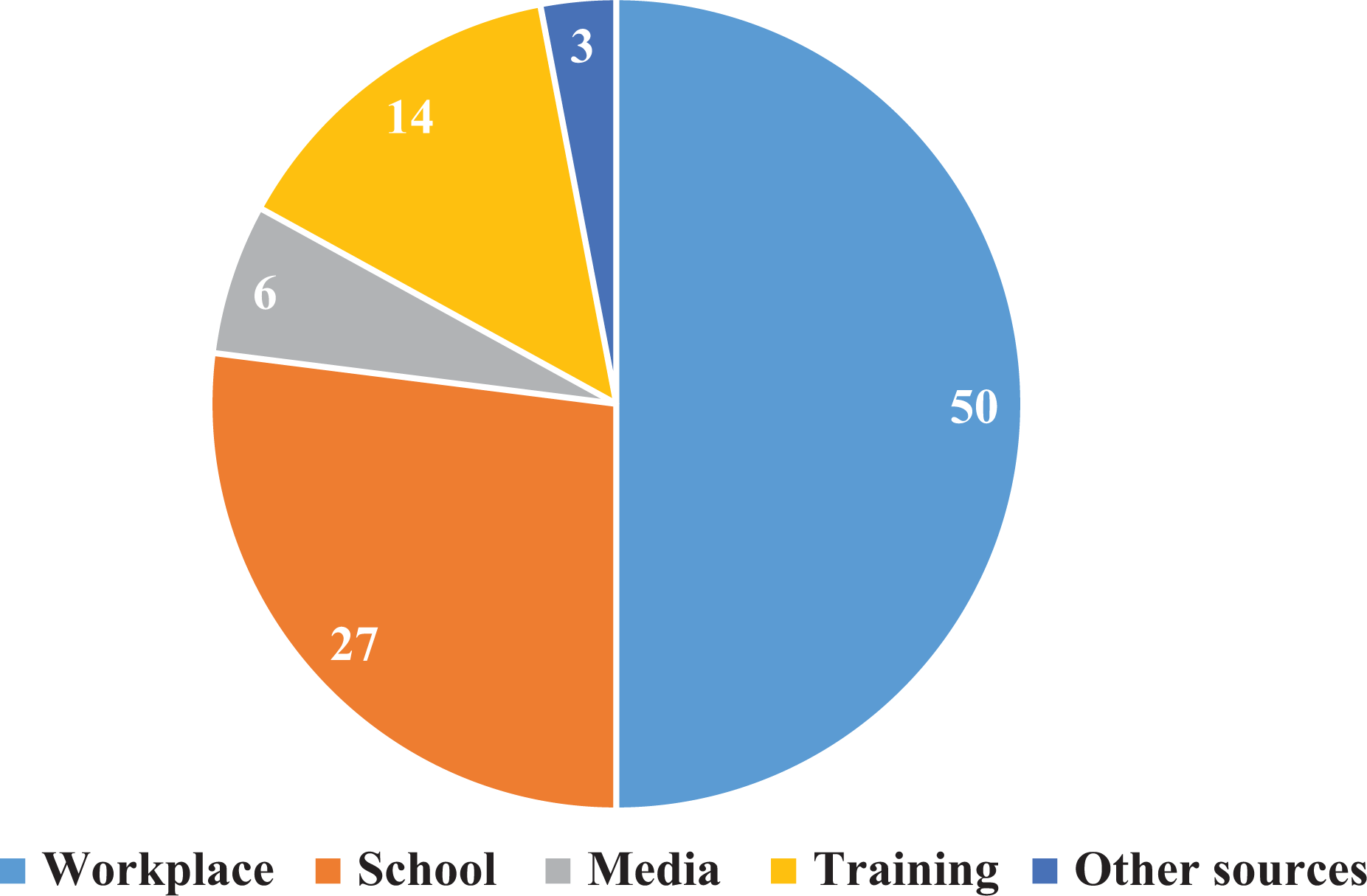
Sources of nursing staff knowledge about patients’ rights (n = 90).
Our study showed that 34.2% of participants have relatively acceptable knowledge (scored 50%–75% of the total knowledge score), and 65.8% of them have acceptable level of knowledge (scored more than 75% of the total knowledge score) of patients’ rights. None of the participants scored less than 50% of the total knowledge score. The least known rights were the “right to know the names and specialties of the healthcare team” and the “right to access their medical record” which were recognized only by 17.2% and 29.2% of participants, respectively (Table 2).
Nursing Staff Knowledge of Patients’ Rights Concepts.

SD: standard deviation.
In addition, we found no statistical association between the knowledge score and the sex, age, educational level, years of experience, whether the participant knows about the existence of the Charter or not, whether the participant received any training about patients’ rights or not, and source of information about patient’s rights. Following multivariable adjustment, there was still no association between age, sex, education or experience, and knowledge as a dichotomous variable.
Discussion
This hospital-based, cross-sectional study shows that the nursing staff at Friendship Teaching Hospital lacked awareness about the Sudanese Charter of patients’ rights. Less half of the nursing stuff in our cohort were not aware of the existence of a Charter of patients’ rights in Sudan. Nonetheless, 65.8% of the nursing staff had an acceptable level of knowledge about patients’ rights.
Our findings are similar to those from other low- and middle-income countries; studies from Turkey and Egypt showed that about half of the nurses and physicians were not aware of the Charter of patients’ rights in their countries; 12,19 the figure rises to 69% in Uganda. 2 Moreover, of the participants who heard of the Sudanese Charter of patients’ rights, only a third of read the Charter. Similarly, Ducinskiene et al. 20 reported in their study that among those of the medical stuff who knew of the existence of the charter of a patients’ rights, only 32.3% read the Charter.
Nevertheless, despite the lack of knowledge about the existence of the Sudanese Charter of patients’ rights, participants in our cohort demonstrated a high level of awareness about the rights. The results of our study were similar to those from comparable demographics. A number of studies in low- and middle-income countries have reported results consistent with our study. Sheikhtaheri et al. 18 found that 69.85% of Iranian nurses had an acceptable level of knowledge regarding patients’ rights. Likewise, other studies from Iran, 11 Yemen, 21 Turkey, 12 and Uganda 2 reported similar results.
The disconnect between knowledge of the presence of a Sudanese Charter of patients’ rights and awareness of the actual rights was uniform. We found no statistical association between the level of awareness and demographics, whether a participant heard about the patients’ rights charter, whether the participant received any training about patients’ rights, source of information about patient’s right’s or following a complaint from a patient regarding patient’s right’s. While one study reported comparable results, 22 the majority of similar studies reported different results and found significant association between nurses’ awareness and work experience, 11,23 sex, 19 educational level, 18 nurses’ marital status, 24 or the being confronted with a problem concerning patient rights. 18
The results of our study raise a question on the disconnect between knowledge about the existence of the Sudanese charter of Patients’ Rights and knowledge about its contents. One justification is that the nurses’ answers on the actual rights are based on their religious and cultural background. El-Sobkey et al. reached a similar conclusion in their study on health professions’ students’ awareness about the charter of patients’ rights in Saudi Arabia. They concluded that the gap can be attributed to the cultural background that encourages all to preserve rights, such as privacy and confidentiality of others. 25 This rationale can be applicable to our study as Sudan has a similar cultural and religious context as Saudi Arabia, especially as the participants in our study generally scored higher in rights such as confidentiality and privacy.
Another justification of the results can be the nature of the knowledge score questions in our survey. While questions on knowledge of the existence of the Sudanese Charter of patients’ rights were yes or no questions, the knowledge score section provided a scale which can potentially lead to a social acceptability bias and prompt the participants to self-report the answers they deem most acceptable by the researchers, especially because the data collectors where physicians. Both explanations can be supported by the lack of association between whether participants in our study received a training regarding the Sudanese Charter of patients’ rights and their level of knowledge of the rights within the Charter.
To interpret the results of our study, limitations must be taken into account. The study only focused on one hospital in Khartoum, Sudan. Therefore, the results cannot be generalized nationwide. Moreover, results were based on self-reporting and, as mentioned above, our survey was subject to social acceptability bias. However, the presence of the social acceptability bias will most likely lead to our study overestimating the results, indicating a lower level of knowledge among the cohort.
Notwithstanding these limitations, our findings have two major implications. First, our study found that no clear efforts have been undertaken by the Ministry of Health to educate nurses following the adoption of Sudanese Charter of patients’ rights. Second, the gap in our results emphasizes the need for further research; not only on the level of nurses’ knowledge of the charter of patients’ rights and its contents but also on whether nurses translate their knowledge into practice, as prior research have found that even nurses and physicians who report knowledge of patients’ rights, rarely implement these rights. 26
We propose that even if nurses are aware of patients’ rights, lack of knowledge on the existence of a formal charter of rights might preclude the nurses from implementing these rights. Thus, as there is evidence that training sessions lead to both better knowledge about the Charter as well as perceptions regarding patients’ rights, 27,28 we recommend that the government to undertake training sessions to educate nursing staff nationwide on the existence the Charter of patients’ rights and its content.