
Abstract
Background:
If collectivistic-oriented family carers choose professional care for dependents with dementia, they risk being stigmatised as failing their obligation. This may influence dementia care choices.
Research question:
How may individualistic and collectivistic values influence choices in dementia care?
Method:
Qualitative design with in-depth interviews with a total of 29 nurses, 13 family members in Norway and the Balkans and 3 Norwegian dementia care coordinators. A hermeneutic content-focused analysis was used.
Ethical considerations:
Ethical approval was obtained from the Regional Ethics Committee for Research, South-Eastern Norway, and the nursing homes’ leadership.
Findings:
Family domain reasons why institutionalisation of dependents with dementia was seen as a last resort: obligation towards family members, particularly parents; worry about other family members’ reactions and inability to cope with the care for the person with dementia. Social domain reasons: feelings of shame and stigma regarding dementia, particularly in connection with institutionalisation of family members.
Discussion:
Children’s obligation towards their parents is an important aspect of the morality of collectivistic societies. Institutionalising parents with dementia may cause feelings of guilt and shame and worry about being stigmatised and ostracised. To avoid blame and rejection, caregiver(s) try to keep the fact that family members have dementia ‘in the family’. The decision to accept professional healthcare for dependents with severe dementia or have them admitted to a geriatric institution was postponed as long as possible.
Conclusion:
Family care morality may constitute a significant barrier against seeking professional help for persons with dementia, a barrier based on the expectation that the family will care for their old, even when suffering from severe dementia. Hence, stigma and shame may significantly affect the provision of care. Culturally tailored information may encourage family carers to seek professional help before the disruptive influence of the disease makes institutionalisation the only feasible option.
Introduction
In individualistic societies, morality and moral practices are justified by societal agreements 1 and perceived as universal. 2 According to Johnstone, 3 morality in ‘large scale’, ‘modern’ or individualistic societies is perceived as a goal rather than a means to an end and is expressed through compliance to rules rather than through the quality of relationships. Relationships in such societies tend to be less close, less intense and of less importance, both on the individual and the societal planes. 3 As opposed to this, in ‘small-scale’, ‘traditional’ or collectivistic societies, morality tends to be a process – to an end – and is expressed through the quality of various inter-human relationships, characterised by values like friendship, family loyalty, empathy, altruism and trust rather than the observation of abstract deontological principles. These divergent societal trends regarding morality tend to influence whether family care or professional care is seen as morally the best way to care for persons with severe dementia. A collectivistic background tends to lead to a preference for family care, and to cope with the care for person with dementia within the family tends to be a question of honour and duty.
Background
Hofstede 4 established individualism and collectivism as concepts to help differentiate between various cultures. As these concepts dichotomise the world without considering that most cultures have both individualistic and collectivistic characteristics, their use has both supporters and critics. One may find many common values across this dichotomous divide, and there may be great differences between members of one and the same cultural group. Furthermore, there is a transitional trend from collectivism to individualism in many urban areas. 5 Even so, these concepts are found to be useful to this discussion.
Within collectivistic philosophy, the group is the core element. The individuals must learn to fit in and find their role in the society to which they belong: The self is a part of a community, defined relative to others, concerned with belongingness, dependency, empathy, reciprocity and focused on small, selective in-groups at the expense of out-groups. The interdependent self exercises control to the interior, so that cognition and representation involve attentiveness to others, and personal attributes and actions are situationally bound. Autonomy becomes secondary, whereas relationships with others are emphasized, being ends in themselves.
6
(p. 2)
Within individualistic thought, the individual constitutes the core entity. As opposed to collectivistic societies where reciprocal dependence and the group’s communal goals, values, norms and world views guide behaviour, individualistically oriented persons perceive themselves as autonomous in relation to others, focus on personal goals and act based on personal perceptions and values.
8,9
Thus, an independent understanding of the self is the norm in individualistic societies: The distinctiveness of people, the uniqueness of a person, autonomy, and independence are emphasized. This requires construing oneself as an individual and speaking one’s mind…The consequence is that large, more inclusive but superficial in-groups are the norm, as opposed to the small, selective in-groups of the interdependent self construals.
6
(pp. 2–3)
If family carers no longer can cope with the care of dependents with severe dementia and need to accept assistance from professional healthcarers, either through home care or through having to institutionalise the dependent, they may be stigmatised by other family members and neighbours as failing their obligation. This consequence of collectivistic family care expectations is a topic that so far has received little attention. We have not been able to find previous studies focusing on how individualistic and collectivistic values may influence care choices for family members with severe dementia.
The research question is: How may individualistic and collectivistic values influence choices in dementia care?
Research methods
Literature searches
The electronic search engines used were CINAHL, Medline, Oria, Google Scholar and PubMed. In these searches were used a combination of the terms ‘collectivism’, ‘individualism’, ‘culture’, ‘stigma’, ‘dementia’ and ‘Alzheimer’s disease’ in English and Scandinavian languages.
The empirical studies
This article is based on the Norwegian (Oslo 1 and 2), Montenegrin and Serbian parts of an international study: ‘Good dementia care in a multicultural society’. i
These four sets of data have a qualitative design with an in-depth interview approach. A purposive sampling strategy was used to identify potential respondents. The heads of the respective geriatric institutions chose which family members and nurses to invite as participants. No honorarium was offered.
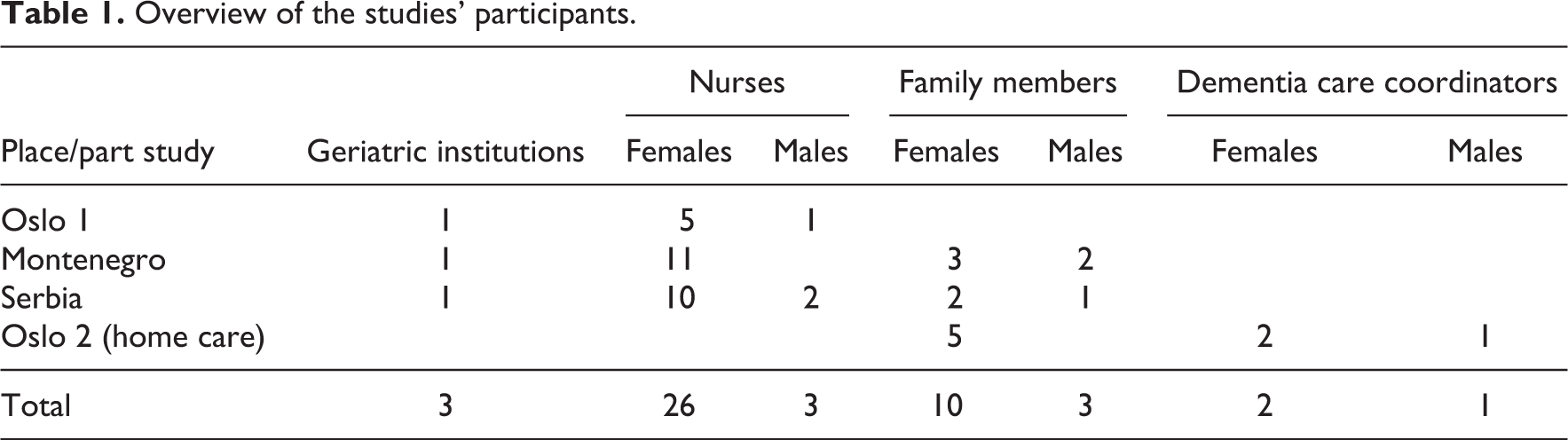
The interviewees in all parts of the study – patients’ close family members and nurses and in the Oslo-2 part-study also “dementia care coordinators” within the municipal home care services – were asked the following question: Based on your experiences from this geriatric institution/home care, can you tell us stories that illustrate good dementia care? A total of 13 family members, 29 nurses and 3 ‘dementia care coordinators’ were interviewed (Tables 1 and 2).
Overview of the studies’ participants.
National/ethnic backgrounds of the studies’ participants.

The interviews took the form of an electronically recorded talk where the interviewees were encouraged to share their thoughts and recount their experiences. Follow-up questions and the ‘mirroring’ of statements were used to develop, clarify and verify statements. This open approach allowed cultural issues to come to the fore.
Data analysis
The four sets of data were first studied separately and then in conjunction with each other after all interviews were transcribed. A content-focused approach was chosen to formulate themes touching the core of the situations or meanings found in the interviews. 17 No software was used.
The analysis was hermeneutic in character where we strived for depth of understanding through a circular investigation of the interview and literature texts. 18 Rigour was obtained through reading and re-reading the interview texts separately doing our best to ‘remain open to the meaning of the other person or the text’ 18 (p. 268), all the while re-evaluating our conceptions and deepening our understanding. We then consolidated our perceptions through discussing our findings and commenting on each other’s inputs. Context and culture were prominent issues, and we did our best to understand the cultural perception of people with dementia and the stigma of having relatives institutionalised. Gadamer 18 teaches us to be open, curious, communicate authentically and to realise that the fusion of horizons through the reading of texts leads to the creation of something new. Being two authors has been helpful, as we have discussed the meaning of the various findings and thusly done our best to avoid bias.
Ethical considerations
The project was approved by the Regional Ethics Committee for Research, South-Eastern Norway, and by the local heads of the respective healthcare institutions. All interviewees were informed orally and in writing that participation was confidential and voluntary and that they were free to withdraw from the project at any time. All interviewees signed an informed consent form. To ensure anonymity, we present the four-part studies as two main sets of data: Balkan data and Oslo data. The recorded interviews were deleted after transcription. Transcriptions are stored according to ethical research guidelines. 19
Limitations and critical remarks
Although professional interpreters were used during the Serbian, Montenegrin and one of the Oslo interviews, there is always a danger of meaning being changed or lost in translation. Furthermore, some of the interviews with Oslo nurses and family members where interpreters were not used would have run easier and the content been richer and more detailed if the interviewees had spoken a language with which they were more comfortable. These interviewees should therefore also have been offered the assistance of an interpreter.
Gender may influence both how situations are perceived and how experiences and feelings are expressed. In this study, only about 18% of the interviewees are males. We therefore do not have adequate data to discuss gender differences in relation to the research question.
Findings
All the interviewees except the ethnic Norwegians stressed culturally based family care expectations. Norwegian interviewees focused on family care orientation only when talking about their experiences working with non-western patients and their families. The results are organised based on two main domains: the family domain and the societal domain.
The family domain
Within collectivistic thought, care of the sick is a question of familial duty. Our family carer interviewees explained that they did everything they possibly could to care for their dependents at home for as long as possible. Healthcare professionals were only contacted when the situation became unmanageable. An Oslo family interviewee, for instance, related how her husband would shout and cry whenever she left the apartment. She was not even able to take out the trash as he would panic as soon as she was out of view thinking she had left him and gone back to their home country. In the end, admitting him to a nursing home was the only solution. According to one of the Oslo dementia care coordinators, many find it difficult to accept the offer of professional home care even when in dire need of such assistance. The three dementia care coordinators all found dementia to be a much more taboo topic among non-Western immigrants than among Norwegians. According to them, in many immigrant families, the professional healthcare providers may not be given leave to visit the person in need of care if the word ‘dementia’ is used when the family is first contacted.
Only six of the Balkan nurses and one of the nurses in the Oslo study said they would have chosen to have their parents in a nursing home if they developed dementia. The rest of the nurse interviewees were more ambivalent about placing a family member with severe dementia in a care facility or rejected such a move outright.
There seem to be three main reasons why institutionalisation of a dependent with dementia was seen as the very last resort:
1. Obligation towards family members, particularly parents:
It is my duty as daughter to nurse my parents…I would probably have tried to nurse my parents if possible…There have to be such institutions and there is a great need for them, but I think it is right to care for the family’s old [oneself]. (Balkan nurse)
‘[O]ne has to take time for one’s mother. That is very important…I would not have placed her in a home’ (Balkan nurse). Caring for a family member with dementia ‘is my task. My parents cared for me when I was a baby; they did everything for me. Now my mother is ill and I threw her out’ (Oslo family carer). Some of the interviewees worried that if they are not able to care for their own parents, they will be negative role models for their children, which will increase the risk of being sent to a nursing home when they themselves grow old.
2. Family carers worrying about other family members’ reactions if their parents were to live in a care facility: ‘What I care about is what my closest family would say to me…I would have had problems with my family’ (Balkan nurse). An Oslo interviewee found it difficult to tell family and friends that his father, a man of high standing in the local immigrant community, had developed dementia. But people started to notice mental changes in him and these could not be kept a secret. This made the family carers both worry that the father would lose public honour and they themselves would be rejected by the extended family for not honouring their duty towards the patient if they had to admit him to a nursing home.
3. Family carers are no longer able to cope with the care for their dependent: ‘It is not as if we wish for him to live in a nursing home. We don’t, but there is no other way. He is large and heavy and needs care 24/7’ (Oslo interviewee). A typical viewpoint is that ‘…for me it was absolutely the last resort’ (Balkan family member). To no longer be able to cope with the amount of care needed is hard: ‘It was hard to have to take her out of the family context and bring her here…We felt it was very regrettable’ (Balkan family carer). ‘The painful feeling, I had when I brought mother here [to the nursing home]! It pains me constantly’ (Oslo family carer). The dementia care coordinators held that in immigrant families ‘one feels that one wants to care for one’s parents oneself. And when one no longer can cope, one feels shame’. Oslo findings show that interviewees try to visit their institutionalised family members at least 3–4 times a week and that they get a bad conscience whenever they are not able to do so and that they “stretch” themselves as far as possible.
The societal domain
Both Balkan and Oslo interviewees talked about the feelings of shame and stigma in their societies regarding dementia and particularly in connection with institutionalisation of family members with dementia: ‘We want to care for Father ourselves. And when we are not able to do so any longer, it gives you shame’ (Oslo interviewee). A Balkan nurse explained that ‘a person is denounced if someone sends their family member to a nursing home. It is still shameful…I am not able to picture myself placing [my parent] in a nursing home’. Another Balkan nurse explained that It is very stigmatising. The attitude is that it is totally unacceptable that persons who have nurtured us and cared for us in our younger days and as adults, when the day comes that they need nurturing and nursing care, are being stowed away. That is perceived as turning one’s back on them.
‘To be placed in a nursing home is punishment, that one punishes one’s parents’ (Balkan nurse).
A Balkan interviewee explained that the general view is that old people, particularly an old man is supposed to be treated as the most important member of the family; he is supposed to be cared for and nursed and be looked after…one endures and does not discuss any different solution…one is to nurse one’s parents at home, regardless. In our culture we do not send our parents to nursing homes. We care for them ourselves. But here in Norway this is impossible…As we live here in Norway [my compatriots] say that it is customary, but deep down inside they do not think it is the right thing to do. there were no other alternative. Because they would understand that one has other responsibilities…and that it therefore would not be possible to give your mother the right kind of care and that there really is no true choice.
Discussion
Individualism and collectivism are concepts which express a fundamentally different construction of oneself and others and how one understands the relationship between the individual and the society, including professional healthcare. As seen in the findings section, family care traditions tend to be strong in collectivistic societies. The adult children themselves as well as members of their extended family and social network tend to expect them to care for their old parents, also when the parents suffer from severe dementia. In our studies, nursing homes were described as a last resort. As the reasons for this overarch the family and the societal domains, the discussion is focused on preserving family honour and moral obligations.
Preserving family honour: stigma avoidance
One of the central aspects regarding the dilemma of admitting a dependent with severe dementia to a geriatric institution or not is the collectivistic ethical demand of ‘bestowing honor upon one’s family, caring for aging parents, and carrying out parents’ wishes and dreams even after their death…Children are socialized to experience guilt and shame if they violate these principles – even after reaching adulthood’ 20 (p. 549).
In-group obligations are intrinsic facets of any collectivistic society’s ‘honour code’ or set of rules group members are expected to follow. 21 A person’s honour depends on the collective’s evaluation of his or her acts, and to act in conflict with the honour code creates public disapproval, dishonour and shame. As an example of this, Mohammadi claims that ‘[h]onour in the context of the Afghan community means complying in public with moral codes, social norms and essential interests of the group’ 22 (p. 1).
The interviewees who had placed family members with dementia in a nursing home tended to feel guilt and shame about the institutionalisation of their dependent. According to Arneson, 23 shame stems from feeling negatively judged according to the dominant standard of a given society or group. This is reflected in the interviews with several of the Balkan and Oslo interviewees. Many of the latter group of interviewees were worried about ‘loss of face’. Public loss of face may be seen as public stigma, that is, stigma in the societal domain, which refers to the reactions to lay persons towards a stigmatised individual or group. 24 Goffman 25 held that we are not aware of the society’s demands upon us ‘until an active question arises as to whether or not they will be fulfilled. We then realize that certain assumptions are being made about what is expected of us’ (p. 12). These expectations typically elicit a social process ‘characterised by exclusion, rejection, blame or devaluation’ 26 (p. 441).
If excluded by family and social network, the care person(s) become(s) isolated and forced to carry the load of caring all alone. To avoid blame and rejection, the caregiver(s) may try to keep the fact that a family member has dementia ‘in the family’ and make a valiant effort ‘to balance their caregiving role with maintaining previously held relationships, even though this [may prove] difficult’ 16 (p. 240). This was also the case among our Balkan family interviewees, as well as among many of the Oslo family interviewees. Dementia care coordinators often found it difficult having professional care accepted in the immigrant population even when both the patient and the family carers are in dire need of assistance. In one case, a daughter had to move to Norway to help her brother and his wife care for their father with dementia as they no longer were able to cope on their own and did not want help from professional healthcarers.
Moral obligation
To have family members admitted to a care facility does not conform with the cultural expectations of many ethnic groups and becomes a sign of the family’s moral failure. 25,27 The feeling of moral obligation to care for one’s parents was strong among both our Balkan and Oslo interviewees. They felt that they had failed their obligation towards their institutionalised parents and as role models for their children. The obligation children, particularly daughters, have towards their parents is an important aspect of the morality of collectivistic societies. It constitutes a part of what Jeske 28 has named special obligations.
Jeske 28 places special obligations in the ethical realm of common sense morality and points to several reasons why a person may have special obligations, for instance, the intrinsically understood quality of special relationships like being related and from childhood having received care from the person who now is in need of assistance himself/herself. This means that one’s obligations are particularly pointed at the person or persons who one may feel obliged to help whenever they are in need of care. Not being able to fulfil one’s filial duty tends to lead to a bad conscience.
The form and strength of the moral obligation, then, is decided by the individual’s relationship to the person or persons in question. Hence, within a collectivistic basic value system, (a) ‘the importance of social ties over individual desires and successes’ are stressed and (b) ‘the needs and the beneficence of the family or other important group (e.g. clan, nation, religious group) over needs of the individual person’ 20 (p. 549) are prioritised.
This feeling of moral obligation seems to be a rather universal sentiment. A study among 10 non-Western ethnic and two linguistic groups in Australia hailing from three different continents 29 shows that in all but three of these groups, stigma is common in connection with dementia, and in all the groups, family care is preferred and institutional care is either totally taboo or seen as a last resort. In the same vein, Wallhagen and Yamamoto-Mitani 11 found in their study among American and Japanese family caregivers that both groups considered the provision of care to old dependent family members a moral duty. As in our interviews, ‘this moral obligation derived partly from the life-long nurturing and care that the parent had provided to the caregiver…and from beliefs about reciprocity. Caregivers felt it was now time for them to repay their parents’ 11 (p. 68). However, the expectations regarding the manner of care may be different among, for instance, individualistically oriented ethnic Norwegians 30,31 and collectivistic-oriented immigrants. Among ethnic Norwegians, professional care tends to be perceived as the best solution for both patient and family and accepted as the “natural” step when a dependent develops severe dementia.
While some researchers find that traditional values continue to be honoured and that adult children are heavily involved in the care of old parents, 32,33 others detect changes in the attitudes of the younger generation regarding this. 34,35 Variations such as these we also found among our interviewees. In the Balkans, pace of life and family structures are changing, particularly in more urban areas. Even so, the morality concerning dementia care is different from Norwegian individualistic morality where seeking assistance from professional healthcarers is valued and more or less viewed as the norm. Individualistic societies are fundamentally contractual, which for instance is seen when all members of the Norwegian society have the right to receive the healthcare they need, which means that the healthcare system is obliged to offer the healthcare required. Hence, individualism may be seen as the primary value complex that healthcare ethics is based on both intellectually and morally. Many nursing ethicists see nurses’ responsibility towards specific individuals (persons with healthcare needs) as nursing’s motivating power 36,37 rather than the family and the individual as one entity with healthcare needs. In collectivistic societies, the tendency is to view morality as a process to reach a goal. Morality ‘is expressed through the quality of relationships (as characterised by values like friendship, family loyalty, empathy, altruism, the ability to trust in the family etc.), rather than a deontological adherence to abstract principles’ 3 (p. 145).
When one of the Balkan family interviewees used the word ‘regrettable’ to describe her feelings about having to have a dependent institutionalised, this seems to reflect the primary importance of the collectivistic traditions through a processional and relational understanding of morality. The decision to have the dependent with severe dementia admitted to a geriatric institution was something this and many of the family carers had postponed as long as possible.
Conclusion
We will argue that a collectivist obligation of family care is among the principal reasons why patients from many ethnic minority and immigrant groups may not receive the professional care they need, even when residing in Western countries like Norway where professional home care and later in the development of the disease, institutionalisation of patients with severe dementia is common or even the norm. Our interviewees with various collectivistic backgrounds clearly show a family care morality. This may constitute a significant barrier against seeking professional help for persons with dementia, a barrier based on traditions where the family is expected to care for their old, even when suffering from severe dementia. Stigma and shame may add significant obstacles to the well-being and quality of life both in persons with dementia and their families and affect the provision of care to those who need it.
This is something which health authorities in countries with well-developed professional geriatric healthcare services need to take to heart when considering how to reach out to members of the immigrant population in need of professional care. Information about available treatment and care options needs to be related in a way that is acceptable to the family. This will make it easier for the family to accept professional healthcare for their dependent with dementia. Culturally tailored information may furthermore encourage family carers to seek professional help at an early stage of a dependent’s dementia instead of as a last resort when the disruptive influence of the disease is felt so strongly that institutionalisation is the only feasible option. This will benefit the physical, psychological and social health of both the patient and his or her family. To achieve this, Hallén
38
holds that [t]he societal challenges regarding dementia diseases are so immense that increased formalized research across national borders is needed. The great increase in the number of persons with dementia is alarming in all countries, and we have to coordinate competencies as well as efforts internationally. (p. 6)
Footnotes
Acknowledgements
Program Director Anne Lene Sørensen, Lovisenberg Diaconal University College, Oslo, conducted all the Balkan interviews.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.