
Abstract
Background:
Nursing is a profession that has always been accompanied with common ethical concerns. There are some evidences which indicate that narrative writing on traumatic experiences may improve an individual’s emotional health.
Objective:
This study aimed to determine the effectiveness of narrative writing on moral distress of nurses working in intensive care unit.
Research design:
This study was a clinical trial with pre- and post-test design. The frequency and intensity of moral distress was measured by a valid and reliable questionnaire (Corely) at baseline and after 8 weeks. The intervention group was asked to write about their deepest emotions and stressful experiences in the intensive care unit for 8 weeks.
Participants and research context:
Using consensus sampling, 120 nurses of intensive care unit and neonatal intensive care unit of the teaching hospitals (in Iran) were invited to and were randomly allocated into the intervention and control groups.
Ethical considerations:
Participation was voluntary, data were anonymized, and the confidentiality of the participating nurses and their institutions maintained. The ethical approval was obtained from an IRB or research ethics committee.
Findings:
In total, 106 nurses completed the trial consisting of 87.75% females. The mean work experience of nurses in the intervention and control groups was 7.21 ± 4.96 and 8.28 ± 5.45 years, respectively. Independent t-test showed no statistical difference neither in the intensity of moral distress (P = 0.8), nor in its frequency (P = 0.5) between the two groups.
Discussion:
As nurses constantly face ethical tensions, moral distress is a phenomenon that results from the different situations of critical care units. Their concern about receiving negative feedback from the managerial level may have influenced the outcome of the intervention.
Conclusion:
Narratives writing by the nurses showed no effect on reducing the intensity and frequency of moral distress. It seems that due to the intensity of moral distress in clinical settings, we need to test variety solutions to reduce the problem.
Introduction
Nursing is a profession that has always been intrinsically accompanied with common ethical concerns. 1 Moral commitment in taking care of the patients is an integral part of nursing care in the nurse–patient relationship. 2 The concept of moral distress was initially defined by Jameton in 1984 in his book named “Nursing Practice: The Ethical Issues.” He believed that when a person has the knowledge of the ethically appropriate action to take but cannot act upon it due to encountering organizational barriers such as time constraint, lack of supervisors’ support, the imbalance of power between doctors and nurses, organizational policies, or legal restrictions, it will result in moral distress. 3 The clinical environment of the intensive care units (ICUs) is full of moral situations leading to moral distress. According to the evidences in Iran, the nurses in ICU still suffer from moral distress as stated by Atashzadeh Shorideh et al. 4 and Borhani et al. 5 “ICU nurses have to make and perform many moral decisions on a daily basis. However, in practice, they cannot always act according to their own beliefs. Thus, they are likely to experience moral distress as well.”
Due to the close contact of nurses with the patients, they identify such tensions much earlier in comparison to the physicians. 6 Because of conflict in care, patients’ suffering, delay in clinical decision-making for end-stage patients, the inappropriate use of healthcare recourses, poor communication between the doctor and patient’s family, and ignoring the patient’s wish, ICU nurses experience the highest level of moral distress. 7 In the study by Corley, 8 a moderate to high level of moral distress was reported by the ICU nurses; many of the participants mentioned invasive treatments and prolonging the patient’s life as the main factors causing moral distress. In Elpern et al.’s 9 study, a moderate level of moral distress was experienced by ICU nurses. Studying moral distress among the nurses working in the ICUs of Iran has revealed a high level of distress among them. 9 moral distress imposes significant adverse consequences on the physical and mental health of the nurses under pressure and their colleagues, patient care and working environment, and in general, on the efficiency of the health centers and healthcare services. The available evidence suggests that encountering stressful situations has resulted in lack of self-worth; interference with personal communications; and also psychological (depression), behavioral (crying and nightmares), and physical (palpitation and headache) impacts on the nurses. 10 In 2012, Wiegand and Funk 11 reported that nurses experience a range of anger, frustration, and depression when encountering moral distress. Furthermore, moral distress has been reported as a principal factor in attrition and resignation. 12 A review of literatures during 1984–2011 by Oh and Gastmans 13 showed that many nurses experienced burnout and moral tension in complicated caring situations which had negative impact on their professional function. In qualitative study (2016), the experiences of nurses, clinical nurse leaders, physicians, and other health professionals of three ICUs showed that the most common causes of moral distress were worries about the care provided by other healthcare-workers, the amount of care provided, poor communication, inconsistent care plans, and end-of-life decision-making. 14 moral distress needs to be responded in the best possible way. In this respect, the Canadian Nurses Association 15 has highlighted and recommended special attention to certain principles such as diagnosing moral distress, referral to nursing ethics codes, requesting support from colleagues, supporting the healthcare team and ethical committees, nursing associations and unions regarding moral distress.
Beumer
16
suggested conducting workshops as an effective intervention for reducing moral distress. One of the available models regarding moral distress belongs to Lawrence. In this model he studied how nurses’ moral distress, education level, and critical reflective practice are related to their work engagement. He also recommended interventions such as debriefing, participation in ethical continuing medical education
Reviewing the literature in the last few decades shows that writing about important and stressful life experiences can improve one’s physical and emotional health status. 18 In other words, when people narrate their emotional experiences into words, a significant change in their mental and physical health is observed. In addition, narrative writing/speaking about emotional subjects can improve the emotional status which can itself cause positive effects on the somatic health. 18,19 Pennebaker, an American psychologist first introduced narrative writing as a therapeutic approach to the medical community. He asked his students to write about their deepest traumatic emotional thoughts and experiences for 20 min in four consecutive days. The investigations were performed 4 months later revealed positive effects for narrative writing in comparison to the control group. 20
Most of the studies performed on narrative writing have included patients. To date, very few studies have investigated the use of this non-medical approach as a technique for expressing the thoughts and emotions as a means of coping with stress among nurses. Berlinger 21 writes that the critique of situations that cause moral distress is difficult but writing about them is a way to critically examine these experiences.
Therefore, this study attempted to test the hypothesis of using narrative writing in a hospital setting. This study was performed aimed at determining the effectiveness of narrative writing on moral distress among nurses working in ICUs.
Trial design
Materials and methods
This single-blinded randomized clinical trial was conducted in 2015 in Golestan University of Medical Sciences, Gorgan, Iran on nurses working in the two hospitals in ICUs. One hospital is a specialized center with 400 active beds over 85 years of age. The other is 3 years old and with 300 beds in the field of medical surgical units, obstetrics and gynecology units, and ICUs.
The data analyzer was blind to the allocation of groups to intervention and control. The study had a pre-test post-test design. In order to control unexpected and unpredictable variables, the comparison was used before and after intervention. In the research by Kadivar et al. 22 the pre-test post-test method was used.
The study protocol was fully approved by the Ethics Committee of Golestan University of Medical Sciences (Code: 25181693102122). An informed consent was obtained from each participant prior to study entrance. The trial was registered in the Iranian registry of clinical trials (IRCT201408137821N12) before starting participant recruitment.
The inclusion criteria were as follows: BSc degree in nursing, at least 6 months of work experience in the ICU, no history of an acute stressful experience, and not using any medication related to psychotic disorders in the last 6 months. The participants were excluded from the study in case of leaving the ICU during the study period.
According to the random numbers table, nurses who had the criteria for entering the study and were willing to participate in the study, divided into two groups of intervention and control. For the intervention group, in coordination with the head nurse and considering their free time, an educational session was held to explain how to write clinical narratives. At the time of the training sessions, nurses of the control group were not present at the hospital.
Of 130 nurses working in the ICUs, 120 filled the inclusion criteria and were enrolled in the study (Figure 1). By using the table of random numbers, 60 nurses were allocated using random blocks of four or six in a 1:1 ratio to each of the intervention and control groups.
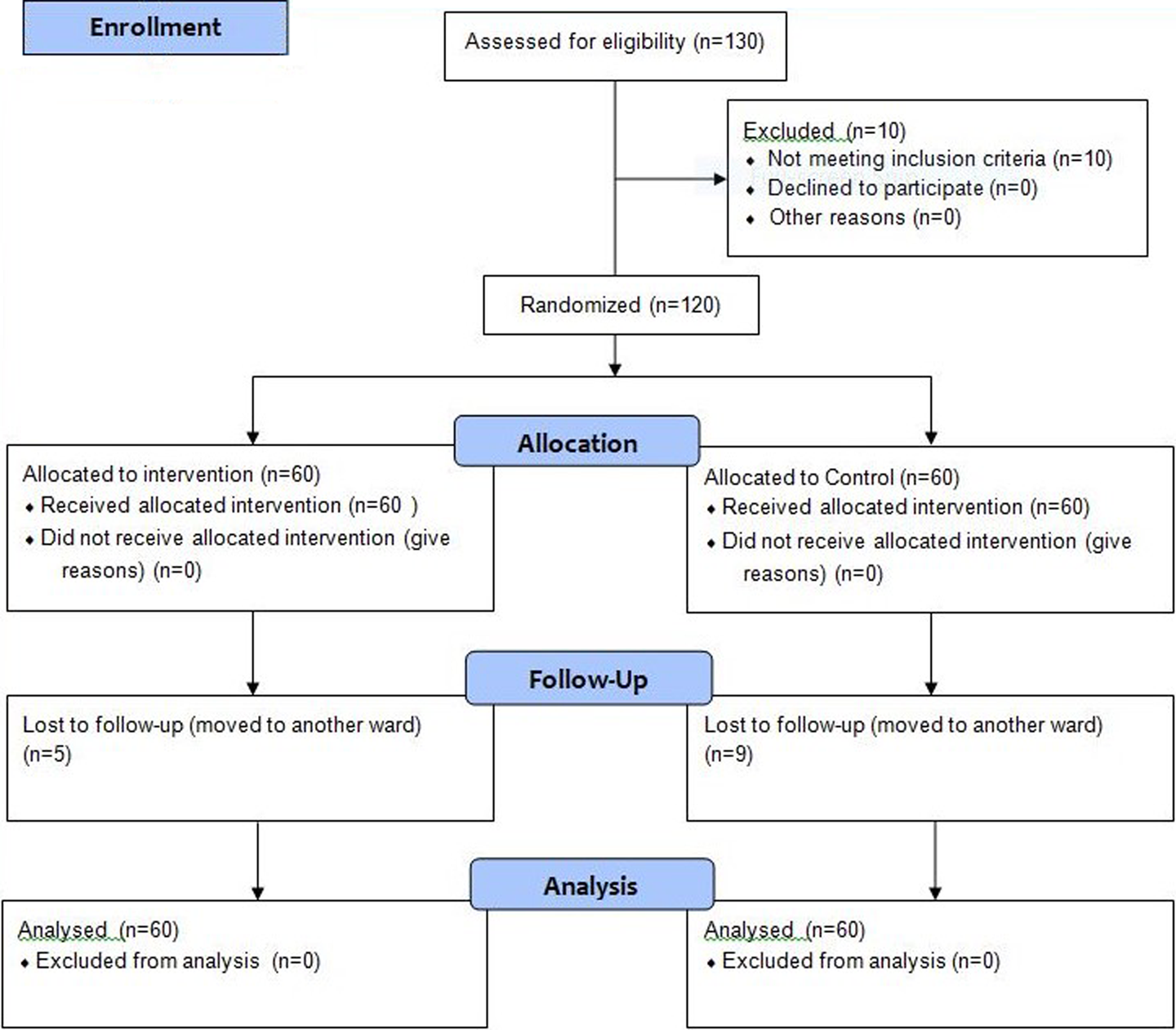
Flow diagram for participants included in study.
The nurses in the intervention group were asked to narrate their thoughts and emotions regarding their tensions at least once a week for 8 weeks in the form of words, including their best/worst moral experience, most difficult moment, worst behavior in relation to the patient, colleagues, doctors, supervisors, patient’s accompanies, and the service personnel in notebooks designed with this purpose.
Notebooks with 15 pages of the A5 size were provided; the first few pages consisted of the study guideline. The definition of moral stress, narrative writing, and a sample of this type of writing was included. The remaining blank pages were divided into eight sections for the 8 weeks of narrative writing. The notebooks were checked by one of the researcher (project leader) to assure of its relation with the topic of research (moral distress).
The intervention was run for 8 weeks for the following reasons: the nurses of the ICU had very high workload due to a shortage of manpower. At the same time, the hospital accreditation scheme was implemented in Iran, which was associated with a large amount of written work, then prolonging the duration of the intervention due to current organizational constraints in hospitals, was perceived extra burden on nurses and therefore be considered one of the limitations of the study. Liao et al. 23 also referred to the local and systems factors and limited opportunities to engage in narrative medical writing among medical residents. Evidences regard to the duration of the narrative writing and subsequent follow-up were varied from 3 day 22 to 4 weeks, 24 7 to 10 weeks 16 and 6 months. 25 But the subjects of none of those studies were on moral distress. In Beumer’s study, the effect of workshop on moral tension was investigated after 7–10 weeks follow-up. 16
The required data were collected by data registration form, moral distress questionnaire and narrative-writing notebook. The data registration form consisted of demographic data such as age, work experience, and type of employment. The Corley moral distress questionnaire which is translated to Persian and its validity and reliability are confirmed in the Iranian population was used for data collection. This questionnaire was translated by Nafchi et al. 26 by the two-way translation method both from English to Persian and vice versa, and two versions were studied regarding the case agreement. Its validity was approved by 10 professors of the Nursing and Midwifery School. The content validity index (CVI) of the questionnaire was 88% with a Cronbach’s alpha coefficient of 90%. 26 The frequency and intensity of moral distress among nurses was measured by 21 items based on the 5-point Likert-type scale. Frequency of moral distress in this questionnaire is defined as the number of exposures to stressors which ranges from “never exposed: 0 score” to “frequent exposure: 5 scores.” moral distress intensity is expressed as the amount of stress experienced by the patient when encountering stressful situations; it varies from “it causes no distress for me: 0 score” to “it causes major distress for me: 5 scores.”
The participants were randomly divided into two groups; and a briefing meeting was held to familiarize them with the study protocol and the notebook filling. The intervention group was asked to narrate in words at least once a week for 8 weeks. At the end of the study course, the moral distress questionnaire was once again filled for both groups.
We used intention-to-treat analysis. The collected data were analyzed by the SPSS, version 18. Normality assumption was initially done to choose the appropriate parametric/non-parametric tests. The frequency and intensity of moral stress had a normal distribution in both groups. Therefore, paired-sample t-test and independent-sample t-test were used for intergroup comparisons. The significance level was set at P < 0.05.
Results
Among the 120 nurses enrolled in the study, 106 nurses; 51 controls and 55 interventions completed the study course. In intervention group lost to follow-up was five and in control group lost to follow-up was nine (those participants transferred to other units during the study). In total, 89.1% of the interventions and 82.4% of the controls were female. In total, 58.2% of the interventions and 62.7% of the controls were officially recruited and 98.2% and 98% had a BSc degree in nursing, respectively. The Kolmogorov–Smirnov test showed no meaningful difference between the two groups in this respect. The mean age of the participants in the study and control group was 33.72 ± 6.34 years and 31.20 ± 5.62 years, respectively (P = 0.34). The mean length of work experience was 7.21 ± 4.96 and 8.28 ± 5.45 years, respectively (P = 0.29; Table 1).
Demographic data of the nurses.
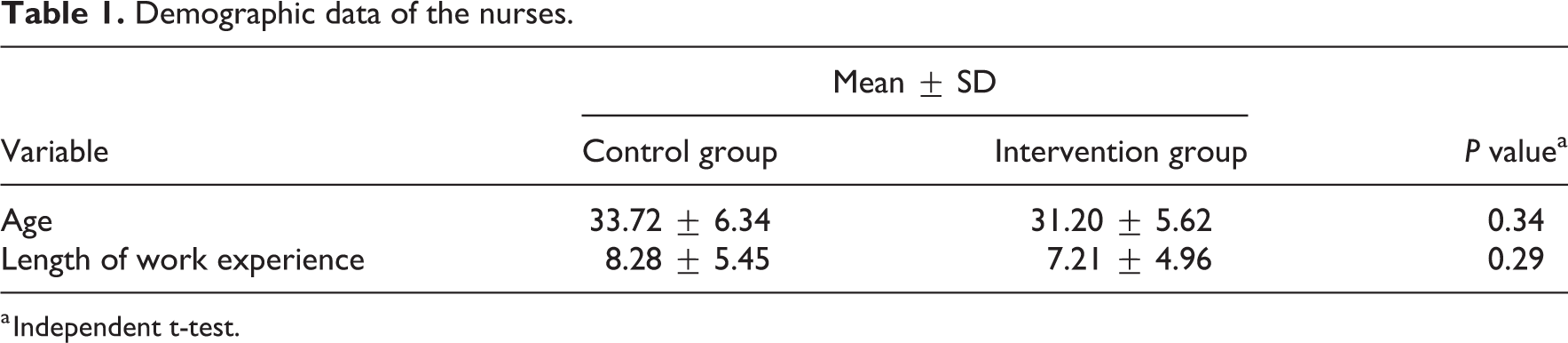
a Independent t-test.
Comparing the mean and standard deviation of moral distress intensity (P = 0.17) and moral distress frequency (P = 0.49) in the control group showed no significant differences (Table 2). Comparing the mean and standard deviation of moral distress intensity (P = 0.8) and moral distress frequency (P = 0.27) in the intervention group showed no significant differences (Table 2).
The intensity and frequency of moral distress before and after in intervention and control groups.
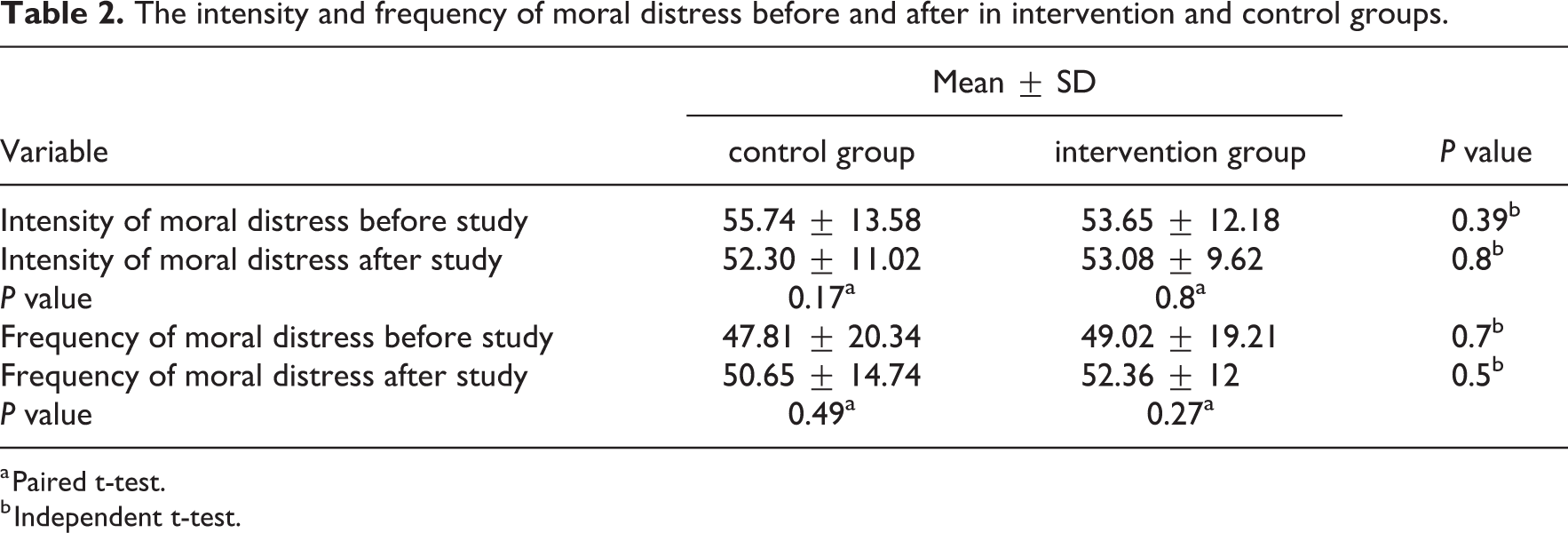
a Paired t-test.
b Independent t-test.
Comparing the mean and standard deviation of moral distress intensity in both groups before (P = 0.39) and after intervention (P = 0.8) showed no significant differences. The frequency of moral tension before (P = 0.7) and after the intervention (P = 0.5) also showed no statistically significant difference (Table 2).
Discussion
The findings of this study showed that narrative writing for 8 weeks by ICU nurses had no remarkable impact on their moral distress level and no meaningful difference was observed between the interventions and controls in this respect. This research is the first study in Iran that examined the effect of narrative writing on moral distress of nurses in ICU. The use of narrative writing in hospital setting and ICU was a new feature of this study. It seems that clinical situation, time restriction of nurses in ICU, and high workload has been effective in creating the present results. In a meta-analysis conducted in 2006, the health effect of expressive writing regarding stressful and traumatic events was studied in 42 clinical trials. The results revealed minor or no effects for expressive writing on detrimental health outcomes. 27 In the study by Borimnejad et al., 24 narrative writing was not effective on the psychological distress of 78 vitiligo patients too. Although the results of the mentioned study are in agreement with the findings of this study, yet the study populations differed. This study also showed no positive effect for expressive writing in reducing moral distress among nurses. In the study by Mohamadi et al., 25 regarding the effect of ethics training on the moral distress experienced by nurses, the teaching proved to result in significant reduction in moral distress in this group, but the intervention was educational and different from this study.
This study is the first survey investigating narrative writing on moral distress among nurses in clinical units. In the study by Smyth et al., 28 regarding the effect of narrative writing of stressful events on reducing the symptoms of patients’ affected by asthma and rheumatoid arthritis, the pulmonary function of asthma patients improved significantly after 4 months of expressive writing.
Petrie et al. 29 also investigated the effect of narrative writing on the immunity system’s function in HIV patients, showing a positive effect on the CD4 level. In the study by Baikie et al. 30 in Australia, the effect of narrative writing was examined on patients with psychological disorders; it demonstrated reduced stress levels among such patients. The results of the abovementioned studies all confirm the role of narrative writing in reducing clinical symptoms in various diseases, yet our study had inconsistent results. This difference could be due to the study population, cultural differences, or different measurement scales. Cultural discrepancies and performing the study in Iran could have affected the obtained results.
As these findings suggest a positive effect in reducing the clinical symptoms in the patient population, this technique has also been applied as an effective strategy among students and healthy individuals in certain studies. In the study by Pennebaker et al., 31 expressive writing among students resulted in reduced referral rates to health centers.
Pizarro 32 also reported reduced stress levels among students who used narrative writing following encounter with traumatic events, their results were again in disagreement with our findings.
From another perspective, the positive effects of narrative writing on somatic health are related to the number of such narrations, 33 whereas an increase in the number of sessions resulted in more positive outcomes in adolescents. This study suggested that expressive writing in consecutive days can have a positive influence on the negative experiences of adults; however, the interval between sessions should be increased for adolescents so that he or she has enough time to process and trigger the emotions by writing. 34
In this study, narrative writing was done at least once a week for a duration of 2 months, resulting in no positive outcome. Therefore, a longer duration and more frequent narrations may be required to demonstrate a positive impact on the moral distress experienced by nurses.
The aforementioned studies were mostly performed on non-nurse populations, whereas our study sample consisted of nurses working in the ICUs whom experience a far different occupational distress level in comparison to other groups.
Nevertheless, age, sex, culture, social class, and personality type can affect the final outcome. In a study using a text-analysis computer program, it was shown that those benefit the most from writing who try to use more positive-emotion words and fewer negative words and phrases. 19 In this study due to the nature of moral distress, the words used by nurses mostly had a very high negative burden. The lack of respectful working relations, pressures imposed by physicians and managers, financial problems, and the workload were all the negative experiences narrated by the studied nurses.
In a study taking into account 10 trials on non-official care givers providing support to the elderly and disabled, written emotional disclosure led to trauma reduction in four studies and improved general psychological health in three others. However, no evidence was found regarding improvement in depression, anxiety, physical symptoms, quality of life, or life burden. 35
Some evidence suggest that teaching religious beliefs during university education 36 and conducting educational workshops, 16 educational programs, changing the working culture, active engagement with hospital ethics committees, journal clubs, and official teaching courses can positively affect moral distress. 37 Nevertheless, further clinical trials on larger populations and for longer intervals with clearly described interventions and standardized outcome measures are needed to confirm these findings.
It is suggested that in future studies compare writing narration in a use standardized and laboratory setting with the actual situation in the clinical one. Iranian nurses in ICU are involved with lots of paper works, it might be better to use oral narration (such as storytelling) instead of written. It seems that nurses should be familiar with writing narration and reflection thinking from studenthood so that they can better use it as a clinical nurse in dealing with work tension or moral distress.
The main limitation of this study was the nurses’ concern regarding writing of their moral distress in the notebooks. Moreover, our people are not used to writing; therefore, the nurses did not feel comfortable with the notebooks. The lack of appropriate physical space and adequate time due to their workload was another limitation in this respect.
Conclusion
The study findings showed that weekly narrative writing for events that cause moral distress in the work environment did not result in reduced moral distress among the ICU nurses during 8 weeks.
The reason may be the lack of appropriate physical, cultural, and social conditions for performing this intervention. It seems that the basic root of stress and the way nurses deal with these issues every day has affected the final outcome. Moreover, the probability of an undesired feedback from the matrons and supervisors may have avoided the nurses to freely narrate all aspects of the experienced tensions. On the other hand, the act of just writing about such situations without taking appropriate measures for reducing them in the wards may have also influenced the study results. Therefore, the following issues are recommended to be considered in future studies: studying the role of narrative writing of positive events on the moral distress of ICU nurses and studying the role of online narrative writing and also storytelling on moral distress reduction among ICU nurses.
Footnotes
Acknowledgements
The authors wish to thank the Education Development Center and Deputy of Research, Golestan University of Medical Science, as well as the officials and ICU staff of the Teaching Hospitals for their participations. This article was derived from a master thesis of Smat Saeedi at Golestan University of Medical Sciences, Gorgan, Iran.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The research proposal was financially supported by Golestan University of Medical Sciences.